

Abstract
Objectives:
Throughout human evolutionary history, parasites and pathogens were a major cause of mortality-modern urban life with public health infrastructure has changed disease exposure. We examine associations between boiling water, using latrines, mosquito net usage, and biomarkers among the Tsimane, a nonindustrial subsistence population with little public health infrastructure.
Methods:
We conducted cross sectional surveys on water, latrines, and bed nets among 507 heads of households (aged 18–92 years, median age 41 years). Regression models estimated associations between behaviors and health biomarkers (ie, white blood cell count [WBC], hemoglobin, eosinophil count, and erythrocyte sedimentation rate) adjusting for age, sex, body mass index, wealth, schooling, and distance to the nearby market town.
Results:
Latrine use is associated with 6.5% lower WBC count (β = −679.6, P = .031, SE = 314.1), 17.4% lower eosinophil counts (β = −244.7, P = .023, SE = 107.2), and reduced odds of eosinophilia (adjusted OR = 0.40, P < .019, 95% CI = 0.18–0.86). Boiling water and mosquito net use are not significantly associated with any biomarkers measured.
Conclusions:
In a subsistence population currently undergoing epidemiological transition, we find that latrine use was associated with several objective measures of health. This suggests that relatively low cost and low maintenance public health interventions may wish to focus on latrine use, as there is unmet need and potential health benefits for those who use latrines. Additionally, while the cost is higher, public health organizations aimed at improving sanitation may be able to use minimally invasive field-collected biomarkers as a diagnostic to objectively test the efficacy of interventions with greater specificity than anthropometric measurements.
1. INTRODUCTION
Throughout most of human evolutionary history, parasites and pathogens were a major cause of morbidity and mortality. In industrialized urban environments with sanitation and clean water, obesity-related noncommunicable diseases and cardiovascular disease have become highly prevalent. However, from an evolutionary perspective these chronic diseases of aging may be relatively novel compared to “old friends” like certain parasites and pathogens (Kaplan et al., 2017; Rook, 2009; Rook, Lowry, & Raison, 2013). Nearly 2.5 billion people worldwide lack access to adequate sanitation facilities, 71% of whom live in rural communities (WHO/UNICEF, 2015). Contaminated water is a major source of pathogens causing infectious diarrheal diseases, which are a leading cause of death worldwide, accounting for 4.6 billion cases and 2.2 million deaths per year (Selendy, 2011). In addition to diarrheal disease, mosquito-borne diseases disproportionately burden low- and middle-income countries, especially rural communities, and indigenous populations (Hotez, Bottazzi, Franco-Paredes, Ault, & Periago, 2008). Diarrheal and mosquito-borne diseases are exacerbated by inadequate sanitation. Use and uptake of latrines, mosquito nets, and boiling water prior to consumption can therefore dramatically improve individual and community health in a cost-effective manner. These three interventions do not require formal infrastructure (eg, electricity), and can be done by individuals, not requiring political or governmental organization. While feasible to implement, the costs of boiling may be high depending on the availability of fuel. Similarly, latrines take time and energy to build; both latrines and mosquito nets need to be well maintained. Here we examine how objective sub-clinical health biomarkers covary with use of latrines, mosquito nets, and with boiling water prior to consumption in a rural indigenous population of forager-horticulturalists, that while living in environments similar to those experienced throughout evolutionary history, are currently undergoing an epidemiological transition.
Latrines are often considered the first crucial step toward improved sanitation. Pit latrines are cost effective and often the first step toward higher-cost toilet systems (Mara, Lane, Scott, & Trouba, 2010). Moving from open defecation to a fixed latrine is associated with reduced burden of diarrheal diseases, lower rates of neglected tropical diseases, and less undernutrition by interrupting fecal-oral transmission pathways (Mara et al., 2010). However, unimproved latrines are not universally effective: a recent randomized controlled trial in rural India found no evidence that latrine construction reduced exposure to fecal contaminants, diarrheal disease and mortality (Clasen et al., 2014). Heterogeneity within rural populations of latrine access and use offers an opportunity to understand the extent to which latrines can reduce pathogen load, independently and/or through interactions with clean water and bed nets.
Access to clean drinking water is also fundamental in reducing the spread of fecal contaminants and diarrheal disease. For the ∼660 million people who lack access to clean drinking water, 8 of 10 of which live in rural areas, boiling water is an effective strategy for removing pathogens (WHO/UNICEF, 2015). While there are a variety of water treatment methods available (eg, chlorination, filtration, etc.), boiling water is the most common household water treatment method, used by 1.2 billion people worldwide (Cohen & Colford, 2017), and was likely the first water treatment method (Speth, 2015). There is evidence of wet-cooked food and boiling in the upper Paleolithic, and possibly as early as the middle Paleolithic (Henry, Brooks, & Piperno, 2011; Speth, 2015). Just as cooking increases food digestibility (Carmody, Weintraub, & Wrangham, 2011; Carmody & Wrangham, 2009) in part through eliminating bacteria (Smith, Carmody, Dutton, & Wrangham, 2015) and parasites (Perry, 2014), boiling water reduces pathogen load, and in calorie-limited settings permits greater energetic allocations to critical life functions apart from combating infection, including growth, and reproduction.
Mosquitos are vectors for a number of diseases such as malaria, dengue, yellow fever, West Nile virus, chikungunya, and other neglected tropical diseases. In the context of Bolivia, bed nets also are protective against phlebotomine sand flies, which transmit leishmaniosis (Teles et al., 2016). Malaria and other neglected tropical diseases account for an estimated 720 000 deaths and 49 000 years of life lost per year (Roth et al., 2018). There are a number of well-studied human genetic adaptations to malaria, suggesting that humans have a long coevolutionary history with malarial disease (Etkin, 2007; Perry, 2014). Mosquito nets can be effective at preventing mosquito bites, especially among young children; a recent review estimated that use of insecticide-treated nets can reduce childhood mortality by one-fifth and overall malaria incidence by nearly one half (Pryce, Richardson, & Lengeler, 2018). However, in many rural areas, the efficacy of bed nets has been questioned, as the quality of nets and general misuse (eg, as fishing nets) can hinder effectiveness (Mutuku et al., 2013).
In this manuscript we test for associations between boiling water, latrines, and mosquito net usage, and objective health biomarkers among Tsimane forager-horticulturalists of lowland Bolivia. Most previous studies of public health have used simple indirect measures of health, such as anthropometric measurements like body mass index (BMI). Such measures provide crude insight into health status, but may not accurately assess undernutrition or obesity (Hruschka & Hadley, 2016), and do not address the functioning of other bodily systems, such as the immune or endocrine systems. We chose biomarkers that provide a more comprehensive view of current health status, including hemoglobin (Hb; a marker of anemia status), total white blood cell count (WBC; a marker of overall pathogen burden), eosinophil count (a marker of helminth infection), and erythrocyte sedimentation rate (ESR; a marker of general inflammation) (Blackwell et al., 2016).
Tsimane have relatively low levels of market integration, minimal or no access to electricity and no access to potable running water or other forms of community-level sanitation including sewage treatment (Gurven et al., 2017). Tsimane practice a traditional lifestyle of horticulture, fishing and hunting, producing the vast majority of their calories via their own subsistence efforts (Kraft et al., 2018; Stieglitz et al., 2014; Trumble, Smith, O’Connor, Kaplan, & Gurven, 2014). Tsimane communities vary in distance and access to the closest market town of San Borja (population ∼30 000), where individuals have access to a hospital and pharmacies (Alami, Stieglitz, Kaplan, & Gurven, 2018). Some Tsimane communities have access to wells or water pumps. Previous Tsimane research found evidence of fecal coliforms and Escherichia coli in the local Maniqui river (along which ∼60 Tsimane communities are located), and fecal coliforms in open wells (Rosinger & Tanner, 2015). With contaminated water sources, evidence of a high pathogen load from soil transmitted helminths and numerous other infectious exposures (Blackwell et al., 2011; Blackwell et al., 2015; Blackwell et al., 2016), and a high mosquito burden, the Tsimane are an ideal population to estimate the relative efficacy of sanitation, clean water, and mosquito nets for improving health in a nonmalarial Amazonian context, and to demonstrate that biomarkers can be an effective tool for assessing the success of public health interventions.
While many studies examine how water, bed nets, and sanitation interact with health in rural settings, we expand on the current literature by testing whether these behaviors are additive or interactive; for example is latrine use more effective if water is also boiled? Exposure to pathogens such as those found in contaminated water can influence fecundity, growth, and productivity (Blackwell et al., 2015; Blackwell et al., 2016; Blackwell et al., 2017). Since sewage, clean water, and mosquito nets are all commonly utilized by public health interventions, understanding the objective health contributions of water source, sanitation, and mosquito net use can help public health institutions prioritize scarce resources.
2. METHODS
2.1. The Tsimane
The Tsimane Health and Life History Project (THLHP) is an anthropological, biomedical surveillance project, ongoing since 2002 to understand aging and human health through an evolutionary perspective. With a variety of foci, the project combines methods from traditional ethnography with demography, epidemiology, biomedicine, economics, psychology, and gerontology (Gurven, Stieglitz, et al., 2017). There are ∼16 000 Tsimane living in ∼95 communities— ranging in size from about 50 to 600 individuals (Gurven, Stieglitz, et al., 2017). A team composed of Bolivian physicians, biochemists, and Tsimane anthropologists visits each of the 90 sampled Tsimane villages annually or biannually to diagnose and treat health conditions, while monitoring health, demography, and socioeconomic indicators. For all study protocols, institutional IRB approval was granted (University of New Mexico, University of California Santa Barbara, Arizona State University), as was informed consent at three levels: (a) Tsimane government, (b) village leadership, and (c) individual study participants.
2.2. Survey data collection
Our sample is a cross section of households across 46 communities, based on THLHP data collection between January 2013 and November 2014. This time period was selected as it was all biomarker and public health data that were collected before a major flood, which significantly impacted Tsimane health and wellbeing for several years (Rosinger, 2018; Trumble et al., 2018). One head of each household (n = 507, aged 18–92, median age 40 years) was interviewed in their home by trained Tsimane researchers on household water source, use of mosquito nets for sleeping, sanitation habits, and latrine use as a part of a larger study focused on aging. Note all latrines in this study sample are unimproved pit latrines. All heads of household who were present in the community completed a public health interview, and a subset of individuals also provided biospecimens (all individuals over age 40, and a random sample of those aged 18–39). Each interview took ∼45 min. Participants were asked where they most frequently collected their water, most frequent location for defecation, and if they use a mosquito net. Participants were asked how often they boiled water on an ordinal scale, ranging from always, usually, almost never, and never, which was then transformed into a binary always and usually vs never and almost never. Participants were compensated for their time.
2.3. Biomarkers of health status
Fasting morning blood draws were collected by venipuncture by a licensed Bolivian biochemist as a part of routine medical surveillance from a subset of n = 507 individuals. After drawing blood, total leukocyte counts, and hemoglobin were measured with a QBC Autoread Plus dry hematology system (Drucker Diagnostics, PA). A five-part differential measuring relative fractions of neutrophils, eosinophils, lymphocytes, basophils, and monocytes were determined manually with a hemocytometer. ESR was calculated using the Westergren method (Westergren, 1957). Results were communicated to a Bolivian physician who then used the information to help diagnose and treat patients.
Height was collected on a Seca 214 portable stadiometer, and weight measured with a Tanita BC-2300 digital scale. Wealth was calculated based on a material style of life inventory, and individuals were asked about the highest grade level of formal schooling they completed. Adults who had attended adult-education classes were recorded as having a grade level equivalent based on how long they attended.
Health status was assessed by analyzing levels of the following biomarkers: white blood cell count (WBC), hemoglobin (Hb), ESR, and log eosinophil count. The levels of each biomarker can indicate the relative immune health of the individual. In healthy individuals, we would expect to see lower WBC, ESR, and eosinophils, and higher Hb. Each biomarker indicates a different yet complimentary view of the participants baseline immune function (see Table 1).
TABLE 1.
Sample characteristics of Tsimane participants, including biomarkers of health status, as well as proportion of respondents boiling water, using latrines and mosquito nets (n = 507)
| Mean | Median | 95% CI | ||
| White blood cell count (cells/mm3) | 10 430.5 | 10 100.0 | 10 147.4 | 10 713.6 |
| Hemoglobin (g/dL) | 13.8 | 14.0 | 13.7 | 13.9 |
| Erythrocyte sedimentation rate (mm/hr) | 18.8 | 18.0 | 18.0 | 19.6 |
| Eosinophil count (cells/mm3) | 1400.4 | 1141.5 | 1294.6 | 1506.2 |
| Age (years) | 41.8 | 40.8 | 40.6 | 43.0 |
| Body mass index (kg/m2) | 22.9 | 22.8 | 22.6 | 23.1 |
| Distance to market town (km) | 47.3 | 43.2 | 44.8 | 49.8 |
| Sum of wealth (Bolivianos) | 6075.4 | 4773.5 | 5451.6 | 6699.1 |
| Highest grade level | 2.8 | 2 | 2.52 | 3.06 |
| Proportion | 95% CI (Binomial) | |||
| Always/usually boil water | 0.21 | 0.17 | 0.24 | |
| Has latrine | 0.24 | 0.21 | 0.28 | |
| Use mosquito net | 0.85 | 0.00 | 1.00 | |
| Sex (male) | 0.94 | 0.92 | 0.96 | |
| Elevated WBC (>11 000 cells/uL) | 0.40 | 0.35 | 0.45 | |
| Eosinophilia (>500 Eosinophils/uL) | 0.86 | 0.77 | 0.96 | |
| Anemia (Hb <12 g/dL Female, <13 g/dL Male) | 0.08 | 0.60 | 0.11 | |
| Obese (BMI >30 kg/m2) | 0.01 | 0.003 | 0.02 | |
Standard WHO cutoffs for eosinophilia (>500 eosinophils per mm3) (Gotlib, 2017), Obesity (BMI >30 kg/m2) (Garrow & Webster, 1985; Hruschka & Hadley, 2016), Anemia (Hb <12 g/dL for women, <13 g/dL for males) (Domenica Cappellini & Motta, 2015) were also used to create binary variables of disease state.
2.4. Statistical analysis
Linear regression models with robust standard errors were used to examine associations between sanitary survey responses and health biomarkers. All biomarkers approximated a normal distribution except eosinophil counts, which were log transformed for analyses. We controlled for age, sex, distance to the nearby market town of San Borja, and BMI, as previous studies find variation in several biomarkers associated with these factors among the Tsimane (Blackwell et al., 2016; Stieglitz et al., 2015; Trumble et al., 2016; von Rueden et al., 2014). Additionally, as public health campaigns may have visited some communities and not others, we controlled for community regions, and included an interaction term between region and distance to town. Interactions between public health behaviors were tested, but none were significant. Additionally, an index variable of the number of public health behaviors (latrine, boiling water, net use) from 0 to 3 was also created and tested, but was not significant in any model. Past studies indicate that biomarkers vary by season, so a binary variable of rainy season (October through April) vs dry season (May-September) was included (Blackwell et al., 2016). Additional control variables included total asset wealth (log adjusted for normality), and below and above median years of schooling (<2, vs ≥2 years) (Gurven et al., 2017). Many public health related studies find important impacts of wealth and education level of both health status and knowledge of the best public health practices, and thus they were included as control variables.
Logistic regressions with robust standard errors were used to examine associations between sanitary survey responses and clinical cutoffs for eosinophilia, obesity, and anemia. The same control variables (age, sex, distance to town, season, wealth, and education) were used.
Age, body mass index (BMI), and distance to town were centered. Variance inflation factors (VIF) were calculated for all models to ensure there was no collinearity; all VIFs were below 2.5. Analyses were conducted in STATA 14.
3. RESULTS
In this sample, 24% of respondents reported using a latrine (vs open defecation), 21% reported always/usually boiling water (vs almost never, and never), and 85% reported using a mosquito bed net (see Table 1). These behavioral patterns varied by community and region (Figure 1).
FIGURE 1.
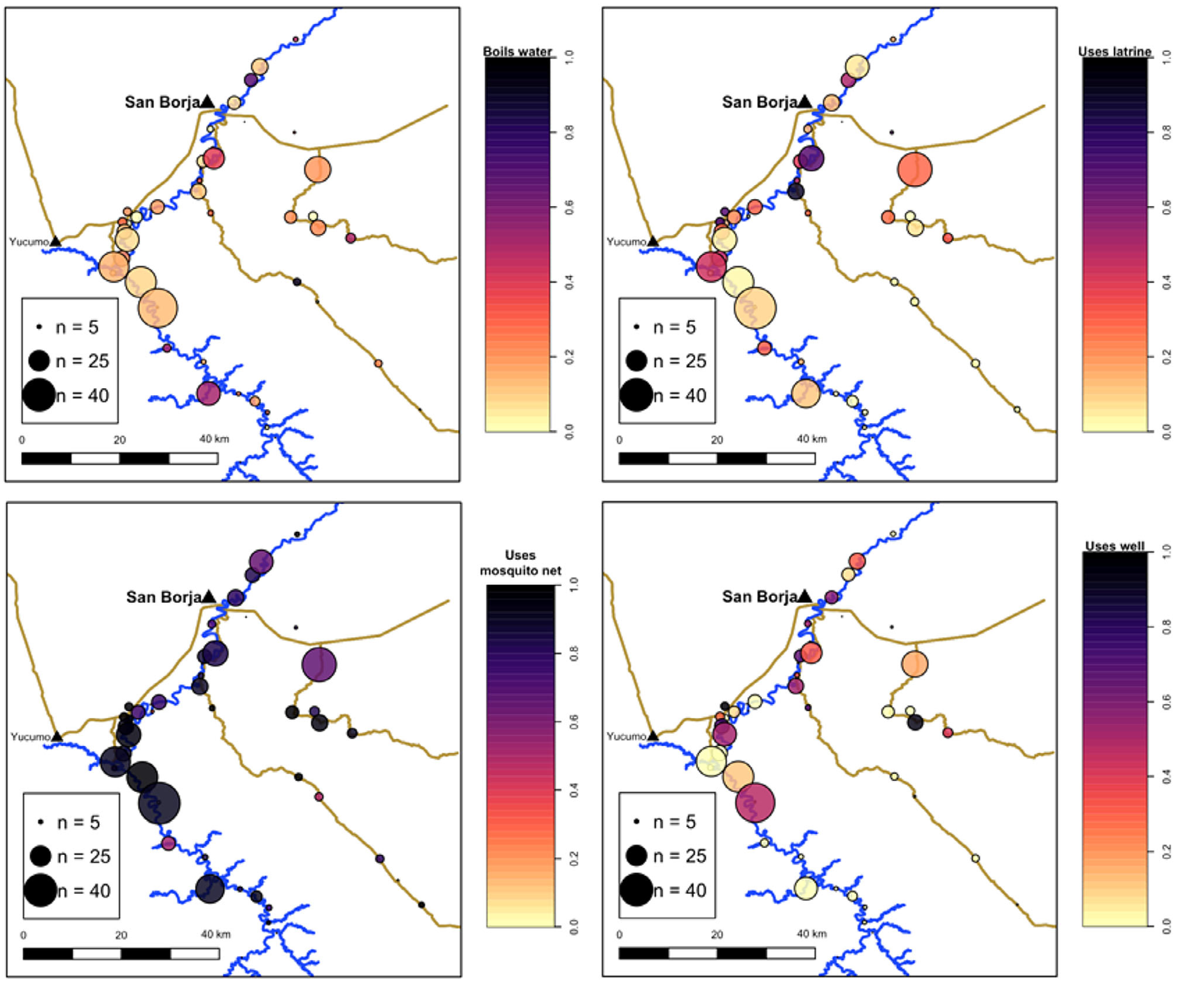
Heat map of health-promoting behaviors across sampled Tsimane communities. The color continuum indicates uptake of health-promoting behavior as the proportion of sampled households per community (light: no uptake; dark: full uptake). Circle size represents sample size per community
3.1. White blood cell counts
Latrine use was significantly associated with lower WBCs (Std. β = −0.085, P = .031) after controlling for age, sex, BMI and distance from town, wet season, log wealth, and education (Tables 2 and S1, Figure 2). Individuals who used latrines had 680 fewer WBCs per mm3, a mean difference 6.5% lower than those who did not use latrines. Boiling water and mosquito net usage were not associated with WBCs.
TABLE 2.
Associations between health-promoting behaviors and health biomarkers
| (1) | (2) | (3) | (4) | (5) | |
|---|---|---|---|---|---|
| Hemoglobin (g/dL) | Sedimentation rate (mm/hr) | Body mass index (kg/m2) | Log eosinophil count | White blood cell count (1000/mm3) | |
| Boil water | −0.177 (0.155) |
−0.165 (1.152) |
0.456 (0.287) |
−0.093 (0.097) |
−523.977 (355.845) |
| Latrine | 0.231 (0.1155) |
−0.981 (1.212) |
0.430 (0.287) |
−0.193* (0.092) |
−679.622* (314.075) |
| Mosquito net | −0.111 (0.210) |
−0.641 (2.295) |
0.427 (0.408) |
0.062 (0.119) |
−17.273 (732.435) |
| Age (centered) | −0.002 (0.006) |
−0.035 (0.040) |
0.009 (0.010) |
−0.008** (0.003) |
−60.764*** (12.554) |
| Distance to town (Centered) | 0.001 (0.002) |
−0.01 (0.015) |
−0.005 (0.005) |
−0.004** (0.014) |
−14.114* (5.788) |
| Body mass index (Centered) | 0.035 (0.022) |
−0.101 (0.182) |
−0.034* (0.014) |
−155.975** (55.521) |
|
| Male | 1 177*** (0.169) |
−7.915*** (2.146) |
0.140 (0.860) |
−0.097 (0.131) |
455.173 (689.471) |
| Season (1 = rainy) | 0.087 (0.127) |
−3.081** (0.951) |
0.001 (0.238) |
−0.294*** (0.080) |
−282.344 (320.752) |
| Log wealth | 0.152 (0.085) |
0.861 (0.599) |
0.524** (0.172) |
−0.001 (0.051) |
−428.536* (183.409) |
| Grade level > =2 | 0.090 (0.143) |
0.694 (1.109) |
1.03*** (0.266) |
0.089 (0.087) |
−217.296 361.589 |
| N | 490 | 327 | 503 | 320 | 475 |
| R2 | 0.063 | 0.089 | 0.088 | 0.177 | 0.155 |
Note: Each column represents a separate model controlling for age, distance to town, BMI, sex, season, total wealth, and schooling.
P < .05
P < .01
P < .001, parenthesis indicate SE.
FIGURE 2.
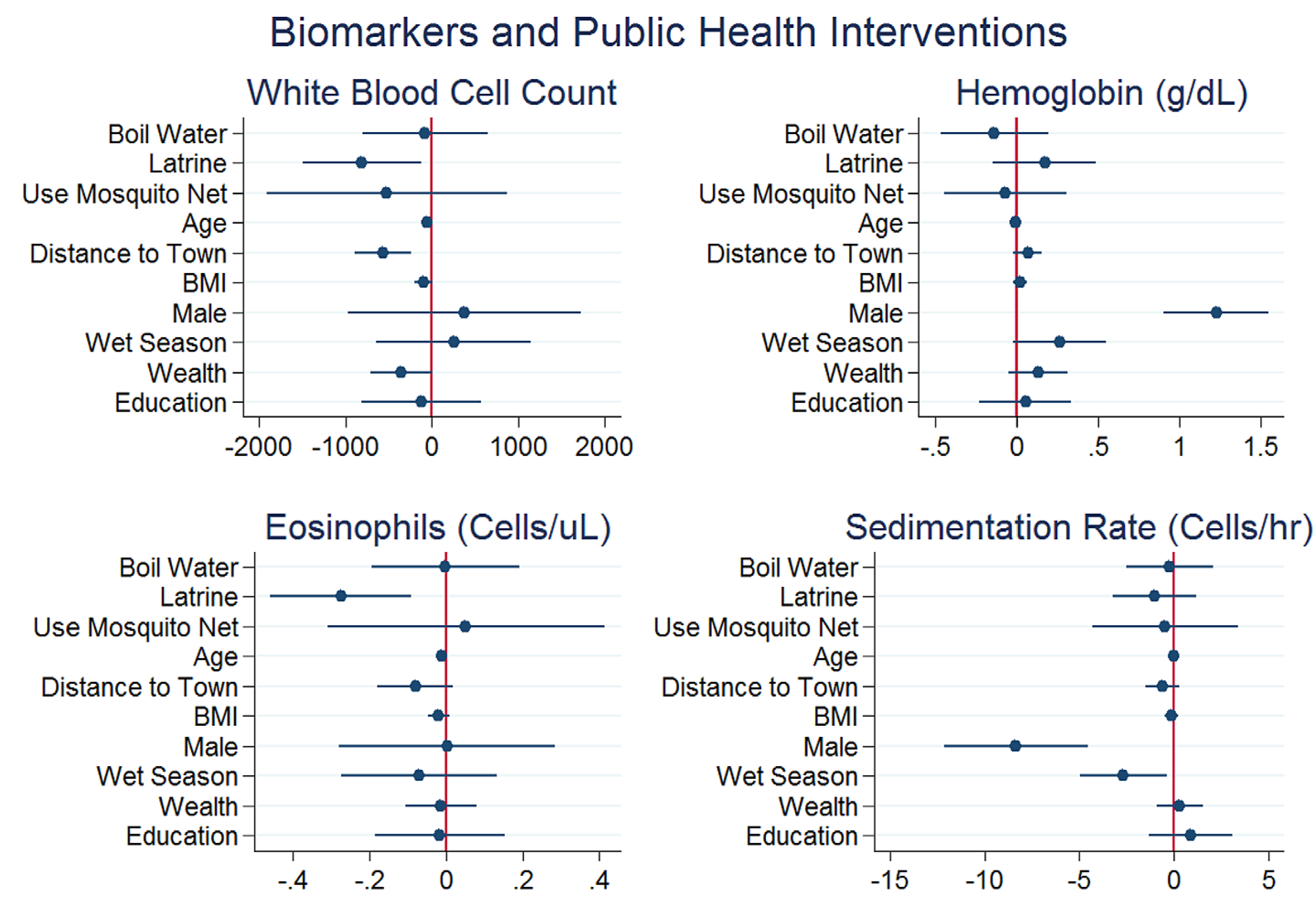
Associations between health-promoting behaviors and health biomarkers: white blood cell count, A, hemoglobin, B, eosinophil count, C, and erythrocyte sedimentation rate, D. Beta coefficients (95% CIs) are shown from regressions in Tables 2 and S1
3.2. Eosinophil counts
Latrine use was significantly associated with lower eosinophil counts (Std. β = −0.193, P = .036), while boiling water and net use did not impact eosinophil counts (all P > .342) (Tables 2 and S1, Figure 2). Individuals who used latrines on average had 245 fewer eosinophil counts, or levels ∼17.4% lower.
3.3. Hemoglobin
Neither latrine use, boiling water, nor mosquito net use were significantly associated with Hb levels (all P > .136) (Tables 2 and S1, Figure 2).
3.4. ESR
Neither latrine use, boiling water, nor mosquito net use were significantly associated with lower ESR, (all P > .153) (Tables 2 and S1, Figure 2).
3.5. Binary health outcomes
Logistic regressions were used to examine associations between behaviors and binary health outcomes including eosinophilia (elevated eosinophil count above 500 cells/uL), anemia (hemoglobin <12 g/dL for women and < 13 g/dL for males), being overweight (BMI > 25 kg/m2), and obesity (BMI >30 kg/m2), see Table 3. Latrine use was associated with a decreased odds of having eosinophilia (OR = 0.40, P < .019, 95% CI =0.18–0.86), controlling for age, BMI, sex, distance to town, season, log wealth and schooling. There were no associations between anemia status and these behaviors. Interestingly, the odds of obesity were higher among those who used latrines, (OR = 6.40, P = .019, CI = 1.70–25.67) with the same control variables, as were the odds of being overweight (OR = 1.71, P = .038, 95% CI = 1.30–2.84).
TABLE 3.
Associations between clinical cutoffs for health conditions and boiled water, latrine use, and mosquito net use
| (1) | (2) | (3) | (4) | |
|---|---|---|---|---|
| Eosinophilia | Anemia | Overweight | Obese | |
| Boil Water | 0.975 | 1.354 | 1.420 | 1.418 |
| (0.430–2.211) | (0.760–2.413) | (0.829–2.435) | (0.318–6.325) | |
| Latrine | 0.394* | 0.595 | 1.710* | 6.392* |
| (0.183–0.861) | (0.323–1.098) | (1.030–2.840) | (1.357–30.122) | |
| Mosquito net | 0.839 | 1.150 | 1.935 | |
| (0.110–6.395) | (0.379–3.487) | (0.504–7.433) | ||
| Age (centered) | 0.987 | 1.011 | 1.025* | 1.007 |
| (0.963–1.01) | (0.992–1.030) | (1.005–1.045) | (0.949–1.068) | |
| Distance to town (Centered) | 0.992 | 1.000 | 1.000 | 1.022* |
| (0.980–1.004) | (0.992–1.008) | (0.991–1.009) | (1.002–1.043) | |
| Body mass index (Centered) | 0.899 | 0.923 | 0.825 | 0.146 |
| (0.805–1.005) | (0.833–1.022) | (0.324–2.104) | (0.024–0.911) | |
| Male | 0.485 | 0.818 | 1.325 | 2.222* |
| (0.098–2.412) | (0.318–2.101) | (0.828–2.121) | (0.576–8.567) | |
| Season (1 = rainy) | 0.296*** | 1.120 | 1.314 | 1.931 |
| (0.140–0.626) | (0.694–1.805) | (0.984–1.756) | (0.634–5.885) | |
| Log wealth | 1.183 | 0.746* | 2.466 | 0.618 |
| (0.767–1.827) | (0.558–0.997) | (1.390–4.374) | (0.082–4.647) | |
| Grade level > =2 | 1.338 | 1.169 | 1.420** | 1.418 |
| (0.573–3.126) | (0.687–1.987) | (0.829–2.435) | (0.318–6.325) | |
| N | 320 | 503 | 503 | 480 |
| Pseudo R2 | 0.092 | 0.024 | 0.062 | 0.182 |
Note: Each column represents a separate model controlling for age, distance to town, BMI, sex, season, total wealth, and schooling. Note all obese individuals had mosquito nets.
P < .05
P < .01
P < .001, parenthesis indicate 95% CI.
Figure 2 demonstrates the relative impacts of each public health behavior on the measured biomarkers and allows for cross comparison to identify which behaviors have the strongest association for each of the four biomarkers. When controlling for age, sex, BMI, and distance to market town, season, log wealth and education latrine use is associated with the largest health impact for WBC, Hb, and eosinophils.
4. DISCUSSION
We investigated whether boiling water, latrine use, and mosquito net use were associated with biomarkers of health in an indigenous population without access to centralized clean water or sanitation facilities. Latrine use, but not boiled water or mosquito net usage, was associated with positive immune complements. Overall, latrine use was more strongly correlated with biomarkers of health status.
4.1. Latrine use
Household heads reporting latrine use had a number of positive health outcomes compared to household heads who did not have latrines. Specifically, latrine use was correlated with higher WBC and lower eosinophils, though it was not associated with ESR or Hb. This appears to indicate that latrine use is associated with lower pathogen and parasite exposure, leading to reductions in chronic infection and immune activation. While latrine use was not associated with positive outcomes for all biomarkers, it should be noted that latrines do not protect against exposures to animal feces, unclean water, or soil-transmitted helminths outside of the household. As only 24% of households reported regular latrine use, lower levels of latrine use in other community members may put those who use latrines at risk of exposure to pathogens and parasites. A recent study in Gambia reported that even households with pit latrines restricted access (particularly for children), so even with 100% latrine coverage, it would be reasonable to expect some environmental fecal contamination (Stoller et al., 2011).
Over time, latrines become filled or break down without proper maintenance. Among the Tsimane, it is common to stop using older latrines as they break down. While we did not assess latrine quality, or ask about how many unusable latrines were present, we specifically asked where individuals went to the bathroom most frequently. It is possible that some of the participants may have recently had latrines that were no longer functional at the time of the interview, but this was not assessed.
A similar study in rural Bangladesh found that availability of sanitary facilities such as latrines was associated with positive child health outcomes and reduced under five mortality, controlling for effects of socioeconomic status of the family (Halder & Kabir, 2008). However, there was a strong correlation between socioeconomic status and the availability of adequate latrines in the rural Bangladeshi communities studied, thus exposing children in the lowest socioeconomic quintile to higher rates of illness and mortality (Halder & Kabir, 2008). Tsimane communities are relatively egalitarian, so variance in socioeconomic status may not correlate with latrine use in the same way; in this sample wealth was not associated with latrine controlling for age, sex, distance to town, and education. Yet previous studies among the Tsimane report that individuals with more political influence present more favorable biomarkers of health status (von Rueden et al., 2014).
4.2. Boiling water
Boiling water was not statistically associated with any biomarker of health. The efficacy of boiling water may be compromised by insufficient boiling time, recontamination post boiling, or consuming beverages containing unboiled water outside of the household, findings which have been corroborated by other studies on boiling water efficacy (Firth et al., 2010), as well as studies on the water sources reported by Tsimane men and women (Rosinger & Tanner, 2015). However, other confounding factors could also explain such results; higher rates of exposure to parasites in other daily activities such as interaction with livestock, food processing, or household latrine type would not be impacted by boiling water. Boiling water may not be a viable option for some rural communities, as boiling water costs time, energy, materials, and time that is not always readily available or accessible; such trade-offs could contribute to insufficient boiling times or recontamination (Tumwine, 2005).
Studies on water boiling behavior in rural populations worldwide have noted the inconsistency of implementing boiled water as an effective method to prevent disease. A randomized controlled trial on water boiling and water storage in rural Peru demonstrated that even in communities which had widely accepted and adopted the boiling water, there were no significant reductions in fecal contaminants such as E. coli in drinking water (Heitzinger et al., 2016). Another study on boiling water efficacy in rural Guatemala noted that boiling water significantly improved the quality of the drinking water, but did not altogether remove the risk of waterborne pathogens (Rosa, Miller, & Clasen, 2010). The authors attribute much of the existing risk to recontamination, which is a possible explanation for the results here as well.
4.3. Mosquito net use
Mosquito net use was not significantly associated with any biomarker outcomes. Despite the presence of some mosquito-borne pathogens in lowland Bolivia (eg, endemic Dengue and yellow fever), there is little evidence of malarial risk near San Borja. That said, it is important to note that the majority (85%) of individuals reported using mosquito nets, and so the minimal population variation may have obfuscated any observable associations. In such an environment, mosquito nets might not serve as important a role as the other behaviors under study. Alternatively, mosquito net quality and integrity, or misuse might explain the lack of association between mosquito nets and health outcomes. If mosquito nets with numerous holes are being used, they may not be able to keep out mosquitoes or to prevent disease (Mutuku et al., 2013). Additionally, since most people spend the majority of waking hours outside mosquito nets engaged in physically active subsistence activities, bites could be occurring at other times of day when individuals are not protected by bed nets (Gurven et al., 2016; Gurven, Jaeggi, Kaplan, & Cummings, 2013). While malaria is not a major concern, parasitic diseases like leishmaniasis are common in the area (Eid, San Sebastian, Hurtig, & Goicolea, 2019), and the preferred mosquito nets have tiny holes to help prevent the transmission of leishmania protozoa from small phlebotomine sandflies. Additionally, proper use of mosquito nets can help ensure a better night of sleep, which can have a range of beneficial consequences (Koenker, Loll, Rweyemamu, & Ali, 2013).
In contrast to the results of our study, a comprehensive review on the international efficacy of mosquito net use in malarial endemic regions found that use of a bed net was correlated with at least a 17% lower rate of child mortality compared to those without a net, highlighting the continued validity of nets in those environments (Pryce et al., 2018). That said, a separate study analyzed the effect of long-lasting insecticide treated mosquito nets in nine municipalities in the state of Rondônia, Brazil in a similar ecology to the Tsimane territory and found no relationship between annual parasitic incidence and the introduction of the mosquito nets (Vieira, Basano, Katsuragawa, & Camargo, 2014). These results were attributed to mosquito feeding habits that favored the early evening, when individuals are outside and not protected by the use of a net (Vieira et al., 2014). The contradicting results of the two studies suggest that public health organizations wishing to implement mosquito nets may need to better understand the ecology and behaviors of people and mosquitos before implementing bed net interventions.
4.4. Decision making around health behaviors
The uptake of public health behaviors have additional costs in terms of time, energy, and opportunity costs. Collecting dry firewood to boil water can be a significant burden, as can digging and maintenance of latrines. The Tsimane live in a high mortality environment, and previous studies report that many individuals see health and morbidity as outside of their control; even if they do engage in public health behaviors or seek formal medical treatment in the nearby town of San Borja, they are likely to become ill again (Alami et al., 2018). This combination of costs to enact these public health behaviors, and the perception that health is outside of individual control could potentially explain low uptake of latrines or water boiling.
4.5. Logistical and cost considerations
All the biomarker data reported here were analyzed in a mobile laboratory in the communities where data were collected, and thus did not require a cold chain or extensive instrumentation. While point of care hemoglobin measurements often cost several dollars per sample, other analyses such as a complete blood count require only a microscope, a low cost hemocytomer, a few chemical reagents to stain slides, and the time of a trained and licensed biochemist. As point-of-care medical monitoring devices become more popular and cheaper, monitoring health in low resource settings will become significantly easier. Measuring BMI or skinfolds can give some information about health status, but point-of-care devices can provide more direct evidence of how interventions are impacting health status. Biomarker collection allows researches conducting interventions to see exactly which specific aspects of health or immune function are being impacted by targeted intervention. Such strategies could be beneficial for communities facing specific infection risks that may not be obvious when just collecting anthropometric measurements.
4.6. Limitations
This is a cross sectional study, and thus it is difficult to directly assess causal influences of boiling water, latrine use, and mosquito nets on health status. We included seven control variables that were potentially confounding, but future studies will more fruitfully employ longitudinal measures of public health behavior in order to examine how the uptake or loss of such behaviors impact individual health. The data presented here are also all from adult heads of household, and highly male biased, and thus the results may not generalize to children or other family members. Most water collection is done by women and children, and thus male respondents may be over estimating the proportion of time that water is being boiled (Rosinger, 2018). Children facing trade-offs between growth and immune function may be at particular risk (Blackwell et al., 2017; Urlacher et al., 2018), especially because children are usually bare-foot, and therefore have more direct exposure to soil-transmitted parasites. Future studies will focus on how these behaviors impact child growth and well-being.
All public health behaviors were self-reported, and direct measures of water intake or latrine use were not assessed. Previous studies in other populations suggest that self-reported behavior may overestimate actual behavior—in this case interviewers could see latrines and mosquito nets as they conducted interviews, and thus we have reason to believe that these are likely reliable responses. Latrine depth and distance from the home were not measured, so it is possible that improper latrine construction or use could be confounding the results. Similarly, water boiling times or storage conditions were not assessed, and could provide routes to contamination even if water was brought to a full boil for the recommended time. Additionally, even if individuals have a latrine and always boil water at home, they may come into contact with fecal matter or contaminated water outside of the home. Finally, even perfect mosquito net use and adherence would not prevent all mosquito bites.
While we see no statistical difference between the biomarker profiles of those who reported boiling water, and the profiles of those who do not always boil water, these results may have been confounded by drinking water outside of the home. In a normal day, 96% of Tsimane will drink unprocessed water, either from river, hand pump, well, or through drinking chicha (a fermented manioc/corn/plantain drink) (Rosinger & Tanner, 2015). Approximately half of the daily total water consumption comes from food sources (eg, fruit), but each additional 100 mL of raw water consumed was associated with higher odds of presenting with gastrointestinal distress (Rosinger & Tanner, 2015). Tsimane have significantly higher water intake than industrialized populations, and simultaneously report higher levels of dehydration as measured by urinary specific gravity (Rosinger, 2015; Rosinger & Tanner, 2015). Thus, if individuals are getting additional water outside the home, or if they are drinking chicha in others’ homes, they may be underreporting the amount of unprocessed water exposure, and even if they are boiling all water consumed at home such exposures outside the home could obfuscate the impacts of boiling water within the home.
While we do control for season (wet vs dry season), we do not have data on daily rainfall, and even if such data were available it would be difficult to interpret. It may be that rainfall the day of data collection would have no impact on biomarkers, but rainfall the 2 weeks prior would have a larger effect.
Data are not available on what communities have received public health information from governmental or nongovernmental organizations. Medical staff from the Tsimane Health and Life history project (Gurven, Stieglitz, et al., 2017) and the Tsimane Amazonian Panel Study (Tanner, 2005) have done public and individual level counseling on public health behaviors over the past 15 years. A map of uptake of behaviors (Figure 1) shows variable access and uptake, but which communities have had formal or informal public health campaigns is not known. It is likely that most of such information would have been disseminated following the creation of Catholic Mission Fatima in 1957, the Tsimane Gran Consejo in 1989 and the Tsimane-specific health clinic located on the edge of San Borja near the Evangelical mission headquarters soon after (Huanca, 2000). The 2010 election of Jorge Anez-the first Tsimane mayor of the market town of San Borja (Reyes-García et al., 2014), also may have led to more immunization and information campaigns to a broader range of Tsimane communities, and thus most interventions have likely been a relatively recent occurrence.
4.7. Conclusion
Clean water and industrial sanitation played critical roles in reducing mortality during the epidemiological transition (Barrett, Kuzawa, McDade, & Armelagos, 1998; Omram, 1983). While many people living in cities take this for granted, parasites, and pathogens sicken billions of people per year worldwide, particularly in rural communities with lower access to public health resources. Here we examined sanitation, boiling water, and bed net usage in a traditional subsistence population with high parasite and pathogen exposure. Human evolution occurred in a mosaic of environments, and while no single environment encompasses the entirety of the human evolutionary past, we know that cities are evolutionarily novel; by examining health in nonindustrial populations we can both better understand global human variation, and what conditions may have been like prior to cities and fast food.
While boiling water can have health benefits in rural communities, latrine use had the largest impact on the biomarkers of general inflammation and immune activation stemming from parasite and pathogen exposure. Increased access to latrines in a population can reduce the total disease exposure in a population, but it requires community cooperation and adherence. If all individuals strictly adhered to latrine standards, the relative pathogenic load in untreated water could eventually diminish, potentially further reducing disease risk. Therefore, if more focus could be given to promoting latrine use in rural populations, it could help reduce the burden of helminths and gastrointestinal diseases. In summary, this study suggests that simple collection of easy to measure biomarkers in a field setting has the resolution to assess health differences associated with health promoting behaviors. Public health interventions aimed at improving sanitation may be able to use minimally invasive field collected biomarkers as a population level diagnostic to test their efficacy if measured before and after public health campaigns.
Supplementary Material
ACKNOWLEDGMENTS
We would like to thank the Tsimane participants, the Gran Consejo Tsimane, THLHP staff, and Dr. Megan Jehn. Support for this project came from the National Institutes of Health (NIH)/National Institute on Aging (NIA) grant RF1AG054442–01. JS acknowledges IAST funding from the French National Research Agency (ANR) under grant ANR-17-EURE-0010 (Investissements d’Avenir program).
Funding information
Agence Nationale de la Recherche, Grant/Award Number: ANR-17-EURE-0010; National Institute on Aging, Grant/Award Number: RF1AG054442-01
Footnotes
CONFLICT OF INTEREST
The authors have no conflicts of interest to report.
SUPPORTING INFORMATION
Additional supporting information may be found online in the Supporting Information section at the end of this article.
REFERENCES
- Alami S, Stieglitz J, Kaplan H, & Gurven M (2018). Low perceived control over health is associated with lower treatment uptake in a high mortality population of Bolivian forager-farmers. Social Science & Medicine, 200, 156–165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barrett R, Kuzawa CW, McDade T, & Armelagos GJ (1998). Emerging and re-emerging infectious diseases: The third epidemiologic transition. Annual Review of Anthropology, 27(1), 247–271. [Google Scholar]
- Blackwell AD, Tamayo MA, Beheim B, Trumble BC, Stieglitz J, Hooper PL, … Gurven M (2015). Helminth infection, fecundity, and age of first pregnancy in women. Science, 350(6263), 970–972. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blackwell AD, Trumble BC, Maldonado Suarez I, Stieglitz J, Beheim B, Snodgrass JJ, … Gurven M (2016). Immune function in Amazonian horticulturalists. Annals of Human Biology, 43(4), 1–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blackwell AD, Urlacher SS, Beheim B, von Rueden C, Jaeggi A, Stieglitz J, … Kaplan H (2017). Growth references for Tsimane forager-horticulturalists of the Bolivian Amazon. American Journal of Physical Anthropology, 162(3), 441–461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blackwell AD, Gurven MD, Sugiyama LS, Madimenos FC, Liebert MA, Martin MA, … Snodgrass JJ (2011). Evidence for a peak shift in a humoral response to helminths: Age profiles of IgE in the Shuar of Ecuador, the Tsimane of Bolivia, and the U.S. NHANES. PLoS Neglected Tropical Diseases, 5(6), e1218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carmody RN, Weintraub GS, & Wrangham RW (2011). Energetic consequences of thermal and nonthermal food processing. Proceedings of the National Academy of Sciences, 108(48), 19199–19203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carmody RN, & Wrangham RW (2009). The energetic significance of cooking. Journal of Human Evolution, 57(4), 379–391. [DOI] [PubMed] [Google Scholar]
- Clasen T, Boisson S, Routray P, Torondel B, Bell M, Cumming O, … Odagiri M (2014). Effectiveness of a rural sanitation programme on diarrhoea, soil-transmitted helminth infection, and child malnutrition in Odisha, India: A cluster-randomised trial. The Lancet Global Health, 2(11), e645–e653. [DOI] [PubMed] [Google Scholar]
- Cohen A, & Colford JJM (2017). Effects of boiling drinking water on diarrhea and pathogen-specific infections in low-and middle-income countries: A systematic review and meta-analysis. The American Journal of Tropical Medicine and Hygiene, 97 (5), 1362–1377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Domenica Cappellini M, & Motta I (2015). Anemia in clinical practice—Definition and classification: Does hemoglobin change with aging? Seminars in Hematology, 52(4), 261–269. [DOI] [PubMed] [Google Scholar]
- Eid D, San Sebastian M, Hurtig A-K, & Goicolea I (2019). Leishmaniasis patients’ pilgrimage to access health care in rural Bolivia: A qualitative study using human rights to health approach. BMC International Health and Human Rights, 19(1), 12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Etkin NL (2007). The co-evolution of people, plants, and parasites: Biological and cultural adaptations to malaria. Proceedings of the Nutrition Society, 62(2), 311–317. [DOI] [PubMed] [Google Scholar]
- Firth J, Balraj V, Muliyil J, Roy S, Rani LM, Chandresekhar R, & Kang G (2010). Point-of-use interventions to decrease contamination of drinking water: A randomized, controlled pilot study on efficacy, effectiveness, and acceptability of closed containers, Moringa oleifera, and in-home chlorination in rural South India. The American Journal of Tropical Medicine and Hygiene, 82(5), 759–765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garrow JS, & Webster J (1985). Queteleťs index (W/H2) as a measure of fatness. International Journal of Obesity, 9(2), 147–153. [PubMed] [Google Scholar]
- Gotlib J (2017). World Health Organization-defined eosinophilic disorders: 2017 update on diagnosis, risk stratification, and management. American Journal of Hematology, 92(11), 1243–1259. [DOI] [PubMed] [Google Scholar]
- Gurven M, Fuerstenberg E, Trumble B, Stieglitz J, Beheim B, Davis H, & Kaplan H (2017). Cognitive performance across the life course of Bolivian forager-farmers with limited schooling. Developmental Psychology, 53(1), 160–176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gurven M, Jaeggi AV, Kaplan H, & Cummings D (2013). Physical activity and modernization among Bolivian Amerindians. PLoS One, 8(1), e55679. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gurven M, Stieglitz J, Trumble BC, Blackwell AD, Beheim B, Davis H, … Kaplan H (2017). The Tsimane health and life history project: Integrating anthropology and biomedicine. Evolutionary Anthropology, 26, 54–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gurven MD, Trumble BC, Stieglitz J, Yetish G, Cummings D, Blackwell AD, … Pontzer H (2016). High resting metabolic rate among Amazonian forager-horticulturalists experiencing high pathogen burden. American Journal of Physical Anthropology, 161, 414–425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Halder AK, & Kabir M (2008). Child mortality inequalities and linkage with sanitation facilities in Bangladesh. Journal of Health , Population, and Nutrition, 26(1), 64. [PMC free article] [PubMed] [Google Scholar]
- Heitzinger K, Rocha C, Quick R, Montano S, Tilley D, Mock C, … Hawes S (2016). The challenge of improving boiling: Lessons learned from a randomized controlled trial of water pasteurization and safe storage in Peru. Epidemiology & Infection, 144(10), 2230–2240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Henry AG, Brooks AS, & Piperno DR (2011). Microfossils in calculus demonstrate consumption of plants and cooked foods in Neanderthal diets (Shanidar III, Iraq; spy I and II, Belgium). Proceedings of the National Academy of Sciences, 108(2), 486–491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hotez PJ, Bottazzi ME, Franco-Paredes C, Ault SK, & Periago MR (2008). The neglected tropical diseases of Latin America and the Caribbean: A review of disease burden and distribution and a roadmap for control and elimination. PLoS Neglected Tropical Diseases, 2(9), e300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hruschka DJ, & Hadley C (2016). How much do universal anthropometric standards bias the global monitoring of obesity and undernutrition? Obesity Reviews, 17(11), 1030–1039. [DOI] [PubMed] [Google Scholar]
- Huanca L (2000). Tsimane indigenous knowledge, swidden fallow management and conservation. Florida: University of Florida. [Google Scholar]
- Kaplan H, Thompson RC, Trumble BC, Wann LS, Allam AH, Beheim B, … Thomas GS (2017). Coronary atherosclerosis in indigenous south American Tsimane: A cross-sectional cohort study. Lancet, 389(10080), 1730–1739. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koenker HM, Loll D, Rweyemamu D, & Ali AS (2013). A good nighťs sleep and the habit of net use: Perceptions of risk and reasons for bed net use in Bukoba and Zanzibar. Malaria Journal, 12(1), 203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kraft T, Stieglitz J, Trumble BC, Martin M, Kaplan H, & Gurven M (2018). Nutrition transition in two lowland Bolivian subsistence populations. American Journal of Clinical Nutrition, 108, 1183–1195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mara D, Lane J, Scott B, & Trouba D (2010). Sanitation and health. PLoS Medicine, 7(11), e1000363. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mutuku FM, Khambira M, Bisanzio D, Mungai P, Mwanzo I, Muchiri EM, … Kitron U (2013). Physical condition and maintenance of mosquito bed nets in Kwale County, coastal Kenya. Malaria Journal, 12(1), 46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Omram A (1983). The epidemiologic transition theory. A preliminary update. Journal of Tropical Pediatrics, 29(6), 305–316. [DOI] [PubMed] [Google Scholar]
- Perry GH (2014). Parasites and human evolution. Evolutionary Anthropology: Issues, News, and Reviews, 23(6), 218–228. [DOI] [PubMed] [Google Scholar]
- Pryce J, Richardson M, & Lengeler C (2018). Insecticide-treated nets for preventing malaria. Cochrane Database of Systematic Reviews, 11, 1–66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reyes-García V, Paneque-Gálvez J, Bottazzi P, Luz AC, Gueze M, Macía MJ, … Pacheco P (2014). Indigenous land reconfiguration and fragmented institutions: A historical political ecology of Tsimane’lands (Bolivian Amazon). Journal of Rural Studies, 34, 282–291. [Google Scholar]
- Rook GA (2009). Review series on helminths, immune modulation and the hygiene hypothesis: The broader implications of the hygiene hypothesis. Immunology, 126(1), 3–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rook GAW, Lowry CA, & Raison CL (2013). Microbial ‘old friends’, immunoregulation and stress resilience. Evolution , Medicine, and Public Health, 2013(1), 46–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosa G, Miller L, & Clasen T (2010). Microbiological effectiveness of disinfecting water by boiling in rural Guatemala. The American Journal of Tropical Medicine and Hygiene, 82(3), 473–477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosinger A (2015). Heat and hydration status: Predictors of repeated measures of urine specific gravity among Tsimane’adults in the Bolivian Amazon. American Journal of Physical Anthropology, 158(4), 696–707. [DOI] [PubMed] [Google Scholar]
- Rosinger A, & Tanner S (2015). Water from fruit or the river? Examining hydration strategies and gastrointestinal illness among Tsimane’adults in the Bolivian Amazon. Public Health Nutrition, 18(6), 1098–1108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosinger AY (2018). Household water insecurity after a historic flood: Diarrhea and dehydration in the Bolivian Amazon. Social Science & Medicine, 197, 192–202. [DOI] [PubMed] [Google Scholar]
- Roth GA, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, … Abdelalim A (2018). Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the global burden of disease study 2017. The Lancet, 392 (10159), 1736–1788. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Selendy JM (2011). Water and sanitation-related diseases and the environment: Challenges, interventions, and preventive measures. Hoboken, New Jersey: John Wiley & Sons. [Google Scholar]
- Smith AR, Carmody RN, Dutton RJ, & Wrangham RW (2015). The significance of cooking for early hominin scavenging. Journal of Human Evolution, 84, 62–70. [DOI] [PubMed] [Google Scholar]
- Speth JD (2015). When did humans learn to boil. PaleoAnthropology, 2015, 54–67. [Google Scholar]
- Stieglitz J, Jaeggi AV, Blackwell AD, Trumble BC, Gurven M, and Kaplan H. 2014. Work to live and live to work: Productivity, transfers, and psychological well-being in adulthood and old age. Washington, D.C.: The National Academies Press. [Google Scholar]
- Stieglitz J, Trumble BC, Thompson ME, Blackwell AD, Kaplan H, & Gurven M (2015). Depression as sickness behavior? A test of the host defense hypothesis in a high pathogen population. Brain, Behavior, and Immunity ., 49, 130–139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stoller NE, Gebre T, Ayele B, Zerihun M, Assefa Y, Habte D, … House JI (2011). Efficacy of latrine promotion on emergence of infection with ocular chlamydia trachomatis after mass antibiotic treatment: A cluster-randomized trial. International Health, 3(2), 75–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tanner SN (2005). A population in transition: Health, culture change, and intestinal parasitism among the Tsimane’of lowland Bolivia. University of Michigan. [Google Scholar]
- Teles CBG, Santos APAD, Freitas RA, AFJd O, Ogawa GM, Rodrigues MS, … Camargo LMA (2016). Phlebotomine sandfly (Diptera: Psychodidae) diversity and their Leishmania DNA in a hot spot of American cutaneous Leishmaniasis human cases along the Brazilian border with Peru and Bolivia. Memórias Do Instituto Oswaldo Cruz, 3(7): 423–432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trumble BC, Blackwell AD, Stieglitz J, Thompson ME, Suarez IM, Kaplan H, & Gurven M (2016). Associations between male testosterone and immune function in a pathogenically stressed forager-horticultural population. American Journal of Physical Anthropology, 161(3), 494–505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trumble BC, Smith EA, O’Connor KA, Kaplan HS, & Gurven MD (2014). Successful hunting increases testosterone and cortisol in a subsistence population. Proceedings of the Royal Society B: Biological Sciences, 281(1776), 20132876. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trumble BC, Stieglitz J, Jaeggi AV, Beheim B, Schwartz M, Seabright E, … Gurven M (2018). Parental hormones are associated with crop loss and family sickness following catastrophic flooding in lowland Bolivia. Physiology & Behavior, 193, 101–107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tumwine JK (2005). Clean drinking water for homes in Africa and other less developed countries. Clean drinking water for homes in Africa and other less developed countries. British Medical Journal Publishing Group. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Urlacher SS, Ellison PT, Sugiyama LS, Pontzer H, Eick G, Liebert MA, … Snodgrass JJ (2018). Tradeoffs between immune function and childhood growth among Amazonian forager-horticulturalists. Proceedings of the National Academy of Sciences, 115(17), E3914–E3921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vieira GD, Basano SA, Katsuragawa TH, & Camargo LMA (2014). Insecticide-treated bed nets in Rondônia, Brazil: Evaluation of their impact on malaria control. Revista Do Instituto de Medicina Tropical de São Paulo, 56(6), 493–497. [DOI] [PMC free article] [PubMed] [Google Scholar]
- von Rueden CR, Trumble BC, Emery Thompson M, Stieglitz J, Hooper PL, Blackwell AD, … Gurven M (2014). Political influence associates with cortisol and health among egalitarian forager-farmers. Evolution, Medicine, and Public Health 2014, 2014(1), 122–133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- WHO/UNICEF. 2015. Progress on drinking water and sanitation: 2015 update and MDG assessment. World Health Organization and UNICEF Geneva. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.