

Abstract
BACKGROUND:
Thyrotoxicosis is a common medical problem. Thyroid nuclear imaging with either I123 or technetium-99m (Tc-99m) pertechnetate are used to determine the cause. Although I123 has been the standard technique, Tc-99m pertechnetate is now commonly used, acceptable and easier to perform. The commonly used normal value of Tc-99m pertechnetate is 1–4%, but lower normal values have been reported in different populations.
OBJECTIVE:
Determine normal reference range of Tc-99m pertechne-tate thyroid uptake for thyroid scintigraphy in Saudi Arabia.
DESIGN:
Retrospective, cross-sectional.
SETTING:
Nuclear medicine service at tertiary care center in Riyadh.
PATIENTS AND METHODS:
We used data from biochemically euthyroid patients who underwent a thyroid Tc-99m pertechnetate scan while having parathyroid scintigraphy for hyperparathyroidism between April 2009 to April 2019. Medical records and biochemical thyroid function tests were reviewed and Tc-99m pertechnetate thyroid uptake values were determined for each patient.
MAIN OUTCOME MEASURES:
Thyroid uptake of Tc-99m pertechne-tate in euthyroid patients.
SAMPLE SIZE:
167
RESULTS:
The mean and median uptake of Tc-99m pertechnetate in euthyroid patients were 0.86% and 1.0%, respectively, and the inter-quartile range was 0.0–1.0%. The normal reference range in the study population was 0.2-2%. Thyroid uptake inversely correlated with age in females (r=−0.37, P<.001), males (r=−0.46, P=.001), and for all patients (r=?0.39, P<.0001).
CONCLUSION:
The range for normal thyroid Tc-99m pertechnetate was lower than the standard 1-4% range. Moreover, uptake decreased with age. Further studies are needed to establish the normal age-adjusted uptake for the thyroid Tc-99m pertechnetate scan.
LIMITATIONS:
Single center and retrospective.
CONFLICT OF INTEREST:
None.
INTRODUCTION
Thyrotoxicosis is a common condition mostly affecting women. Common causes of thyrotoxicosis include overproduction of thyroid hormones as in Graves’ disease, toxic multinodular goiter or toxic adenoma. Transient thyrotoxicosis due to excessive release of thyroid hormone from an inflamed thyroid gland due to thyroiditis is an important self-limiting differential diagnosis. Thyroid function tests (serum thyroid-stimulating hormone, thyroxine [T4] and triiodothyronine [T3]) with serology for thyroid antibodies help to determine the cause in most cases. However, most patients will likely need nuclear scanning to determine the cause more accurately and to guide treatment options. Thyroid nuclear imaging commonly includes a thyroid scan with uptake using either I123 or technetium-99m (Tc-99m) pertechnetate.1
Thyroid uptake and scanning is a diagnostic imaging study that allows the physician to determine the functioning status of the thyroid gland. Different causes of thyrotoxicosis have specific imaging findings. In addition to images, thyroid uptake (a quantitative measure of thyroid function), is often provided. Thyroid uptake is the percentage of the radioactive dose lodged in the thyroid gland at a standard time. This information is useful in deciding the treatment option as well as the dose of I131 for treatment of hyperthyroidism causes when indicated.2 The I123 thyroid scan and uptake has been a standard procedure for several decades. The uptake of this radiotracer is physiological. After entering the thyroid gland, it binds to the amino acid tyrosine, and is incorporated into thyroid hormones. Thyroid scintigraphy using radioactive Tc-99m pertechnetate has become an accepted alternative to I123 scan due to its superior qualities such as availability, short duration of the procedure, lower cost and radiation dose. This radiotracer follows the same pathway to enter the thyroid gland as I123. However, Tc-99m pertechnetate does not organify like I123.3,4
Thyroid uptake with Tc-99m is measured at 20 minutes after injection as by this time the level of tracer up-take reaches a plateau.5 A small percentage of Tc-99m pertechnetate is seen in the thyroid gland at this time, usually 1–4%.6 Researchers have reported different normal ranges in different geographical regions and different populations. The normal ranges for thyroid uptake in euthyroid patients vary within different geographical areas.7 Moreover, uptake is affected by other factors like medications, different hormones and conditions such as pregnancy.8,9 Also, fluctuation of the normal value of Tc-99m pertechnetate over time has been reported. Blum and Chandra found that normal thyroid uptake had changed twice over a period of 20 years.10 Therefore, it is important to periodically re-establish reference ranges of thyroid uptake for each demographic area and population. This is necessary to ensure that the sensitivity of this diagnostic test is high in patients with thyrotoxicosis.
PATIENTS AND METHODS
This retrospective cross-sectional study was conducted at the nuclear medicine service at King Abdulaziz Medical City (KAMC) in Riyadh between April 2009 and April 2019. We identified all patients of Saudi nationality that underwent Tc-99m sestamibi scintigraphy. KAMC provides all levels of care for patients from all over Saudi Arabia. Patients who also had thyroid imaging with Tc-99m pertechnetate as part of dual-tracer subtraction parathyroid scintigraphy for hyperparathyroidism were reviewed. All patients in the study underwent 99-mTc scanning for investigation of primary hyperparathyroidism. None had secondary or tertiary hyperparathyroidism. Inclusion was based on the following criteria: (1) a thyroid scan was done within 3 weeks of parathyroid scintigraphy; (2) patients had undergone a Tc-99m thyroid uptake scan; (3) patients were biochemically euthyroid for 12 months before scanning; and (4) clinically euthyroid after the uptake scan. Exclusion criteria were a history of thyroid or use of antithyroid medication, iodinated contrast or radio-nuclide administration within 6 months of thyroid scanning, and previous thyroid surgery or radioiodine treatment. Patients data was obtained from a search of the electronic medical records at KAMC. We gathered demographic data, thyroid function test results for a year before the thyroid scan, the clinical history of thyroid diseases, surgery or medication and findings on thyroid scintigraphy.
The procedure for determining thyroid uptake first involved measuring the Tc-99m pertechnetate dose in the dose calibrator. Then Syringe radioactivity before injection, immediately after injection and exact injection time was noted in all cases. The imaging was performed by the standard thyroid scan protocol at about 20 minutes after the administration of 5 mCi of Tc-99m pertechnetate. A 20% energy window was centered at 140keV. The details are described at: https://humanhealth.iaea.org/HHW/NuclearMedicine/Endocrinology/GuidelinesandLiterature/SNMEndocr/SNM_-_Thyroid_Scintigraphy.pdf. All patients were asked to drink water immediately before imaging to clear any Tc-99m pertechnetate labelled saliva from the esophagus. Images of the neck were performed using a pinhole collimator in anterior, left anterior oblique and right anterior oblique projections 5 centimeters from the neck. All anterior views were collected for a preset time of 300 seconds. The thyroid uptake was calculated at anterior neck as 20-minute images. The net dose was calculated as the pre-injection syringe activity minus the residual activity in an empty syringe. The net dose and times of measurement were recorded for calculation of the thyroid uptake measurement. Uptake was calculated automatically by the nuclear scan software using the formula:
% uptake = [(thyroid count - background count)/(pre-injection syringe count-post injection syringe count)] × 100%
(All the counts are corrected for the decay of Tc 99m pertechnetate and acquisition time).
The statistical analyses were done using statistical software SAS version 9.4 (SAS Institute Inc., Cary, North Carolina, United States) and R programming language tools (beeswarm and ggplot2 packages) (https://www.r-project.org/). Descriptive statistics for continuous and categorical variables were expressed as mean and standard deviation as well as median, interquartile range and percentage (%). Normality of the distribution of continuous covariates was checked using the Shapiro-Wilk test and quantile-quantile plots. Group comparisons were done using parametric and nonpara-metric tests, and the statistical significance level alpha (α<0.05) was assumed. For assessment of correlation between variables, the Pearson or Spearman correlation tests were used depending on the distribution of the data.
RESULTS
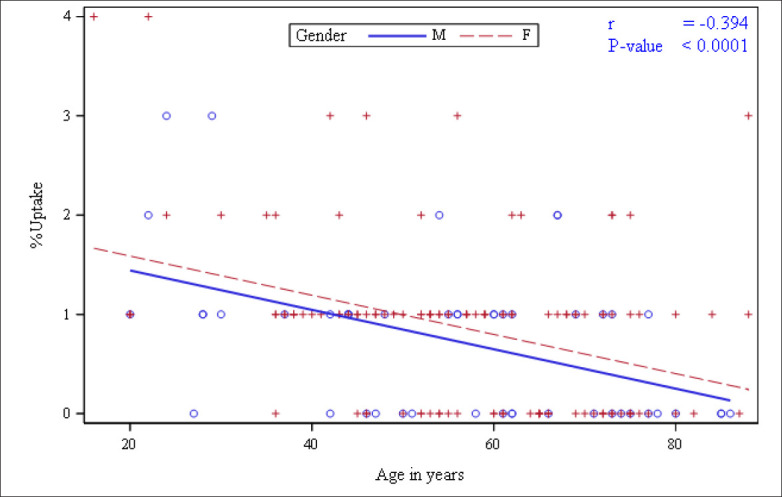
Of 650 patient records, 167 met inclusion criteria (Table 1). Percent uptake and uptake distribution are shown in Table 1 and Figure 1. The percent uptake distributions were normally distributed after log transformation. There was a negative correlation between percent uptake of Tc-99m pertechnetate and age (r= −0.39; P<.0001) (Figure 2). The correlations between the age in male and female subjects were statistically significant (r=−0.46; P=.001) and (r=−0.37; P<.001, respectively) (Figures 3 and 4). A cumulative frequency curve indicated a normal reference range of 0.2–2.0% for the study population (Figure 5).
Table 1.
Thyroid-stimulating hormone (TSH) levels and uptake in the study population.
| Age Median (IQR) | TSH Median (IQR) | Uptake Median (IQR) | |
|---|---|---|---|
| Overall | 57 (45–70) | 1.82 (1.20–2.60) | 0.67 (0.39–1.18) |
| Gender | |||
| Male | 59 (44–71.5) | 1.82 (1.2–2.32) | 0.54 (0.31–0.95) |
| Female | 57 (45–69) | 1.82 (1.15–2.74) | 0.68 (0.42–1.20) |
Figure 1. Distribution of 99mTc pertechnetate uptake in the study group by sex (n=167).
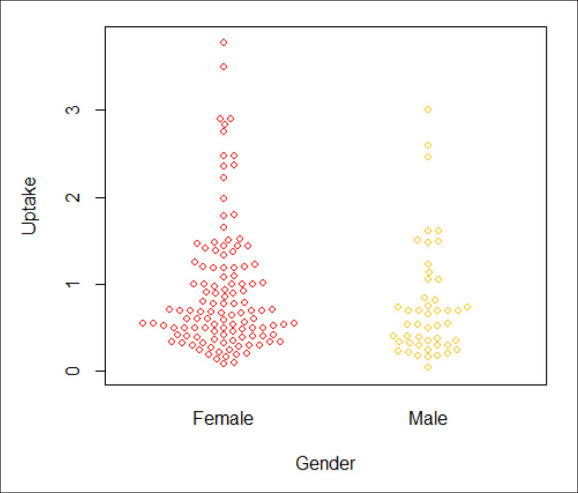
Figure 3. Relationship between 99mTc pertechnetate uptake and age in males.
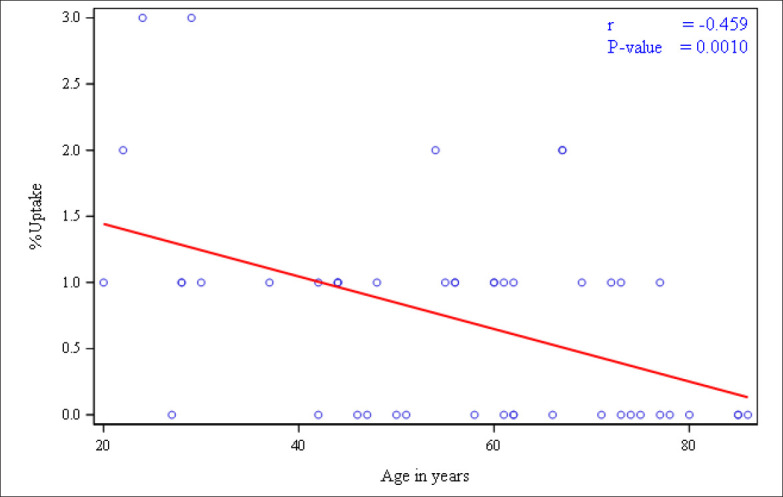
Figure 4. Relationship between 99mTc pertechnetate uptake and age in all females.
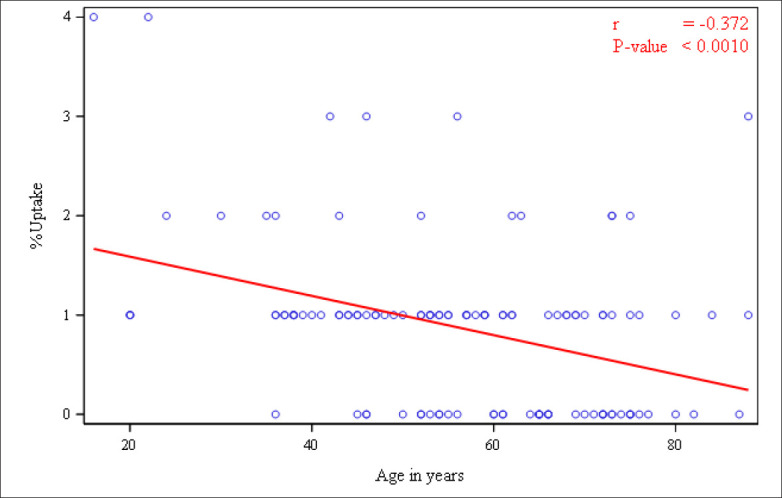
Figure 5. The cumulative frequency of 99mTc pertechnetate uptake.
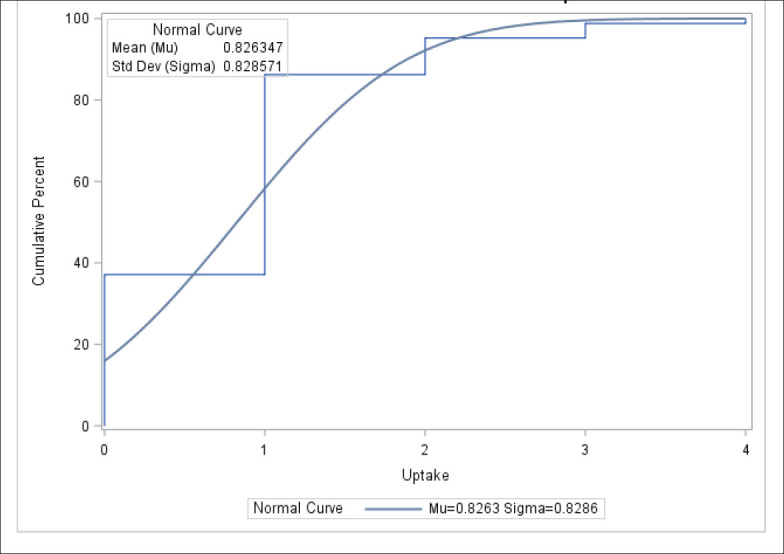
Figure 2. Relationship between 99mTc pertechnetate uptake and age in all patients.
DISCUSSION
This study assessed the normal values for thyroid Tc-99m pertechnetate uptake in a Saudi population who were clinically and biochemically euthyroid. The normal reference range for Tc-99m pertechnetate uptake used by our institute and many others in the Middle East and the world is 0–4.0%, which is relatively wide. In this study, the normal Tc-99m pertechnetate uptake reference range was calculated as 0.2–2.0%. Both the upper and the lower range limits are lower than the standard range. These findings are similar to the recently reported data from other regions outside the Middle East. Published geographical location-specific normal reference ranges for thyroid uptake of Tc-99m pertechnetate are rare and vary significantly.11,12 The most recently published ranges are as follows: Ramos et al (0.4–1.7%) from Brazil, Hamunyela et al (0.15–1.69%) from Namibia, and Macauleya et al (0.5–1.4%) from the UK.11,13,14 To our knowledge there are no published reports of normal reference values for thyroid Tc-99m pertechnetate uptake from institutions in Saudi Arabia or the Middle East. This study was an attempt to evaluate the normal values of Tc-99m pertechnetate in the Saudi population. Moreover, in this study it was evident that Tc-99m pertechnetate uptake changes with age as the uptake decreased with older age. As Tc-99m pertechnetate uptake is commonly used in investigating patients with thyrotoxicosis, it is of paramount importance to establish the normal values for this diagnostic test. The accuracy of the test has major implications in clinical practice as it guides diagnosis and management of patients with thyrotoxicosis.
Tc-99m pertechnetate is becoming the radiotracer of choice in patients with thyrotoxicosis. When compared to 123I, Tc-99m pertechnetate tracer is relatively cheap, has a low radiation dose and the result of the test is obtained in one visit.3,4 This study finding of a narrow reference value for thyroid Tc-99m pertechne-tate uptake is of clinical significance in patients with thyroid disorders. In previous studies, the sensitivity and specificity of Tc-99m pertechnetate uptake at these lower reference values were 92–97% and 87-97%, respectively.15,16 Further studies to determine the sensitivity and specificity of these new reference normal values in our population are needed.
Despite being retrospective and an indirect assessment of thyroid Tc-99m pertechnetate uptake, our study sheds light on the importance of determining diagnostic test accuracy for every population and stresses the need to avoid the use of common general reference values. Future work should ideally look at establishing an age-corrected normal thyroid Tc-99m pertechnetate uptake range given the statistically significant age variation in this study. A prospective multicenter study is needed to further confirm the normal values of this test in the Saudi population. However, ethical approval for a prospective study and informed consent could be a challenge due to the administration of radioactive material. Moreover, future research to determine the impact of diet and commonly used medications that might interfere with Tc-99m pertechnetate results are needed. We recommend periodic location-specific revalidation of normal reference values of Tc-99m pertechnetate up-take to maintain quality assurance with this important and commonly used diagnostic test. The study suggests that the current thyroid Tc-99m pertechnetate up-take reference range used in our institution and many other centers in the region may not be accurate. This study documents lower than normal thyroid uptake values for technetium-99m pertechnetate in Saudi Arabia. It is recommended that these new reference values be used for the population in Saudi Arabia.
Funding Statement
None.
REFERENCES
- 1.Ross DS, Burch HB, Cooper DS, Greenlee MC, Laurberg P, Maia AL, Rivkees SA, Samuels M, Sosa JA, Stan MN. 2016 american thyroid association guidelines for diagnosis and management of hyperthyroidism and other causes of thyrotoxicosis. Thyroid [Internet]. 2016;26(10):1343-421. [DOI] [PubMed] [Google Scholar]
- 2.Iqbal A, Rehman A. Thyroid Uptake and Scan. [Updated 2020 Oct 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021. Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK555978/. [PubMed] [Google Scholar]
- 3.Kusić Z, Becker DV, Saenger EL, Paras P, Gartside P, Wessler T, Spaventi S. Comparison of technetium-99m and iodine-123 imaging of thyroid nodules: Correlation with pathologic findings. J Nucl Med [Internet]. 1990. Apr;31(4):393–9. [PubMed] [Google Scholar]
- 4.Giovanella L, Avram AM, Iakovou I, Kwak J, Lawson SA, Lulaj E, Luster M, Piccardo A, Schmidt M, Tulchinsky M. EANM practice guideline/SNMMI procedure standard for RAIU and thyroid scintigraphy. European journal of nuclear medicine and molecular imaging [Internet]. 2019;46(12):2514-25. [DOI] [PubMed] [Google Scholar]
- 5.Smith JJ, Croft BY, Brookeman VA, Teates CD. Estimation of 24-hour thyroid uptake of I-131 sodium iodide using a 5-minute uptake of technetium-99m pertechnetate. Clin Nucl Med [Internet]. 1990. Feb;15(2):80-3. [DOI] [PubMed] [Google Scholar]
- 6.Atkins HL. Technetium-99m pertechnetate uptake and scanning in the evaluation of thyroid function. In: Seminars in nuclear medicine [Internet] 1971 Elsevier. 1971;345-55. [DOI] [PubMed]
- 7.Nelson JC, Renschler A, Dowswell JW. The normal thyroidal uptake of iodine. Calif Med [Internet]. 1970. Jun;112(6):11-4. [PMC free article] [PubMed] [Google Scholar]
- 8.STANLEY MM, Astwood EB. The response of the thyroid gland in normal human subjects to the administration of thyrotropin, as shown by studies with I131. Endocrinology [Internet]. 1949;44(1):49-60. [DOI] [PubMed] [Google Scholar]
- 9.Kearns JE, Philipsborn Jr HF. Values for thyroid uptake of I-131 and protein-bound iodine in” normal” individuals from birth to twenty years. Quarterly Bulletin of the Northwestern University Medical School [Internet]. 1962;36(1):47. [PMC free article] [PubMed] [Google Scholar]
- 10.Blum M, Chandra R. Lower normal values for 131I thyroid uptake not related to the ingestion of white bread. Journal of Nuclear Medicine [Internet]. 1971;12(11):743-5. [PubMed] [Google Scholar]
- 11.Anjos DA, Etchebehere EC, Santos AO, Lima MC, Ramos CD, Paula RB, Camargo EE. Normal values of [99mTc] pertechnetate uptake and excretion fraction by major salivary glands. Nucl Med Commun [Internet]. 2006;27(4):395-403. [DOI] [PubMed] [Google Scholar]
- 12.Ramos CD, Wittmann DEZ, Etchebe-here, Elba Cristina Sá de Camargo, Tambascia MA, Silva CAM, Camargo EE. Thyroid uptake and scintigraphy using 99mTc pertechnetate: Standardization in normal individuals. Sao Paulo Medical Journal [Internet]. 2002;120(2):45-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hamunyela RH, Kotze T, Philotheou GM. Normal reference values for thyroid uptake of technetium-99m pertechnetate for the namibian population. Journal of Endocrinology, Metabolism and Diabetes of South Africa [Internet]. 2013;18(3):142-7. [Google Scholar]
- 14.Macauley M, Shawgi M, Ali T, Curry A, Howe K, Howell E, Jefferson E, James A, Perros P, Petrides GS. Assessment of normal reference values for thyroid uptake of technetium-99m pertechnetate in a single centre UK population. Nucl Med Commun [Internet]. 2018;39(9):834-8. [DOI] [PubMed] [Google Scholar]
- 15.Uchida T, Suzuki R, Kasai T, Onose H, Komiya K, Goto H, Takeno K, Ishii S, Sato J, Honda A. Cutoff value of thyroid uptake of 99mTc-pertechnetate to discriminate between graves’ disease and painless thyroiditis: A single center retrospective study. Endocr J [Internet]. 2015:EJ15-0441. [DOI] [PubMed]
- 16.Fadime D. Cut off value of technetium uptake in the differential diagnosis of graves, disease and subacute thyroiditis. Asia Oceania Journal of Nuclear Medicine and Biology [Internet]. 2020;8(1):54. [DOI] [PMC free article] [PubMed] [Google Scholar]