

Abstract
Some research suggests that compared with younger adults, older adults have more homogeneous, less diverse daily life experiences because everyday situations and activities become increasingly stable and routine. However, strong empirical tests of this assumption are scarce. In two complementary studies, we examined whether older age is associated with less diversity in daily life experiences (e.g., regarding social interaction partners, activities, and places across and within days) and, if so, to what extent health limitations account for these age differences. In Study 1, we used daily diaries to investigate diversity across days among younger (N = 246; Mage = 21.8 years, SD = 2.5) and older adults (N = 119; Mage = 67.7 years, SD = 5.3). In Study 2, we investigated diversity within days employing experience sampling methods over three weeks in an adult life span sample (N = 365; range = 14–88 years). Results showed that across and within days, the daily lives of older adults were less diverse regarding their social interaction partners. Yet, older adults reported more diversity in activities within days and across days in the afternoons, whereas younger adults reported less diverse activities partly due to working or studying more often. Age differences remained statistically significant when controlling for health limitations. We conclude that age differences in the diversity of daily life are nuanced, depending on the domain and the level of analysis.
Keywords: diversity of daily situations, life span, health, everyday life, experience sampling method
For some people, daily life can be highly diverse with many different activities and social partners both during the day (e.g., morning vs. afternoon), and across days of the week. Other people might follow routines more consistently and experience more homogeneous days. The daily life people pursue is often a mixture of selecting activities that meet one’s interests, needs, and constraints (M. M. Baltes, Wahl, & Schmid-Furstoss, 1990; Carstensen, Isaacowitz, & Charles, 1999; Wrzus, Wagner, & Riediger, 2016) as well as fulfilling (societal) expectations related to developmental tasks regarding working and parenting roles (Havighurst, 1974; Hutteman, Hennecke, Orth, Reitz, & Specht, 2014). During young adulthood, developmental tasks are mainly concerned with exploring and mastering new tasks and roles (Arnett, 2000; P. B. Baltes, 1987; Havighurst, 1974; Hutteman et al., 2014). In contrast, later in adulthood, social roles (e.g., as a partner, parent, or employee) and environments (e.g., place of residence, workplace) are often more established (Hutteman et al., 2014), offering and demanding less diverse daily lives. With further advancing age, elective selectivity (i.e., purposeful restriction to specific goals given the increasingly limited resource capacity, e.g., Riediger, Li, & Lindenberger, 2006) as well as lossbased selectivity in reaction to aging-related impairments in mobility or physical health, can also narrow daily activities including social life (P. B. Baltes, 1987; M. M. Baltes et al., 1990; Paillard-Borg, Wang, Winblad, & Fratiglioni, 2009).
In two studies, ranging across three weeks to six months, we examined whether the diversity of people’s daily lives differed across adulthood from 18 years to old age up to around 80 years. Diversity of everyday life refers to the experience of varying situations during or across days (e.g., different social contacts or activities). The term diversity is used synonymously with variety of different categories of a phenomenon (Benson, Ram, Almeida, Zautra, & Ong, 2018), whereas variability often refers to fluctuating intensity in single states over time such as positive mood or extraverted behavior (Benson et al., 2018; Fleeson & Gallagher, 2009; Kuppens, Oravecz, & Tuerlinckx, 2010). For example, an adult who engages mainly in one activity during the day (e.g., studying or working) experiences less diversity during this day than an adult who engages in several different activities and thus situations. At the same time, diversity can be both adaptive and maladaptive: Too much homogeneity often elicits boredom, whereas too much variety can be taxing and establishing daily routines can help to conserve personal resources (Cloninger, 1987; González-Cutre, Sicilia, Sierra, Ferriz, & Hagger, 2016).
Psychology has long acknowledged the importance of situations in shaping human behavior and development (e.g., P. B. Baltes, 1987; Funder, 2016; Lewin, 1939; Magnusson, 1981; Wahl & Gerstorf, 2018). Previous research has primarily focused on the frequency of specific situations (e.g., M. M. Baltes et al., 1990; Wrzus et al., 2016), but not on the diversity across situation types. Such a variable-centered approach, that is, examining the frequency people engage in specific activities, for example, hours or percentage working, hours or percentage religious activities (e.g., Curtis, Windsor, Mogle, & Bielak, 2017; Kahneman, Krueger, Schkade, Schwarz, & Stone, 2004), addresses a very different question compared with examining diversity across several variables, that is, the composition of activities within the day or within the week of a person. In addition, research in other areas such as affective variability or control diversity has shown that indices of diversity uniquely predict mental and physical health over and above mean levels (e.g., Benson et al., 2018; Drewelies, Koffer, Ram, Almeida, & Gerstorf, 2019; Kuppens et al., 2012).
Knowledge on age-related differences in the diversity of people’s daily lives would be valuable for multiple areas of research and practical application. These areas include age differences, for example, in situational influences on goal pursuit (e.g., Riediger & Freund, 2008), in person-situation interactions (e.g., Wrzus et al., 2016), and generally in the role of environmental influences on social, cognitive, or personality development (e.g., Caspi, Roberts, & Shiner, 2005; Hertzog, Kramer, Wilson, & Lindenberger, 2008; Wahl & Gerstorf, 2018; Wrzus & Roberts, 2017). Such studies often examine the entire adult life span. Accordingly, the current study also examines the adult life span development instead of focusing solely on old age. In addition to examining diversity across the adult life span, we furthermore test whether health limitations may contribute to, or moderate, age differences in daily life diversity because health limitations can impede, for example, the engagement in social activities (M. M. Baltes et al., 1990; Curtis et al., 2017; Lee et al., 2018). Next, we describe age differences in the diversity of daily life, before addressing how health limitations may contribute to them.
Age Differences in the Diversity of Daily Life
During young adulthood, developmental tasks are mainly concerned with exploring and mastering several new roles and tasks, such as developing committed romantic partnerships, establishing a family, and pursuing work-related goals (Havighurst, 1974; Hutteman et al., 2014). Typically, young adults are not settled yet in terms of long-lasting partnerships, jobs, or residence. Therefore, diverse daily situations may result from these tasks and may be necessary to accomplish them. In addition, physical capacity is at its peak in young adulthood, enabling young adults to actively seek and deal with multiple and fluctuating situations (Baltes, 1987).
Throughout middle adulthood, maintaining a satisfying occupation and social relationships with one’s spouse, family, and friends as well as seeking stability through established pathways are central developmental tasks (P. B. Baltes, 1997; Havighurst, 1974). For older adults, occupational and family related demands may be less frequent, yet health-related and social losses may become more prevalent (P. B. Baltes, 1987, 1997; Havighurst, 1974). These losses might constrain the possibilities of older adults to create or seek diverse situations, so that their daily lives may become more stable. In addition, with older age, adults might purposely focus on certain activities and people to concentrate resources (i.e., elective selection, Luong, Rauers, & Fingerman, 2015). Research supports these interpretations as older adults spend much of their time alone or with the same set of partners, such as their spouse or family members (M. M. Baltes et al., 1990; Horgas, Wilms, & Baltes, 1998; Wrzus et al., 2016).
Two different aspects characterize the majority of diversity of daily life across adulthood: engagement in different activities (i.e., what people are doing) and interactions with different social partners (i.e., with whom time is spent; e.g., Magnusson, 1981; Rauthmann, 2015; Saucier, Bel-Bahar, & Fernandez, 2007). Although there can be some overlap between activities and social partners (e.g., social interactions can be one specific domain of activities and some activities are inherently social), many different activities can be pursued alone or with distinct social partners (e.g., leisure or work activities alone or with others, respectively). Thus, diversity of activities and of social partners are theoretically and also likely empirically distinct. We furthermore focus on activities and interactions with others because people have some agency in selecting and influencing these domains directly (Buss, 1987)—contrary to larger geographic, political, or societal conditions.
Daily Activities
Daily life can consist of many different activities such as working, doing chores, participating in leisure activities, socializing, or sleeping (e.g., Kahneman et al., 2004; Parisi, 2010). Previous research has mainly focused on age differences in the engagement in specific activities (e.g., hours spent doing certain activities; M. M. Baltes et al., 1990; Paillard-Borg et al., 2009), whereas everyday diversity of activities has been examined less frequently. As an exception, it has been observed that the pursuit of novel leisure activities was lower with older age (e.g., exploring new hobbies), whereas the longing to maintain stability through regular and familiar leisure activities was higher in older age compared with younger adults (Iso-Ahola, Jackson, & Dunn, 1994).
Correspondingly, involvement in various types of activities (e.g., regularly engaging in mental activities like reading as well as in physical activities like swimming) decreases with older age (Paillard-Borg et al., 2009). Older adults may have fewer possibilities to engage in diverse leisure activities because the amount of time spent with obligatory activities (e.g., self-care, housework) is higher compared with leisure activities in later adulthood (M. M. Baltes et al., 1990; Paillard-Borg et al., 2009). In line with this argument, the frequency of participation in leisure activities decreases with age (Gordon, Gaitz, & Scott, 1976) and older people spend more time resting (Horgas et al., 1998).
However, many previous studies have relied on generalized, retrospective reports of daily activities, which elicits the criticism that older adults might remember or report their daily activities with less specificity than younger adults, which in turn would lead to reports of more homogeneous activities with age. In fact, when using ambulatory (momentary) assessments of activities in daily life, studies show that young adults do not report engaging in more heterogeneous activities during the day than do older adults (Lee et al., 2018; Wrzus et al., 2016). Similarly, diversity of activities during one recalled day did not vary between young-old (age range = 60–75 years) and old-old (age range = 75–92 years) adults (Parisi, 2010). Together, these results suggest that retrospective biases over longer recall periods may influence the types of results obtained regarding age differences in diversity of daily life.
Another methodological issue to consider is that in experience sampling or daily diary studies, the specificity with which activities are assessed or categorized by people can affect conclusions regarding the diversity of activities. That is, the chosen unit-of-analysis is relevant, for example, whether the participants or the researchers distinguish shopping, doing laundry, or preparing meals or combine the activities into household chores. We readdress this issue and explain the choice for the current studies in The Present Studies section.
Daily Social Partners
Socioemotional selectivity theory (Carstensen, 1995; Carstensen et al., 1999) posits that with advancing age, people increasingly start to perceive their future as limited and consequently focus more on short-term goals, such as emotional gratification and social harmony. These changes lead to a stronger focus on cultivating close relationships and thus to a reduced network size due to pruning less close partners from the network (Carstensen, 1995). Previous research has shown that younger and older adults differ significantly regarding their social environments: Older adults have smaller social networks (Wrzus, Hänel, Wagner, & Neyer, 2013), less social contact (Cornwell, 2011), especially with friends, neighbors, and other acquaintances (Sander, Schupp, & Richter, 2017), and adopt fewer unique social roles in their daily life (Altergott, 1990). In their everyday life, older adults spend much time alone and mostly interact with close relatives, such as with a spouse or family members (M. M. Baltes et al., 1990; Horgas et al., 1998; Wrzus et al., 2016). In contrast, diverse peer relationships are most important during young adulthood (Reitz, Zimmermann, Hutteman, Specht, & Neyer, 2014). A study using ambulatory assessments in daily life showed that younger adults typically interacted with more diverse partners during the day than older adults (Wrzus et al., 2016).
Social network size and social contact decrease from young to middle adulthood (Sander et al., 2017; Wrzus et al., 2013), while emotional closeness with a selected few is maintained or actually enhanced (Carstensen, 1992). Even in very old age, emotionally close relationships are maintained, offering opportunities to interact with diverse people. At the same time, the majority of more distant relationships are reduced (Lang & Carstensen, 1994), thus limiting the overall pool of available interaction partners (e.g., Wrzus et al., 2013). As a consequence, the possibility to interact with different social partners on a daily basis may be reduced for older adults and could lead to less diversity in social contacts.
Health and the Diversity of Daily Life
Some studies suggest that a person’s physical health and functional capacities, which decrease across adulthood, may influence personal opportunities and create barriers in daily life (M. M. Baltes et al., 1990; Curtis et al., 2017; Horgas et al., 1998; Paillard-Borg et al., 2009). People who suffer from physical or cognitive constraints often find themselves faced by many impairments, such as reduced energy levels or limited out-of-home mobility (Janke, Davey, & Kleiber, 2006; Lindesay & Thompson, 1993; Rosso, Taylor, Tabb, & Michael, 2013). Indeed, social vitality, that is, social participation, starts declining among many people in midlife (Reitz & Staudinger, 2017). Accordingly, individual health limitations might impede a diverse lifestyle, as people who suffer from physical constraints might be less mobile, adaptable, or energetic, which are capacities that would facilitate a diverse lifestyle. We therefore investigated how individual differences in health limitations might account for age differences in the diversity of daily life and how health limitations might differentially impede daily life diversity (i.e., activities and social partners) differently in older age compared with younger adulthood. Again, we focus on the engagement in diverse activities and the diverse involvement with other persons (i.e., social partners).
Daily Activities
Multiple studies have consistently shown that better health is positively associated with general activity engagement and the frequency of participation in leisure activities (M. M. Baltes et al., 1990; Garfein & Herzog, 1995; Janke et al., 2006; Lefrancois, Leclerc, & Poulin, 1997; McGuire, Dottavio, & O’Leary, 1986; Menec, 2003; Paillard-Borg et al., 2009; Seale & Iso-Ahola, 1988). For example, lower functional health was associated with fewer physical and religious activities, but with more resting and obligatory activities such as medical treatments (M. M. Baltes et al., 1990) and chores (Garfein & Herzog, 1995). Two studies with older adults showed that physical functioning was significantly associated with the engagement in specific activities (Garfein & Herzog, 1995; Paillard-Borg et al., 2009): Physical limitations were associated with not only less participation in physical activities, but also in mental activities (e.g., reading; Paillard-Borg et al., 2009). In contrast, one recent study with adults aged 50 to 84 years (Curtis et al., 2017) observed no associations between average health (i.e., physical symptoms, amount of daily pain) and physical or mental activities, and even reported higher social and mental activities on days with more intense symptoms or pain. However, the overall level of symptoms and pain was very low, which suggests that somewhat increased levels of physical symptoms might not have impeded daily life. Overall, pronounced health limitations seem to relate to fewer opportunities to shape one’s daily life and to pursue different leisure activities.
Daily Social Partners
Good health is associated with more frequent social activities and interactions—both in the general population (Lee, Jang, Lee, Cho, & Park, 2008) and especially among older adults (M. M. Baltes et al., 1990; Curtis et al., 2017; Menec, 2003; Rosso et al., 2013). In addition, social isolation is more common among physically disabled women aged 65 and older (Simonsick, Kasper, & Phillips, 1998). In a typical week, 23% of socially isolated women do not interact at all with friends or relatives, a trend that gets more pronounced for the most severely disabled. Thus, healthier adults generally experience more diverse social involvement, and this applies specifically for older adults (Curtis et al., 2017; Menec, 2003; Rosso et al., 2013). It is possible that younger adults have greater compensatory means compared with older adults, so for them health limitations will compromise social involvement less (Curtis et al., 2017).
The Present Studies
The question of whether older adults have a less diverse, more homogeneous daily life compared with younger adults has not been addressed adequately in most previous studies due to two shortcomings. First, many previous studies used retrospective questionnaires regarding which activities and social partners people generally engage in. Such questionnaires might be more prone to age-specific recall and reporting biases compared with end-of-day or experience sampling reports (e.g., Robinson & Clore, 2002; Schwarz, Park, Knäuper, & Sudman, 1999). Second, most of these studies investigated the absolute amount of engagement in certain activities or with specific people, yet they did not examine the unique role of daily life diversity, that is, engagement in different activities or social interactions. Research on other domains (e.g., emotion, self-control) demonstrated the additional contribution of diversity indices in predicting mental and physical health over and above mean levels (e.g., Benson et al., 2018; Drewelies et al., 2019; Kuppens et al., 2012). Using two complementary data sets, we address previous limitations by examining age differences in participants’ daily life diversity both within and across days.
The objectives of the present studies were (a) to investigate whether age and health limitations are significant predictors of diversity in different domains of daily life (i.e., daily activities, social partners, places only in Study 2) and (b) to test whether age moderates the association between health limitations and diversity of daily life. We quantified the diversity of daily life with respect to daily activities, social partners, and places (addressed in Study 2) because these domains are meaningful and often used to describe daily situations (Rauthmann et al., 2014; Saucier et al., 2007). With respect to the specific categories of activities, social partners or places, we chose categories that (a) were applicable for the age range from young adults to old age, (b) were validated and frequently used in experience sampling studies (e.g., Rauthmann et al., 2014; Riediger & Freund, 2008; Sonnenberg et al., 2012), and (c) captured the majority of daily situations while keeping the number of categories manageable for daily life assessments (as indicated by the low occurrence of selecting “other” options in previous studies using the same categories; Wrzus et al., 2016).
Study 1 employed a daily diary approach with three periods of daily assessments on 10 consecutive evenings each. This study allowed us to examine diversity across days, which enabled us to cover a longer time span of several weeks and months. Study 2 used an experience sampling method with multiple assessments per day occurring on several days, which allowed for studying diversity within days. Thus, we were able to study diversity on a more fine-grained scale. Within-days and across-days diversity are theoretically distinct because people can engage in quite diverse activities during the day with many different people and in different places, but days might be highly similar (i.e., high within-day diversity, low across-day diversity) or vice versa. Examining both types of diversity allows us to thoroughly investigate age- and health-related differences in daily diversity. Thus, based on the aforementioned literature, we formulated the hypotheses presented in the following text.
Hypothesis 1 predicts that older age is associated with less daily life diversity regarding activities and social interaction partners, both in number and in kind. Given that older age is associated with impaired health, Hypothesis 2 predicts that individual differences in health will partly account for age differences in the diversity of daily life. We further assumed (Hypothesis 3) that it might be possible for younger adults to partly compensate for health limitations, but that health limitations have a stronger association with older adults’ diversity of daily life. This hypothesis rests upon previous knowledge that older adults face several challenges related to the process of aging, which might reduce the possibilities to compensate health limitations (i.e., age is a moderator of the association between health limitations and diversity of daily life). We did not have specific predictions regarding different indicators of health limitations such as impairments of the musculoskeletal or the cardiovascular system; instead we assumed that various health limitations can impede daily life and therefore examined a variety of health indicators. Differences between indicators are explored.
Study 1: Age Differences in Daily Life Diversity Across Days
In Study 1, we investigated age differences in the diversity of daily life across days and focused on two indicators of diversity: Variety in social partners and variety in activities. In addition, we examined variety in activities within days, that is, differences in activities from morning to evening.
Method
Participants.
The sample was part of a longitudinal study on personality development of younger and older adults (Quintus, Egloff, & Wrzus, 2019, article available on osf.io/p9zb5/). More details on the sample and the power analyses are reported in the online supplemental material. We recruited participants via local newspapers, flyers in public places (cafés, drug stores, vocational schools), mailing lists, and introductory courses for younger and older adults at a large German university. Of the 382 participants who initially registered for the study, 365 (73.2% female) completed at least 10 of 30 daily diary questionnaires and were included in the analyses. The sample consisted of 246 (67.4%) younger adults (M = 21.84; SD = 2.45; range = 18–32) and 119 (32.6%) older adults (M = 67.73; SD = 5.26; range = 51–78). All participants had completed secondary school education (German Abitur), and most younger and older participants were students (75.9%), whereas the rest had either attained vocational training (7.1%) or were retired (16.5%). Information on health of the sample and age differences therein are reported in Table 1.
Table 1.
Study 1: Means, Standard Deviations for Diversity of Activities Across and Within Days, Diversity of Social Partners Across Days, and Health Indicators and Zero-Order Correlations Among Variables
| YA | OA | Age difference | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | M (SD) | M (SD) | t | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
| 1. Diversity of activities within daysa Diversity of activities across days |
.36a (.06) | .39b (.06) | −5.00** | — | |||||||
| 2. Morning | .51a (.11) | .49a (.13) | 1.14 | .27** | — | ||||||
| 3. Afternoon | .56a (.12) | .62b (.09) | −5.01** | .46** | .35** | — | |||||
| 4. Evening | .59a (.11) | .54b (.13) | 3.38** | .01 | .22** | .16** | — | ||||
| 5. Diversity of social partners across days | .57a (.08) | .55b (.08) | 2.37* | .01 | .10 | .06 | .11* | — | |||
| 6. Subjective health problemsb | .01a (.74) | −.02a (.75) | 0.27 | .01 | −.04 | .04 | .09 | −.09 | — | ||
| 7. Chronic illnesses | 2.24a (3.11) | 5.08b (4.45) | −6.25** | .04 | .03 | .20** | .05 | −.09 | .45** | — | |
| 8. Functional limitations | 1.50a (.83) | 1.84b (.94) | −3.33** | .07 | .04 | .16** | .02 | −.08 | .50** | .54** | — |
Note. Columns 1 to 8 report zero-order correlations among variables for the entire sample. Means with different subscripts differ with p < .05 between younger adults (YA) and older adults (OA).
Diversity of activities within days refers to activities that vary between morning, afternoon, or evening.
Aggregate of subjective poor health (MYA 2.41, SDYA = 1.16; MOA = 2.55, SDOA = 1.15), t(363) = −1.15, p = .25; visits to doctors (MYA = 2.35, SDYA = .96; MOA = 2.77, SDOA = .89), t(250.70 = −4.20, p < .01; and sick days (MYA = 3.34, SDYA = 1.56; MOA = 2.27, SDOA = 1.65), t(362) = 6.03, p < .01; all three variables were z-standardized before aggregation due to different measurement scales.
p < .05.
p < .01.
Procedure.
At the beginning of the study (Fall 2015), participants received study information, provided informed consent, and completed online questionnaires and tests at home, as well as at the university laboratory in small age-homogeneous group sessions on the following day. During the following half year, participants completed daily online questionnaires on 10 consecutive evenings every 2 months (i.e., three waves of 10 daily assessments; M = 28.1 assessments per person, SD = 4.2, average compliance rate = 94%). During the 30 assessment days, participants received emails at 6 p.m. and reminders at 10 p.m. with personalized links to complete the online questionnaire, which was created using the online survey platform SoSci Survey (https://soscisurvey.de). Participants received a reimbursement of €49 (appr. $US 66) for completing this procedure and prorated reimbursement in case of drop out. The Ethics Committee of the Johannes Gutenberg University Mainz approved the study. The complete list of measures is available on OSF (osf.io/3s5bf).
Diversity measures derived from daily questionnaires.
In the daily questionnaires, participants characterized their day regarding their activities during the morning, afternoon, and evening. Furthermore, participants described the most important situation they experienced during the day, based on their own judgment, as well as which social partners and people were present during this experience. The experience was also rated on other dimensions (e.g., valence, behavior) for a separate research question on personality development (Quintus et al., 2019, article available at osf.io/p9zb5/).
Activities across and within days.
Each day, participants reported their main activity during the morning, afternoon, and evening by choosing one out of eight categories: work/study, domestic or other chores (e.g., laundry, shopping), private visit (family or friends), active leisure activities alone (e.g., sports, events), active leisure activities with others, other leisure activities alone (e.g., watching TV), other leisure activities with others (e.g., watching TV), or sleeping. Categories were adapted from Riediger and Freund (2008) and Wrzus and colleagues (2016) and covered a broad range of daily activities (e.g., Rauthmann, 2015).
The diversity of activities was calculated with the Shannon’s entropy index because this index conveys both richness and evenness of distribution of categories (Benson et al., 2018), has specified and easily interpretable boundaries between 0 and 1, appropriately takes the nested structure of daily diary data into account (Benson et al., 2018; Koffer, Ram, & Almeida, 2018; Lee et al., 2018) and allows direct comparisons with recent publications (e.g., on stressor diversity or daily activities; Koffer et al., 2018; Lee et al., 2018).
In general, the index is calculated as follows:
where m is the number of categories and p is the proportion of each category (1 to m) for a specific individual i. Higher scores indicate more diverse activities. We computed the indices separately per participant, daytime (i.e., morning, afternoon, evening), and 10-day period, which were then averaged across the three 10-day periods to indicate across-day diversity. The within-days diversity scores were also computed using Shannon’s entropy index separately for each day and across morning, afternoon, and evening activities. These scores were then averaged across all completed days per person.
Social partners across days.
Each day, participants indicated whether other persons were present during the most important situation of their day. They could choose one out of seven answer categories: nobody, one person, two persons, three to five persons, six to 10 persons, 11 to 20 persons, and more than 20 persons. For analyses, these categories were recoded into four content-related categories: alone, dyad, small group (two to five people), big group (more than six people). We computed Shannon’s entropy index again across each 10-day period and then averaged the three periods to indicate intraindividual diversity regarding the across-day involvement with other persons. Table S1 in the online supplemental material provides information on the distribution of the diversity indices. The number of completed assessments per person (M = 28.1, SD = 4.2, rage = .12, p = .02) was very high and thus virtually unrelated to the diversity of persons or activities (rs = .01–.06).
Health measures (single session assessment).
Participants completed different questionnaires and tests mainly on personality characteristics (e.g., to examine other research questions; study overview available on osf.io/p9zb5/) and on their physical health, which was relevant for the current research question. The measures are described in the following text.
Subjective health problems.
Participants answered three questions concerning their health, which have been validated in national panel studies (e.g., Sacker, Worts, & McDonough, 2011): “How would you describe your current health status?” on a seven-point Likert scale ranging from 1 (very good) to 7 (very bad); “How often have you been to a doctor during the last 6 months (except dentists)?” on a five-point Likert scale, where 1 = never, 2 = once, 3 = 2–5 times, 4 = 5–10 times, and 5 = more than 10 times; and “How long have you been ill during the last 6 months?” on an eight-point scale, where 1 = 0 days, 2 = 1–2 days, 3 = 3–5 days, 4 = 1 week, 5 = 2–3 weeks, 6 = 4–6 weeks, 7 = 6–8 weeks, and 8 = more than 8 weeks. Before averaging these three items (α = .55, Ω = .55), z scores were computed for each item to compensate for the different rating scales. Age differences in raw values are reported in the note to Table 1.
Chronic illnesses.
Participants reported diagnosed chronic illnesses using an adapted health conditions checklist from the Midlife Development in the United States study (see Marmot & Fuhrer, 2004). Participants answered the questions, “Has a doctor observed that you currently suffer from one or more of the following illnesses? If so, what is the severity level of this illness?” by indicating the severity level of each illness on a four-point scale ranging from 1 (low severity level) to 4 (high severity level) in case of its existence and 0 (does not apply) in case the illness was not diagnosed. Listed illnesses were allergies, cardiovascular diseases, neurological disorder (e.g., Parkinson disorder), mental disorder (e.g., major depression), cancer, skin disease, respiratory disease, gastric or intestinal disease, diabetes, otolaryngological diseases, skeletal disorder, and other disease(s). Severity levels were summed over all items.
Functional limitations.
Participants answered the question, which was adapted from the German Socioeconomic Panel Study (Deutsches Institut für Wirtschaftsforschung Berlin, 2013), “Apart from brief illnesses, does your current health status impede your daily life activities, e.g., at home, or at work? To what extent?” on a five-point Likert scale ranging from 1 (not at all) to 5 (very much). All health measures were correlated (see the present Table 1 and Table S2 in the online supplemental material for age groupspecific correlations).
Control analyses.
Student status (1 = student, −1 = nonstudent) was included in analyses as a control variable to test the robustness of results. Up to four outliers occurred per diversity index (see Table S3 in the online supplemental material for details). The outliers were three standard deviations beyond the average and were winsorized to the 0.1 or 99.9 percentile, respectively. Analyses on age and health differences in the diversity of daily activities were conducted with original and winsorized variables, and identical results were obtained using winsorized variables (see Table S3 in the online supplemental material). Statistical analyses were computed with SPSS 22 (IBM Corp. 2013). The analysis code is available on osf.io/p9zb5/.
Results and Discussion
Table 1 presents descriptive statistics for the daily life diversity scores and health indicators as well as zero-order correlations among variables for the entire sample. Age-group specific correlations are reported in Table S2 in the online supplemental material.
Age differences in diversity of daily life.
Our first research question addressed age differences in diversity of activities and social partners. Compared with younger adults, older adults reported less diverse activities in the evenings and less diversity of social partners, which was consistent with Hypothesis 1. However, older adults reported more diverse activities during the afternoons and over the day (i.e., from morning to evening; see Table 1), compared with younger adults, which was not in line with Hypothesis 1.
Health limitations and diversity of daily life.
Our second research question examined the extent to which age differences in daily life diversity may be accounted for by health limitations. In separate regression models, we predicted diversity of social partners and diversity of activities across- and within-days from age group (−1 = younger adults, 1 = older adults) as well as subjective health problems, chronic illnesses, functional limitations (see Table 2). To test our third hypothesis, we also included the interaction terms of the health indicators with age in these regression analyses to examine whether associations between health and daily life diversity are more pronounced for older adults, relative to younger adults. All health indicators were included in the regression models simultaneously to control for shared variance. Results of separate regression analyses are reported in the online supplemental material (see Tables S5 through S7).
Table 2.
Study 1: Results From Linear Regression Analyses With Age, Subjective Health Problems, Functional Limitations, and Chronic Illnesses as Predictors and Age as Moderator Predicting the Diversity of Activities Across and Within Days as Well as the Diversity of Social Partners Across Days
| Diversity of activities across days | ||||||
|---|---|---|---|---|---|---|
| Variable | Diversity of activities within days | Morning | Afternoon | Evening | Diversity of social partners across days | |
| Age | .26** [.15, .37] | −.13* [−.25, −.01] | .16** [.05, .27] | −.24** [−.36, −.13] | −.15* [−.26, −.04] | |
| Subjective health problems | −.02 [−.16, .12] | −.18* [−.32, −.04] | −.09 [−.23, .05] | .04 [−.10, .18] | −.19** [−.33, −.05] | |
| Subjective Health Problems × Age | −.09 [−.23, .05] | −.12 [−.26, .02] | −.08 [−.22, .06] | .01 [−.13, .15] | −.22** [−.36, −.08] | |
| Chronic illnesses | −.07 [−.21, .07] | .09 [−.05, .23] | .14* [.00, .27] | .17* [.03, .31] | .04 [−.10, .18] | |
| Chronic Illnesses × Age | .09 [−.04, .22] | .08 [−.05, .22] | .12 [−.01, .25] | .20** [.07, .33] | .02 [−.11, .15] | |
| Functional limitations | .06 [−.08, .20] | .11 [−.03, .26] | .08 [−.06, .22] | −.10 [−.23, .04] | .01 [−.13, .15] | |
| Functional Limitations × Age | −.04 [−.17, .10] | .08 [−.06, .22] | −.04 [−.18, .09] | −.16* [−.30, −.03] | .04 [−.10, .18] | |
| Model fit | ||||||
| F(3, 347) | 4.41 | 1.53 | 4.81 | 4.46 | 2.91 | |
| p | <.01 | .16 | <.01 | <.01 | <.01 | |
| Adjusted R2 | 6% | 1% | 7% | 6% | 4% | |
Note. β values and the 95% confidence intervals (in brackets) are reported for each predictor. Age is a contrast coded categorical variable (−1 = younger adults, 1 = older adults). Subjective health, chronic illnesses, and functional limitations were centered. The same pattern of results was achieved with winsorized variables. The functional limitations-by-age interaction on diversity of evening activities was not significant without the other health indicators in the model.
p < .05.
p < .01.
Regarding the diversity of activities (see Table 2), the regression model predicting diversity of morning activities was not statistically significant. For diversity in afternoon activities, older adults reported more diverse activities in the afternoons than younger adults, and this effect remained significant even with the inclusion of health indicators in the model. Regarding the diversity of evening activities, older adults showed less diverse engagement than younger adults, and this effect remained significant even when taking health into account. Our third hypothesis was only partly supported: Age moderated the association of both chronic illnesses and functional limitations with the diversity of evening activities (see Table 2). Among older adults, evening activities were more diverse with greater chronic illnesses, but this effect did not occur for younger adults (see Figure 1). In addition, for older adults, evening activities were slightly less diverse with more functional limitations, but this association was not significant for younger adults. Of note, this age-by-functional limitation interaction was not statistically significant (β = −.02, p = .77, CI [–.12, .09]), when functional limitations were the only health indicator in the model (see Table S7 in the online supplemental material). We therefore refrain from depicting and interpreting this finding further, as it might result from intercorrelations among the health indicators (Cohen, Cohen, West, & Aiken, 2003). All other effects and interactions remained robust in separate regression analyses (see Tables S5 through S7 in the online supplemental material). None of the health indicators predicted the diversity of activities within days (see Table 2).
Figure 1.
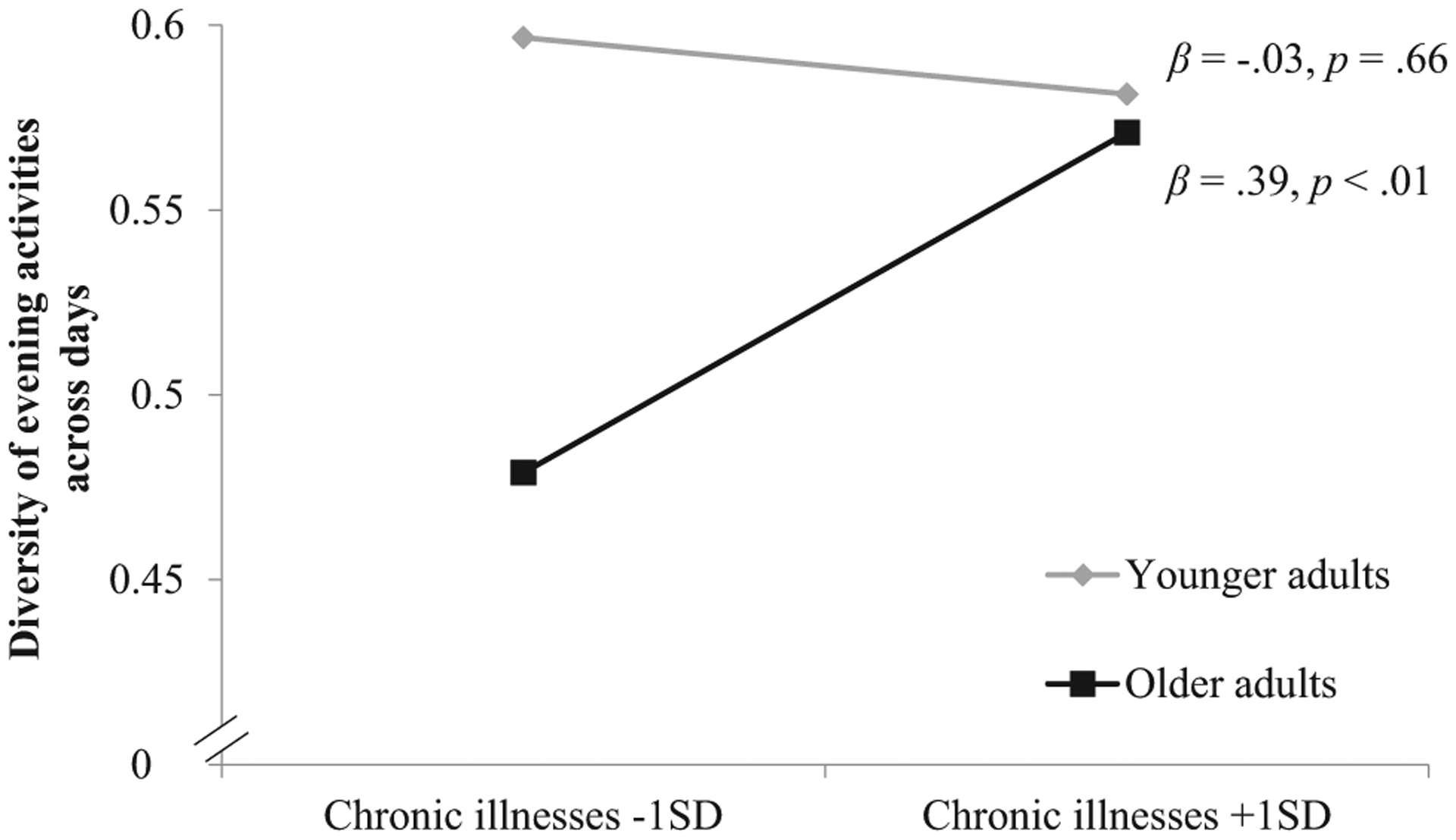
Study 1: Age moderates the association between chronic illnesses and the diversity of evening activities across days.
Regarding the diversity of social partners across days, the age difference remained significant and similar in size when health limitations were taken into account: Older adults reported less diverse involvements with other persons than younger adults (see Table 2). Consistent with Hypothesis 3, among older but not younger adults, subjective health problems were associated with less diversity of persons across days (see Figure 2).
Figure 2.
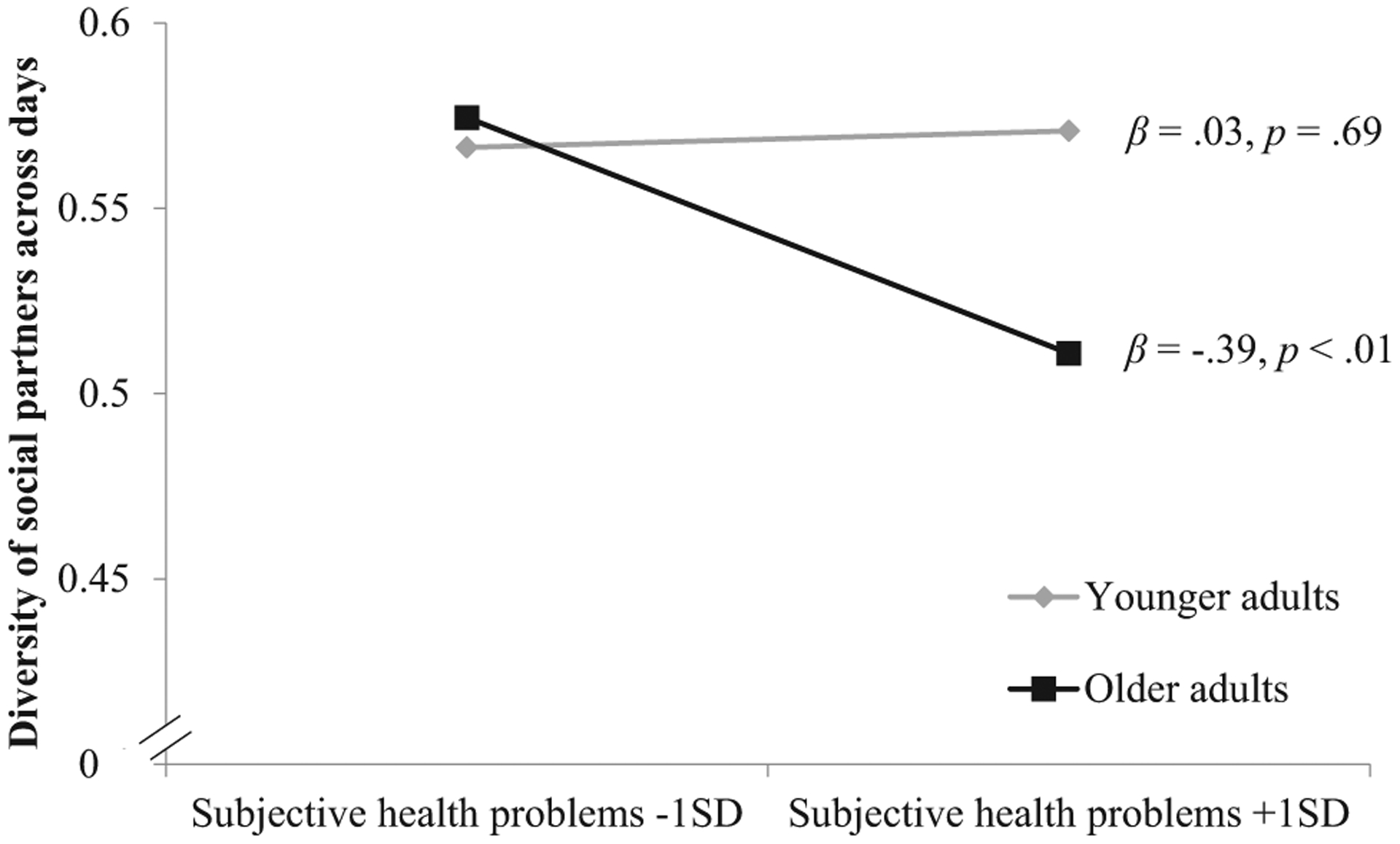
Study 1: Age moderates the association between subjective health problems and the diversity of social partners across days.
Because the sample consisted partly of younger and older students, control analyses took the student status into account. The results remained generally robust (see the online supplemental material).
Study 2: Age Differences in Daily Life Diversity Within Days
In Study 2, we moved from investigating diversity in persons and activities across several days, that is, three periods of about 10 days each, to examining diversity within days. Using an experience-sampling method, we gathered information about participants’ daily life experiences about six times a day for 9 days. In Study 2, assessments were randomly scheduled to sample broadly from people’s daily life and to overcome the limitation of Study 1, which relied on evening reports of the main activities during mornings, afternoons, and evenings as well as on persons involved in daily situations. In addition to diversity of persons and activities, Study 2 also examined the diversity of locations because different locations are an additional important characteristic of daily life diversity that signifies diversity through mobility (Hirsch, Winters, Ashe, Clarke, & McKay, 2016; Hirsch, Winters, Clarke, & McKay, 2014). Thus, Study 2 aimed at replicating the results from Study 1 on a more fine-grained time scale and at extending the previous results by examining the places people were at in their daily lives. Furthermore, whereas Study 1 examined mainly younger and older students, Study 2 used a community-based, life span sample that also included middle-aged adults, which allowed us to elucidate age differences across adulthood comprehensively.
Method
Participants.
Participants (N = 365) from three different regions in Germany were recruited by a fieldwork agency and part of an ongoing longitudinal project, the Multi-Method Ambulatory Assessment Project (Riediger, 2018; Riediger, Schmiedek, Wagner, & Lindenberger, 2009). Participants of the assessment in 2013 ranged in age from 14.0 to 88 years (M = 43.87 years, SD = 20.24). The sample was approximately stratified by gender (45.5% men) and age group (12% were between 14 and 18 years, 20% were between 19 and 29 years, 13% were between 30 and 39 years, 13% were between 40 and 49 years, 13% were between 50 and 59 years, 17% were between 60 and 69 years, and 12% were between 70 and 88 years). Of the 320 participants who had already finished school, 26% held a degree from an (applied) university (13% of the 19 to 29 year olds, 26% of the 30 to 39 year olds, 19% of the 40 to 49 year olds, 28% of the 50 to 59 year olds, 41% of the 60 to 69 year olds, 34% of the 70 to 88 year olds). For more details on the sample and the procedure, see also Luong, Wrzus, Wagner, and Riediger (2016). Because the original sample contained adolescents, we calculated the analyses with the full sample to retain statistical power, and we repeated the analyses with adults 18 years and older as reported at the end of the Results section.
Procedure.
In Study 2, participants first received an individual instruction session in their homes, during which they provided informed consent before they completed a computer-assisted personal interview (CAPI) with questions regarding their health, socioemotional functioning and other constructs. They also received instructions on the experience-sampling method and completed a tutorial experience-sampling questionnaire on the same mobile phones used in the daily life assessments (Huawei Ascend G330 with 4-in. display, 480 pixel × 800 pixel, and customized Android software that ensured reliable assessments also when participants were offline). During three experience-sampling periods, which started the day after the instruction, participants carried the phone with them at all times. Each of the three experience-sampling periods comprised three consecutive assessment days, and each period was separated by 6 days, covering a total of 3 weeks. On each experience-sampling day, 6 assessments occurred pseudorandomly about every 2 hr over a 12-hr window (M = 2.07 hr, SD = 0.68 hr difference between answered assessments per day). Participants had chosen the assessment window according to their personal waking habits. At each assessment, the phones prompted participants to answer a short questionnaire displayed on the phone. Participants navigated and responded to the questionnaire using the mobile phone’s touchpad. If participants did not respond, they received two auditory reminder signals after five and after 10 min. If there was still no response, the questionnaire closed, thus reducing participants’ degree of freedom in determining when to answer the questions. Technical support was constantly available for each participant from the interviewers who conducted the instruction sessions.
To obtain a sufficient number of assessments, experience-sampling periods were extended for a day if participants completed fewer than five assessments on a given day. Overall, 1.27 (SD = 1.78) of these extension days were scheduled per participant. Participants thus completed an average of 55.7 assessments, (SD = 4.9) in total, and at least five of six daily assessments on 91.7% of their assessment days, (SD = 12.1). After the experience-sampling phase, participants again answered questionnaires during a second individual session in their homes and received a reimbursement of approximately $US135 (€100). The Ethics Committee of the Max Planck Institute for Human Development, Berlin, approved the study.
Diversity measures regarding places, activities, and social partners derived from repeated assessment during the experience-sampling period.
At each momentary assessment, participants reported where they were at that moment (i.e., momentary place) choosing one of the following categories: at home, at work/school/university, in a public building, at a visit, in transit, and other. To indicate in which activities they were currently engaged (i.e., momentary activity), participants could choose one or more of the following categories: work/school/study, chores, doctor visit/official errand, leisure activity, conversation/visit, watching TV/doing nothing/napping, and other. We excluded cases with more than three concurrent activities at a single assessment because they might bias diversity scores slightly, which depict the proportion of each category’s occurrence and thus would add to more than 100% when multiple activities are chosen. Multiple choices did not constitute a severe problem because reports of multiple activities occurred in less than 1% of all cases. To assess social partners, participants reported who was currently with them, and could choose one or more of the following categories: nobody (single choice), partner, family, friends, colleagues/fellow students, strangers, or other.
As in Study 1, we computed diversity indices based on Shannon’s entropy per day and domain (i.e., places, activities, and persons), and then averaged across all days for each participant and diversity domain (i.e., places, activities, social partners). Similar to Study 1, the number of experience sampling assessments per person was very high (M = 55.7, SD = 4.9, rage = −.24, p < .01) and were unrelated to the diversity of persons, places, or activities (rs ranged between −.03 and .01).
Health measures (single session assessment).
Chronic illnesses and functional limitations were assessed as in Study 1. Subjective health problems differed from the Study 1 measurement as it was based on a five-point Likert scale ranging from 1 (very good health) to 5 (bad health). As a fourth indicator of general health, participants rated health complaints and answered the question “Which of the following complaints do you currently have?” on a five-point scale where 1 = none, 2 = little, 3 = middle, 4 = intensive, 5 = most intensive. The complaints were heavy sweating, sleep disorders, heart complaints, physical exhaustion/diminished energy, joint and muscle complaints, irritability, anxiety, depressive mood, and constant pain. Severities of complaints were then averaged.
Control variables.
Participants provided demographic information during the initial CAPI. From these data, we created three effect-coded control variables that may contribute to diversity in daily life: (a) participants’ family status (1 = married/steady relationship, −1 single/divorced/widowed), (b) occupational status (1 = full- or half-time employment, −1 = no employment), and (c) parental status (1 = one or more children, −1 = no children). Four outliers (outside the range of 3 standard deviations from the mean) in diversity of places and one outlier in diversity of activity were observed. These outliers were winsorized to the 0.1 or 99.9 percentile, respectively. Analyses on age and health differences in the diversity of places and activities were conducted with winsorized and original data, and virtually identical results were observed with both sets of analyses (see Table S4 in the online supplemental material).
Results and Discussion
Table 3 reports descriptive statistics on the diversity of places, persons, and activities within days and the health indicators as well as zero-order correlations among all variables. Table S1 in the online supplemental material provides further information on the distribution of the diversity indices.
Table 3.
Study 2: Means, Standard Deviations, and Zero-Order Correlations for Age, Diversity of Places, Activities, and Social Partners Within Days, Subjective Health Problems, Functional Limitations, Chronic Illnesses, and Health Complaints
| Variable | M (SD) | 1a | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Age | 43.9 (20.2) | — | ||||||||
| 2. Diversity of places within days | .27 (.07) | −.23** | — | |||||||
| 3. Diversity of activities within days | .52 (.10) | .13* | .16** | — | ||||||
| 4. Diversity of social partners within days | .42 (.13) | −.39** | .42** | .29** | — | |||||
| 5. Subjective health problems | 2.31 (.92) | .39** | −.20** | .09** | −.16** | — | ||||
| 6. Chronic illnesses | 2.29 (3.33) | .38** | −.16** | .07 | −.20** | .53** | — | |||
| 7. Functional limitations | 1.74 (1.03) | .32** | −.13* | .12* | −.14* | .63** | .59** | — | ||
| 8. Health complaints | 1.73 (.59) | .32** | −.18** | .06 | −.19** | .61** | .61** | .62** | — | |
| 9. Education level | .26 (.44) | .21** | −.07 | .13* | −.05 | −.04 | −.05 | −.03 | −.03 | — |
Note. Health information were rated on five-point scales. Education level was dummy coded with 1 for college degree and 0 for no college degree. Columns 1 to 8 report zero-order correlations.
Nonlinear age associations for diversity of places, activities, and social partners are not reported here but are reported elsewhere. No significant quadratic age effects were observed for any of the health indicators.
p < .05.
p < .01.
Age differences in diversity of daily life.
We predicted that higher age would be related to less diversity in daily life and found support for this hypothesis regarding the diversity of places and social partners within days. The zero-order correlations showed that older age was associated with less diversity in daily life places, and remained statistically significant when adjusting for health problems, chronic illnesses, functional limitations, and health complaints (see Table 4). Older age was associated with less diverse social partners in daily life, even when controlling for health problems, chronic illnesses, functional limitations, and health complaints. Moreover, age was associated nonlinearly with the diversity of activities as indicated by the quadratic age effect (see Table 4): The youngest adults and older adults reported somewhat more diverse activities than adults in their late 30s, with large individual differences at any age (see Figure 3 where the predicted minimum of activity diversity is age 38.0 years). This effect remained statistically significant when adjusting for health limitations.
Table 4.
Study 2: Results From Linear Regression Analyses With Age, Subjective Health Problems, Functional Limitations, and Chronic Illnesses as Predictors and Age as Moderator Predicting Diversity of Places, Activities, and Social Partners Within Days
| Variable | Diversity of places within days | Diversity of activities within days | Diversity of social partners within days |
|---|---|---|---|
| Age | −.16** [−.28, −.04] | .07 [−.05, .19] | −.38** [−.49, −.27] |
| Age2 | −.01 [−.13, .11] | .15* [.03, .27] | .02 [−.09, .13] |
| Subjective health problems | −.10 [−.25, .04] | .01 [−.14, .16] | .03 [−.11, −.17] |
| Subjective Health Problems × Age | −.01 [−.16, .13] | .08 [−.07, .22] | .02 [−.11, .16] |
| Chronic illnesses | −.07 [−.23, .10] | .05 [−.12, .21] | −.04 [−.19, .12] |
| Chronic Illnesses × Age | .07 [−.09, .23] | −.13 [−.29, .03] | −.02 [−.16, .13] |
| Functional limitations | .07 [−.09, .23] | .12 [−.04, .28] | .10 [−.05, .25] |
| Functional Limitations × Age | −.09 [−.24, .07] | −.05 [−.21, .11] | −.09 [−.24, .06] |
| Health complaints | −.08 [−.22, .07] | −.05 [−.20, .10] | −.10 [−.24, .04] |
| Health Complaints × Age | .07 [−.08, .21] | .00 [−.14, .15] | −.02 [−.15, .12] |
| Model fit | |||
| F(10, 341) | 2.78 | 1.89 | 6.85 |
| p | <.01 | .04 | <.01 |
| Adjusted R2 | 5% | 2% | 14% |
Note. β values and 95% confidence intervals (in brackets) are reported for each predictor. The same pattern of results was achieved with winsorized variables.
p < .05.
p < .01.
Figure 3.

Study 2: Age differences in diversity of activities within days. Dotted lines represent 95% confidence intervals.
Health and diversity of daily life.
We predicted that individual differences in health partly account for age differences in daily life diversity and that age moderates the associations between health and daily life diversity. Although indicators of health and illnesses were partly related to the diversity of places, activities, and persons on a zero-order level (see Table 3), these associations seemed attributable to shared variance with age because none of the predictors were statistically significant when considered together with age (see Table 4). In addition, counter to the results on between-day diversity, yet similar to the result on within-day activity diversity in Study 1, no significant interactions between age and health indicators were observed in predicting within-day diversity indicators (see Table 4).
As robustness checks, we controlled for relationship, occupational, and parental status (see Table S8 in the online supplemental material), and we repeated the main analyses with the subsample of participants between 18 and 88 years to cover a similar age range as in Study 1. The results fully replicated the previous pattern of reported results (see Tables S9 and S10 in the online supplemental material).
General Discussion
The objectives of the present studies were to examine whether age differences occur in the diversity of daily life, and to what extent health limitations may account for such age differences. In addition, our study investigated whether age moderates associations between diversity of daily lives and health limitations. We predicted that the daily life of older adults would be more homogeneous and accordingly, vary less in social involvement, activities, and locations, compared with younger adults. Our findings on age differences in diversity of daily life demonstrate a pattern that is more complex than expected, but consistent across the two studies, as discussed in the following text.
Age Differences in the Diversity of Daily Life
Our results showed that older adults experience more homogeneity in some areas of daily life: With older age, people reported less diverse social contacts across and within days (Study 1 and Study 2, respectively). These results were consistent across both studies, although Study 1 focused on social contacts during the most important situation of the day, and Study 2 examined pseudorandomly assessed situations per day. The results are in line with previous research that older adults spend most of their time with the same persons (Altergott, 1990; M. M. Baltes et al., 1990; Horgas et al., 1998). One potential reason for less social diversity in daily life could be that social network size and social contact decrease across the life span when people increasingly focus on close others, such as their core family (Cornwell, 2011; Sander et al., 2017; Wrzus et al., 2013). Smaller social networks and less contact limit the pool of potential social contacts to fewer people and thus restrict the number and diversity of social partners to choose from.
Interestingly, age differences diverged when considering different types of activity diversity: Among older adults, evening activities were less diverse than among young adults, and no reliable age differences occurred regarding diversity of morning activities (Study 1). In contrast, afternoon activities and activities during the day were more diverse among older compared with younger adults (Studies 1 and 2). Retirement likely does not account for these results because in Study 2 the age differences occurred well before retirement age. Instead, this age difference might be partly explained by younger adults being occupied with work and studying many hours of the day. This might be especially true for morning and afternoon given that these age differences were weakened when occupational status was statistically controlled. Our findings suggest that older adults do not necessarily have more homogeneous daily lives than younger adults do because younger adults also experience some constraints: For example, due to working or studying, younger adults have relatively structured days, particularly in the mornings and in the afternoons, which leads to reoccurring activities. Yet, evening activities were more diverse among younger adults. Previous research showed age differences in engaging in specific activities: older adults engaged in less leisure, but more obligatory (e.g., self-care, chores) and resting activities (M. M. Baltes et al., 1990; Gordon et al., 1976; Horgas et al., 1998; Paillard-Borg et al., 2009). The current findings complement this research by examining age differences in the diversity of activities across and within days and by highlighting the importance of the time of day in understanding daily life activities.
Health and the Diversity of Daily Life
The studies also examined whether individual differences in health partly account for age differences in the diversity of daily life, as older adults are more likely to experience impaired health (P. B. Baltes, 1987; M. M. Baltes et al., 1990; Horgas et al., 1998; Paillard-Borg et al., 2009). We predicted that it might be possible for younger adults to compensate for health limitations, whereas older adults already face several challenges related to aging, which might aggravate health constraints.
In both studies and in contrast to Hypothesis 2, age remained a significant predictor of diversity in daily life even when including different health indicators in the models. Even though health indicators shared some variance with age, age itself was still uniquely associated with daily diversity. These results stand in contrast to findings from other studies, in which old age alone could not explain lower engagement in activities, but instead health status was the most important factor, especially in old age (Lefrancois et al., 1997; McGuire et al., 1986). However, participants in the current studies, especially the older adults, reported relatively low levels of impaired health, which might partly explain why the small age differences in health did not account for age differences in daily life diversity.
Regarding Hypothesis 3, which predicted that health effects on daily life diversity differ with age, the current findings varied across health indicators and only allow preliminary conclusions. In support of Hypothesis 3, we found that only for older adults did health indicators predict diversity across days (Study 1), but not within days (Studies 1 and 2). In line with our predictions, among older adults, subjective health problems predicted less diverse involvements with persons across days. Effects of functional limitations differed depending on whether other health indicators were included in the model. Accordingly, we refrain from drawing definitive conclusions concerning this result, but emphasize that examining multiple health indicators and their common as well as unique effects on daily life diversity seems important also in future studies. Specific chronic illnesses might impair daily life less when people found feasible adjustments (e.g., Curtis et al., 2017). At the same time, subjective evaluations of health often differ from objectively diagnosable illnesses (Wettstein, Schilling, & Wahl, 2016), which might explain that subjective health evaluations and rather objective indicators of illnesses can predict daily activities differently (Curtis et al., 2017).
Other than expected, more severe chronic illnesses were associated with more diverse activity engagements in the evenings among older adults. This effect might result from more resting and medical treatments on days when older adults did not feel well in contrast to leisure activities on the other days (Study 1). Previously, impaired health was strongly associated with more medical treatments and resting activities (M. M. Baltes et al., 1990). A recent daily diary study similarly observed that on days with more physical symptoms, people reported more engagement in quiet, mental activities such as reading or listening to radio (Curtis et al., 2017). Thus, it is possible that chronic illnesses are linked to more diversity in evening activities of older adults, as they engage more in resting and medical activities on days when they feel ill, but not on other days—leading to greater diversity of activities across days, but not within days. When investigating within-day diversity in places, persons, and activities, no associations with health were found. It thus appears that individual differences in health mainly contribute to diversity across days, not within days. This is plausible, given that health indicators may also vary more strongly between days compared with within days. This interpretation, however, awaits empirical support because so far only variability across days and persons has been investigated (Curtis et al., 2017; Wolff et al., 2012).
Limitations and Future Directions
Our studies had a number of strengths, offering unique and complementary data assessed in daily life that allowed examining diversity across as well as within days, and which revealed highly consistent results regarding age differences. However, some limitations need to be mentioned. First, whereas Study 2 included a life span sample stratified by age and gender and recruited from different German regions with different educational background, Study 1 consisted largely of women and all participants held a college entrance degree (i.e., German Abitur). Despite the differences in samples, we observed similar results regarding age differences in the diversity of social partners and of activities within days. This finding indicates that the predicted age differences may be applicable across different population groups. Whether similar age differences in daily life diversity occur in samples of people with greater functional limitations (e.g., people with physical disabilities) remains an open issue, as so far only older adults with functional limitations have been studied (e.g., Simonsick et al., 1998).
Second, the studies focused on categories of persons, activities or places, potentially grouping different instances into the same category. For example, when an adult indicated that he or she is with a friend at the moment, we do not know if this friend is the same person as the friend mentioned in the situations prior or afterward. The same is true for activities (e.g., working) and places (e.g., in a public building). Also, we focused on the main activity, whereas in certain situations people might perform combined activities (e.g., cooking and socializing). Thus, the measures of diversity in the current study might somewhat underestimate the absolute amount of diversity (e.g., different types of work activity). We chose these categories because they (a) were applicable for the age range from young adults to old age, (b) were validated and frequently used in experience sampling studies (e.g., Rauthmann et al., 2014; Riediger & Freund, 2008; Sonnenberg et al., 2012), and (c) captured the majority of daily situations while keeping the number of categories manageable for the mobile assessment (as indicated by the low occurrence of “other” in previous studies using the same categories, Wrzus et al., 2016). Research on taxonomies of situations (i.e., activities, people, places) derived these broad categories from specific fine-grained and often also open-ended responses (Funder, 2016; Morse, Neel, Todd, & Funder, 2015; Rauthmann et al., 2014; Rauthmann, 2015). Yet, this previous research aimed at finding distinct categories of situations (e.g., Morse et al., 2015; Rauthmann et al., 2014). It remains an open issue whether capturing the diversity of activities, persons, or places would need a different approach to distinguish “true” diversity of daily life from people’s ability to conceptualize the complexity of daily life. In addition, future studies could take temporal aspects of activities into account: Studies could examine (a) how variations in activity durations (e.g., long work periods vs. brief periods in transit) contribute to diversity, that is, the likelihood of a different activity a few hours later and (b) how sequences of activities such as weekly or daily routines (e.g., breakfast with spouse, then work followed by lunch with colleagues, again work, and grocery shopping and TV in the evening) describe daily life diversity or homogeneity.
Third, Study 2 used an experience-sampling method that captured the momentary location, activity, and present people up to six times a day—still it did not capture people’s entire days. Likewise, Study 1 relied on fragmentary data because the main activity in the morning, afternoon, and evening was assessed. If the current samples of activities, persons, and locations are indeed random samples of people’s days, it might not be problematic that not all activities, social contacts, and locations are assessed—especially given that several days and weeks were examined, which allow greater generalization of findings compared with, for example, general retrospective ratings or day-reconstruction studies covering one day (Kahneman et al., 2004; White & Dolan, 2009). To achieve more fine-grained information about a person’s day, future studies may need even more precise measurement techniques, for example by using GPS-tracking for locations and traveled area (i.e., activity space; Hirsch et al., 2014, 2016; Zenk, Kraft, Jones, & Matthews, 2019; Zenk, Matthews, Kraft, & Jones, 2018) or audio recordings for social partners (e.g., Mehl, Gosling, & Pennebaker, 2006; Wrzus & Mehl, 2015, 2017). Future studies examining daily diversity in more detail might use such techniques and might further focus on how diversity of daily life predicts important outcomes such as life satisfaction, successful aging, and cognitive development (M. M. Baltes et al., 1990; Hertzog, Kramer, Wilson, & Lindenberger, 2008; Lee et al., 2018; Paillard-Borg et al., 2009).
Finally, in Hypothesis 2 we assumed that individual differences in health partly account for age differences in diversity of daily life. We carefully phrased our assumptions and results to reflect effects of shared variance between age, health status, and daily life diversity indices instead of mediation. Generally, mediation processes cannot be inferred from cross-sectional observational data (Hofer & Sliwinski, 2001; Lindenberger, von Oertzen, Ghisletta, & Hertzog, 2011). Because it seems unfeasible and unethical to experimentally manipulate moderate to severe health limitations to test mediation, longitudinal approaches could be a first step to examine mediational processes in the future (Maxwell & Cole, 2007).
Conclusion
The current studies provide initial evidence that the daily life of older adults is more homogeneous in some areas, such as daily social partners, yet it can be more heterogeneous in daily activities, as younger adults face some restrictions as well due to working or studying. The findings await further confirmation, whether similar age effects occur when choosing different units of analysis for activities, social partners or places (e.g., capturing daily activities in more fine-grained categories; distinguishing places such as rooms within the home). Based on the current findings, it does not seem to be the case that older adults generally experience less diversity in daily life. Instead, both younger and older adults, that is, people at any age, experience variety in some aspects of daily life and monotony in others.
Supplementary Material
Acknowledgments
This research was supported by the German Research Foundation Grant WR 160/1-1 to Cornelia Wrzus and the German Federal Ministry for Education and Research Grants MPI001 and 01UW0706 awarded to Michaela Riediger. Materials and data scripts for the study are available at osf.io/p9zb5/.
Footnotes
This work was presented at the paEpsy meeting in September 9–12, 2019 at Universistät Leipzig, Leipzig, Germany. Both studies are part of larger longitudinal projects, which addressed other research questions using the current samples, but not the same data (e.g. Luong et al., 2016; Quintus, Egloff, & Wrzus, 2017; Quintus et al., 2019; Wrzus, Egloff, & Quintus, 2019). None of the current research questions are addressed in other publications. Descriptive information of health indicators in Study 2 are also reported in Luong et al. (2016).
Supplemental materials: http://dx.doi.org/10.1037/pag0000407.supp
References
- Altergott K (1990). Age, gender and daily life: An analysis of social involvements. Social Indicators Research, 23, 367–380. 10.1007/BF00572530 [DOI] [Google Scholar]
- Arnett JJ (2000). Emerging adulthood. A theory of development from the late teens through the twenties. American Psychologist, 55, 469–480. 10.1037/0003-066X.55.5.469 [DOI] [PubMed] [Google Scholar]
- Baltes MM, Wahl H-W, & Schmid-Furstoss U (1990). The daily life of elderly Germans: Activity patterns, personal control, and functional health. Journal of Gerontology, 45, 173–179. 10.1093/geronj/45.4.P173 [DOI] [PubMed] [Google Scholar]
- Baltes PB (1987). Theoretical propositions of life-span developmental psychology: On the dynamics between growth and decline. Developmental Psychology, 23, 611–626. 10.1037/0012-1649.23.5.611 [DOI] [Google Scholar]
- Baltes PB (1997). On the incomplete architecture of human ontogeny. Selection, optimization, and compensation as foundation of developmental theory. American Psychologist, 52, 366–380. 10.1037/0003-066X.52.4.366 [DOI] [PubMed] [Google Scholar]
- Benson L, Ram N, Almeida DM, Zautra AJ, & Ong AD (2018). Fusing biodiversity metrics into investigations of daily life: Illustrations and recommendations with emodiversity. Journal of Gerontology, 73, 75–86. 10.1093/geronb/gbx025 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buss DM (1987). Selection, evocation, and manipulation. Journal of Personality and Social Psychology, 53, 1214–1221. 10.1037/0022-3514.53.6.1214 [DOI] [PubMed] [Google Scholar]
- Carstensen LL (1992). Social and emotional patterns in adulthood: Support for socioemotional selectivity theory. Psychology and Aging, 7, 331–338. 10.1037/0882-7974.7.3.331 [DOI] [PubMed] [Google Scholar]
- Carstensen LL (1995). Evidence for a life-span theory of socioemotional selectivity. Current Directions in Psychological Science, 4, 151–156. 10.1111/1467-8721.ep11512261 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carstensen LL, Isaacowitz DM, & Charles ST (1999). Taking time seriously. A theory of socioemotional selectivity. American Psychologist, 54, 165–181. 10.1037/0003-066X.54.3.165 [DOI] [PubMed] [Google Scholar]
- Caspi A, Roberts BW, & Shiner RL (2005). Personality development: Stability and change. Annual Review of Psychology, 56, 453–484. 10.1146/annurev.psych.55.090902.141913 [DOI] [PubMed] [Google Scholar]
- Cloninger CR (1987). A systematic method for clinical description and classification of personality variants. A proposal. Archives of General Psychiatry, 44, 573–588. 10.1001/archpsyc.1987.01800180093014 [DOI] [PubMed] [Google Scholar]
- Cohen J, Cohen P, West SG, & Aiken LS (2003). Applied multiple regression/correlation analysis for the behavioral sciences. Mahwah, NJ: Lawrence Erlbaum. [Google Scholar]
- Cornwell B (2011). Age trends in daily social contact patterns. Research on Aging, 33, 598–631. 10.1177/0164027511409442 [DOI] [Google Scholar]
- Curtis RG, Windsor TD, Mogle JA, & Bielak AA (2017). There’s more than meets the eye: Complex associations of daily pain, physical symptoms, and self-efficacy with activity in middle and older adulthood. Gerontology, 63, 157–168. 10.1159/000450786 [DOI] [PubMed] [Google Scholar]
- Deutsches Institut für Wirtschaftsforschung Berlin. (2013). SOEP 2012–Erhebungsinstrumente 2012 (Welle 29) des Sozio-oekonomischen Panels: Personenfragebogen, Altstichproben (SOEP Survey Papers, No. 158). Retrieved from http://hdl.handle.net/10419/88779
- Drewelies J, Koffer RE, Ram N, Almeida DM, & Gerstorf D (2019). Control diversity: How across-domain control beliefs are associated with daily negative affect and differ with age. Psychology and Aging, 34, 625–639. 10.1037/pag0000366 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fleeson W, & Gallagher P (2009). The implications of Big Five standing for the distribution of trait manifestation in behavior: Fifteen experience-sampling studies and a meta-analysis. Journal of Personality and Social Psychology, 97, 1097–1114. 10.1037/a0016786 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Funder DC (2016). Taking situations seriously: The situation construal model and the riverside situational Q-sort. Current Directions in Psychological Science, 25, 203–208. 10.1177/0963721416635552 [DOI] [Google Scholar]
- Garfein AJ, & Herzog AR (1995). Robust aging among the young-old, old-old, and oldest-old. The Journals of Gerontology Series B, Psychological Sciences and Social Sciences, 50, S77–S87. 10.1093/geronb/50B.2.S77 [DOI] [PubMed] [Google Scholar]
- González-Cutre D, Sicilia Á, Sierra AC, Ferriz R, & Hagger MS (2016). Understanding the need for novelty from the perspective of self-determination theory. Personality and Individual Differences, 102, 159–169. 10.1016/j.paid.2016.06.036 [DOI] [Google Scholar]
- Gordon C, Gaitz CM, & Scott J (1976). Leisure and lives: Personal expressivity across the life span. In Binstock R & Shanas E (Eds.), Handbook of aging and the social sciences (pp. 310–341). New York, NY: Van Nostrand Reinhold. [Google Scholar]
- Havighurst RJ (1974). Developmental tasks and education. New York, NY: McKay. [Google Scholar]
- Hertzog C, Kramer AF, Wilson RS, & Lindenberger U (2008). Enrichment effects on adult cognitive development: Can the functional capacity of older adults be preserved and enhanced? Psychological Science in the Public Interest, 9, 1–65. 10.1111/j.1539-6053.2009.01034.x [DOI] [PubMed] [Google Scholar]
- Hirsch JA, Winters M, Ashe MC, Clarke P, & McKay H (2016). Destinations that older adults experience within their GPS activity spaces: Relation to objectively measured physical activity. Environment and Behavior, 48, 55–77. 10.1177/0013916515607312 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hirsch JA, Winters M, Clarke P, & McKay H (2014). Generating GPS activity spaces that shed light upon the mobility habits of older adults: A descriptive analysis. International Journal of Health Geographics, 13, 51. 10.1186/1476-072X-13-51 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hofer SM, & Sliwinski MJ (2001). Understanding ageing. An evaluation of research designs for assessing the interdependence of ageingrelated changes. Gerontology, 47, 341–352. 10.1159/000052825 [DOI] [PubMed] [Google Scholar]
- Horgas AL, Wilms H-U, & Baltes MM (1998). Daily life in very old age: Everyday activities as expression of successful living. The Gerontologist, 38, 556–568. 10.1093/geront/38.5.556 [DOI] [PubMed] [Google Scholar]
- Hutteman R, Hennecke M, Orth U, Reitz AK, & Specht J (2014). Developmental tasks as a framework to study personality development in adulthood and old age. European Journal of Personality, 28, 267–278. 10.1002/per.1959 [DOI] [Google Scholar]
- Corp IBM. (2013). IBM SPSS Statistics for Windows (Version 22.0) [Computer software]. Armonk, NY: IBM Corp. [Google Scholar]
- Iso-Ahola SE, Jackson EL, & Dunn E (1994). Starting, ceasing, and replacing leisure activities over the human life-span. Journal of Leisure Research, 26, 227–249. 10.1080/00222216.1994.11969958 [DOI] [Google Scholar]
- Janke M, Davey A, & Kleiber D (2006). Modeling change in older adults’ leisure activities. Leisure Sciences, 28, 285–303. 10.1080/01490400600598145 [DOI] [Google Scholar]
- Kahneman D, Krueger AB, Schkade DA, Schwarz N, & Stone AA (2004). A survey method for characterizing daily life experience: The day reconstruction method. Science, 306, 1776–1780. 10.1126/science.1103572 [DOI] [PubMed] [Google Scholar]
- Koffer RE, Ram N, & Almeida DM (2018). More than counting: An intraindividual variability approach to categorical repeated measures. The Journals of Gerontology: Series B, 73, 87–99. 10.1093/geronb/gbx086 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kuppens P, Oravecz Z, & Tuerlinckx F (2010). Feelings change: Accounting for individual differences in the temporal dynamics of affect. Journal of Personality and Social Psychology, 99, 1042–1060. 10.1037/a0020962 [DOI] [PubMed] [Google Scholar]
- Kuppens P, Sheeber LB, Yap MBH, Whittle S, Simmons JG,& Allen NB (2012). Emotional inertia prospectively predicts the onset of depressive disorder in adolescence. Emotion, 12, 283–289. 10.1037/a0025046 [DOI] [PubMed] [Google Scholar]
- Lang FR, & Carstensen LL (1994). Close emotional relationships in late life: Further support for proactive aging in the social domain. Psychology and Aging, 9, 315–324. 10.1037/0882-7974.9.2.315 [DOI] [PubMed] [Google Scholar]
- Lee HY, Jang S-N, Lee S, Cho S-I, & Park E-O (2008). The relationship between social participation and self-rated health by sex and age: A cross-sectional survey. International Journal of Nursing Studies, 45, 1042–1054. 10.1016/j.ijnurstu.2007.05.007 [DOI] [PubMed] [Google Scholar]
- Lee S, Koffer RE, Sprague BN, Charles ST, Ram N, & Almeida DM (2018). Activity diversity and its associations with psychological well-being across adulthood. The Journals of Gerontology: Series B, 73, 985–995. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lefrancois R, Leclerc G, & Poulin N (1997). Predictors of activity involvement among older adults. Activities, Adaptation and Aging, 22, 15–29. 10.1300/J016v22n04_03 [DOI] [Google Scholar]
- Lewin K (1939). Field theory and experiment in social psychology: Concepts and methods. American Journal of Sociology, 44, 868–896. 10.1086/218177 [DOI] [Google Scholar]
- Lindenberger U, von Oertzen T, Ghisletta P, & Hertzog C (2011). Cross-sectional age variance extraction: What’s change got to do with it? Psychology and Aging, 26, 34–47. 10.1037/a0020525 [DOI] [PubMed] [Google Scholar]
- Lindesay J, & Thompson C (1993). Housebound elderly people: Definition, prevalence and characteristics. International Journal of Geriatric Psychiatry, 8, 231–237. 10.1002/gps.930080306 [DOI] [Google Scholar]
- Luong G, Rauers A, & Fingerman KL (2015). The multifaceted nature of late-life socialization: Older adults as agents and targets of socialization. In Grusec JE & Hastings PD (Ed.), Handbook of socialization: Theory and research (Vol. 2nd, pp. 109–131). New York, NY: Guilford Press. [Google Scholar]
- Luong G, Wrzus C, Wagner GG, & Riediger M (2016). When bad moods may not be so bad: Valuing negative affect is associated with weakened affect-health links. Emotion, 16, 387–401. 10.1037/emo0000132 [DOI] [PubMed] [Google Scholar]
- Magnusson D (1981). Toward a psychology of situations: An interactional perspective. Hillsdale, NJ: Lawrence Erlbaum. [Google Scholar]
- Marmot MG, & Fuhrer R (2004). Socioeconomic position and health across midlife. In Brim OG, Ryff CD, & Kessler RC(Eds.), How healthy are we? A national study of well-being at midlife (pp. 64–89). Chicago, IL: University of Chicago Press. [Google Scholar]
- Maxwell SE, & Cole DA (2007). Bias in cross-sectional analyses of longitudinal mediation. Psychological Methods, 12, 23–44. 10.1037/1082-989X.12.1.23 [DOI] [PubMed] [Google Scholar]
- McGuire FA, Dottavio D, & O’Leary JT (1986). Constraints to participation in outdoor recreation across the life span: A nationwide study of limitors and prohibitors. The Gerontologist, 26, 538–544. 10.1093/geront/26.5.538 [DOI] [PubMed] [Google Scholar]
- Mehl MR, Gosling SD, & Pennebaker JW (2006). Personality in its natural habitat: Manifestations and implicit folk theories of personality in daily life. Journal of Personality and Social Psychology, 90, 862–877. 10.1037/0022-3514.90.5.862 [DOI] [PubMed] [Google Scholar]
- Menec VH (2003). The relation between everyday activities and successful aging: A 6-year longitudinal study. The Journals of Gerontology Series B, Psychological Sciences and Social Sciences, 58, S74–S82. 10.1093/geronb/58.2.S74 [DOI] [PubMed] [Google Scholar]
- Morse PJ, Neel R, Todd E, & Funder D (2015). Renovating situation taxonomies: Exploring the construction and content of fundamental motive situation types. Journal of Personality, 83, 389–403. 10.1111/jopy.12111 [DOI] [PubMed] [Google Scholar]
- Paillard-Borg S, Wang H-X, Winblad B, & Fratiglioni L (2009). Pattern of participation in leisure activities among older people in relation to their health conditions and contextual factors: A survey in a Swedish urban area. Ageing and Society, 29, 803–821. 10.1017/S0144686X08008337 [DOI] [Google Scholar]
- Parisi JM (2010). Engagement in adulthood: Perceptions and participation in daily activities. Activities, Adaptation and Aging, 34, 1–16. 10.1080/01924780903552246 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Quintus M, Egloff B, & Wrzus C (2017). Predictors of volitional personality change in younger and older adults: Response surface analyses signify the complementary perspectives of the self and knowledgeable others. Journal of Research in Personality, 70, 214–228. 10.1016/j.jrp.2017.08.001 [DOI] [Google Scholar]
- Quintus M, Egloff B, & Wrzus C (2019). Momentary processes predict long-term development in explicit and implicit representations of Big Five traits: An empirical test of the TESSERA framework. Manuscript submitted for publication. [DOI] [PubMed]
- Rauthmann JF (2015). Structuring situational information. European Psychologist, 20, 176–189. 10.1027/1016-9040/a000225 [DOI] [Google Scholar]
- Rauthmann JF, Gallardo-Pujol D, Guillaume EM, Todd E, Nave CS, Sherman RA, … Funder DC (2014). The Situational Eight DIAMONDS: A taxonomy of major dimensions of situation characteristics. Journal of Personality and Social Psychology, 107, 677–718. 10.1037/a0037250 [DOI] [PubMed] [Google Scholar]
- Reitz AK, & Staudinger UM (2017). Getting older, getting better? Toward understanding positive personality development across adulthood. In Specht J (Ed.), Personality development across the lifespan (pp. 219–241). New York, NY: Academic Press. 10.1016/B978-0-12-804674-6.00014-4 [DOI] [Google Scholar]
- Reitz AK, Zimmermann J, Hutteman R, Specht J, & Neyer FJ (2014). How peers make a difference: The role of peer groups and peer relationships in personality development. European Journal of Personality, 28, 279–288. 10.1002/per.1965 [DOI] [Google Scholar]
- Riediger M (2018). Ambulatory assessment in survey research: The multi-method ambulatory assessment project. In Erlinghagen M, Hank K, & Kreyenfeld M (Eds.), Innovation und Wissenstransfer in der empirischen Sozialund Verhaltensforschung. Festschrift für Gert G. Wagner (pp. 85–100). Frankfurt, Germany: Campus Verlag. [Google Scholar]
- Riediger M, & Freund AM (2008). Me against myself: Motivational conflicts and emotional development in adulthood. Psychology and Aging, 23, 479–494. 10.1037/a0013302 [DOI] [PubMed] [Google Scholar]
- Riediger M, Li S-C, & Lindenberger U (2006). Selection, optimization, and compensation as developmental mechanisms of adaptive resource allocation: Review and preview. In Birren JE & Schaie KW (Eds.), Handbook of the psychology of aging (pp. 289–313). Amsterdam, the Netherlands: Elsevier. 10.1016/B978-012101264-9/50016-1 [DOI] [Google Scholar]
- Riediger M, Schmiedek F, Wagner GG, & Lindenberger U (2009). Seeking pleasure and seeking pain: Differences in prohedonic and contra-hedonic motivation from adolescence to old age. Psychological Science, 20, 1529–1535. 10.1111/j.1467-9280.2009.02473.x [DOI] [PubMed] [Google Scholar]
- Robinson MD, & Clore GL (2002). Episodic and semantic knowledge in emotional self-report: Evidence for two judgment processes. Journal of Personality and Social Psychology, 83, 198–215. 10.1037/0022-3514.83.1.198 [DOI] [PubMed] [Google Scholar]
- Rosso AL, Taylor JA, Tabb LP, & Michael YL (2013). Mobility, disability, and social engagement in older adults. Journal of Aging and Health, 25, 617–637. 10.1177/0898264313482489 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sacker A, Worts D, & McDonough P (2011). Social influences on trajectories of self-rated health: Evidence from Britain, Germany, Denmark and the USA. Journal of Epidemiology and Community Health, 65, 130–136. 10.1136/jech.2009.091199 [DOI] [PubMed] [Google Scholar]
- Sander J, Schupp J, & Richter D (2017). Getting together: Social contact frequency across the life span. Developmental Psychology, 53, 1571–1588. 10.1037/dev0000349 [DOI] [PubMed] [Google Scholar]
- Saucier G, Bel-Bahar T, & Fernandez C (2007). What modifies the expression of personality tendencies? Defining basic domains of situation variables. Journal of Personality, 75, 479–503. 10.1111/j.1467-6494.2007.00446.x [DOI] [PubMed] [Google Scholar]
- Schwarz N, Park D, Knäuper B, & Sudman S (1999). Cognition, aging, and self-reports. Philadelphia, PA: Psychology Press. [Google Scholar]
- Seale MS, & Iso-Ahola SE (1988). Determinants of leisure behaviour among retired adults. Therapeutic Recreation Journal, 22, 38–46. [Google Scholar]
- Simonsick EM, Kasper JD, & Phillips CL (1998). Physical disability and social interaction: Factors associated with low social contact and home confinement in disabled older women (The Women’s Health and Aging Study). The Journals of Gerontology Series B, Psychological Sciences and Social Sciences, 53, S209–S217. 10.1093/geronb/53B.4.S209 [DOI] [PubMed] [Google Scholar]
- Sonnenberg B, Riediger M, Wrzus C, & Wagner GG (2012). Measuring time use in surveys - How valid are time use questions in surveys? Concordance of survey and experience sampling measures. Social Science Research, 41, 1037–1052. 10.1016/j.ssresearch.2012.03.013 [DOI] [PubMed] [Google Scholar]
- Wahl H-W, & Gerstorf D (2018). A conceptual framework for studying COntext Dynamics in Aging (CODA). Developmental Review, 50, 155–176. 10.1016/j.dr.2018.09.003 [DOI] [Google Scholar]
- Wettstein M, Schilling OK, & Wahl H-W (2016). “Still feeling healthy after all these years”: The paradox of subjective stability versus objective decline in very old adults’ health and functioning across five years. Psychology and Aging, 31, 815–830. 10.1037/pag0000137 [DOI] [PubMed] [Google Scholar]
- White MP, & Dolan P (2009). Accounting for the richness of daily activities. Psychological Science, 20, 1000–1008. 10.1111/j.1467-9280.2009.02392.x [DOI] [PubMed] [Google Scholar]
- Wolff JK, Brose A, Lövdén M, Tesch-Römer C, Lindenberger U, & Schmiedek F (2012). Health is health is health? Age differences in intraindividual variability and in within-person versus between-person factor structures of self-reported health complaints. Psychology and Aging, 27, 881–891. 10.1037/a0029125 [DOI] [PubMed] [Google Scholar]
- Wrzus C, Hänel M, Wagner J, & Neyer FJ (2013). Social network changes and life events across the life span: A meta-analysis. Psychological Bulletin, 139, 53–80. 10.1037/a0028601 [DOI] [PubMed] [Google Scholar]
- Wrzus C, & Mehl MR (2015). Lab and/or field? Measuring personality processes and their social consequences. European Journal of Personality, 29, 250–271. 10.1002/per.1986 [DOI] [Google Scholar]
- Wrzus C, & Mehl MR (2017). Ecological sampling methods for studying everyday situations. In Funder D, Rauthmann J, & Sherman R (Eds.), The Oxford handbook of psychological situations. New York, NY: Oxford University Press. [Google Scholar]
- Wrzus C, Egloff B, & Quintus M (2019). Context matters: Longitudinal development of self-rated and implicitly measured Big Five traits in younger and older students. Manuscript submitted for publication.
- Wrzus C, & Roberts BW (2017). Processes of personality development in adulthood: The TESSERA framework. Personality and Social Psychology Review, 21, 253–277. 10.1177/1088868316652279 [DOI] [PubMed] [Google Scholar]
- Wrzus C, Wagner GG, & Riediger M (2016). Personality-situation transactions from adolescence to old age. Journal of Personality and Social Psychology, 110, 782–799. 10.1037/pspp0000054 [DOI] [PubMed] [Google Scholar]
- Zenk SN, Kraft AN, Jones KK, & Matthews SA (2019). Convergent validity of an activity-space survey for use in health research. Health & Place, 56, 19–23. 10.1016/j.healthplace.2019.01.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zenk SN, Matthews SA, Kraft AN, & Jones KK (2018). How many days of global positioning system (GPS) monitoring do you need to measure activity space environments in health research? Health & Place, 51, 52–60. 10.1016/j.healthplace.2018.02.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.