

Abstract
Introduction:
Falls are the leading cause of injury-related mortality and morbidity in the elderly. Physical activity plays a key role in the prevention of falls and stimulates postural control. The aim of this study was to compare a general physical activity program for the elderly with a Pilates program to evaluate the effects on balance and on reducing the risk of falling.
Materials and Methods:
Forty-six subjects were enrolled in this study, but only 41 were included in the study. The subjects were divided into 2 groups: Pilates group (P-G) and a group following a nonspecific program of physical activity (Pa-G). Each subject underwent the hand grip test, Berg balance scale test, and posturographic analysis.
Results:
Spearman correlation coefficient showed correlations between the following parameters: BBS versus hand grip test (r = 0.68); BBS versus ellipse surface area (r = −0.75). There were significant differences between groups after the exercise program: both groups showed an improvement in performance but the P-G recorded significantly better results than the Pa-G.
Discussion and conclusions:
This study confirmed that physical activity improves both balance and strength. However, our data show that Pilates has a greater effect on these physical abilities than a general physical activity program.
Keywords: pilates, exercise, falls, balance, posture, physical activity program
1. Introduction
Over the past few decades, life expectancy has gradually increased; as a result, the world population is aging.[1] The scientific literature shows us that life expectancy has increased significantly, and the proportion of elderly in the global population is increasing. Moreover, the number of those aged over 85 years is projected to increase by 2040.[1] Falls are the leading cause of injury-related mortality and morbidity in the elderly.[2,3] In 2008, Sturnieks et al[4] showed the changes in the vestibular, somatosensory, and visual systems that occur as a consequence of aging. Accordingly, some studies have emphasized that these progressive changes slow down information feedback.[5] This causes a reduction in useful information that reaches the posture control centers.[6] Physical activity plays a key role in the prevention of falls as it limits the loss of muscle mass and strength and stimulates postural control; after injury, it also improves recovery.[7–10] Physical activity guidelines for seniors recommend muscle-strengthening activity performed on two or more days per week with at least 150 minutes per week of moderate-intensity aerobic exercise.[11] Some studies have suggested that only specific exercise programs could reduce the risk of falls.[12,13] Such physical activity stimulates reaction time, cognitive performance, sensory stimulation, and social interaction. This contributes to improving neuroplasticity.[14] However, the literature has shown that not all types of physical activity programs can improve balance to an extent that prevents someone from actually falling over.[15,16] Studies in the literature have presented controversial data on which type of exercise may be most effective for this purpose.[17,18] Balance training and leg strength training have been identified as adequate methods to reduce the risk of falling. Balance is essential for moving and standing; therefore, postural training, to stimulate stability, should also have an important role in preventing falls.[19,20] Many studies investigating the risk of falling among the elderly have concluded that exercise is an effective strategy to decrease the risk of falls and improve balance.[18,21] However, the scientific literature does not sufficiently clarify the specific type of physical activity or the minimum intensity required to provide optimal benefits. Human balance depends on coordinated integration of somatosensory, vestibular, and visual input.[22] Some studies indicate that the changes after some exercise programs are lasting and structured; improvements persisted even after ceasing the activity. The literature has shown that Pilates can stimulate balance and improve the postural system.[23,24] Bird et al[25] showed that changes occur in the central nervous system at the level of synaptic connections, with changes in the cortical map and muscle activation strategies. Balance disorders are among the most common causes of falls in older adults and often lead to injury, disability, loss of independence, and limitations.[26] Patti et al[27] explained that 14 weeks of program of Pilates exercise is sufficient to modify posturography.[23] Therefore, it could more efficiently reduce the risk of falls in the elderly. However, there are studies that have shown a limited impact of Pilates on falls.[28,29] The effects may have been overestimated due to the low methodological quality of studies.[30]
1.1. Hypothesis Section
The aim of our randomized controlled trial (RCT) was to compare a general physical activity program for the elderly with a Pilates program to evaluate the effects on balance and on reducing the risk of falling.
2. Materials and methods
2.1. Study design and context
Our study was carried out in compliance with the principles of the Italian Data Protection Act (196/2003) and the Declaration of Helsinki. Written informed consent was obtained from each subject before the participation. The study was inserted in the Adapted Physical Activity Prevention Program which had obtained Ethical Approval (assigned number 553/EC). Forty-six subjects were enrolled in this study. All participants were recruited from the University of Palermo Sports Lab. According to our inclusion criteria, we selected participants who were nontrained healthy individuals with no pain; >55 years’ old; without a positive diagnosis for any disease; and not former professional athletes.[10] The subjects were divided using a 1:1 randomization strategy into two groups: a Pilates group (P-G) and a group following a nonspecific program of physical activity (Pa-G). The allocation sequence was computer generated, with group allocation directed by a research assistant who did not participate in the study (Fig. 1). The Consolidated Standards of Reporting Trials (CONSORT) Statement was set as a standard.[31] Five participants subsequently dropped out of the exercise program in the Pilates group due to incompatibility with working hours and were therefore excluded from the study. The P-G was composed of 18 subjects (4 men and 14 women; age: 63.94 ± 4.37 years; height: 165.91 ± 0.07 cm; weight: 67.82 ± 11.83 kg); the Pa-G was composed of 23 subjects (9 men and 14 women; age: 63.26 ± 4.44 years; height: 153.91 ± 007 cm; weight: 75.78 ± 13.54 kg). Weight was measured to the nearest 100 g (Wunder 960 classic). Height was measured using a portable Seca stadiometer, sensitive to changes of up to 1 cm (Seca 220, Hamburg, Germany). All measurements were performed twice, and the arithmetic mean was recorded for evaluation.[32] The group characteristics are reported in Table 1. The groups were comparable in terms of age. Participants in the P-G completed a Pilates matwork exercise program, whereas the Pa-G group carried out a nonstandardized and equipment-free exercise program that included a sequence of stretching exercises and aerobic exercise (160 minutes of moderate-intensity aerobic activity each week)[11]; both programs were administered for 13 weeks. The Pilates matwork program is described in Table 2.[7,23] In 2016, Patti et al[23] used a similar exercise program to reduce lower back pain. Two screening procedures were managed by an examiner blinded to group assignment at the following times: before the study (T0, baseline) and 13 weeks after the conclusion of the exercise interventions (T1).
Figure 1.
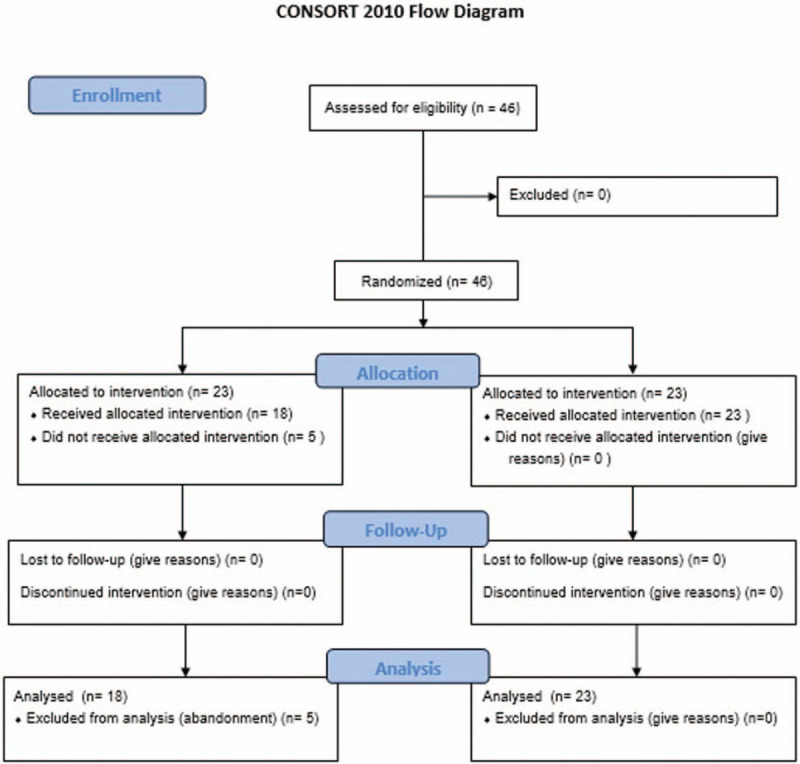
Flowchart of study.
Table 1.
Participants’ characteristics.
| P-G | Pa-G | P | |
| Subjects (n) | 18 | 23 | |
| Age, y | 63.94 ± 4.37 | 63.26 ± 4.44 | ns |
| Height, cm | 165.91 ± 0.07 | 153.91 ± 0.07 | .0001 |
| Weight, kg | 67.82 ± 11.83 | 75.78 ± 13.54 | ns |
Table 2.
| Exercises | Time | Repetitions | Objectives and hints |
| Diaphragmatic breathing exercises | 5 min | ||
| Mobilization of the pelvis and principal joints | 10 min | Retroversion, anterior tilt, and rotation of pelvis; mobilization of the spine and larger joints | |
| Hundreds | 5 min | Repetitions of 30 s with 1 min of recovery between repetitions[22] | Exercise to increase torso stability and abdominal strength. |
| Roll up | 5 min | Repetitions. Exhale and contract the abdominals[22] | Mobilization of the spine. Strengthening the abdominals, the kinetic chain back and hamstring muscles. |
| Single-leg circles with bent leg (basic exercise) | 5 min | Repetitions for pelvis stabilization—Repetitions for mobilization of the hip[22] | Stabilization basin, mobilization of the hip (maximum range of the circle). A breathing cycle for each circle |
| Spine stretch | 5 min | 5 Repetitions + 5 repetitions with 2 min of recovery between repetitions; breathing out, bring your upper body forward contracting your abdominals and avoiding bending of the spine[7] | Lengthening of the muscles of the back legs, torso and neck; mobilization of the spine |
| Rolling like a ball | 5 min | Self-massage of the spine, activation of the abdominal muscles | |
| Single-leg stretch | 5 min | 20 Repetitions | Stabilization of the pelvis, strengthening the abdominals and hip flexors of the neck |
| Diaphragmatic breathing exercises | 5 min |
2.2. Pilates Program
All Pilates matwork sessions were conducted under the supervision of a sport and exercise science specialist with 15 years of experience in the Pilates method. Classes were 50 minutes in duration, the intervention was to be held 3 times per week. All exercises were completed at each session and could be performed at 2 levels of difficulty: basic and intermediate. All exercises were performed on a rubber mat of minimum 3/4 inch thick (Table 2).
2.3. Method of Testing
2.3.1. Posturography analyses
The posturography analyses were administered using the FreeMed system (the FreeStep v.1.0.3 software, produced by Sensor Medica, Guidonia Montecelio, Roma, Italy). The platform's sensors are 24 K gold; this permits high repeatability and reliability.[33] For posturography assessment, each participant performed the Romberg test with standardized positioning: feet placed side-by-side, forming an angle of 30° with both heels separated by 4 cm.[23] The following parameters of the statokinesigram were considered in open-eyes conditions: length of the sway path (SP) of the center of pressure (CoP) and ellipse surface area (ES).[34]
2.3.2. Berg balance scale
The Berg balance scale (BBS) evaluates a subject's performance on 14 items that are common in everyday life. This test is the criterion standard in measuring fall risk and quantitatively evaluating balance. The test is rated through the researcher's observation of individual test performance. Each item is scored from 0 to 4. The total score is obtained by summing the scores of the 14 items. A score of 4 points in a task represents normal performance, with 0 corresponding to inability to perform the task.
2.3.3. Hand grip test
This tested isometric grip strength for hands. Strength was measured using an electronic dynamometer (KERN-MAP). The subject stood with the shoulder adducted and neutrally rotated. The forearm lay along the hips in a neutral position. The best performance of the stronger hand was taken into account.[34,35]
2.3.4. Statistical Analysis
All data were coded in an Excel file. Statistical analysis was performed using StatSoft's STATISTICA software (Windows, version 8.0; Tulsa, OK) and GraphPad Prism software (Windows, version 5.0; La Jolla, CA). The evaluators were “blind” to the data belonged to the specific P-G or Pa-G group. Shapiro–Wilk's normality test was used to analyze the data distribution. Spearman correlation coefficient was used to evaluate the correlation between the tests. The Analysis of variance test (Bonferroni multiple comparison test) or Kruskal-Wallis test (Dunn multiple comparison test) were used, when appropriate, to detect significant differences of performance before and after interventions in both groups (T0 vs T1). In addition, the unpaired t-test (P < .05) or Mann–Whitney test for independent variables were used, when appropriate, to detect significant differences between groups’ performance (P-G vs Pa-G). Descriptive statistical analysis was performed using the mean ± SD and a 95% confidence interval (P < .05).
3. Results
The anthropometric data of the 2 groups are shown in Table 1. In analysis of the BBS and ES, the Shapiro–Wilk normality test showed a non-Gaussian distribution. Conversely, hand grip testing and the length of the SP of the CoP showed a Gaussian distribution. Moreover, Spearman correlation coefficient showed correlations between the following parameters: BBS vs hand grip test (r = 0.68); BBS vs ES (r = −0.75). Graphical representations are shown in Figures 2 and 3. The correlations were significant at P < .05. In the Table 3 showed the analysis of variables before and after interventions in both groups. In P-G, there were significant differences in Ellipse variables (T1 vs T2: P < .05) and in length of SP (T1 vs T2: P < .001). However, in Pa-G showed a difference significative in length of SP (T1 vs T2: P < .001). Subsequently, we evaluated the differences between the performance of the groups. There were no significant differences between the groups at baseline (Table 4; Figures 4–6). However, there were significant differences between the groups after the exercise programs (Table 5). Both groups showed an improvement in performance, but the Pilates group recorded significantly better results than the Pa-G (Table 4; Figures 4–6).
Figure 2.

Pearson correlation index: hand grip test vs BBS.
Figure 3.

Pearson correlation index; ellipse surface area vs BBS.
Table 3.
Analysis of variables before and after interventions in both groups.
| P-G (t0) (n = 18) mean ± SD (95% CI | P-G (t1) (n = 18), mean ± SD (95% CI) | Mean difference | P | Pa-G (t0) (n = 23), mean ± SD (95% CI) | Pa-G (t1) (n = 23), mean ± SD (95% CI) | Mean difference | p values | |
| Hand grip test, kg∗ | 22.06 ± 7.87 | 30.14 ± 6.94 | −8.082 | ns | 19.24 ± 7.04 | 23.18 ± 8.48 | −3.944 | ns |
| BBS | 51.67 ± 2.93 | 54.89 ± 2.92 | −3.222 | ns | 50.39 ± 2.35 | 52.35 ± 2.67 | −10.43 | ns |
| Ellipse, mm2 | 145.1 ± 104.1 | 69.83 ± 40.98 | 75.28 | 0.05 | 158.1 ± 76.32 | 108.6 ± 63.20 | 14.09 | ns |
| Length of sway path, mm∗ | 618.8 ± 162.7 | 501.8 ± 124.7 | 117 | 0.001 | 608.7 ± 82.64 | 563.2 ± 77.57 | 45.49 | 0,001 |
Analysis of variance.
† Kruskal-Wallis test.
Table 4.
Baseline analysis of variables between groups.
| P-G (t0) (n = 18), mean ± SD (95% CI) | Pa-G (t0) (n = 23), mean ± SD (95% CI | Mean difference | P | |
| Hand grip test, kg∗ | 22.06 ± 7.87 | 19.24 ± 7.04 | 2.822 | Ns |
| BBS† | 51.67 ± 2.93 | 50.39 ± 2.35 | 1.275 | ns |
| Ellipse, mm2† | 145.1 ± 104.1 | 158.1 ± 76.32 | −12.99 | ns |
| Length of sway path, mm∗ | 618.8 ± 162.7 | 608.7 ± 82.64 | 10.09 | ns |
BBS = Berg Balance Scale, CI = confidence interval.
Student t test.
Mann–Whitney U test.
Figure 4.

Hand grip analysis.
Figure 6.
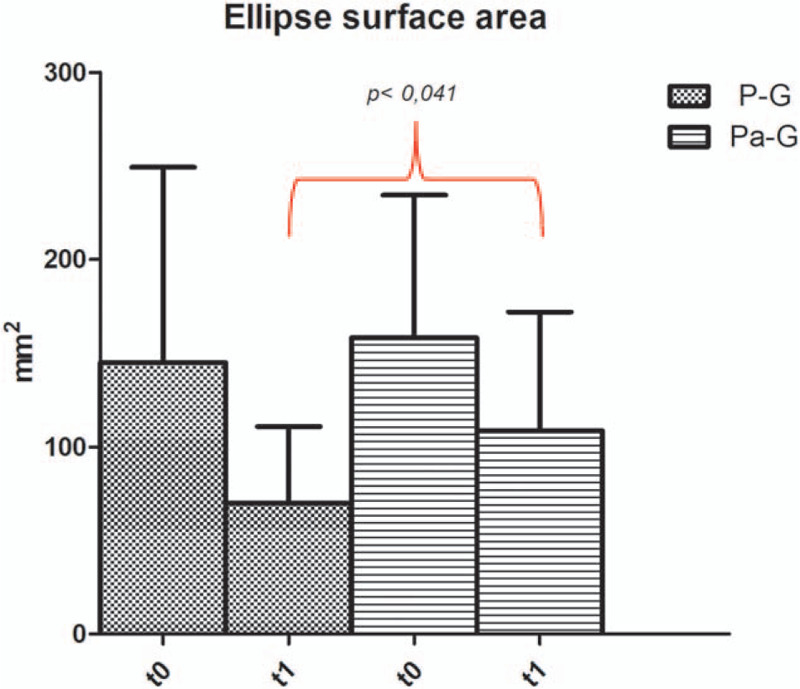
Ellipse surface area analysis.
Table 5.
Post-intervention analysis of variables between groups.
| P-G (t1) (n = 18), mean ± SD (95% CI) | Pa-G (t1) (n = 23), mean ± SD (95% CI | Mean difference | P | |
| Hand grip test, kg∗ | 30.14 ± 6.94 | 23.18 ± 8.48 | 6.960 | .007 |
| BBS† | 54.89 ± 2.92 | 52.35 ± 2.67 | 2.541 | .0003 |
| Ellipse, mm2† | 69.83 ± 40.98 | 108.6 ± 63.20 | −38.80 | .041 |
| Length of sway path, mm∗ | 501.8 ± 124.7 | 563.2 ± 77.57 | 55.58 | ns |
BBS = Berg Balance Scale, CI= =confidence interval.
Student t test.
Mann–Whitney U test.
Figure 5.
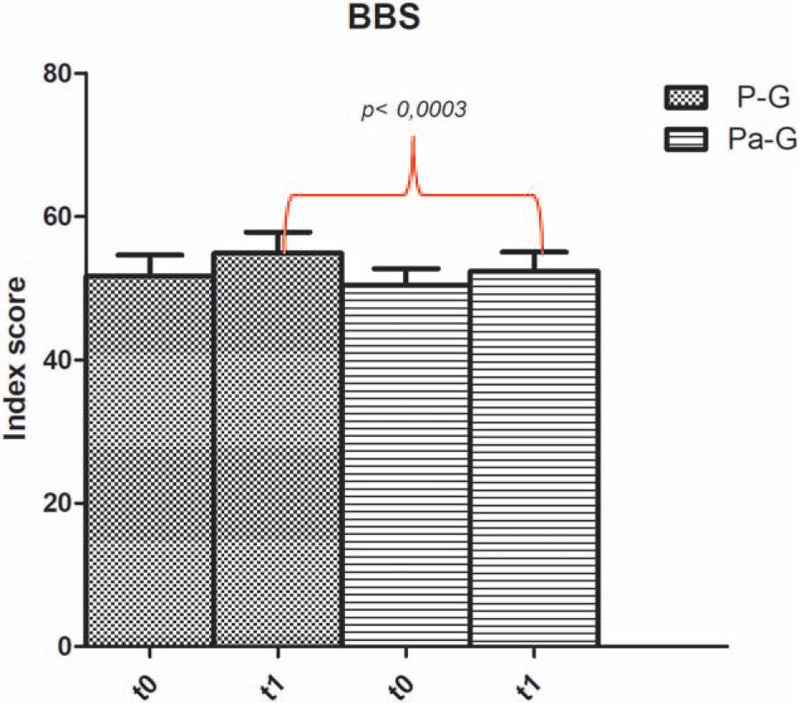
BBS analysis.
4. Discussion
The purpose of our RCT was to investigate the effectiveness of a Pilates exercise program in the prevention of falls with respect to a general physical activity program. Our results confirmed those in the literature.[15,36,37] This study showed that physical activity improves balance and has a positive influence on fall prevention. However, the literature reports conflicting results.[28,29,38] The Pilates method is designed to improve general body flexibility and health, focusing on enhancing core strength, posture, and coordination of breathing through movement.[39] In 2018, Moreno-Segura et al[29] showed that Pilates might also reduce falls among the elderly, but studies on the matter are still too scarce to draw definitive conclusions on the effects of this exercise program. However, the literature underlines how Pilates improves balance and suggests that it may produce greater improvements in terms of balance than other training programs.[29] In this study, we evaluated the sample using a scale for fall risk. The BBS is the criterion standard in measuring fall risk. The Spearman correlation coefficient showed an inverse correlation between the BBS and ES (r = −0.75). This correlation strengthens the relationship between balance and the risk of falls and also proposes that posturographic analysis may be useful in preventing falls. Similarly, the analysis showed a correlation between the BBS and hand grip test results, suggesting a relationship between upper limb strength and balance control. Fujita et al[40] showed results in accordance with those from this study: the authors demonstrated that lower grip strength and dynamic body balancing ability were significant risk factors. Many studies have shown that muscle strength affects balance. However, due to aging and degenerative processes of both the nervous system and the muscular system, the elderly suffer muscle weakness and balance instability.[18,41] Pilates is a training style that significantly affects muscle strength.[42–45] The purpose of our study was to evaluate the effectiveness of a Pilates exercise intervention on balance control and compare it to a general physical activity program. This study provides evidence of the effects of physical activity in improving BBS, hand grip, and posturography variables. However, our data showed that the Pilates program produces greater improvements than a general physical activity program. The Pilates program that we used in our study included both mental and physical elements with specific control and strengthening of the abdominal, paraspinal, and gluteal muscles.[46] Many studies have identified core fitness as a good fall prevention strategy. Both exercise groups showed improvements, but PG showed significantly more improvement than Pa-G. One possible explanation for this is that Pilates’ principles include multiple components and challenge balance, core strength, lower extremity strength, and flexibility. In 2018, Moreno-Segura et al[29] showed conclusions in accordance with our results. However, although the authors identified in Pilates a program that may produce greater improvements in terms of balance than other training approaches oriented to the same end, the effect on falls was not decisive. Nevertheless, PG participants improved their abilities in terms of static and dynamic balance and stability; in addition, the subjects showed improved performance in the BBS, a specific scale to evaluate fall risk. The BBS is the most frequently used scale among the tests utilized for this purpose.[47] Improvements in both performances likely identify a lower risk of falls. This theory is in agreement with the study by Pereira et al.[48] Bird et al's study is interesting. In 2012, the authors suggested that the improvements in balance persisted and that this could be explained by changes occurring in the central nervous system at the level of synaptic connections and, therefore, with different muscle activation strategies.[25] Other studies have also shown that strengthening from the practice of Pilates could influence balance capabilities.[49] We propose that Pilates program creates the conditions for a greater postural improvement than a general physical activity program and this could ultimately reduce the risk of falling in the elderly. The limits of this study are identified on the age of the sample taken into consideration; the subjects analyzed had an age at the limit with old age, therefore without important balance deficits. Second, the number of subjects was small. Furthermore, the Pilates group further decreased in number after the abandonment of 5 subjects due to their inability to participate in the Pilates program due to personal incompatibilities on the time of the Pilates lesson
5. Conclusion
In conclusion, our data provide evidence that a 13-week program of physical exercise is sufficient to modify balance but that the Pilates program seems to have greater effectiveness. Definitely, our results suggest that Pilates could be considered for stabilization training and to reduce the risk of falls in the elderly.
Author contributions
Antonino Patti and Antonio Palma designed the study, discussed the results and drafted the paper; Daniele Zangla performed the testing and participated in drafting paper; Francesco Fischietti, Nese Sahin and Cataldi Stefania helped with discussion of results and overviewed previous researches; Antonio Palma and Gioacchino Lavanco did statistical analyses and drafted the paper.
Conceptualization: Antonino Patti, Antonio Palma.
Data curation: Daniele Zangla, Fatma Nese Sahin, Stefania Cataldi, Francesco Fischietti.
Formal analysis: Gioacchino Lavanco.
Investigation: Antonino Patti, Daniele Zangla, Fatma Nese Sahin, Stefania Cataldi, Antonio Palma.
Methodology: Antonino Patti, Fatma Nese Sahin, Francesco Fischietti.
Supervision: Gioacchino Lavanco, Antonio Palma.
Writing – original draft: Antonino Patti, Gioacchino Lavanco, Antonio Palma, Francesco Fischietti.
Footnotes
Abbreviations: BBS = Berg Balance Scale; CoP = Coordinates of the center of pressure; ES = Ellipse surface area; P-G = Pilates Group; Pa-G = Physical activity Group; RCT = Randomized Controlled Trial; RTS = Stimulates Reaction Times; SP = Length of sway path of the CoP.
How to cite this article: Patti A, Zangla D, Sahin FN, Cataldi S, Lavanco G, Palma A, Fischietti F. Physical exercise and prevention of falls. Effects of a Pilates training method compared with a general physical activity program: a randomized controlled trial. Medicine. 2021;100:13(e25289).
The authors report no conflicts of interest.
Ethics approval and consent to participate: The study was inserted in the Adapted Physical Activity Prevention Program which had obtained Ethical Approval (assigned number 553/EC). This study was performed in compliance with the Declaration of Helsinki, the European Union recommendations for Good Clinical Practice (document 111/3976/88, July 1990), and the principles of the Italian data protection act (196/2003) were observed. Informed consent was obtained from all individual participants included in the study.
Consent to publish: All authors give consent for publication
Availability of data and materials: The datasets generated and/or analyzed during the present study are not available [REASON WHY DATA ARE NOT PUBLIC], but are available from the corresponding author on reasonable request.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
- [1].Shryock HS, Siegel JS, Larmon EA. Census USBot The Methods and Materials of Demography U S Department of Commerce, Bureau of the Census 1980. [Google Scholar]
- [2].Stenhagen M, Nordell E, Elmstahl S. Falls in elderly people: a multifactorial analysis of risk markers using data from the Swedish general population study ’Good ageing in Skane’. Aging Clin Exp Res 2013;25:59–67. [DOI] [PubMed] [Google Scholar]
- [3].Patti A, Mammina C, Cataldo MC, et al. Relationship between hypertension and accidental falls: the potential positive effects of physical exercise on blood pressure. J Biol Res (Italy) 2015;88:113–4. [Google Scholar]
- [4].Sturnieks DL, St George R, Lord SR. Balance disorders in the elderly. Neurophysiol Clin 2008;38:467–78. [DOI] [PubMed] [Google Scholar]
- [5].Tuunainen E, Jantti P, Poe D, et al. Characterization of presbyequilibrium among institutionalized elderly persons. Auris Nasus Larynx 2012;39:577–82. [DOI] [PubMed] [Google Scholar]
- [6].Tuunainen E, Poe D, Jantti P, et al. Presbyequilibrium in the oldest old, a combination of vestibular, oculomotor and postural deficits. Aging Clin Exp Res 2011;23:364–71. [DOI] [PubMed] [Google Scholar]
- [7].Patti A, Bianco A, Karsten B, et al. The effects of physical training without equipment on pain perception and balance in the elderly: A randomized controlled trial. Work 2017;57:23–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Faraldo-Garcia A, Santos-Perez S, Rossi-Izquierdo M, et al. Posturographic limits of stability can predict the increased risk of falls in elderly patients with instability? Acta Otolaryngol 2016;136:1125–9. [DOI] [PubMed] [Google Scholar]
- [9].Campbell AJ, Robertson M, Gardner MM, et al. Randomised controlled trial of a general practice programme of home based exercise to prevent falls in elderly women. BMJ 1997;315:1065–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Bianco A, Patti A, Bellafiore M, et al. Group fitness activities for the elderly: an innovative approach to reduce falls and injuries. Aging Clin Exp Res 2014;26:147–52. [DOI] [PubMed] [Google Scholar]
- [11].Piercy KL, Troiano RP, Ballard RM, et al. The Physical Activity Guidelines for Americans. JAMA 2018;320:2020–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Nelson ME, Rejeski WJ, Blair SN, et al. Physical activity and public health in older adults: recommendation from the American College of Sports Medicine and the American Heart Association. Med Sci Sports Exerc 2007;39:1435–45. [DOI] [PubMed] [Google Scholar]
- [13].Borges EG, Cader SA, Vale RG, et al. The effect of ballroom dance on balance and functional autonomy among the isolated elderly. Arch Gerontol Geriatr 2012;55:492–6. [DOI] [PubMed] [Google Scholar]
- [14].Heuninckx S, Wenderoth N, Swinnen SP. Systems neuroplasticity in the aging brain: recruiting additional neural resources for successful motor performance in elderly persons. J Neurosci 2008;28:91–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Skelton D, Dinan S, Campbell M, et al. Tailored group exercise (Falls Management Exercise—FaME) reduces falls in community-dwelling older frequent fallers (an RCT). Age Ageing 2005;34:636–9. [DOI] [PubMed] [Google Scholar]
- [16].Bellafiore M, Battaglia G, Bianco A, et al. Improved postural control after dynamic balance training in older overweight women. Aging Clin Exp Res 2011;23:378–85. [DOI] [PubMed] [Google Scholar]
- [17].Gine-Garriga M, Roque-Figuls M, Coll-Planas L, et al. Physical exercise interventions for improving performance-based measures of physical function in community-dwelling, frail older adults: a systematic review and meta-analysis. Arch Phys Med Rehabil 2014;95:753–69. e753. [DOI] [PubMed] [Google Scholar]
- [18].Thomas E, Battaglia G, Patti A, et al. Physical activity programs for balance and fall prevention in elderly: a systematic review. Medicine 2019;98:e16218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Melzer I, Benjuya N, Kaplanski J. Postural stability in the elderly: a comparison between fallers and non-fallers. Age Ageing 2004;33:602–7. [DOI] [PubMed] [Google Scholar]
- [20].Baczkowicz D, Szczegielniak J, Proszkowiec M. Relations between postural stability, gait and falls in elderly persons—preliminary report. Ortop Traumatol Rehabil 2008;10:478–85. [PubMed] [Google Scholar]
- [21].Fernandez-Arguelles EL, Rodriguez-Mansilla J, Antunez LE, et al. Effects of dancing on the risk of falling related factors of healthy older adults: a systematic review. Arch Gerontol Geriatr 2015;60:1–8. [DOI] [PubMed] [Google Scholar]
- [22].Winter DA, Patla AE, Frank JS. Assessment of balance control in humans. Med Prog Technol 1990;16:31–51. [PubMed] [Google Scholar]
- [23].Patti A, Bianco A, Paoli A, et al. Pain perception and stabilometric parameters in people with chronic low back pain after a pilates exercise program: a randomized controlled trial. Medicine 2016;95:e2414. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Casonatto J, Yamacita CM. Pilates exercise and postural balance in older adults: a systematic review and meta-analysis of randomized controlled trials. Complement Ther Med 2020;48:102232. [DOI] [PubMed] [Google Scholar]
- [25].Bird ML, Hill KD, Fell JW. A randomized controlled study investigating static and dynamic balance in older adults after training with Pilates. Arch Phys Med Rehabil 2012;93:43–9. [DOI] [PubMed] [Google Scholar]
- [26].Cuevas-Trisan R. Balance problems and fall risks in the elderly. Clin Geriatr Med 2019;35:173–83. [DOI] [PubMed] [Google Scholar]
- [27].Irez GB, Ozdemir RA, Evin R, et al. Integrating pilates exercise into an exercise program for 65+ year-old women to reduce falls. J Sports Sci Med 2011;10:105–11. [PMC free article] [PubMed] [Google Scholar]
- [28].Gabizon H, Press Y, Volkov I, et al. The effects of pilates training on balance control and self-reported health status in community-dwelling older adults: a randomized controlled trial. J Aging Phys Act 2016;24:376–83. [DOI] [PubMed] [Google Scholar]
- [29].Moreno-Segura N, Igual-Camacho C, Ballester-Gil Y, et al. The effects of the pilates training method on balance and falls of older adults: a systematic review and meta-analysis of randomized controlled trials. J Aging Phys Act 2018;26:327–44. [DOI] [PubMed] [Google Scholar]
- [30].Barker AL, Bird ML, Talevski J. Effect of pilates exercise for improving balance in older adults: a systematic review with meta-analysis. Arch Phys Med Rehabil 2015;96:715–23. [DOI] [PubMed] [Google Scholar]
- [31].Schulz KF, Altman DG, Moher D, et al. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. PLoS Med 2010;7:e1000251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Patti A, Bianco A, Sahin N, et al. Postural control and balance in a cohort of healthy people living in Europe: an observational study. Medicine 2018;97:e13835. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Patti A, Bianco A, Messina G, et al. Evaluation of podalic support and monitoring of balance control in children with and without dyslexia: a pilot study. Sustainability (Switzerland) 2020;12: [Google Scholar]
- [34].Patti A, Maggio MC, Corsello G, et al. Evaluation of fitness and the balance levels of children with a diagnosis of juvenile idiopathic arthritis: a pilot study. Int J Environ Res Public Health 2017;14: [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Bianco A, Jemni M, Thomas E, et al. A systematic review to determine reliability and usefulness of the field-based test batteries for the assessment of physical fitness in adolescents—The ASSO Project. Int J Occup Med 2015;28:445–78. [DOI] [PubMed] [Google Scholar]
- [36].Fan C. Exercise for preventing falls in older people living in the community: summary of a cochrane review. Explore 2020;16:274. [DOI] [PubMed] [Google Scholar]
- [37].Poulton G, Funderburke Matney B, Williams T, et al. Exercise to reduce falls in older adults. Am Fam Phys 2020;101:42–3. [PubMed] [Google Scholar]
- [38].Patti A, Bianco A, Paoli A, et al. Effects of pilates exercise programs in people with chronic low back pain: a systematic review. Medicine 2015;94:e383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [39].Lee SM, Lee CH, O'Sullivan D, et al. Clinical effectiveness of a pilates treatment for forward head posture. J Phys Ther Sci 2016;28:2009–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [40].Fujita K, Kaburagi H, Nimura A, et al. Lower grip strength and dynamic body balance in women with distal radial fractures. Osteoporos Int 2019;30:949–56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [41].Rubenstein LZ. Falls in older people: epidemiology, risk factors and strategies for prevention. Age Ageing 2006;35: suppl 2: ii37–41. [DOI] [PubMed] [Google Scholar]
- [42].Oliveira LC, Pires-Oliveira DA, Abucarub AC, et al. Pilates increases isokinetic muscular strength of the elbow flexor and extensor muscles of older women: A randomized controlled clinical trial. J Bodyw Mov Ther 2017;21:2–10. [DOI] [PubMed] [Google Scholar]
- [43].Gomes CS, Pedriali FR, Urbano MR, et al. The effects of Pilates method on pelvic floor muscle strength in patients with post-prostatectomy urinary incontinence: a randomized clinical trial. Neurourol Urodyn 2018;37:346–53. [DOI] [PubMed] [Google Scholar]
- [44].Aibar-Almazan A, Martinez-Amat A, Cruz-Diaz D, et al. The influence of pilates exercises on body composition, muscle strength, and gait speed in community-dwelling older women: a randomized controlled trial. J Strength Cond Res 2020. [DOI] [PubMed] [Google Scholar]
- [45].Park JH, Kim HJ, Choi DH, et al. Effects of 8-week Pilates training program on hamstring/quadriceps ratio and trunk strength in adolescent baseball players: a pilot case study. J Exerc Rehabil 2020;16:88–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [46].Sorosky S, Stilp S, Akuthota V. Yoga and pilates in the management of low back pain. Curr Rev Musculoskelet Med 2008;1:39–47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [47].Avdic D, Skrbo A. Co-relation between risk factors of falls down and the Berg balance scale in elderly people (third age). Bosn J Basic Med Sci 2003;3:49–55. [DOI] [PubMed] [Google Scholar]
- [48].Pereira VV, Maia RA, Silva SM. The functional assessment Berg Balance Scale is better capable of estimating fall risk in the elderly than the posturographic Balance Stability System. Arq Neuropsiquiatr 2013;71:5–10. [DOI] [PubMed] [Google Scholar]
- [49].Vieira ND, Testa D, Ruas PC, et al. The effects of 12 weeks Pilates-inspired exercise training on functional performance in older women: a randomized clinical trial. J Bodyw Mov Ther 2017;21:251–8. [DOI] [PubMed] [Google Scholar]