

ABSTRACT
Objectives: Bney Brak city tops Israel’s COVID-19 infection rate and mortality. Before the Jewish New Year (two-day gathering) SARS-CoV-2 PCR positivity rates were 17.6% and reached 28.1% two weeks later Taffix – an innovative nasal powder creates a protective gel over the nasal mucosa blocking viruses from infecting nasal cells, was tested for efficacy in preventing SARS CoV2 infection.
Methods: In a prospective users survey, 243 members of an ultra-orthodox community that participated in two days prayers were followed for 14 days following this ‘superspread’ event. Eighty-three used Taffix throughout holiday’s prayers and the following two weeks (ITT). Eighty-one used it regularly (PP). Two used it rarely if at all. The remaining 160 did not use Taffix.
Results: After 14 days, 0/81 (0%) of (PP) Tafffix users, 2/83 (2.4%) of (ITT) Taffix users and 16/160 (10%) nonusers were infected. Odds ratio for infection among Taffix users was 0.22, a reduction of 78% (95%CI 1%–95%). No side effects reported.
Conclusion: Taffix could be an additional tool against COVID19 spread, in addition to recommended safety measures. This is the first time that a prevention measure of SARS-CoV-2, beyond the use of masks, has proved effective.
KEYWORDS: SARS-CoV-2, prevention, Hypromellose, nasal spray, low pH
1. Introduction
On September 18, 2020, Israel was a world leader in the number of new COVID-19 cases per million citizens. The infection rate among its ultra-orthodox communities was double that of the general population. In the city of Bney Brak (population ~200000, mostly ultra-orthodox jews) on September 30th there were 23.6 confirmed COVID-19 patients per 1000 citizens, and a total of 4741 active confirmed cases [1]. Of note, the mortality rate in Israel was 182 per million citizens while the calculated mortality in Bney Brak is more than double that: 380 per million.
In 2020, the New Year holiday (Rosh Hashana) began on the evening of September 18 and lasted for two days spent in closed quarter synagauges ending in large celebrations involving big crowds. This event raised concern for a potential post-mass gathering outbreak.
The objective of this study was to test the efficacy of Taffix nasal spray in preventing the potential after effects of a super spreader event caused by mass-gathering ahead of the Jewish New Year.
Indeed, in mid-September just before Rosh Hashana (Jewish New Year) there were about 17.6% positivity rates in the city of Bney Brak, and those actually climbed to 28.1% two weeks later [1] A similar trend was identified in other ultra-orthodox communities both in Israel and in greater NYC [2].
Viral entry through the nasal mucosa is considered a main mechanism in SARS-CoV-2 infection [3]. .Taffix’s main ingredient – Hydroxypropyl methyl cellulose, (Hypromellose or HPMC) is a muco-adhesive gel-forming cellulose derivative. Upon reaching the nasal mucosa HPMC is known to absorb fluids and create a micron-sized gel [4] . The gel covers the nasal cells and prevents viruses from engaging with the receptors that are necessary for the viral penetration into the cells. Additionally, Taffix creates a local acidic microenvironment of pH 3.5 on mucosal surfaces, which remains stable for up to 5 h. An acidic microenvironment in the nose was shown to prevent multiple respiratory viruses such as N1H1 influenza and Rhinoviruses and recently SARS-C0V-2 from infecting cells [5,6].
Taffix has been tested in three in vitro studies to gauge its effectivity in blocking and disabling respiratory viruses SARS-CoV-2 and H1N1 influenza and Lentivirus.
The purpose of the study of the SARS-CoV-2 study was to test whether the Taffix can form a protective barrier against this virus. Using qRT-SARS-CoV-2 PCR techniques and plaque essay Taffix™ treatment reduced the amount of viral RNA by more than 4 logs [6]
The purpose of the H1N1 study was to test the direct effect of the pH of different Taffix formulations on H1N1 virus’ ability to reduce the viability of MDCK cells. MDCK cells were treated with saline, Hypromellose, or Taffix with or without virus. H1N1 virus pretreated with saline for 5 minutes reduced cell viability to 27%. Pretreatment of viruses with Hypromellose alone (pH-6.8) reduced cell viability to 37% while pretreatment of viruses with Taffix (low pH) for 5 minutes resulted in 88% cell viability, attesting to ability of Taffix to disable aggressive respiratory viruses. Another study performed with Lentivirus containing a green fluorescent reporter which was used as a model virus, showed a significant reduction in cell infectivity. (supplementary information 1and 2)
Taffix – is an acidified Hypromellose nasal powder spray inhaler approved for sale and used for prevention of respiratory viral infections. Taffix received CE marketing approval (DE/CA09/0760/N18/001) and the Israeli Ministry of Health marketing authorization (Amar- 33010001) and other countries. Taffix is sold in Israel since early July 2020 and in over 15 countries in Europe and South America reaching hundreds of thousands of users. No reports of adverse events were registered in the post-marketing database kept in compliance with regulatory requirements.
To assess real-life effect of Taffix in reducing SARS-CoV-2 infection rates following an anticipated mass social gathering in closed environment during the Rosh Hashana holiday, we conducted a prospective user survey at an ultra-orthodox synagogue in Bney Brak, a highly endemic community.
2. Materials and methods
This is a prospective user survey of a commercially available product. Taffix (a powder nasal spray comprised HPMC, citric acid, sodium citrate, benzalkonium chrloride and menthol manufactured by Nasus Pharma. Israel) .
We collaborated with a medium-sized synagogue community consisting of some 250 members. Based on a pre-prepared survey procedure all members of the community received a preliminary notification inviting them to participate in the survey. . Critical to the cooperation of the community members and their individual compliance, was the strong support and encouragement of the spiritual leadership of the community: the Rabbi and the wardens (Gabbaim). Typically, in ultra-orthodox communities – this community is very close knit and its members are well familiar with each other as well as to well known to the leaders of the community. The synagogue serves as the center around which the community day lives revolves. Importantly, it was clarified to the volunteers that Taffix offers an extra layer of protection and does not replace the mandatory use of masks. This was clearly and repeatedly explained to all participants. Though a user survey of a commercially available product does not require Ethics committee approval all participant signed an informed consent. (supplementary information 3)
Of note: At this synagogue members could not enter or remain indoors without properly wearing a mask throughout the whole of the services. The prayer room was divided to ‘capsules’ and every effort was made to prevent mingling of people beyond their allocated capsule.
Members of the community who expressed their interest in using Taffix throughout Rosh Hashana prayers and the following two weeks were eligible to collect a Taffix bottle at the synagogue the day before Rosh Hashana prayer and received written instruction on the proper usage of the device. Family members residing in the same house hold were also eligible to receive Taffix bottles (one each). The volunteers committed to use Taffix whenever encountering a large social interaction and reapply it every five hours whenever they were leaving their residence for the following two weeks. Weekly reminders to all participants were sent directly through the community e-mail system and close attention and monitoring was carried out to substantiate the number of confirmed (SARS-CoV-2 PCR tests offered freely in the city) new cases in the community
All participants declared at the beginning of the study that they have not contracted COVID before.
SARS-CoV-2 PCR testing (free in Israel) was performed based on clinical symptoms or in cases of a contact with a verified COVID case, and in all house hold members of a verified COVID case.
By the 14 day after the Rosh Hashana holiday the wardens of the synagogue followed up each family with a personal phone interview. Members and their families were asked to report whether they have used Taffix, how often and under what circumstances they used it, and whether there were new cases of COVID-19 infection since Rosh Hashana confirmed by SARS-CoV-2 PCR testing and whether there were any adverse events while using Taffix. All information from the phone interview was recorded and summarized. Information about the total number of confirmed new COVID-19 cases in the rest of the community was also collected and confirmed. Confirmed cases were defined as all SARS-CoV-2 PCR positive cases during days 1–14 of the follow up period. Classification of a positive case was based only on positive SARS-CoV-2 PCR test across the two groups of users and non-users. At that time period serological testing was not available freely and was not performed.
3. Statistical methods
The analysis of the results was performed first on the ITT (Intent-to-treat) population data (All members who used Taffix) and then on the PP (Per-Protocol) population. (members who used Taffix regularly according to instruction)
The Fisher’s exact test for the comparison of two proportions (from independent samples), expressed as a percentage, was applied to compare the contagion rate between Taffix users and none users.
Fisher’s exact test is used to calculate an exact P-value for a 2 × 2 frequency table with small number of expected frequencies.
All tests are two-tailed, and a p-value of 5% or less is considered statistically significant.
The data were analyzed using the SAS ® version 9.4 (SAS Institute, Cary North Carolina).
4. Results
Overall, 243 members of the Synagogue participated in the two days holidays prayers (at least seven hours spent in the synagogue each day in a closed room). The day before Rosh HaShana 113 Taffix bottles were collected. Of the 243 members, 83 (34%), men women and children above the age of 12 years, (as per Taffix indication) reported Taffix use, of which 81 (98%) reported per protocol use instructed before entering a populated area and every 5 hours. Two (2%) members used Taffix ‘once or twice’ throughout the 14 days period160 (66%) members of the community from this population of families, either did not collect the Taffix at all or collected it and did not use it at all, not even once.
The ITT group (83 users) comprised of 29 (35%) females and 54 males (65%), and the non users group of 82 (51%) females and 78 (49%) males. The two out of 83 ITT group who did not use Taffix as instructed were males (out of protocol).
28 users (33.7%) were below age 18 though as per Taffix instruction for use only children above age 12 could use Taffix. In the non-users group 46.9% were below age 18. 66.3% of the users were adults (18–40y: 44.6%, 40–60y-18.1% and 3% above 60) and 53.1% in the non users group. Of 243 members of the community, eighteen (7%) were confirmed as new SARS-CoV-2 infections during the 14 days following Rosh Hashana based on positive SARS-CoV-2 PCR test: Among the eighteen new confirmed cases sixteen (89%) of them did not collect or used Taffix, two (11%) collected Taffix but did not adhere to recommended use, that being only once or twice throughout the whole two weeks period. One of them was diagnosed 2 days after Rosh Hashana (possibly exposed prior to the beginning of the survey). All 81 members who used Taffix regularly according to the instruction for use were not infected at all during the study period of 14 days following Rosh Hashana.
In the ITT population, 2/83 (2.4%) of Taffix users and 16/160 (10%) of Taffix non-users were infected. The odds ratio for SARS-CoV-2 infection in Taffix users were 0.22 (0.05–0.99, Mid P exact = 0.028) and therefore a reduction of 78% (95%CI 1%-95%) in odds of infection.
In the PP population, 0/81 (0%) of the Taffix users and 16/160 (10%) of the Taffix non-users were infected. The odds ratio for SARS-CoV-2 infection in Taffix users were 0 (0.00–0.38, Mid P exact <0.001). (See Figure 1 for the Rate of positive SARS-CoV-2 PCR tests in the city of Bney Brak and in Israel following mass gathering events on Jewish New Year, September 18–October 1st.)
Figure 1.
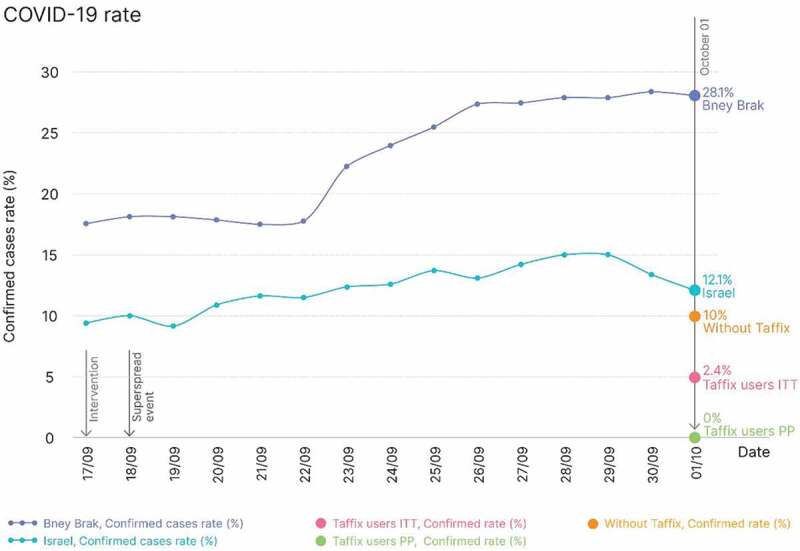
Rate of positive SARS-CoV-2 PCR tests in the city of Bney Brak and in Israel following mass gathering events on Jewish New Year, September 18–October 1st
There were no reports of side effects and most users commented on the ease of use and had no problem in adapting the use of Taffix to their daily routine.
5. Discussion
This study shows a significant reduction in infection rate among people who used Taffix for primary prevention of SARS-CoV-2 infection, despite high-risk exposure and reduction of above 4 fold in the risk of infection. Primary prevention in the context of a viral epidemic refers to the ability to prevent persons from being infected. In general, primary prevention can be achieved through measures such as altering risky behavior, vaccination, pharmacotherapy, and other measures.
During most of the COVID 19 pandemic health care organizations and authorities, for lack of a better alternatives, had to refer to centuries-old measures such as social distancing (the equivalent of the medieval ‘quarantine’ [7], the use of masks by the general public [8] and hygiene. During the last year unparalleled efforts were made to develop vaccines – perhaps the only true primary prevention therapeutic modality using modern day technology. A look at the list of drugs approved by Emergency Use Authorization by FDA indicates that with the exception of vaccine all approved drugs, whether antivirals, anti neoplastic or immune modulating, were aimed at the complications of COVID-19 disease in moderate to severe disease [9]. Most of the scientific work was focused on ameliorating disease severity and reducing mortality. Very few primary prevention measures were suggested and evaluated such as vitamin D, Hydroxy Chloroquine and diet.
The role of Vit D in primary prevention of COVID-19 and in ameliorating disease severity and mortality is still not clear: Vitamin D may enhance innate and adaptive immunity. Because antigen-presenting cells have the ability to synthesize 1,25-dihydroxyvitamin D from 25-hydroxyvitamin D, it has been postulated that vitamin D3 supplementation could improve the function of macrophages and dendritic cells, thereby ameliorating overall immune response. Illie et al reported negative correlations between mean levels of vitamin D in each country and the number of COVID-19 cases/1 M, and mortality. Vitamin D levels were severely low in the aging population especially in Spain, Italy and Switzerland. This is also the most vulnerable group of the population in relation to COVID-19 [10]. Mordaca reviewed Vitamin D ‘s many mechanisms by which it reduces the risk of microbial infection and death, including physical barrier, cellular natural immunity, and adaptive immunity. Vitamin D supplementation has shown favorable effects in viral infections including influenza and HIV. However he concluded that the effects of vitamin D supplementation during COVID-19 infection sill remain controversial [11]. On 17 December 2020, the National Institute for Health and Care Excellence (NICE), in collaboration with Public Health England and the Scientific Advisory Committee on Nutrition, published an updated rapid review of recent studies on vitamin D and COVID-19. Their recommendations support the current government advice, revised in April, 2020, during the first lockdown in the UK, for everyone to take vitamin D supplements to maintain bone and muscle health during the autumn and winter months however as for prevention of COVID-19 infection the panel concluded that there is insufficient evidence to support this claim at this time [12].
The role of Hydroxychloroquine (HCQ) and chloroquine (CQ) during the COVID-19 epidemic was rightly termed: ‘The never ending story.’ [13]. The antiviral effects of CQ and HCQ have been demonstrated in vitro due to their ability to block viruses like coronavirus SARS in cell culture. CQ and HCQ have been proposed to reduce immune reactions to infectious agents, inhibit pneumonia exacerbation, and improve lung imaging investigations. CQ analogs have also revealed the anti-inflammatory and immunomodulatory effects in treating viral infections and related ailments. . Hydroxychloroquine was advocated as an effective primary prevention pharmacotherapy: In a recently published systematic review and meta-analysis Lewis et al [14] looked at the evidence for primary prevention of COVID-19 with HCQ among health care workers. and concluded that although pharmacologic prophylaxis is an attractive preventive strategy against COVID-19, the current body of evidence failed to show clinical benefit for prophylactic hydroxychloroquine and showed a higher risk of adverse events when compared to placebo or no prophylaxis.
Microbiome’s influence on human health is attracting the interests of scientists and the public alike. In the context of COVID-19, the higher risk of disease severity and mortality associated with Obesity, Diabetes and pregnancy serves as another indirect indicator that microbiome differences associated with genetic, ethnic and cultural background could explain some of the additional risk associated with COVID-19 in certain patients groups [15] . These facts makes it critical to consider both how the microbiome, shaped by biosocial processes, affects susceptibility to the coronavirus and, conversely, how COVID-19 disease and prevention measures may affect the microbiome. This knowledge may prove key in prevention and treatment, and long-term biological and social outcomes of this pandemic. This issue remained open as additional studies are required to deepen our understanding on this potentially important topic [16].
On this background, the approach of primary prevention in the nasal cavity suggested here by Taffix is novel and may have significant implications on public health:
We conducted a prospective user survey in a densely populated city, during peak epidemic period with high incidence of transmission ahead of what was perceived to be a super-spreading event during the Jewish Rosh Hashana prayers. Based on prior in vitro studies conducted by the developers that showed high viricidal activity of the Taffix against SARS-CoV-2 (6) the prospective users survey was performed to gauge the real life effect of Taffix in preventing further outbreak of COVID-19 disease before an event that involved mass gathering of people. Users reported a substantially lower infection rates compared with persons from the same community with similar exposure. This significant reduction despite high risk exposure suggests significant effectiveness of Taffix in prevention of SARS-CoV-2 infection and reduction of above 4-fold in the risk of infection. Of note in this time period the number of new cases in the city of Bney Brak increased by 1.6 folds as positivity rates went from 17.6% to 28.4.
Comparison of the demographics between the users and non users need some explanation:
The ratio of females to males among the users group (35%-65%) is probably influenced by the fact that Taffix is not recommended for use in pregnant and breast feeding women without prior consultation with their physician. The average birth rate in Israel orthodox community is 6.6 children per woman, in comparison to 2.7 in non-orthodox population [17]- and could explain the under representation of females in the user’s group. The under representation of female among the user’s group should actually strengthen the finding of our study since women in the city of Bney Brak were found to have a significantly less prone to contracting COVID:19 A serological survey in Beney Beraq – A Joint Project of the CBS, Israel Ministry of Health, Gertner Institute and Bney Beraq Municipality [18] found a significant difference between males and females positive serological testing for SARS-CoV-2: 12.1% vs 6,2%. This survey included some 20000 participants representative of the total inhabitants of the city. Serological results were found to be highly correlated to prior SARS-CoV-2 PCR testing . One would expect higher risk of infection among a group were males are over represented – this was not the case in our survey.
Another age group that was precluded from being properly represented in the user group was the age group below 18 years of age – while among the non-users children below age 18 comprise some 47% - (similar to the general demographics in the city of Bney Brak 48% [19]) of the group – only 33.6% of the users were below 18 since Taffix is not recommended for children below the age of 12. There are several limitation of the study that should be discussed: Our results could be influenced by selection bias whereby people who were more concerned about the possibility of infection would choose to use any additional protection offered to them and might be more careful in observing social distancing and use of masks.
While this certainly is a possibility several points should be considered: 1. Prayers in the synagogue were performed in compaince with safety measures such as masks and social distancing. (see methods). 2. Even in countries where the use of masks and social distancing was adhered to and enforced- the infection rate dropped dramatically but did not reach anything near zero infection rate – attesting the relative but not absolute protection of these measures [20]. 3. On a community level even reducing infection rate among people who are more aware of the risks and are not fully protected due to the limitation of the current safety measures and extremely high prevalence in the community- can significantly lower the numbers of patients and the risks associated with contracting the disease. 4. These results suggest further that Taffix provided protection to people who used it as instructed, not only in the community gathering but also at home, where they did not wear a mask, even when they had an infected family member leaving in the same household.
Additional limitation of this user survey might be the relatively small size of the community and the under-representation of women of childbearing age and teen agers in the users group compared to the non-users explained above. As such conclusion with regards to these age groups should be considered more carefully. Obviously, a prospective clinical study will enrich our understanding of the relative efficacy and the specific circumstances where Taffix will be most efficient in preventing infection. That being said the results of this user survey indicate that among users of Taffix there was a significantly lower infection rate with SARS-CoV-2 infection.
6. Conclusion
Our prospective user survey showed lower SARS-CoV-2 infection rates in Taffix users during a high risk mass gathering. No adverse events were reported. Further evaluation by controlled clinical trials will be helpful in defining more precisely target populations and means of encouraging adherence.
To our knowledge this is the first time that any measure to prevent infection in SARS-CoV-2 virus was proven effective beyond the use of masks. Until such time that global vaccination will be achieved – strengthening the current safety measure could be meaningful in curbing the spread of infection. Given the excellent safety profile of Taffix and its significant efficacy in preventing infection following what is defined as high-risk infection event – it seems that this additional layer of protection may have a role in reducing the risks of infection. . While our results are based on real life survey – the significant difference between users and non users of an additional layer of protection is noteworthy. While world wide, countries are struggling to reach high level of immunity through vaccination, and current safety measures such as social distancing and use of masks have proven insufficient, these finding could indeed raise some hope and be added to our meager arsenal for preventing the SARS-CoV-2 infection.
Funding Statement
Nasus Pharma is the manufacturer of Taffix and has donated the product for the survey and paid for statistical and data analysis performed by independent company (Medistat).
Declaration of interest
D Megiddo is the CEO of Nasus Pharma, the manufacturer of Taffix. T Lapidot is the VP clinical of Nasus Pharma, the manufacturer of Taffix. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Reviewer disclosures
Peer reviewers on this manuscript have received an honorarium for their review work, Peer reviewers on this manuscript have no other relevant financial or other relationships to disclose.
Author contributions
SK and YN developed the study protocol and participated in the analysis of the results and the written manuscript
DM and TL developed the study protocol and participated in the analysis of the results and the written manuscript as well as in the follow up and operation of the study
References
- 1.[cited 2021 March1]. Available from: https://datadashboard.health.gov.il/COVID-19/general
- 2.[cited 2021 March1]. https://www1.nyc.gov/site/doh/covid/covid-19-data-recent.page. Available from: https://www.wsj.com/articles/new-york-citys-daily-coronavirus-infection-rate-hits-highest-level-in-months-11601395229
- 3.Sungnak W, Huang N, Bécavin C, et al. SARS-CoV-2 entry factors are highly expressed in nasal epithelial cells together with innate immune genes. Nat Med. 2020;26(5):681‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Popov TA, Emberlin J, Josling P, et al. In vitro and in vivo evaluation of the efficacy and safety of powder hydroxypropylmethylcellulose as nasal mucosal barrier. Med Devices (Auckl). 2020;13:107–113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hull D, Rennie P, Noronha A, et al. Effects of creating a non-specific, virus-hostile environment in the nasopharynx on symptoms and duration of common cold. Acta Otorhinolaryngol Ital. 2007;27(2):73–77. [PMC free article] [PubMed] [Google Scholar]
- 6.Mann B, Moreau BG, Lapidot T, et al. TaffiX nasal powder forms an effective barrier against SARS-CoV-2. Biomed J Sci Tech Res. 2021;33(3).25483–5 [Google Scholar]
- 7.CDC . [cited 2021 March1]. Available from: https://www.cdc.gov/quarantine/historyquarantine.html#:~:text=Quarantine%20Now-,The%20Middle%20Ages,for%2040%20days%20before%20landing
- 8.Strasser BJ, Schlich T.. A history of the medical mask and the rise of throwaway culture. Lancet. 2020. July 4;396(10243):19–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.FDA . [cited 2021 March1]. Available from: https://www.fda.gov/emergency-preparedness-and-response/mcm-legal-regulatory-and-policy-framework/emergency-use-authorization#coviddrugs
- 10.Ilie PC, Stefanescu S, Smith L. The role of vitamin D in the prevention of coronavirus disease 2019 infection and mortality. Aging Clin Exp Res. 2020;32(7):1195–1198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Murdaca G, Pioggia G, Negrini S. Vitamin D and Covid-19: an update on evidence and potential therapeutic implications. Clin Mol Allergy. 2020. November 19;18(1):23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.NICE . [cited 2021 March1]. Available from: https://www.nice.org.uk/guidance/ng187
- 13.Gasmi A, Peana M, Noor S, et al. Chloroquine and hydroxychloroquine in the treatment of COVID-19: the never-ending story. Appl Microbiol Biotechnol. 2021. February;105(4):1333–1343. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lewis K, Chaudhuri D, Alshamsi F, et al. The efficacy and safety of hydroxychloroquine for COVID-19 prophylaxis: a systematic review and meta-analysis of randomized trials. PLoS One. 2021. January 6;16(1):e0244778. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Fedullo AL, Schiattarella A, Morlando M, et al. Mediterranean diet for the prevention of gestational diabetes in the Covid-19 era: implications of Il-6 in diabesity. Int J Mol Sci. 2021;22:1213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Finlay BB, Amato KR, Azad M, et al. The hygiene hypothesis, the COVID pandemic, and consequences for the human microbiome. Proc Natl Acad Sci U S A. 2021. February 9;118(6):e2010217118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.[cited 2021 March1]. Available from: https://www.idi.org.il/media/15500/haredi-2020.pdf
- 18.[cited 2021 March1]. Available from: https://www.cbs.gov.il/en/mediarelease/Pages/2020/Serological-Survey-in-Bene-Beraq.aspx
- 19.[cited 2021 March1]. Available from: https://www.btl.gov.il/mediniyut/situation/statistics/btlstatistics.aspx?type=1&id=6100
- 20.Rader B, White LF, Burns MR, et al. Mask-wearing and control of SARS-CoV-2 transmission in the USA: a cross-sectional study. Lancet Digit Health. 2021. March 3;(3):e148–e157. doi: 10.1016/S2589-7500(20)30293-4. [DOI] [PMC free article] [PubMed] [Google Scholar]