

ABSTRACT
Background: Use of manual therapy (MT) is a risk factor for the development of work-related musculoskeletal disorders (WRMDs) in physical therapists (PTs) although the current evidence is limited on this topic.
Objectives: The purpose of this study was to understand the type, association, and prevalence of WRMDs among practitioners of MT, explore relationships between MT and WRMD, and determine impacts of WRMDs on PTs.
Design: Cross-sectional survey design.
Methods: A web-based survey was distributed through the Academy of Orthopaedic Physical Therapy of the American Physical Therapy Association. The survey gathered information on the respondents’ professional profiles, any WRMDs sustained, and how those injuries affected their professional and personal lives.
Results: Overall, 38.5% of PT respondents using MT reported having sustained an MT attributable WRMD. Female respondents reported a greater rate of MT attributable injuries. Although exposure risk is cumulative, novice practitioners are also injured.
Limitations: Generalizability of these results may be limited because of the sample size and specific population responding.
Conclusion: Over one-third of PT survey respondents reported WRMDs attributable to MT. The results indicated WRMDs may begin early in one’s career and tend to accumulate over years of practice. MT educational programming at all levels warrants emphasis on practitioner safety.
KEYWORDS: Work-related musculoskeletal disorders, manual therapy, manual physical therapist, physical therapy, work-related injury
Introduction
Work-related musculoskeletal disorders (WRMDs) are common within the field of physical therapy and have been reported by one investigator to affect nearly 91% of all physical therapists (PTs) at some point during their careers [1]. Some studies show these injuries occur commonly within the first 4–5 years of practice, with a 1-year incidence being 20.7%, while other investigators report physical therapists higher in age sustain more work-related injuries [1–6]. These injuries, perceived as directly related to physical therapy practice, affect PTs in many aspects, including their practice strategies and clinical decision-making, as well as in their lives outside of work. In response to WRMDs, PTs may seek medical treatment, modify their own activities of daily living, and, if severe, may be unable to work [2,3,6]. Within their practices, PTs may employ a variety of strategies to help prevent further injuries. These strategies include: outsourcing their patients to their colleagues, modifying their own positions and patients' positions during interventions, avoiding the use of the injured body region, using additional tools or equipment for assistance, and using alternative treatment techniques [1–3,5-8]. According to Cromie et al. [1] and Vieira et al. [6], the injury-responses from PTs are widely varied. Additional responses include: changing treatment strategies to avoid further injuries, filing workers’ compensation claims, reducing patient contact time, and as many as 16%–39% either changing practice settings or leaving the profession altogether.
WRMDs among PTs in all practice settings have been associated with activities such as patient handling, frequent trunk movements, awkward positioning, increased patient contact time, clinician skill level, size discrepancies, and strength of the PT [1–3,5,6,8]. The most frequent area of the body associated with WRMDs in all PT practice settings is the low back, accounting for a lifetime prevalence as high as 79.6% of all injuries, followed by injuries of the neck, wrist, hand, thumb, upper back, and elbows [1,5,6,8]. Cromie et al. [1] reported clinicians working in ‘private practice’ had more neck, upper back, elbow, wrist, hand, and thumb symptoms. Vieira et al. [6] reported similar findings that clinicians who care for patients with musculoskeletal disorders typically have higher rates of thumb, elbow, wrist, and hand pain, especially if the clinician performs manual examination and treatment for their patients.
There is limited evidence of the relationship of WRMDs and the practice of manual therapy (MT), as well as the impacts of these injuries have on PTs who perform MT. The disciplines of osteopathy and chiropractic also offer limited, but valuable information toward the relationship between WRMDs and the utilization of MT [9,10]. While the performance of MT is clearly identified as one of the risk factors associated with WRMDs among physical therapists, incomplete information is available in literature as to the type, causes, prevalence, and relationship of MT and WRMDs. Given this lack of evidence, the purpose of this study was to understand the type, cause, and prevalence of WRMDs, explore the relationship between MT and WRMDs, along with determining the impact of this relationship has on physical therapists.
Methods
Participants
The population sought for survey distribution included those who were members of the Academy of Orthopaedic Physical Therapy (AOPT) of the American Physical Therapy Association (APTA), and specifically those practicing physical therapists who have performed MT during their careers. The subject population included males and females of any ethnic background and health status and ranged from the ages of 21–80 years. Subjects who had never performed MT in their careers or were not licensed PTs were asked not to participate in the survey. Informed consent was provided when subjects initiated the survey by first viewing an introductory explanation of the survey and an agreement to participate by advancing to the start of the survey. The research protocol and consent were approved by the Institutional Review Board of the University of Kentucky.
Instrument
Using the Qualtrics® instrument, a web-based survey was designed containing 36 questions seeking demographic characteristics, career experiences related to MT, education, training, any occurrence of WRMDs directly attributable to MT, and the impact of injuries on clinical decision-making and practice. Impacts on personal well-being, home lives, and other personal activities were also assessed (See Appendix 1). The survey was beta tested with three clinicians with particular interest in this topic, from which minor changes were made within the structure of the survey. Additionally, one independent external reviewer assessed the survey, resulting in additional edits. Once completed, the survey was sent to the AOPT of the APTA for approval and distribution to all members via electronic mail with an introduction to the survey and a hyperlink to access the web-based survey.
Procedure
Access to the self-administered web-based survey was distributed to the approximately 20,000 members of the AOPT. An electronic mail message with the hyperlink included a cover letter that stated the purpose of the study, a summary of the content of the questionnaire, contact information for follow-up questions, and assurance of confidentiality was distributed by the AOPT to its members. The survey was open for approximately 4 weeks during February and March 2018. Because of the evaluative nature of manual therapy, only licensed physical therapists were encouraged to complete the survey. AOPT members who were not licensed physical therapists were asked to not complete the survey.
Data analysis
Upon closure of the survey, data were exported from Qualtrics® and subsequently analyzed by using SPSS® (version 23) software for Windows (IBM Corp. IBM SPSS Statistics. Armonk, NY). Pearson Chi-square analyses were utilized to evaluate group differences. A logistic regression was also modeled for WRMD after a full factorial model for biological sex, height, and weight examining for particular associations in the response data. Frequencies and descriptive statistics were also calculated. A probability of p < 0.05 was considered statistically significant.
Results
A total of 361 members responded to the survey. Participant characteristics are summarized in Table 1. The participant sample included 53.6% (n = 190) females and 47.4% (n = 171) males. Participants ranged from 24 to 72 years of age, with a mean age of 41.4 years. Professional experiences ranged from new graduates within their first year of practice (7.2%) to those who held greater than 30 years of experience (16.9%). Over half of the members (53.0%) held clinical doctorate degrees; however, academic degrees varied from Bachelor’s to Doctorates of Philosophy (PhD) to any combination of those available. Additionally, 128 (37.2%) respondents described having acquired advanced or specialized MT credentials. Average weekly caseload was reported to be 47.2 visits per week with an estimated average of 60% of patient cases being indicated for MT interventions.
Table 1.
Respondent characteristics
| Characteristics/Results | N* | Percentage |
|---|---|---|
| Gender | ||
| Males | 171 | 47.4% |
| Females | 190 | 53.6% |
| Mean Age (years) | 41.4 | – |
| Years Practiced | ||
| 1 year or less | 26 | 7.2% |
| 2–4 years | 78 | 21.6% |
| 5–10 years | 72 | 20% |
| 20–30 years | 61 | 16.9% |
| >30 years | 61 | 16.9% |
| Mean Height (inches) | ||
| Males | 70.9 | – |
| Females | 65.3 | – |
| Mean Weight (pounds) | ||
| Males | 190.8 | – |
| Females | 149.5 | – |
| Body Mass Index | 360 | – |
| Normal/Healthy Weight (18.5-24.9) | 176 | 47.85% |
| Overweight (25.0-29.9) | 136 | 38.5% |
| Obese (>30) | 48 | 13.4% |
| Respondents who obtained advanced MT credentials | 128 | 37.2% |
| Number of Injured Respondents |
57 | 44.0% |
| Knowledge of Alternative Techniques | 263 | 77.0% |
*n will be larger than the number of respondents due to select all that apply option on question
Injury rate was also examined relative to body mass index (BMI) as has been completed in other studies evaluating WRMDs and PT practice and because of the common perception of a possible association. When examining the physical characteristics of all the respondents, the mean values for males were 70.9 inches (180.1 cm) in height and weight of 190.8 pounds (86.5 kg), and for females, a height of 65.3 inches (165.9 cm) and weight of 149.5 pounds (67.8 kg). When considering these factors in relation to BMI categories per the Centers for Disease Control and Prevention (CDC) [11], 31% (n = 53) males and 64.7% (n = 123) females were at a ‘Normal/Healthy Weight’, 53.8% (n = 92) of males and 23.2% (n = 44) of females were ‘Overweight’, and 15.2% (n = 26) of males and 11.6% (n = 22) of females were ‘Obese’.
Table 1 provides a summary of the results of this study. Overall, 129 (38.5%) individuals responding to the survey reported having sustained a WRMD attributed to using MT. Female respondents had a higher rate of injury with 43.6% (n = 75) reporting injury as compared to 33.1% of males (n = 54). Chi-square analysis of these survey response data indicates that females had an odds ratio of WRMDs at 1.56 to that of male respondents (p = 0.0495). Of the 129 respondents who reported having sustained WRMDs, 27.6% (n = 27) had 4 years or less of clinical practice, 30.5% (n = 18) had 5 to 10 years of experience, 47.1% (n = 33) had 10 to 20 years of experience, 37.7% (n = 20) had 20 to 30 years of experience, and 56.3% (n = 31) with those practicing for greater than 30 years reporting injuries (Figure 1). Predictably, these data suggest the risk of injury is cumulative with years of exposure of practicing MT.
Figure 1.
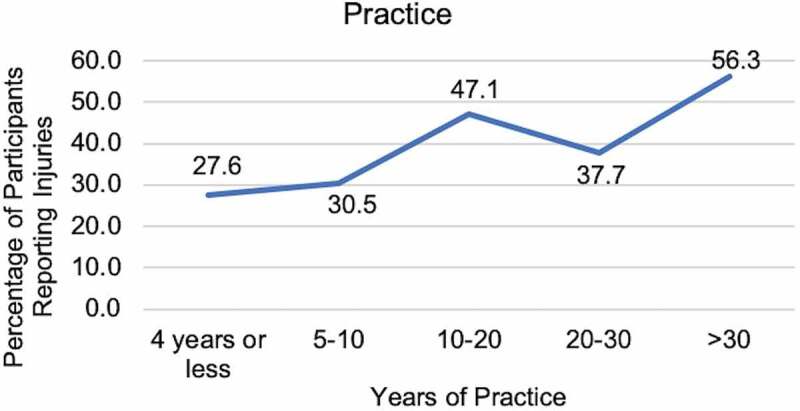
Rate of injury based on years of practice
Any indicator of practitioner stature in the relationship of occurrence of WRMDs was not evidenced in the current data. No significant associations between occurrence of injury and measures of clinician BMI, height, and weight were revealed. No significant relationship of BMI categories to injury occurrence was detected once analyses controlled for biological sex (p = 0.476). Only sex out of all possible main effects with their interactions was statistically significant. The model suggests that there is an association between sex and WRMD. The R-squared values for height correlation to injury being determined to be 0.0026 (p = 0.28) and weight at 0.0025 (p = 0.29).
Among all respondents, 37.2% (n = 128) reported having earned advanced manual therapy credentials consisting of: Certified Orthopedic Manipulative Therapist, Certified Manual Physical Therapist, Manual Therapy Certification, Functional Manual Therapy Certifications, Orthopedic Manual Therapy Certificate, Fellow of the American Academy of Orthopedic Manual Physical Therapist credentials, and other unspecified credentials. Among females, 39.5% (n = 66) reported obtaining advanced MT credentials as along with 34.5% (n = 61) of males. Among those specifically reporting a history of WRMDs, 44% reported having earned advanced manual therapy credentials. The chronological relationship was not established between occurrence of injury and qualification of advanced credentials.
Multiple body regions were documented to be affected with the leading area being the wrist and hand (80.6%), followed by the lumbar/back region (28.0%), shoulder (20.1%), elbow (16.3%), neck (14.0%), hip and pelvis (5.4%), ‘other regions not described’ (4.7%), knee (3.9%), and ankle (1.6%) (Figure 2). Thus, while wrist and hand injuries are most common, involvement of other body regions of MT practitioners may also occur with remarkable frequency.
Figure 2.
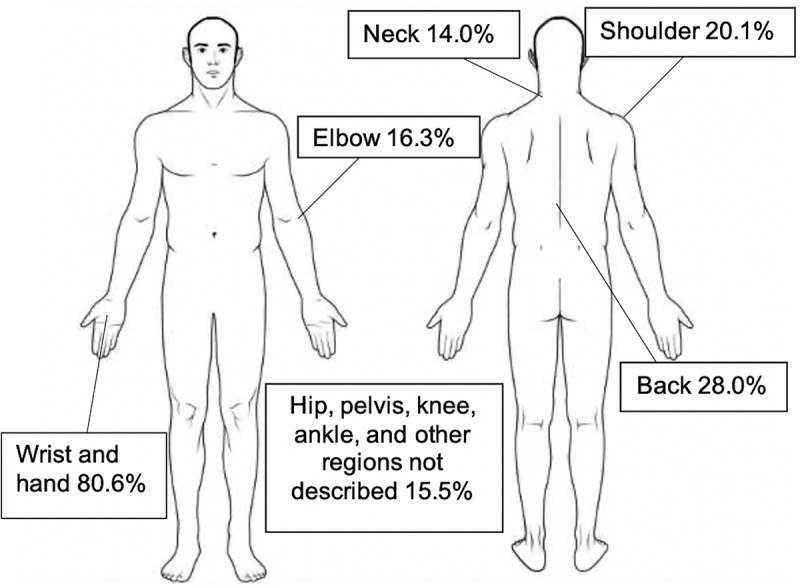
Areas affected by WRMDs among respondents
The results of these injuries were reported to cause widespread changes within the clinicians’ clinical practice and overall career, as well as in non-occupational aspects of their lives, as seen in Figure 3. Overall, 11.1% (n = 14/126) of respondents who sustained WRMDs reported having changed their career paths due to these injuries. Clinically, albeit a small sample among this group, seven participants were required to reduce their working hours, while eight others relocated to a setting with less perceived risk or to an administrative position. Notably, 60.6% (n = 77/127) reported significant effects from their injuries outside of the work setting and in their personal and family lives, including affecting their fitness (75.3%, n = 58), hobbies (70.1%, n = 54), and instrumental activities of daily living (IADLs) (33.8%, n = 26).
Figure 3.
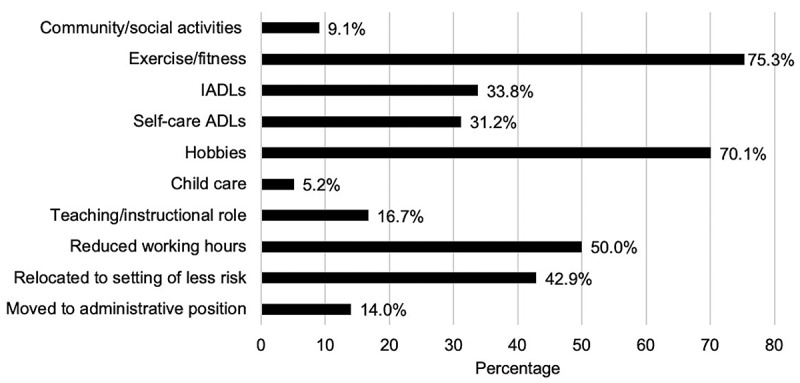
Clinical and non-clinical effects from injury
A large majority at 77.4% (263/340) of all respondents reported having obtained knowledge of alternative MT techniques intended to reduce the risk of practitioner injury. Respondents reported having learned of these techniques from multiple sources including their original physical therapy school curriculum, current employer, prior employer, continuing education courses, evidence-based research, colleague, and self-teachings. Among those with alternative technique knowledge, 32.6% (n = 86/361) reported having learned alternative techniques with a practitioner safety focus from their original educational curricula. Among those reporting injuries, 26.4% (n = 34/129) reported having learned alternative techniques with a safety focus in their physical therapy educational curricula. The chronological relationships of injury onset and learning of alternative techniques were not established.
Discussion
This study was created to provide additional evidence to the limited body of research regarding WRMDs related to the use of MT within the profession of PT. The results of this survey provide greater insight about the specific relationship between WRMDs and the practice of physical therapy utilizing MT in a manner consistent with the current literature, expanding upon that previously reported evidence. MT has been described as one among several other risk factors relating to WRMDs in the profession of physical therapy, yet the available evidence on the topic is not robust [1–3,6,12]. This study revealed that the occurrence of injuries attributable to MT is a professional issue by affecting a significant proportion (38.5%) of practitioners responding to this survey. Notably, the female clinicians responding to this survey did so indicate 1.56 times greater odds of becoming injured compared to males. Several studies have suggested that female PTs tend to sustain more injuries throughout their professional careers compared to males [2,4,6,8,13]. Vieira et al. [6] inferred this incidence may be due to a biomechanical disadvantage resulting from size and strength differences between sexes. Regression analysis of the biometric data among these survey respondents, however, did not reveal specific associations of height, weight, and BMI once analyses controlled for biological sex. Muaidi et al. [8] proposed that females experienced a higher prevalence of injury due to lower BMI [6,8]. With BMI being an index of proportions of height and weight rather than absolute values in relation to potential size disadvantages of practitioner to patient, the investigators of this study hypothesized that BMI would not be a predictive factor for injury. The hypothesis of practitioners having smaller stature with height and weight being related to injury was not supported in these data. Population characteristic differences in this study and that previously published could account for the inconsistency of these results in existent evidence. The risk for injury may also be influenced by numerous other factors; these may include practitioner–patient interaction frequency, application of manual therapy frequency along with PT positioning, length of time dedicated to treatment, repetitive tasks, and size discrepancies [1,5,6]. These factors, however, may be difficult to isolate and for which to control in data analyses.
Years of practice and commensurately potential exposure to biomechanical stresses relating to potential injury, in combination with developing manual therapy skills provide for two trajectories which likely follow similar, if not parallel, paths over the career of practitioners. To identify these trajectories within study populations would very likely present technical challenges for investigators and to quantify the same for analyses would similarly require very intricate study methodology in large populations. King et al. [4] compared rate of injury in clinicians younger and older than 55 years of age and found there were no significant differences between those ‘older’ versus ‘younger’. Likely is that while practitioners accumulate exposure over time with patient interactions, they are also similarly developing more clinical skills, including the ability to expand MT options with techniques which may allow for the reduction of WRMDs risk. Thus, while the practitioner accumulates exposure to risk, skill development may similarly accumulate a compensatory risk reduction. These factors may be represented in the current data with injury rates in early and late in career stages. When comparing the rate of injury among therapists who had been practicing less than 5 years versus those who had been practicing longer than 5 years, other studies have shown that the rate of injury was often highest among those within their first 5 years of practice [1–3,5,6,8,13]. The current study also found that the risk of injury begins early in a clinician’s career with 27.6% experiencing at least one injury during their first 4 years of practice. The data collected for this study did not isolate etiological factors related to injury; however, limited professional experience or lack of knowledge of adequate alternative MT techniques may hypothetically be contributors to the occurrence of injury early in a career. Thus, the protective effect of experience and greater manual therapy knowledge may be limited in result, however, because of cumulative exposure over one’s career, including the 56.3% rate of injury among practitioners in this study with greater than 30 years or more experience. Thus, these data may be interpreted as similar to that of King et al. [4] with injury rates reflecting perhaps a lack of knowledge or skill early in one’s career and the cumulative exposure effect over years of practice. As such, reduction of risk early in one’s career may be of particular importance to lessen early career injury risk and the cumulative effect of particular biomechanical stresses over time.
With the current data indicating risk of injury being significant in early years of practice coupled with only 26.4% (n = 34/129) of those reporting injury having learned of alternative methods from their initial curricular studies, physical therapy educational programs and clinical instructors are perhaps challenged to include more complete offerings of alternative techniques directed at injury risk reduction in preparing entry-level practitioners. The data regarding this precise relationship of early practice knowledge and risk of injury are incomplete and warrant further research, yet the consistency of data across this and multiple other studies highlights that risk of injury early in one’s practice years is remarkable and warrants the attention of educators.
Knowledge of alternative techniques presumably offering greater safety for the practitioner may be presumed as important but is largely hypothetical. Data are scant on particular manual techniques and any accompanying elevated or reduced risk of practitioner injury. Anecdotal knowledge and experience accompanying basic biomechanical knowledge may serve as the basis for what many manual therapists cite as techniques with lower risk of injury. Although research to identify techniques with particularly elevated or reduced risk may be difficult to complete pragmatically, the need is clear to explore this in future research endeavors.
The risk of PTs sustaining injuries to the wrist and hand from the utilization of MT has been well documented in the literature [1,2,5,6,12,13]. There are fewer publications discussing the injuries occurring at other body regions affected by the practice of MT [1–6,8,12]. Findings from the current study provide further support for the wrist and hand being most commonly affected (80.6%), but also show that areas of the back (28.0%), shoulder (20.1%), elbow (16.3%), and neck (14.0%) are also being frequently affected. Although technique knowledge intended to protect the hands or thumbs is critical for practitioners of MT to learn, strategies to protect other regions of the practitioners’ anatomy are also important. Instruction in MT prudently will include whole-body protective strategies.
The relationship of advanced manual therapy training and credentials and the occurrence of injury are unclear in the present data. Injury rates among those with and without advanced manual therapy credentials are similar. Among those with advanced manual therapy credentials, 44% reported injury, slightly higher than the overall rate among respondents. Numerous factors may be contributing to those results, however, including cumulative exposure. Those with advanced credentials may be more likely to choose manual interventions, thereby increasing their overall exposure risk. Thus, caution is warranted with the interpretation of these data as representations of specific survey population characteristics may be included. Further, those with a greater interest in manual therapy and perhaps with advanced credentials may have been more likely to complete the survey than those with lower interest levels and without advanced credentials.
Career trajectory, clinical practice, and life outside of the clinic are also being impacted by these injuries. Consistent with other evidence, the current study found that clinicians altered their treatment approaches, increased use of exercise prescription, referred patients to other colleagues, and/or increased the use of therapeutic modalities in response to their injury. Other effects of injuries reported in this survey included the need to transition into educational roles or administrative positions at the time of injuries, relocating to settings of perceived less risk, or reductions of working hours. The impact of injuries also reportedly expanded beyond careers and clinical practice, affecting the fitness, social involvements, hobbies, and abilities to perform daily activities. The expansive impacts of these injuries affect the quality of life and clinical practice of PTs who become injured, potentially with cascading effects on the profession as a whole. The risk of injury was shown to be present early in a clinician’s career and tend to accumulate over time. The accumulation of injury over time can affect career transitions by those injured and may potentially result in the loss or reduced influence of the most experienced and knowledgeable practitioners who could otherwise serve as valuable mentors to less experienced and knowledgeable clinicians.
The results of this study should be considered within its limitations. Only members of the Academy of Orthopaedic Physical Therapy were provided access to the survey with a relatively small cross-sectional sample size limiting generalizability. While a limited response rate occurred, the survey has provided novel information not previously available. While these limitations are noteworthy, the data resulting from this study are in many cases consistent with that from similar studies from physical therapy and other disciplines in which therapeutic manual interactions with patients occur. Further research may allow for more complete understanding of etiological trends and the effect of alternative technique knowledge.
Conclusion
The risk of WRMDs with the practice of MT is significant and warrants consideration with educators of MT at all levels. Entry-level educational curricula, post-graduate educational curricula, and clinical instructors may benefit future practitioners with sufficient inclusion of techniques intended to provide a lower risk of injury, which may be of particular importance in the early years of practitioners’ careers. Female practitioners may have a particularly elevated risk of injury and may be well served to have a heightened pursuit of protective strategies. The present study also highlights the potentially far-reaching effects of WRMDs among PTs, making this a professional issue. In addition to changing direct patient care decisions in individual situations, more expansive effects are evidenced by changes in career paths and work patterns. Additionally, the effects of WRMDs outside of the work setting may be significant to the personal and family lives of practitioners. Reduction of risk of WRMDs warrants further research and the attention of the profession for the continued growth of MT as a key feature of physical therapy practice for the future.
Supplementary Material
Acknowledgments
The authors would like to thank the Academy of Orthopaedic Physical Therapy for their support and distribution of the survey. Additionally, the authors would like to thank Alejandro Villasante-Tezanos, PhD and Sydney Thompson, MS for their assistance with the statistical analyses. Finally, they would like to thank Matt Lee, PT, DPT, OCS, FAAOMPT, Angela Darragh, PT, CFFM, Amy O’Neal, PT, and Anthony Powell, PT, CSCS for their assistance as beta testers for the survey.
Biographies
Lauren Cornwell, PT, DPT graduated with her Doctorate of Physical Therapy from the University of Kentucky. She is a licensed physical therapist at Orthopedic and Neurological Consultants in Pickerington, Ohio. This article is based on the research she performed for her doctoral dissertation.
Haley Doyle, PT, DPT graduated from the University of Kentucky in 2019 with her Doctorate in Physical Therapy. She is currently working as a licensed physical therapist in an outpatient clinic with interests in manual therapy, orthopedics, and sports medicine.
Megan Stohner, PT, DPT is a licensed physical therapist with the Kentucky Orthopedic Rehab Team in Frankfort, Kentucky. She graduated with a Doctorate of Physical Therapy from the University of Kentucky in 2019. This article reports on research initiated for her doctoral dissertation.
Charles Hazle, Jr., PT, PhD is an Associate Professor at the University of Kentucky and has previously published and presented on alternative manual therapy techniques and methodological approaches for technique adaptation for size disadvantaged clinicians. He also has numerous other publications relating to manual therapy and imaging in physical therapist practice.
Disclosure statement
No potential conflicts of interest were reported by the authors.
Supplementary material
Supplemental data for this article can be accessed here.
References
- [1].Cromie JE, Robertson VJ, Best MO.. Work-related musculoskeletal disorders in physical therapists: prevalence, severity, risks, and responses. Phys Ther. 2000;80(4):336–351. [DOI] [PubMed] [Google Scholar]
- [2].Campo M, Weiser S, Koenig K, et al. Work-related musculoskeletal disorders in physical therapists: a prospective cohort study with 1-year follow-up. Phys Ther. 2008;88(5):608–619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Adegoke BO, Akodu AK, Oyeyemi AL. Work-related musculoskeletal disorders among Nigerian physiotherapists. BMC Musculoskelet Disord. 2008;9:112–120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].King P, Huddleston W, Darragh AR. Work-related musculoskeletal disorders and injuries: differences among older and younger occupational and physical therapists. J Occup Rehabil. 2009;19(3):274–283. [DOI] [PubMed] [Google Scholar]
- [5].Rozenfeld V, Ribak J, Danziger J, et al. Prevalence, risk factors and prevention strategies in work-related musculoskeletal disorders among Israeli physical therapists. Physiother Res Int. 2010;15:176–184. [DOI] [PubMed] [Google Scholar]
- [6].Vieira ER, Schneider P, Guidera C, et al. Work-related musculoskeletal disorders among physical therapists: a systematic review. J Back Musculoskelet Rehabil. 2016;29(3):417–428. . [DOI] [PubMed] [Google Scholar]
- [7].Hazle CR, Lee M. Strategies to overcome size and mechanical disadvantages in manual therapy. J Man Manip Ther. 2016;24(3):120–127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Muaidi QI, Shanb AA. Prevalence causes and impact of work related musculoskeletal disorders among physical therapists. J Back Musculoskelet Rehabil. 2016;29(4):763–769. [DOI] [PubMed] [Google Scholar]
- [9].Hansen MC, Aagaard T, Christensen HW, et al. Work-related acute physical injuries, chronic overuse complaints, and the psychosocial work environment in Danish primary care chiropractic practice-a cross-sectional study. Chiropr Man Therap. 2018;26:4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].McLeod GA, Murphy M, Henare TM, et al. Work-related musculoskeletal injuries among Australian osteopaths: a preliminary investigation. Int J Osteopath Med. 2018;27:14–22. [Google Scholar]
- [11].About Adult BMI . Centers for disease control and prevention. [updated 2017 August29; cited 2019 Feb] . Available from: https://www.cdc.gov/healthyweight/assessing/bmi/adult_bmi/index.html
- [12].Darragh AR, Campo M, King P. Work-related activities associated with injury in occupational and physical therapists. Work (Reading, Mass). 2012;42(3):373–384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Rossettini G, Rondoni A, Schiavetti I, et al. Prevalence and risk factors of thumb pain in Italian manual therapists: an observational cross-sectional study. Work (Reading, Mass). 2016;54(1):159–169. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.