

Abstract
Background
The results of randomized trials show that breast cancer screening by mammography reduces breast cancer mortality by up to 40% in women aged 50-69 years. Because of these results, by 1998, 22 countries, including Canada, had established population-based organized screening programs. This paper presents the results of screening mammography in 1996 for 7 provincially organized breast cancer screening programs in Canada.
Methods
Analyses of interim performance indicators for screening mammography have been calculated from data submitted to the Canadian Breast Cancer Screening database. The data set consisted of data from 7 provincial programs and was limited to mammographic screens for women aged 50-69 years (n = 203 303). Screening outcomes and performance indicators were calculated for abnormalities detected by screening mammography only.
Results
The abnormal recall rate was 9.5% for first screens and 4.6% for subsequent screens, and the cancer detection rate per 1000 women screened was 6.9 for first screens and 3.8 for subsequent screens. The positive predictive value (i.e., the proportion of women who tested positive by mammography who were found to have breast cancer on screen-initiated diagnostic work-up) increased from 7.2% at the first screen to 8.2% at subsequent screens. Estimated participation rates within organized programs varied from 10.6% to 54.2%, depending on the province.
Interpretation
For 1996, organized breast cancer screening programs met or exceeded many of the interim measures used in international programs. It is possible to translate the benefits of breast cancer screening by mammography, as demonstrated in randomized trials, into population-based community programs. Screening mammography through organized programs should increase to allow more comprehensive monitoring in Canada.
The aim of screening mammography is to detect malignant breast cancer when there are no clinical signs or symptoms of breast disease, at a stage when effective treatment can be offered. The results of randomized trials show that screening mamography among women aged 50-69 years can reduce breast cancer mortality by up to 40%.1,2,3 This has led to a growth in breast cancer screening by mammography in industrialized countries. As of 1998, at least 22 countries had established national, jurisdictional or pilot population-based breast cancer screening programs.4
The delivery of screening mamography varies in different countries. In the United States, breast cancer screening by mammography takes place within the context of general medical care and special programs aimed at marginalized women.5 Other countries have established population-based breast cancer screening programs. Some of the most completely reported and longstanding national programs are in the United Kingdom,6 the Netherlands,7 Sweden8 and Australia.9
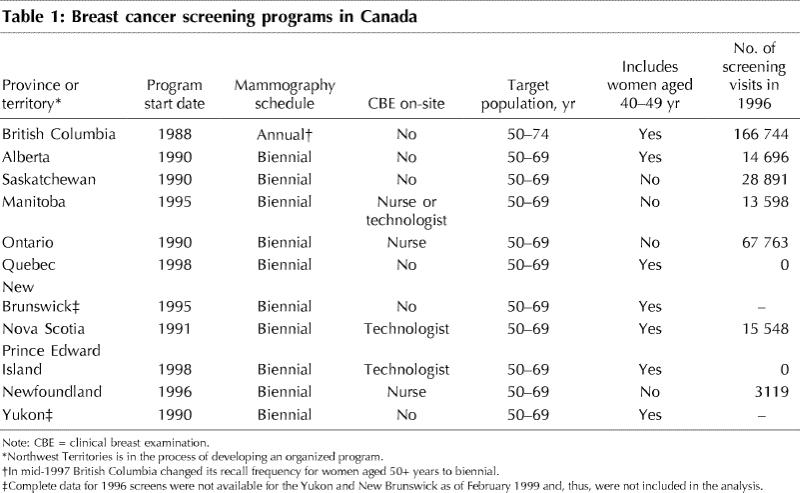
In Canada women can access mammography through the fee-for-service system or, for women in the target age range, by participating in provincial or territorial organized breast cancer screening programs, with or without a referral from their family physician. In 1988, there was a single provincial, organized breast cancer screening program in Canada. By 1996 (the latest date for which complete information is available from the Canadian Breast Cancer Screening Database), there were organized programs in 8 provinces and 1 territory. Table 1 summarizes the different provincial and territorial programs. Within the organized programs, the number of screening visits for women of all ages increased substantially from 4475 in 1988 to 310 359 in 1996.10
Table 1
Population-based screening programs offer an unprecedented opportunity to assess the effectiveness of screening mammography in a community setting. The goal of every breast cancer screening program, and the measure by which a program should be evaluated, is a reduction in breast cancer mortality. However, a significant reduction is expected only after 7-10 years with 70% of the target population receiving mammography.11 To enable population-based programs to evaluate their performance sooner, interim indicators of effectiveness based on the results of randomized trials have been developed.11,12 These indicators include such measures as the participation rate, abnormal recall rate, cancer detection rate and the stage of disease. Although favourable values for these outcomes do not guarantee a reduction in mortality, it is anticipated that they will precede reductions in breast cancer deaths. In general, published results from other organized programs meet and even exceed such early performance indicators.6,7,8,9
In December 1992, the federal government announced the Canadian Breast Cancer Initiative (CBCI), which was provided with a total budget of $25 million over 5 years. Continued funding for the CBCI has been provided by Health Canada. The Canadian Breast Cancer Screening (CBCS) Initiative, which is 1 of the 6 programs that form part of the CBCI, provided support for the development of the CBCS database. This database was established in 1993 with the goal of monitoring and evaluating the performance of organized breast cancer screening programs. Its creation allows the comparison of outcomes from provincial and territorial programs with international indicators. This report presents the results of the performance of screening mammography within 7 provincial organized screening programs for the year 1996 and compares them with those published from the United Kingdom,6 the Netherlands,7 Sweden8 and Australia.9
Methods
Data are submitted by organized programs to the CBCS database according to a set of common data items, defined in a data dictionary developed by representatives of the organized screening programs and Health Canada. All screening programs perform a 2-view mammogram, which is referred to as a screen in this report. Some programs also offer clinical breast examination (CBE) on-site as part of the screening visit.
Data used in the analysis included screening results (normal or abnormal) and, for women with an abnormal finding, the reason for referral to assessment. This information was collected using check-off forms completed by the program radiologists. Over 95% of women with abnormal screen results had complete follow-up information, which included diagnostic tests, test results, a final diagnosis of benign or primary breast cancer (in situ or invasive) and, where applicable, tumour size, nodal status and stage of disease. Information about diagnostic tests and their outcomes was obtained from the women's physicians. Staging information on the cancers detected within the program was collected through data linkage with cancer registries or by deriving the information from pathology reports or from the attending physicians' reports.
Upon receipt, the data underwent a first series of data quality checks whereby they had to conform to the database's business rules, which require the inclusion of range checks, a value list and logic checks before the data may be loaded onto the database. During the loading process, a second series of data quality checks was performed.
This report presents the results for 1996, using data submitted to the CBCS database up to February 1999. The 1996 calendar year was used because it was the most recent year for which complete information was available. Data from programs in the following provinces were combined to form the data set: British Columbia, Alberta, Saskatchewan, Manitoba, Ontario, Nova Scotia and Newfoundland. A subset of data was selected for these analyses. Inclusion rules for the subset consisted of the following:
· Screening mammography, with or without CBE, performed on women aged 50-69 years (target age range) was included. This accounted for 65.5% of screening visits in 1996 (n = 203 303).
· For some programs, a screening visit also included CBE (Table 1). In rare cases, CBE is offered in the absence of a screening mammogram. These cases consisted of less than 1% (n = 45) of total visits and were excluded from the analyses.
· Screening outcomes and performance indicators were calculated for abnormalities detected by screening mammography only. If a woman had a normal mammogram but an abnormal CBE, her results were not considered to be "abnormal" for the purpose of these analyses.
The following values were calculated: abnormal recall rate, cancer detection rate, benign-malignant biopsy ratio, positive predictive value and participation rate. An abnormal recall rate is defined as the proportion of screening mammograms that lead to a referral for diagnostic investigation. The benign-malignant open biopsy ratio is the ratio of the number of women with a benign diagnosis after screen-initiated open biopsy to the number of women with a diagnosis of breast cancer found through screen-initiated open biopsy. The cancer detection rate is the rate of screen-detected breast cancer per 1000 screens. This includes cases of invasive and ductal carcinoma in situ (DCIS) and excludes lobular carcinoma in situ. The positive predictive value of screening (PPV) is the proportion of patients with abnormal results found to have breast cancer on screen-initiated diagnostic work-up.
The participation rate is defined as the proportion of women in the target age group who attended a screening program at least once in 2 years. It was calculated by using census projections for 1996 as estimates of the number of women in the target age range in each province.13 The population estimates were then halved to provide an approximation of participation rates at least once every 2 years. Participation rates were estimated in this way for all provinces, including BC where annual screening was offered in 1996, in order to treat provinces in a comparable manner.
The results are presented by first screens, subsequent screens and total screens. A first screen is defined as the first time a woman is screened within an organized breast cancer screening program. The results are compared with those of other established screening programs.
Results
The estimated participation rates of women in the target age range within organized breast screening programs are depicted in Fig. 1 The participation rate ranged from 10.6% to 54.2%.
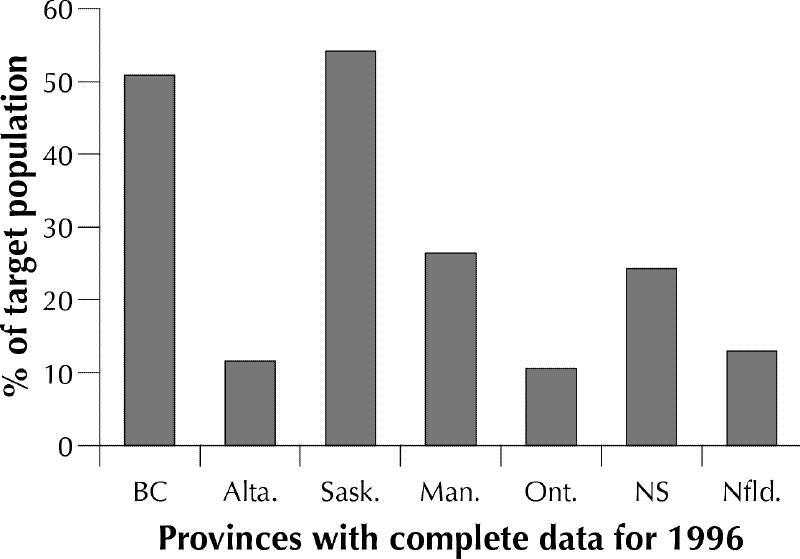
Fig. 1: Estimate of the proportion of the target population* who participated in provincial breast cancer screening programs in Canada in 1996. *Target population is defined as women aged 50-69 years. Estimates were derived from Statistics Canada.13 Population estimates were then halved to provide an approximation of participation rates at least once every 2 years.
A summary of mammography performance indicators is shown in Table 2. On initial screening (n = 65 262), the abnormal recall rate was 9.5%. For the 138 041 subsequent screens, the abnormal recall rate was much lower (4.6%). For women with abnormal screening results, the most common diagnostic procedures performed involved imaging techniques: diagnostic mammography in 57.7% of procedures and ultrasonography in 26.2%. The balance of procedures reported were invasive, with fine needle aspirations accounting for 2.6% and biopsies reported for 13.5%. The majority of biopsies were open, with or without fine wire localization (10.7%). Only 2.8% were core biopsies. Of the 1945 open biopsies performed, 854 procedures resulted in a final diagnosis of cancer. The benign-malignant biopsy ratio was 1.3:1.
Table 2
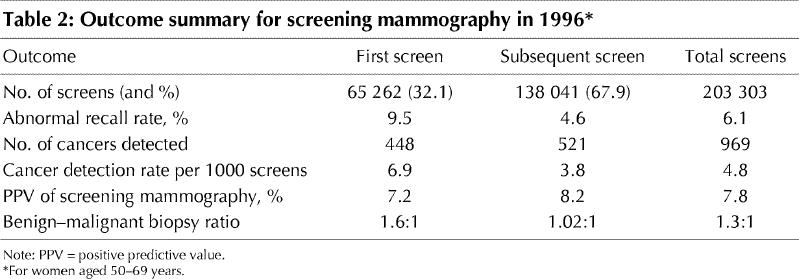
In total, 969 women were diagnosed with cancer following abnormal results on screening mammography; 448 were identified at first screen and 521 were identified at subsequent screening, resulting in a cancer detection rate per 1000 screens of 6.9 and 3.8 respectively. The PPV for organized screening programs was 7.8%; it increased from first screen to subsequent screening (from 7.2% to 8.2%).
Of the 969 cancers detected, 799 (82.5%) were invasive and 170 (17.5%) were DCIS (Table 3). Almost three-quarters (74.0%) of the cancers for which staging information was available were stage 0 or I. For invasive tumours, 53.7% were less than 15 mm in diameter and 76.9% had a negative nodal status. Cancers that were detected in subsequent screens were smaller in size (59.1% v. 47.5% were less than 15 mm in diameter), and a greater proportion did not have lymph node involvement (80.3% v. 73.0%).
Table 3
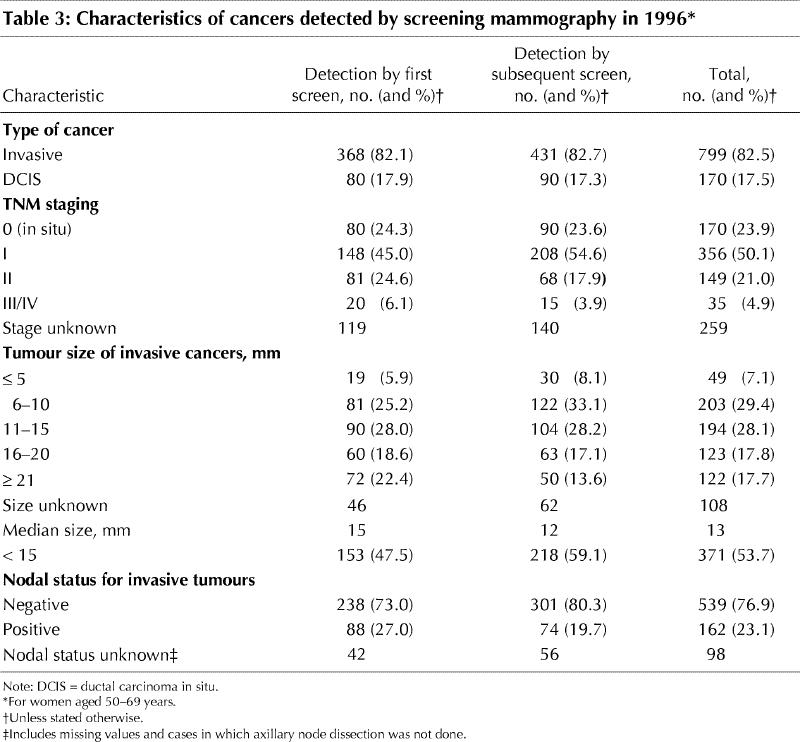
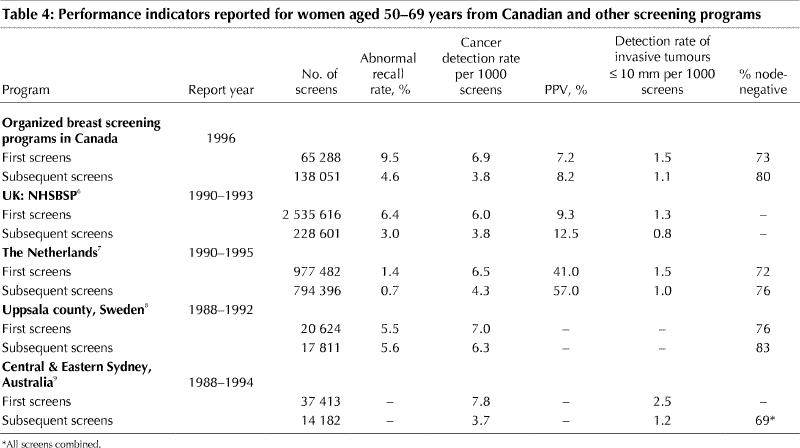
Table 4 provides a comparison of the performance of mammography in Canadian, organized breast cancer screening programs with that in other programs. The abnormal recall rate for first screens is somewhat higher and the PPV is lower in comparison with other programs, especially when compared with the Netherlands. However, other indicators such as the cancer detection rates, the rate of small invasive cancers and the nodal status of invasive cancers are consistent with other programs.
Table 4
Interpretation
Data collection and the ongoing evaluation of screening mammography are essential components of organized screening programs. The 1996 results confirm that organized screening, even in the early days of introduction into the community, is effective in achieving a number of interim measures that are necessary for a future reduction in mortality from breast cancer.
As expected, the abnormal recall rate was higher for first screens (9.5%) than subsequent screens (4.6%). This pattern was expected and occurs because current mammograms may be compared with previous mammograms when women attend for subsequent screening. The abnormal recall rate for first screens was somewhat higher than those of other programs (1.4%-6.4%). The continued expansion of organized breast cancer screening in Canada may be a factor. Two new provincial programs were implemented in 1995 and 1996, and new sites were being added within older organized programs. Reports have shown that as radiologists gain experience within screening programs, the rate of abnormal mammograms tends to decrease and stabilize.14 However, while programs evolve and increase their capacity, the abnormal recall rate may continue to pose a challenge to provincial and territorial programs.
Another explanation for the differences in abnormal recall rates and PPV between the Netherlands and other programs, including those in Canada (Table 4), is the diversity among the screening programs. A survey of 22 countries with organized screening programs indicates that programs differ in their level of organization, invitation methods, process for reading and interpreting mammograms and follow-up for abnormal results.5 The International Breast Cancer Screening Network is an international collaborative effort designed to bring together breast cancer screening programs for the purpose of producing comparable data on the policies, administration and results of population-based breast cancer screening. It is expected that methodologies for the evaluation and reporting of outcomes from screening mammography will be developed to better assess the impact of breast cancer screening in the population.
The breast cancer detection rates among Canadian programs (6.9 and 3.8 per 1000 for first and subsequent screens respectively) are comparable with those published by other programs (6.0-7.8 per 1000 for first screens and 3.7-6.3 per 1000 for subsequent screens). Staging data show that breast cancers are also being detected at an early stage, with 53.7% of invasive tumours being less than 15 mm in diameter and 76.9% node-negative. These findings are consistent with standards based on the results of the Swedish 2-county randomized trial,12 which state that in order to achieve a reduction in mortality, more than 50% of invasive tumours should be less than 15 mm in diameter and more than 70% should be node-negative. Women with these cancers have a better prognosis and a greater likelihood of having breast-conserving surgery and potentially less "aggressive" adjuvant therapy.15
Noninvasive cancers in the form of DCIS represented 17.5% of screen-detected cancers in organized programs. This finding is well within the standard (10%-20% of screen-detected cancers) established in Australia.16 There are differing opinions over the value of detecting these noninvasive cancers. Some researchers argue that DCIS is a precursor to invasive cancer, whereas others state that DCIS does not always lead to invasive disease.17 It is worth noting that there was a 314% increase in the incidence rates of DCIS in the United States from 1983 to 1993, most of which is attributed to increased detection through mammography.17
The term "interval cancer" describes breast cancers that are detected in the interval between regular sessions of screening mammography. Data on interval cancers were not complete for 1996 and were, therefore, not included in this report. For 1997-1998, information about interval cancer rates will indicate whether programs are detecting a substantial proportion of all screen-detectable preclinical breast cancers and the frequency with which missed cancers may be limiting the efficacy of breast cancer screening.
The goal of reducing population mortality by screening mammography is conditional on the regular participation of 70% of women in the target age group.11 In Canada, the National Population Health Survey in 1996 indicated that 53.7% of women aged 50-69 years self-reported having had a screening mammogram in the previous 2 years. Of these women, we estimate that in 1996, close to one-quarter (21%) were screened through organized programs. There are no systematically collected data that would enable the assessment of the performance of opportunistic screening mammography that takes place outside the organized programs. Low participation rates in programs can be attributed to a number of factors including the lack of capacity to perform screening mammography within organized settings; the difficulty in shifting preventive health care practices from the use of opportunistic screening to the use of organized screening; an inability in some jurisdictions to access population lists that allow programs to personally invite women in the target age range; and a lack of understanding or disbelief concerning the potential benefits of regular screening mammography among women and physicians.
Participation in organized screening programs has probably increased substantially since 1996. In 1999, all provinces and one of the territories had organized programs. In addition, recent developments in provincial- and territory-based programs and in provincial policies (e.g., some provinces now reimburse radiologists for screening mammography only if it is conducted within organized programs) indicate that an increasing number of Canadian women will receive screening through organized programs. Such developments will allow for better monitoring of the results of screening and will add to the body of literature on the performance of screening mammography within Canada.14,15,18,19,20,21,22
An organized screening program permits the recruitment of women in target groups that are hard to reach, promotes increased return attendance, may decrease health care system costs, and includes routine and ongoing quality assurance, evaluation and overall program monitoring.15,23 The development of organized screening programs in Canada should help ensure that the population health benefits of breast cancer screening are realized for Canadian women.
These analyses show that it is possible to translate the benefits of breast cancer screening by mammography, as demonstrated under the rigorous conditions set in randomized controlled trials, into population-based community programs. More complete monitoring of the population effects of screening mammography would be possible if a greater proportion of current screening mammograms were performed within organized breast cancer screening programs.
Footnotes
This article has been peer reviewed.
Competing interests: None declared.
Reprint requests to: Ms. Judy Snider, Centre for Chronic Disease Prevention and Control, Health Canada, Tunney's Pasture, Ottawa ON K1A 0L2; fax: 613 941-2057; Judy_Snider@hc-sc.gc.ca
References
- 1.Kerlikowske K, Grady D, Rubin SM, Sandrock C, Ernster VL. Efficacy of screening mammography. A meta-analysis. JAMA 1995;273:149-54. [PubMed]
- 2.Shapiro S, Venet W, Strax P, Venet L, Roeser R. Ten to fourteen-year effect of screening on breast cancer mortality. J Natl Cancer Inst 1982;69:349-55. [PubMed]
- 3.Tabar L, Gad A, Holmberg LH, Ljungquist U, Fagerberg C, Baldetorp L. Reduction in mortality from breast cancer after mass screening with mammography: randomized trial from the Breast Cancer Screening Work Group of the Swedish National Board of Health and Welfare. Lancet 1985;i:829-32. [DOI] [PubMed]
- 4.Ballard-Barbash R, Klabunde C, Paci E, Broeders M, Coleman EA, Fracheboud J. Breast cancer screening in 21 countries: delivery of services, notification of results and outcomes ascertainment. Eur J Cancer Prev 1999;8:417-26. [DOI] [PubMed]
- 5.Shapiro S, Coleman EA, Broeders M, Codd M, de Koning H, Fracheboud J. Breast cancer screening programmes in 22 countries: current policies, administration and guidelines. Int J Epidemiol 1998;27:735-42. [DOI] [PubMed]
- 6.Moss SM, Michel M, Patnick J, Johns L, Blanks R, Chamberlain J. Results from the NHS breast screening programme 1990-1993. J Med Screen 1995;2:186-90. [DOI] [PubMed]
- 7.Fracheboud J, de Koning HJ, Beemsterboer PM, Boer R, Hendriks JH, Verbeek AL, et al. Nation-wide breast cancer screening in the Netherlands: results of initial and subsequent screening 1990-1995. National Evaluation Team for Breast Cancer Screening. Int J Cancer 1998;75:694-8. [DOI] [PubMed]
- 8.Thurfjell EL, Lindgren JAA. Population-based mammography screening in Swedish clinical practice: prevalence and incidence screening in Uppsala county. Radiology 1994;193:351-7. [DOI] [PubMed]
- 9.Rickard M, Donellan M. Diagnosis of small sized invasive breast cancer by an Australian mammography screening service: surrogate end-points for mortality reduction. Aust N Z J Surg 1998;68:415-8. [DOI] [PubMed]
- 10.Organized breast cancer screening programs in Canada. Ottawa: Health Canada; 1999. Cat no H1-9/13-1999.
- 11.Day NE, Williams DRR, Khaw KT. Breast cancer screening programmes: the development of a monitoring and evaluation system. Br J Cancer 1989;59:954-8. [DOI] [PMC free article] [PubMed]
- 12. Tabar L, Fagerberg G, Duffy SW, Day NE, Gad A, Grontoft O. Update of the Swedish two-county program of mammographic screening for breast cancer. Radiol Clin North Am 1992;30:187-209. [PubMed]
- 13.Population projections for Canada, provinces and territories 1993-2016. Ottawa: Statistics Canada; 1994. Cat no 91-520 occasional.
- 14.Bryant HE, Desautels JE, Castor WR, Horeczko N, Jackson F, Mah Z. Quality assurance and cancer detection rates in a provincial screening mammography program. Work in progress. Radiology 1993;188:811-6. [DOI] [PubMed]
- 15.Olivotto IA, Mates D, Kan L, Fung J, Samant R, Burhenne LJ. Prognosis, treatment and recurrence of breast cancer for women attending or not attending the Screening Mammography Program of British Colombia. Breast Cancer Res Treat 1999;54:73-81. [DOI] [PubMed]
- 16.Commonwealth Department of Human Services and Health. National Program for the Early Detection of Breast Cancer: national accreditation requirements. Canberra: The Department; 1994.
- 17.Ernster VL, Barclay J. Increases in ductal carcinoma in situ (DCIS) of the breast in relation to mammography: a dilemma. J Natl Cancer Inst Monogr 1997;(22):151-6. [DOI] [PubMed]
- 18.Caines JS, Chantziantoniou K, Wright BA, Konok GP, Iles SE, Bodurtha A, et al. Nova Scotia Breast Screening Program experience: use of needle core biopsy in the diagnosis of screening-detected abnormalities. Radiology 1996;198:125-30. [DOI] [PubMed]
- 19.Decker KM, Harrison M, Tate RB. Satisfaction of women attending the Manitoba Breast Screening Program. Prev Med 1999;29:22-7. [DOI] [PubMed]
- 20.Libstug AR, Moravan V, Aitken SE. Results from the Ontario breast screening program, 1990-1995. J Med Screen 1998;5:73-80. [DOI] [PubMed]
- 21.Mah Z, Bryant HE. The role of past mammography and future intentions in screening mammography usage. Cancer Detect Prev 1997;21:213-20. [PubMed]
- 22.Tonita JM, Hillis JP, Lim CH. Medical radiologic technologist review: effects on a population-based breast cancer screening program. Radiology 1999;211:529-33. [DOI] [PubMed]
- 23.Hakama M. Potential contribution of screening to cancer mortality reduction. Cancer Detect Prev 1993;17:513-20. [PubMed]