

This economic evaluation assesses the cost-effectiveness of atezolizumab plus bevacizumab vs sorafenib for patients with unresectable or metastatic hepatocellular carcinoma from a US payer perspective.
Key Points
Question
Is atezolizumab plus bevacizumab a cost-effective first-line treatment compared with sorafenib for unresectable or metastatic hepatocellular carcinoma from a US payer perspective?
Findings
In this economic evaluation of data from a hypothetical sample of 424 patients, compared with the standard sorafenib therapy, atezolizumab plus bevacizumab was associated with an incremental increase in quality-adjusted life-years per patient, with an incremental cost of $156 210 and an incremental cost-effectiveness ratio of $322 500 per quality-adjusted life-year.
Meaning
In this study, atezolizumab plus bevacizumab was associated with clinical benefit but was not cost-effective compared with sorafenib for first-line treatment of unresectable or metastatic hepatocellular carcinoma from a US payer perspective.
Abstract
Importance
Atezolizumab plus bevacizumab as a first-line therapy for patients with unresectable or metastatic hepatocellular carcinoma has been shown to improve overall and progression-free survival compared with standard sorafenib treatment. However, because of the high cost of atezolizumab plus bevacizumab, assessment of its value by considering both efficacy and cost is needed.
Objective
To evaluate the cost-effectiveness of atezolizumab plus bevacizumab vs sorafenib for patients with unresectable or metastatic hepatocellular carcinoma from a US payer perspective.
Design, Setting, and Participants
This economic evaluation was performed from June through September 2020, with a 6-year investment time period. Hypothetical patients were male and female adults 18 years or older who had a diagnosis of locally advanced metastatic or unresectable hepatocellular carcinoma confirmed by histologic or clinical features.
Main Outcomes and Measures
Health care costs (adjusted to 2020 US dollars), life-years, quality-adjusted life-years (QALYs), and incremental cost-effectiveness ratio (ICER) of atezolizumab plus bevacizumab vs sorafenib were examined using a partitioned survival model. One-way deterministic and probabilistic sensitivity analyses were used to examine model uncertainty. The model was also used to estimate price reductions of atezolizumab plus bevacizumab that would achieve more favorable cost-effectiveness.
Results
In the base case analysis of a hypothetical sample of 424 patients, atezolizumab plus bevacizumab was associated with an increase of 0.623 life-years (1.840 vs 1.218 life-years) and 0.484 QALYs (1.412 vs 0.928 QALYs) and with an incremental cost of $156 210 per patient compared with sorafenib. The ICER was $322 500 per QALY (5th to 95th percentile, $149 364-$683 744 per QALY), with 0.6% and 5.1% chance of being cost-effective at willingness-to-pay thresholds of $100 000 and $150 000 per QALY, respectively. The ICER never decreased below $150 000 per QALY in the 1-way sensitivity analyses. To achieve more favorable cost-effectiveness under the thresholds of $150 000 to $100 000 per QALY, the prices of atezolizumab and bevacizumab would need to be reduced by 37% to 47%.
Conclusions and Relevance
In this economic evaluation, atezolizumab plus bevacizumab was associated with clinical benefit but was not cost-effective compared with sorafenib for first-line treatment of unresectable or metastatic hepatocellular carcinoma from a US payer perspective. A substantial reduction in price for atezolizumab plus bevacizumab would be needed to achieve favorable cost-effectiveness for this new therapy.
Introduction
Hepatocellular carcinoma (HCC) is the most common type of liver cancer, accounting for more than 840 000 diagnosed cases and 780 000 deaths worldwide each year.1 Although early-stage disease may be cured by means of treatments such as resection, ablation, or liver transplantation, most patients present with unresectable disease at diagnosis and have a poor prognosis.2 According to the American Cancer Society, liver cancer incidence rates have more than tripled and the death rates have more than doubled since 1980, making it the fastest increasing cause of deaths due to cancer in the US.3
Sorafenib, an oral multikinase inhibitor, was the first approved systemic regimen for unresectable HCC based on results of a phase 3 trial showing a survival advantage over placebo.4 Until recently, no regimens have been demonstrated to be superior to sorafenib in phase 3 trials.5 However, the prognosis with sorafenib is only modestly improved, with a median duration of survival of 6.5 to 14.7 months.4,6,7,8,9,10,11,12,13
Atezolizumab is a fully humanized monoclonal antibody that selectively targets the protein programmed cell death ligand 1 (PD-L1) and restores T-cell immune activity.14 Bevacizumab is a fully humanized monoclonal antibody that targets vascular endothelial growth factor (VEGF),15 which plays important roles in tumor vascularization.16 In addition, anti-VEGF therapies may also enhance anti-programmed death 1 and anti–PD-L1 efficacy by reducing VEGF-mediated immunosuppression within the tumor microenvironment and promoting T-cell infiltration in tumors.17,18
Recently, the IMbrave150 phase 3 randomized clinical trial13 demonstrated a significant improvement in survival with use of atezolizumab plus bevacizumab compared with use of sorafenib in patients with unresectable or metastatic HCC who had not previously received systemic therapy (hazard ratio [HR], 0.58; 95% CI, 0.42-0.79).13 Until now, the combination is the only regimen demonstrated to be superior to the standard sorafenib in phase 3 trials. The overall incidence rates of grade 3 or 4 adverse events were similar in the 2 treatment groups (56.5% for atezolizumab plus bevacizumab vs 55.1% for sorafenib).13 Atezolizumab plus bevacizumab was subsequently approved by the US Food and Drug Administration in May 2020 and has become a new first-line standard of care.19 The objective of this study was to evaluate the cost-effectiveness of atezolizumab plus bevacizumab vs sorafenib as the first-line treatment for patients with unresectable or metastatic HCC from a US payer perspective.
Methods
Patients and Intervention
This economic evaluation was performed at Xi’an Jiaotong University in Xi’an, China, from June through September 2020. The study was deemed exempt from institutional review board approval by the Second Affiliated Hospital of Xi’an Jiaotong University because it did not involve human participants. This study followed the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) reporting guideline.20
The target patient population was the same as that from the IMbrave150 trial.13 Included patients were adults (aged ≥18 years) who had locally advanced metastatic or unresectable HCC or both, with diagnosis confirmed by histologic or clinical features.21 Other inclusion criteria were no history of systemic therapy, a performance status of 0 or 1 on the Eastern Cooperative Group scale, and adequate hematologic and organ function.
Included patients received either first-line atezolizumab-bevacizumab (atezolizumab, 1200 mg, plus bevacizumab, 15 mg per kilogram of body weight, intravenously every 3 weeks) or first-line sorafenib (400 mg orally twice daily). When disease progressed or unacceptable adverse events occurred, the first-line treatments were discontinued and patients in both arms of the study could receive second-line treatments until death. In the IMbrave150 trial,13 69 of 266 patients (25.9%) in the atezolizumab plus bevacizumab arm and 73 of 158 patients (46.2%) in the sorafenib arm received second-line treatment. Tyrosine kinase inhibitors (including regorafenib and cabozantinib) were the second-line options for both arms.13 In addition, the patients in the sorafenib arm could receive immunotherapy as second-line treatment.13
Model Construction
A partitioned survival model was developed to compare health care costs and clinical outcomes associated with atezolizumab plus bevacizumab vs sorafenib for treatment of patients with unresectable or metastatic HCC. The model is frequently used in late-stage oncology modeling.22 The time horizon was 6 years, and more than 98.5% patients died in both treatment arms (Figure 1). The cycle length was 1 month (30 days). The analysis was conducted from a US payer perspective. The primary outputs of the model were cost, life-years, quality-adjusted life-years (QALYs), and incremental cost-effectiveness ratio (ICER). Both costs and clinical outcomes were discounted by 3% annually.23 A willingness-to-pay threshold of $100 000 or $150 000 per QALY gained was used to determine cost efficacy.24,25 The model was constructed using TreeAge Pro 2020 (TreeAge Software).
Figure 1. Fitted Kaplan-Meier Models With Weibull Tails for Overall Survival and Progression-Free Survival.

For each treatment arm (atezolizumab plus bevacizumab and sorafenib) and each end point (overall survival and progression-free survival), event time distributions were estimated using a mixed model with a Kaplan-Meier survival estimator up to the last follow-up and Weibull distribution for the tail after the last follow-up. The IMbrave150 trial only reported survival data within 17 months; thus, the numbers of individuals at risk were not available beyond this period.
Probabilities of overall survival (OS) and progression-free survival (PFS) for atezolizumab plus bevacizumab and sorafenib were extracted from Kaplan-Meier curves in the IMbrave150 trial13 using GetData Graph Digitizer.26 For each treatment arm (atezolizumab plus bevacizumab and sorafenib) and each end point (OS and PFS), event time distributions were estimated using a mixed model, with a Kaplan-Meier survival estimator up to the last follow-up visit and Weibull distribution for the tail after the last follow-up visit. Weibull distributions were generated on the basis of extracted data from Kaplan-Meier curves in IMbrave150 using the methods described by Hoyle and Henley.27 The Weibull distribution was selected because it seemed more biologically and clinically plausible than logarithmic models.28 Fitted mixed models are shown in Figure 1.
Costs
Only direct medical costs were considered, including costs for drugs, drug administration, follow-up visits, management of adverse events, and end-of-life care. Atezolizumab and bevacizumab costs were obtained from the Centers for Medicare & Medicaid Services.29 Body weight was not reported in the IMbrave150 trial. A mean body weight of 73 kg, adopted from an HCC cohort, was used for dose calculation of bevacizumab.30 Sorafenib cost was obtained from Micromedex Redbook Online.31,32 Dose intensity was assumed to be 95% for atezolizumab, 93% for bevacizumab, and 84% for sorafenib, as observed in the IMbrave150 trial.13 Thus, the cost of sorafenib per month would be $14 767.65 ($586.018 per day × 30 days × 0.84 for 400 mg orally twice daily). Regorafenib and cabozantinib costs were also obtained from Micromedex Redbook,31 and dose reduction was based on results of previous studies32,33,34,35,36,37,38 (eTable 1 in the Supplement). Administration costs were obtained from the Medicare physician fee schedule for 2020.39
Patients in both arms of the study were assumed to be routinely followed up until death. The follow-up costs included physician visits, laboratory tests, and imaging (eTable 1 in the Supplement). Patients who experienced disease progression had greater follow-up costs than those who entered the study before disease progression occurred. End-of-life cost was allocated when a patient died, and cost was assumed to be equivalent in both arms.
Grade 3 to 4 adverse events that occurred in 2% or more of the patients in the IMbrave150 trial were included in the model. The related costs were derived from previously published studies32,33,34,35,36,37,38 (eTable 1 in the Supplement). All costs were converted to 2020 US dollars using the medical component of the Consumer Price Index.40
Utilities
Utility values were not reported in the IMbrave150 trial. Kobayashi et al41 calculated utility values by analyzing patient-level data on health-related quality of life in the REFLECT trial, a noninferiority trial in which lenvatinib was compared with sorafenib.11 In this trial, health-related quality of life was assessed using the 3-level version of the European Quality of Life 5-Dimension questionnaire.11 According to Kobayashi et al,41 the utility values were 0.837 for a progression-free patient with sorafenib treatment after subtracting adverse event disutilities and 0.714 for a patient with disease progression. In the base case of the present analysis, these utility values were used for patients receiving sorafenib treatment because the characteristics of patients in the IMbrave150 and REFLECT trials were similar. Data were not available to calculate utility values for atezolizumab-bevacizumab treatment. They were assumed to be the same as those for sorafenib.41
Sensitivity Analyses
A series of sensitivity analyses were performed to assess the robustness of the model and to address the uncertainty in estimates of variables. Hazard ratios, incidences of adverse events, rates of treatment discontinuation, and second-line treatment proportions were varied over their 95% CIs. A wide range of utility values was derived from previous studies32,33,34,35,36,37,38 (eTable 1 in the Supplement). Cost ranges were derived from previously published studies41,42,43 if available; otherwise, a variance of 25% from base case values was assumed. In 1-way sensitivity analyses, the association of each aforementioned parameter with ICERs was examined over its defined range. The ranges of model inputs for sensitivity analyses are listed in eTable 1 in the Supplement. In addition, we estimated price reductions for atezolizumab plus bevacizumab that would achieve more favorable cost-effectiveness under the thresholds of $150 000 to $100 000 per QALY.
A probabilistic sensitivity analysis was performed using 10 000 Monte Carlo simulations; random sampling from the distributions of all parameters was done each time. Distributions were assumed based on parameter types: gamma distribution for costs and body weight; log-normal distribution for HRs; and β distribution for utility, incidences of adverse events, rates of treatment discontinuation, and second-line treatment proportions (eTable 1 in the Supplement).
In the subgroup analyses, the ICER was calculated for each subgroup using the subgroup-specific HRs for OS and PFS obtained from the IMbrave150 trial (eTable 2 in the Supplement). Because of the lack of sufficient data, the same data were assumed for all subgroups except for the subgroup-specific HRs for OS and PFS.
Results
Base Case Results
The base case analysis assessed a hypothetical sample of 424 patients. Results of the base case cost-effectiveness analysis are shown in the Table. Atezolizumab plus bevacizumab treatment was associated with significantly higher health care costs per patient compared with standard treatment with sorafenib ($313 193 vs $156 984), with an incremental cost of $156 210. Of this incremental cost, drug cost accounted for $145 217 and nondrug cost accounted for $10 993. Atezolizumab plus bevacizumab treatment was associated with an improvement of 0.623 life-years (1.840 vs 1.218 life-years) and 0.484 QALY (1.412 vs 0.928 QALYs) per patient compared with standard treatment with sorafenib. The ICER for atezolizumab plus bevacizumab vs sorafenib was estimated to be $322 500 per QALY.
Table. Base Case Results per Patient.
| Results | Atezolizumab plus bevacizumab | Sorafenib | Incremental change |
|---|---|---|---|
| Life-years | 1.840 | 1.218 | 0.623 |
| QALYs | 1.412 | 0.928 | 0.484 |
| Cost, US$ | |||
| Total | 313 193 | 156 984 | 156 210 |
| Druga | 240 137 | 94 920 | 145 217 |
| Nondrugb | 73 056 | 62 064 | 10 993 |
| ICERs, US$ | |||
| Per life-year | NA | NA | 250 907 |
| Per QALY | NA | NA | 322 500 (149 364-683 744)c |
Abbreviations: ICER, incremental cost-effectiveness ratio; NA, not applicable; QALY, quality-adjusted life-year.
Drug cost includes the costs of first- and second-line drugs and administration costs.
Nondrug cost includes the costs of adverse event management, end-of-life care, and follow-up care covering physician visits, laboratory tests, and imaging.
Values in parentheses represent the 5th to 95th percentile range derived from the results of probabilistic sensitivity analysis.
Sensitivity Analyses
The results of 1-way sensitivity analyses are shown in Figure 2. The HR for OS had the greatest influence on the ICER, followed by patient weight, HR for PFS, cost of atezolizumab, utility of progression-free state, cost of bevacizumab, cost of sorafenib, and utility of postprogression state. The associations of other variables with the ICER were negligible. Across a broad variation in the ranges for each variable, the ICER remained greater than $150 000 per QALY. To achieve more-favorable cost-effectiveness under the thresholds of $150 000 to $100 000 per QALY, the price of atezolizumab plus bevacizumab combination treatment would need to be reduced by 37% to 47%.
Figure 2. Tornado Diagram Showing Results of a 1-Way Sensitivity Analysis.
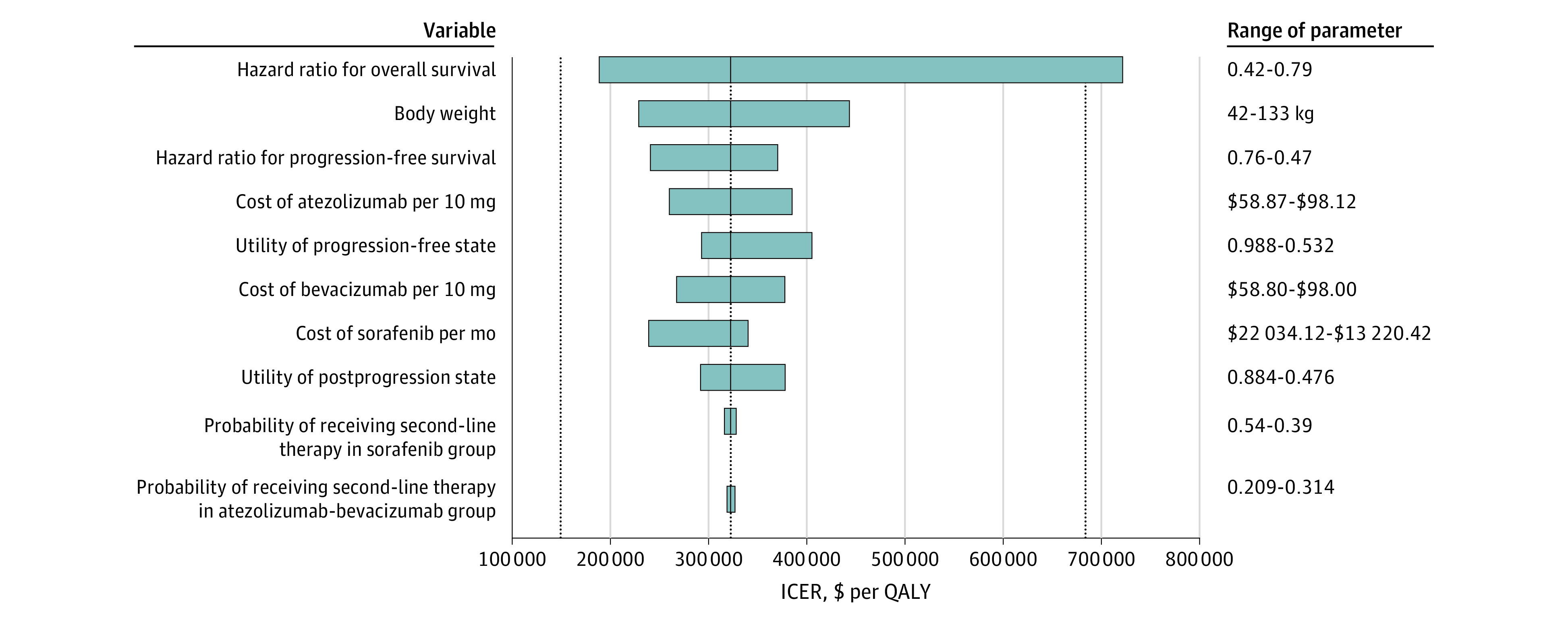
The 10 most influential variables are presented. The dotted line in the middle represents the incremental cost-effectiveness ratio (ICER) of $322 500 per quality-adjusted life-year (QALY) from the base case results. The left and right dotted lines represent the 5th ($149 364 per QALY) and 95th ($683 744 per QALY) per percentiles of ICER, respectively, from the results of probabilistic sensitivity analysis.
In a probabilistic sensitivity analysis of 10 000 simulations, the 5th to 95th percentile range for the ICER was estimated to be $149 364 per QALY to $683 744 per QALY. The cost-effectiveness acceptability curves suggested that the probability of atezolizumab plus bevacizumab being cost-effective compared with sorafenib was 0.6% and 5.1% at willingness-to-pay thresholds of $100 000 and $150 000 per QALY, respectively (Figure 3). A scatterplot showing the 10 000 simulations is presented in the eFigure in the Supplement. The results of subgroup analyses showed that the ICER for atezolizumab plus bevacizumab vs sorafenib was greater than $150 000 per QALY for all patients in clinically relevant subgroups (eTable 2 in the Supplement).
Figure 3. Cost-effectiveness Acceptability Curves.

The curves show the probabilities of being cost-effective at different willingness-to-pay thresholds for atezolizumab plus bevacizumab and sorafenib. QALY, quality-adjusted life-year.
Discussion
To date, atezolizumab plus bevacizumab is currently the first and only treatment superior to sorafenib, the standard of care for unresectable or metastatic HCC.13 Thus, the drug was approved as a new first-line therapy for patients with this disease. However, based on our model, the cost of the new treatment doubled because of higher drug costs. Atezolizumab plus bevacizumab cost $322 500 per additional QALY gained compared with sorafenib from a US payer perspective. The probabilistic sensitivity analysis revealed that the probability of atezolizumab plus bevacizumab being cost-effective was 0.6% and 5.1% at willingness-to-pay thresholds of $100 000 and $150 000 per QALY, respectively. The uncertainty analysis suggests a high likelihood that atezolizumab plus bevacizumab exceeds the usually accepted values for cost-effective incremental costs of care.25
In the 1-way sensitivity analyses, HRs for OS and PFS, drug costs, and health utilities were the most influential parameters. However, across a wide range of each of these parameters, atezolizumab plus bevacizumab was still not cost-effective compared with sorafenib at the willingness-to-pay threshold of $150 000 per QALY. Studies of other malignant neoplasms have suggested improved cost-effectiveness of immunotherapy in certain subgroups of patients.44,45,46 In the present study regarding unresectable or metastatic HCC, an association between treatment and cost-effectiveness was not found in any subgroup, but the results should be interpreted with caution because of the small sample size for each group and the exploratory nature of subgroup analyses.
The willingness-to-pay threshold can substantially affect the cost-effectiveness of a therapy. Drugs used to treat cancer often have higher ICERs than other drugs, and a value of $100 000 or $150 000 per QALY has been suggested as the willingness-to-pay threshold in the US.24,25 Nevertheless, the US Food and Drug Administration approves new drugs used in cancer treatment based on their efficacy and safety. Many of these drugs are used despite an ICER greater than $100 000 or $150 000 per QALY. The present study showed an ICER of $322 500 per QALY for atezolizumab plus bevacizumab vs sorafenib, which is higher than those thresholds. This finding does not suggest opposition to the use of atezolizumab plus bevacizumab for patients with late-stage HCC but rather suggests that policy makers spend more resources on more cost-effective interventions (eg, HCC screening for patients with cirrhosis47) so that they can maximize health gains with a fixed budget by choosing interventions with ICERs from the lowest to highest until the available resources are consumed.25
Recently, a study showed a similar cost-effectiveness balance in China; even in comparison with the present study, atezolizumab plus bevacizumab was reported with more QALYs gained (0.811 QALY) and a substantial reduction in incremental cost ($49 994) because of drug donation programs.48 But the study reported a markedly long OS of 1.736 years (20.832 months) associated with sorafenib compared with results of published phase 3 trials of treatment for unresectable or metastatic HCC.4,6,7,8,9,10,11,12,13 To our knowledge, no other cost-effectiveness analyses of immune checkpoint inhibitors for HCC have been published. Previously, these drugs were evaluated for treatment of other recurrent or metastatic malignant neoplasms, such as head and neck cancers, non–small cell lung cancer, renal cell cancer, and melanoma.49 Because development costs are high, the prices of immune checkpoint inhibitors are often high.50 Thus, it is not uncommon to see an immune checkpoint inhibitor that is not cost-effective mentioned in published economic evaluations. In the present analysis, the addition of bevacizumab (an anti–vascular endothelial growth factor agent) to the immune checkpoint inhibitor atezolizumab made the combination more expensive. If generics or biosimilars can be generated in the future and if government negotiation with pharmaceutical companies is successful, drug prices may decrease so that atezolizumab plus bevacizumab can be affordable.50 As the present analysis has shown, reduction of ICERs to more widely acceptable values requires a substantial price reduction for the combination of atezolizumab plus bevacizumab (37% to 47%).
Limitations
This study has limitations. First, the long-term efficacy of atezolizumab plus bevacizumab for the treatment of unresectable or metastatic HCC remains a question. In long-term follow-up for patients with other malignant neoplasms who received immunotherapy, a plateau appeared on the tail of the survival curve.51,52 The possibility of long-term survival with atezolizumab plus bevacizumab would alter the effectiveness implemented in the model, but it also raises the question of when to stop immunotherapy in a responding patient. In addition, responding patients, although only accounting for a small proportion, may have the opportunity to undergo surgical resection; however, the long-term benefit is unknown, and resection may increase the cost of treatment.
Second, to our knowledge, the IMbrave150 trial13 is the only phase 3 randomized clinical trial in which atezolizumab plus bevacizumab was compared with sorafenib for the treatment of unresectable or metastatic HCC. Parameters of efficacy and safety in the model essentially relied on results of this trial. Any biases within the trial may have affected the cost and effectiveness. For example, the patients enrolled in IMbrave150 were healthier than the general population of patients with unresectable or metastatic HCC, and patients participating in clinical trials often have better adherence to treatment than do those in real-world practice.53
Third, the utility values in the model were not estimated from the IMbrave150 study but from the REFLECT study, in which lenvatinib was compared with sorafenib.12,41 In the present study, the value was directly used for the sorafenib treatment arm because the target patients and adverse events with sorafenib treatment were comparable between the 2 studies.11,13 The IMbrave150 trial showed that atezolizumab plus bevacizumab significantly delayed the decline in quality of life and functioning, even in patients with disease progression.13 Thus, the assumption of the same utility value in both arms in the base case may have underestimated the effectiveness of atezolizumab plus bevacizumab. However, the underestimation would not have changed the cost-effectiveness balance. Even if no utility reduction occurred after disease progression during treatment with atezolizumab plus bevacizumab, an ICER of $255 058 per QALY would still be higher than the willingness-to-pay thresholds.
The present study did not include evaluation of lenvatinib, which is another first-line treatment approved for unresectable or metastatic HCC in the US. Because of similar clinical effectiveness and lower cost compared with sorafenib,11 atezolizumab plus bevacizumab would not be cost-effective compared with lenvatinib.
Conclusions
The findings of this economic evaluation suggest that from the perspective of US payers, atezolizumab plus bevacizumab is unlikely to be cost-effective under current drug pricing at willingness-to-pay thresholds of $100 000 to $150 000 per QALY compared with sorafenib for patients with unresectable or metastatic HCC who have not received systemic therapy. A substantial price reduction for the combination of atezolizumab plus bevacizumab would be needed to achieve favorable cost-effectiveness for this new therapy.
eTable 1. Model Parameters: Baseline Values, Ranges, and Distributions for Sensitivity Analyses
eTable 2. Results for Subgroup Analyses
eFigure. Scatter Plot of Probabilistic Sensitivity Analysis
eReferences.
References
- 1.Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394-424. doi: 10.3322/caac.21492 [DOI] [PubMed] [Google Scholar]
- 2.Park JW, Chen M, Colombo M, et al. Global patterns of hepatocellular carcinoma management from diagnosis to death: the BRIDGE Study. Liver Int. 2015;35(9):2155-2166. doi: 10.1111/liv.12818 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7-30. doi: 10.3322/caac.21590 [DOI] [PubMed] [Google Scholar]
- 4.Llovet JM, Ricci S, Mazzaferro V, et al. ; SHARP Investigators Study Group . Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359(4):378-390. doi: 10.1056/NEJMoa0708857 [DOI] [PubMed] [Google Scholar]
- 5.Villanueva A. Hepatocellular carcinoma. N Engl J Med. 2019;380(15):1450-1462. doi: 10.1056/NEJMra1713263 [DOI] [PubMed] [Google Scholar]
- 6.Cheng AL, Kang YK, Chen Z, et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009;10(1):25-34. doi: 10.1016/S1470-2045(08)70285-7 [DOI] [PubMed] [Google Scholar]
- 7.Cheng AL, Kang YK, Lin DY, et al. Sunitinib versus sorafenib in advanced hepatocellular cancer: results of a randomized phase III trial. J Clin Oncol. 2013;31(32):4067-4075. doi: 10.1200/JCO.2012.45.8372 [DOI] [PubMed] [Google Scholar]
- 8.Johnson PJ, Qin S, Park JW, et al. Brivanib versus sorafenib as first-line therapy in patients with unresectable, advanced hepatocellular carcinoma: results from the randomized phase III BRISK-FL study. J Clin Oncol. 2013;31(28):3517-3524. doi: 10.1200/JCO.2012.48.4410 [DOI] [PubMed] [Google Scholar]
- 9.Cainap C, Qin S, Huang WT, et al. Linifanib versus sorafenib in patients with advanced hepatocellular carcinoma: results of a randomized phase III trial. J Clin Oncol. 2015;33(2):172-179. doi: 10.1200/JCO.2013.54.3298 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Zhu AX, Rosmorduc O, Evans TRJ, et al. SEARCH: a phase III, randomized, double-blind, placebo-controlled trial of sorafenib plus erlotinib in patients with advanced hepatocellular carcinoma. J Clin Oncol. 2015;33(6):559-566. doi: 10.1200/JCO.2013.53.7746 [DOI] [PubMed] [Google Scholar]
- 11.Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163-1173. doi: 10.1016/S0140-6736(18)30207-1 [DOI] [PubMed] [Google Scholar]
- 12.Yau T, Park JW, Finn RS, et al. LBA38_PR-CheckMate 459: a randomized, multi-center phase III study of nivolumab (NIVO) vs sorafenib (SOR) as first-line (1L) treatment in patients (pts) with advanced hepatocellular carcinoma (aHCC). Ann Oncol. 2019;30(suppl 5):v874-v875. doi: 10.1093/annonc/mdz394.029 [DOI] [Google Scholar]
- 13.Finn RS, Qin S, Ikeda M, et al. ; IMbrave150 Investigators . Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382(20):1894-1905. doi: 10.1056/NEJMoa1915745 [DOI] [PubMed] [Google Scholar]
- 14.Herbst RS, Soria JC, Kowanetz M, et al. Predictive correlates of response to the anti-PD-L1 antibody MPDL3280A in cancer patients. Nature. 2014;515(7528):563-567. doi: 10.1038/nature14011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ferrara N, Hillan KJ, Novotny W. Bevacizumab (Avastin), a humanized anti-VEGF monoclonal antibody for cancer therapy. Biochem Biophys Res Commun. 2005;333(2):328-335. doi: 10.1016/j.bbrc.2005.05.132 [DOI] [PubMed] [Google Scholar]
- 16.Finn RS, Bentley G, Britten CD, Amado R, Busuttil RW. Targeting vascular endothelial growth factor with the monoclonal antibody bevacizumab inhibits human hepatocellular carcinoma cells growing in an orthotopic mouse model. Liver Int. 2009;29(2):284-290. doi: 10.1111/j.1478-3231.2008.01762.x [DOI] [PubMed] [Google Scholar]
- 17.Voron T, Colussi O, Marcheteau E, et al. VEGF-A modulates expression of inhibitory checkpoints on CD8+ T cells in tumors. J Exp Med. 2015;212(2):139-148. doi: 10.1084/jem.20140559 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Wallin JJ, Bendell JC, Funke R, et al. Atezolizumab in combination with bevacizumab enhances antigen-specific T-cell migration in metastatic renal cell carcinoma. Nat Commun. 2016;7:12624. doi: 10.1038/ncomms12624 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.US Food and Drug Administration . FDA approves atezolizumab plus bevacizumab for unresectable hepatocellular carcinoma. Published June 1, 2020. Accessed July 16, 2020. https://www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-atezolizumab-plus-bevacizumab-unresectable-hepatocellular-carcinoma
- 20.Husereau D, Drummond M, Petrou S, et al. ; CHEERS Task Force . Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement. BMJ. 2013;346:f1049. doi: 10.1136/bmj.f1049 [DOI] [PubMed] [Google Scholar]
- 21.Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guidance by the American Association for the Study of Liver Diseases. Hepatology. 2018;68(2):723-750. doi: 10.1002/hep.29913 [DOI] [PubMed] [Google Scholar]
- 22.York Health Economics Consortium . Partitioned survival model. Published 2016. Accessed July 16, 2020. https://yhec.co.uk/glossary/partitioned-survival-model/
- 23.Weinstein MC, Siegel JE, Gold MR, Kamlet MS, Russell LB. Recommendations of the Panel on Cost-effectiveness in Health and Medicine. JAMA. 1996;276(15):1253-1258. doi: 10.1001/jama.1996.03540150055031 [DOI] [PubMed] [Google Scholar]
- 24.Bae YHJ, Mullins CD. Do value thresholds for oncology drugs differ from nononcology drugs? J Manag Care Spec Pharm. 2014;20(11):1086-1092. doi: 10.18553/jmcp.2014.20.11.1086 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Neumann PJ, Cohen JT, Weinstein MC. Updating cost-effectiveness—the curious resilience of the $50,000-per-QALY threshold. N Engl J Med. 2014;371(9):796-797. doi: 10.1056/NEJMp1405158 [DOI] [PubMed] [Google Scholar]
- 26.GetData . Graph Digitizer. Accessed June 15, 2020. http://www.getdata-graph-digitizer.com/index.php
- 27.Hoyle MW, Henley W. Improved curve fits to summary survival data: application to economic evaluation of health technologies. BMC Med Res Methodol. 2011;11:139. doi: 10.1186/1471-2288-11-139 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Cammà C, Cabibbo G, Petta S, et al. ; WEF study group; SOFIA study group . Cost-effectiveness of sorafenib treatment in field practice for patients with hepatocellular carcinoma. Hepatology. 2013;57(3):1046-1054. doi: 10.1002/hep.26221 [DOI] [PubMed] [Google Scholar]
- 29.Centers for Medicare & Medicaid Services . 2020 ASP drug pricing files. Published 2020. Accessed August 18, 2020. https://www.cms.gov/medicare/medicare-part-b-drug-average-sales-price/2020-asp-drug-pricing-files
- 30.Grossman RL, Heath AP, Ferretti V, et al. Toward a shared vision for cancer genomic data. N Engl J Med. 2016;375(12):1109-1112. doi: 10.1056/NEJMp1607591 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Truven Health Analytics . Micromedex Redbook Online. Published 2017. Accessed March 16, 2017. https://www.ibm.com/products/micromedex-red-book
- 32.Wilson L, Huang W, Chen L, Ting J, Cao V. Cost Effectiveness of lenvatinib, sorafenib and placebo in treatment of radioiodine-refractory differentiated thyroid cancer. Thyroid. 2017;27(8):1043-1052. doi: 10.1089/thy.2016.0572 [DOI] [PubMed] [Google Scholar]
- 33.Barzey V, Atkins MB, Garrison LP, Asukai Y, Kotapati S, Penrod JR. Ipilimumab in 2nd line treatment of patients with advanced melanoma: a cost-effectiveness analysis. J Med Econ. 2013;16(2):202-212. doi: 10.3111/13696998.2012.739226 [DOI] [PubMed] [Google Scholar]
- 34.Konijeti GG, Grandhe S, Tincopa M, et al. Cost-effectiveness analysis of screening for hepatitis B virus infection in patients with solid tumors before initiating chemotherapy. Clin Gastroenterol Hepatol. 2020;18(7):1600-1608.e4. doi: 10.1016/j.cgh.2019.10.039 [DOI] [PubMed] [Google Scholar]
- 35.Hornberger J, Hirsch FR, Li Q, Page RD. Outcome and economic implications of proteomic test-guided second- or third-line treatment for advanced non-small cell lung cancer: extended analysis of the PROSE trial. Lung Cancer. 2015;88(2):223-230. doi: 10.1016/j.lungcan.2015.03.006 [DOI] [PubMed] [Google Scholar]
- 36.Patel DA, Holdford DA, Edwards E, Carroll NV. Estimating the economic burden of food-induced allergic reactions and anaphylaxis in the United States. J Allergy Clin Immunol. 2011;128(1):110-115.e5. doi: 10.1016/j.jaci.2011.03.013 [DOI] [PubMed] [Google Scholar]
- 37.Kacker S, Ness PM, Savage WJ, et al. The cost-effectiveness of platelet additive solution to prevent allergic transfusion reactions. Transfusion. 2013;53(11):2609-2618. doi: 10.1111/trf.12095 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Imperiale TF, Klein RW, Chalasani N. Cost-effectiveness analysis of variceal ligation vs. beta-blockers for primary prevention of variceal bleeding. Hepatology. 2007;45(4):870-878. doi: 10.1002/hep.21605 [DOI] [PubMed] [Google Scholar]
- 39.Centers for Medicare & Medicaid Services . Medicare physician fee schedule. Published 2020. Accessed August 18, 2020. https://www.cms.gov/apps/physician-fee-schedule/license-agreement.aspx
- 40.FRED Economic Data. Economic Research: Federal Reserve Bank of St Louis. Consumer Price Index for all urban consumers: medical care in U.S. city average. Accessed August 18, 2020. https://fred.stlouisfed.org/series/CPIMEDSL
- 41.Kobayashi M, Kudo M, Izumi N, et al. Cost-effectiveness analysis of lenvatinib treatment for patients with unresectable hepatocellular carcinoma (uHCC) compared with sorafenib in Japan. J Gastroenterol. 2019;54(6):558-570. doi: 10.1007/s00535-019-01554-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Liao W, Huang J, Hutton D, et al. Cost-effectiveness analysis of cabozantinib as second-line therapy in advanced hepatocellular carcinoma. Liver Int. 2019;39(12):2408-2416. doi: 10.1111/liv.14257 [DOI] [PubMed] [Google Scholar]
- 43.Parikh ND, Singal AG, Hutton DW. Cost effectiveness of regorafenib as second-line therapy for patients with advanced hepatocellular carcinoma. Cancer. 2017;123(19):3725-3731. doi: 10.1002/cncr.30863 [DOI] [PubMed] [Google Scholar]
- 44.Matter-Walstra K, Schwenkglenks M, Aebi S, et al. ; Swiss Group for Clinical Cancer Research . A cost-effectiveness analysis of nivolumab versus docetaxel for advanced nonsquamous NSCLC including PD-L1 testing. J Thorac Oncol. 2016;11(11):1846-1855. doi: 10.1016/j.jtho.2016.05.032 [DOI] [PubMed] [Google Scholar]
- 45.Aguiar PN Jr, Perry LA, Penny-Dimri J, et al. The effect of PD-L1 testing on the cost-effectiveness and economic impact of immune checkpoint inhibitors for the second-line treatment of NSCLC. Ann Oncol. 2017;28(9):2256-2263. doi: 10.1093/annonc/mdx305 [DOI] [PubMed] [Google Scholar]
- 46.Zargar M, McFarlane T, Chan KKW, Wong WWL. Cost-effectiveness of nivolumab in recurrent metastatic head and neck squamous cell carcinoma. Oncologist. 2018;23(2):225-233. doi: 10.1634/theoncologist.2017-0277 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Cadier B, Bulsei J, Nahon P, et al. ; ANRS CO12 CirVir and CHANGH groups . Early detection and curative treatment of hepatocellular carcinoma: a cost-effectiveness analysis in France and in the United States. Hepatology. 2017;65(4):1237-1248. doi: 10.1002/hep.28961 [DOI] [PubMed] [Google Scholar]
- 48.Hou Y, Wu B. Atezolizumab plus bevacizumab versus sorafenib as first-line treatment for unresectable hepatocellular carcinoma: a cost-effectiveness analysis. Cancer Commun (Lond). 2020;40(12):743-745. doi: 10.1002/cac2.12110 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Verma V, Sprave T, Haque W, et al. A systematic review of the cost and cost-effectiveness studies of immune checkpoint inhibitors. J Immunother Cancer. 2018;6(1):128. doi: 10.1186/s40425-018-0442-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Siddiqui M, Rajkumar SV. The high cost of cancer drugs and what we can do about it. Mayo Clin Proc. 2012;87(10):935-943. doi: 10.1016/j.mayocp.2012.07.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Gettinger S, Horn L, Jackman D, et al. Five-year follow-up of nivolumab in previously treated advanced non-small-cell lung cancer: results from the CA209-003 study. J Clin Oncol. 2018;36(17):1675-1684. doi: 10.1200/JCO.2017.77.0412 [DOI] [PubMed] [Google Scholar]
- 52.Topalian SL, Hodi FS, Brahmer JR, et al. Five-year survival and correlates among patients with advanced melanoma, renal cell carcinoma, or non-small cell lung cancer treated with nivolumab. JAMA Oncol. 2019;5(10):1411-1420. doi: 10.1001/jamaoncol.2019.2187 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Flather M, Delahunty N, Collinson J. Generalizing results of randomized trials to clinical practice: reliability and cautions. Clin Trials. 2006;3(6):508-512. doi: 10.1177/1740774506073464 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eTable 1. Model Parameters: Baseline Values, Ranges, and Distributions for Sensitivity Analyses
eTable 2. Results for Subgroup Analyses
eFigure. Scatter Plot of Probabilistic Sensitivity Analysis
eReferences.