

Key Points
Question
What are the outcomes following mandatory nonmedical switching from adalimumab originator to adalimumab biosimilars?
Findings
This cohort study of 378 patients treated with adalimumab originator and 348 patients treated with adalimumab biosimilars found no difference in drug retention before and after the switch.
Meaning
In this cohort study, a nonmedical switch from adalimumab originator to an adalimumab biosimilar was not associated with drug retention.
Abstract
Importance
The efficacy of adalimumab biosimilars is similar to that of brand-name adalimumab (Humira, hereinafter originator) in clinical trials. However, limited knowledge about real-world data exists for adalimumab biosimilars.
Objective
To assess the outcomes following a mandatory nonmedical switch from adalimumab originator to adalimumab biosimilars in patients with psoriasis.
Design, Setting, and Participants
This cohort study assesses the outcomes following a switch from adalimumab originator to an adalimumab biosimilar. Patients in the Biological Treatment in Danish Dermatology (DERMBIO) registry, a Danish nationwide registry of all patients treated with biologics (including biosimilars) for psoriasis since 2007, were assessed for eligibility. All patients who switched from adalimumab originator to an adalimumab biosimilar between November 1, 2018, and May 1, 2019, were included in the adalimumab biosimilar cohort. All patients with a visit between May 1, 2017, and November 1, 2017, treated with adalimumab originator were included in the adalimumab originator cohort. Data were analyzed from June 1, 2020, to October 10, 2021.
Exposure
Switch from adalimumab originator to an adalimumab biosimilar.
Main Outcomes and Measures
The primary outcome was 1-year drug retention in patients switching to adalimumab biosimilars compared with patients treated with adalimumab originator. Crude and adjusted retention rates for the adalimumab biosimilar cohort were compared with the adalimumab originator cohort with Cox proportional hazards regression using robust variance.
Results
A total of 348 patients were included in the adalimumab biosimilar cohort (mean [SD] age, 52.2 [13.6] years; 251 [72.1%] male) and 378 patients in the adalimumab originator cohort (mean [SD] age, 51.1 [14.1] years; 272 [72.0%] male). The 1-year drug retention rates were 92.0% (95% CI, 89.0%-94.9%) for the adalimumab biosimilar cohort and 92.1% (95% CI, 89.4%-94.8%) for the adalimumab originator cohort. Similar hazard ratios were observed between the 2 cohorts. The crude hazard ratios were 1.02 (95% CI, 0.61-1.70; P = .94) for all causes of drug discontinuation, 0.82 (95% CI, 0.39-1.73; P = .60) for insufficient effect, and 1.41 (95% CI, 0.52-3.77; P = .50) for adverse events for the adalimumab biosimilar cohort when compared with the adalimumab originator cohort.
Conclusions and Relevance
In this cohort study from Denmark, a nonmedical switch from adalimumab originator to adalimumab biosimilars was not associated with drug retention.
This cohort study assesses the outcomes following a mandatory nonmedical switch from adalimumab originator to adalimumab biosimilars in patients with psoriasis.
Introduction
Biologics are large molecules that target specific parts of the immune system and are often reserved for last-line treatment in patients with psoriasis. During recent years, patents of several brand-name biologics have expired, which has led to the introduction of drugs called biosimilars, which have similar structures and mechanisms of action as the originator biologics.1 Biosimilars for psoriasis are currently available for the tumor necrosis factor α inhibitors etanercept, infliximab, and most recently adalimumab.2 A common approach in the approval of biosimilars is the use of preclinical data and a clinical trial demonstrating biosimilarity (noninferiority and nonsuperiority) to the originator biologic. The biosimilar can then be licensed for all already approved indications.2 The biosimilars of infliximab and etanercept have been approved and used for psoriasis since 2013 and 2016, respectively, and drug survival of these biosimilars has been found in register-based studies to be similar to the originator for psoriasis3 and for rheumatoid arthritis.4,5 Since the expiration of the patent for the adalimumab originator (Humira), multiple adalimumab biosimilars have been approved for psoriasis (Amjevita, Amgevita, and Solymbic [ABP 501]; Cyltezo [BI 695501]; Imraldi and Hadlima [SB5]; and Hyrimoz, Hefiya, and Halimatoz [GP2017]).1 The biosimilars ABP 501 and GP2017 were assessed in clinical trials in patients with psoriasis,6,7 and BI 695501 and SB5 were assessed in clinical trials in patients with rheumatoid arthritis8,9 and later approved for psoriasis. All adalimumab biosimilars had similar efficacy and safety data compared with adalimumab originator.1 However, limited knowledge about real-world data exists for switching to adalimumab biosimilars.
In Denmark, a national guideline dictated a nonmedical mandatory switch of all adults with psoriasis treated with adalimumab originator to GP2017 in the Eastern part of Denmark and SB5 in the Western part of Denmark by November 2018 and a switch from adalimumab originator to ABP 501 for children by November 2018. This guideline provided a unique opportunity to assess real-world data on a mandatory switch of adalimumab originator to adalimumab biosimilars. In this independent study, we assessed the outcomes following a nonmedical switch from adalimumab originator to adalimumab biosimilars on 1-year drug retention, disease severity, and adverse events (AEs). In addition, we assessed the 1-year drug retention of adalimumab biosimilars compared with adalimumab originator in biologic-naive patients. The objectives of the current study were to assess the outcomes following a nonmedical mandatory switch from adalimumab originator to an adalimumab biosimilar and to assess the real-world effectiveness and safety of adalimumab biosimilars compared with adalimumab originator.
Methods
The study was approved by the Danish Data Protection Agency. In Denmark, approval of an ethics committee and informed consent are not required for register studies. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.10
Patient Selection and Study Design
All patients in the Biological Treatment in Danish Dermatology (DERMBIO) registry3,11,12,13,14,15,16,17,18,19,20 were assessed for eligibility, and to maximize data integrity, we considered only patients treated in hospital clinics.3,18 DERMBIO is a prospective, nationwide clinical registry of all patients treated with biologics and/or novel small-molecule agents. The data structure of DERMBIO is congruent with that of a cohort study and has been described previously in detail.11,21 In the current study, 2 types of cohort designs were used to investigate the objectives: a crossover-cohort design to assess the outcomes of a switch to adalimumab biosimilars and a cohort design with a historical control group to assess the real-world effectiveness of adalimumab biosimilars. Data were analyzed from June 1, 2020, to October 10, 2021.
In the crossover-cohort design, most patients were both exposed and unexposed and serve as their own controls.22 This approach limits the confounding of patient characteristics that do not change during the follow-up.22 The setup is original in dermatology, but a similar study design was followed in rheumatology to assess the outcomes of a switch from etanercept originator to biosimilar.5 In the current study, all patients with a registered visit who switched from adalimumab originator to adalimumab biosimilars between November 1, 2018, and May 1, 2019, were included (henceforth the adalimumab biosimilar cohort) (Figure 1A). A time window for inclusion of 6 months after introduction of an adalimumab biosimilar and switch was permitted to comply with differences in registration practice and to allow patients with adalimumab originator to use all their medication. Data were censored in May 2020. A comparator cohort of patients treated with adalimumab originator was established. As a simulation of the setup of the adalimumab biosimilar cohort, all patients with a visit between May 1, 2017, and November 1, 2018, treated with adalimumab originator were included (henceforth adalimumab originator cohort) (Figure 1A). Data were censored in November 2018. Identical inclusion criteria applied for both cohorts; only patients with a visit in the inclusion period were included, and patients had 2 or more years of exposure to adalimumab before the index date because the highest discontinuation rate occurs in the first 24 months, whereafter the yearly drug discontinuation is constant.3 Patients followed up for more than 1 year were censored thereafter. In a post hoc analysis, drug retention in patients with less than 2 years of adalimumab exposure before the index date was assessed. In a sensitivity analysis, the inclusion period for the adalimumab originator cohort was set between November 1, 2016, and May 1, 2017, and data were censored in May 2018 (henceforth the adalimumab originator sensitivity cohort) (Figure 1A).
Figure 1. Study Design.
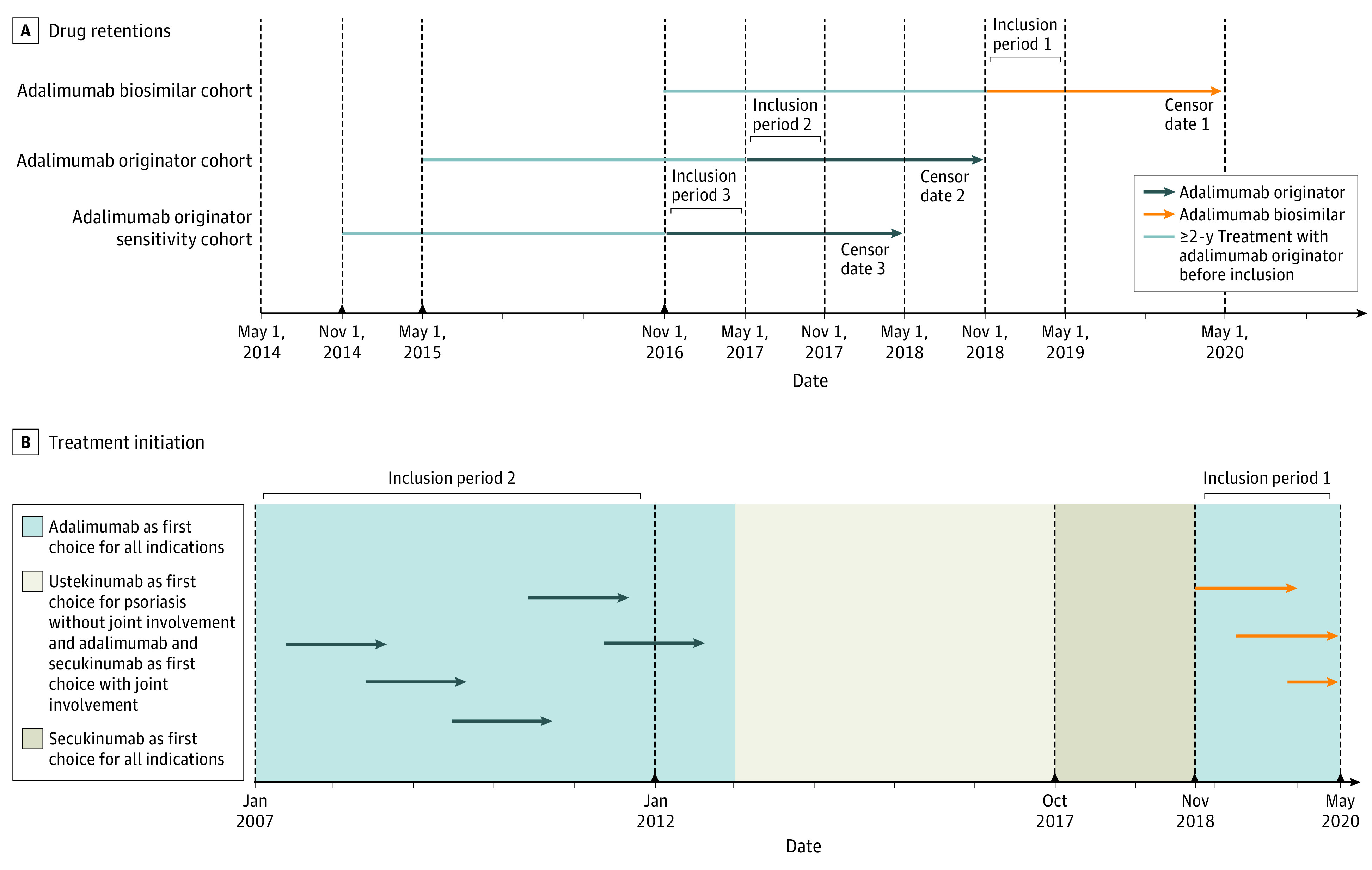
A, One-year drug retentions in patients with 2-year or longer treatment with adalimumab. Inclusion period 1 indicates switching to an adalimumab biosimilar from adalimumab originator between November 1, 2018, and May 1, 2019. Inclusion period 2 indicates a visit between May 1, 2017, and November 1, 2017. Inclusion period 3 indicates a visit between November 1, 2016, and May 1, 2017. B, Biologic-naive patients initiating use of an adalimumab biosimilar between November 1, 2018, and May 1, 2020, and adalimumab originator between January 1, 2007, and January 1, 2012.
The real-world effectiveness of adalimumab biosimilars was investigated by assessing the 1-year drug retention in biologic-naive patients initiating adalimumab biosimilar use from November 1, 2018, onward (biologic-naive biosimilar cohort). The historical comparison cohort comprised patients initiating use of adalimumab originator from January 1, 2007, to December 31, 2012 (biologic-naive originator cohort) (Figure 1B). Patients followed up for more than 1 year were censored thereafter. In Denmark, health care services and biologics are financed through the tax system, and the patients have no out-of-pocket expenditures for treatment with biologics. To ensure equal access to biologics and that use of these products is evidence based, the Danish Medicines Council issues national clinical treatment recommendations. These recommendations are the basis for collection of tenders from the Danish regions’ pharmaceutical organization Amgros. On the basis of tenders and recommendations, a formal treatment guideline is issued that states the order of use of biologics. Adherence to these guidelines is mandatory on a national level and is monitored by Amgros.14 These guidelines dictated adalimumab originator to be first choice in 2007 to 2013 and adalimumab biosimilar from November 2018 onward; thus, this cohort setup resembles that of a cluster randomization study (Figure 1B).
Outcomes
The outcomes following a nonmedical mandatory switch were examined by assessing the 1-year drug retention and risk of treatment stop from all causes, AEs, and insufficient effect in the adalimumab biosimilar cohort after switch and compared with the adalimumab originator cohort before switch. Insufficient effect covered lack and loss of effectiveness, and no distinction between the terms was made. Changes in the Psoriasis Area Severity Index, Dermatology Life Quality Index, drug dosing, and AEs were assessed in both cohorts for patients with 1 or more subsequent visits after the index visit. The real-world effectiveness of adalimumab biosimilars was examined by assessing the 1-year drug retention in the biologic-naive biosimilar cohort and compared with the biologic-naive originator cohort. Drug retention is a commonly used proxy measure for assessing real-world effectiveness,3,23,24 and in the current study, we assessed 1-year retention in patients initiating adalimumab treatment based on guidelines that stated that effectiveness should be evaluated after 3 and 6 months and then once every 6 to 12 months and treatment stopped if no response occurred.25
Statistical Analysis
For continuous data, means (SDs) and medians (interquartile ranges) are reported, and for categorical outcomes, numbers (percentages) are presented. For normally distributed data, an unpaired 2-tailed t test was used to assess differences between groups, and for nonparametric data, the Mann-Whitney test was used. For categorical outcomes, χ2 or Fisher tests were used to assess differences between groups.
Treatment retention was assessed with Kaplan-Meier estimates and the log-rank test. Cox proportional hazards regression was used to compare drug retention between the cohorts. The switch cohort comprised patients who were exposed and unexposed, only exposed, and only unexposed. To take the repeated participants into account, a robust variance was used in the Cox proportional hazards regression, which handles both full and half pairs.26 Hazard ratios (HRs) are presented as crude, partly adjusted, and fully adjusted. The partly adjusted model included adjustment for age and sex, and the fully adjusted model included additional adjustments for time taking adalimumab before the index date, biologic exposure, concomitant methotrexate use, psoriatic arthritis, and body weight. Missing data in the adjusting variables were imputed with a Markov chain Monte-Carlo–based multiple imputation approach with 100 imputations.27 Missing data were considered missing completely at random, and maximal missingness was set to 30%. Of the adjusting variables, only body weight had missing values, with 7% missing data. A 2-sided P < .05 was considered statistically significant.
All data management and statistical analyses were performed using SAS software, version 9.4 (SAS Institute Inc) and Stata software, version 15.0 (StataCorp LLC).
Results
Since November 2018, a total of 453 patients with at least 2-year exposure to adalimumab switched from originator to adalimumab biosimilars. Of these, 89 switched without a registered visit in DERMBIO in the inclusion period, and 16 switched after the inclusion period (Figure 2). In total, 348 (mean [SD] age, 52.2 [13.6] years; 251 [72.1%] male) were included in the adalimumab biosimilar cohort, of whom 186 switched to GP2017 and 162 to SB5. The adalimumab originator cohort comprised 378 patients (mean [SD] age, 51.1 [14.1] years; 272 [72.0%] male). Of the included patients, 256 patients were included in both the adalimumab originator and adalimumab biosimilar cohort. In 290 patients (61.7%), adalimumab was the first biologic with no difference across groups (Table 1).
Figure 2. Flowchart of the Participant Selection Process.

Table 1. Baseline Characteristics and Disease Severity After Change in Treatment.
| Variable | Adalimumab biosimilar cohort (n = 348) | Adalimumab originator cohort (n = 378) | P value |
|---|---|---|---|
| Characteristics | |||
| Male | 251 (72.1) | 272 (72.0) | .96 |
| Methotrexate use, No. (%) | 28 (8.1) | 38 (10.1) | .35 |
| PsA, No. (%) | 133 (38.2) | 159 (42.1) | .29 |
| Age, mean (SD), y | 52.2 (13.6) | 51.1 (14.1) | .22 |
| Weight, mean (SD), kg | 89.9 (21.3) | 91.0 (22.1) | .51 |
| Missing, No. | 32 | 16 | NA |
| BMI, mean (SD) | 28.9 (6.1) | 29.3 (6.4) | .37 |
| Missing, No. | 59 | 39 | NA |
| Disease duration, mean (SD), y | 30.6 (12.6) | 28.5 (12.6) | .03 |
| Missing, No. | 104 | 103 | NA |
| Time receiving adalimumab before inclusion/index date, median (IQR), mo | 70 (57 to 98) | 60 (45 to 85) | <.001 |
| Naive to biologics | 221 (63.5) | 228 (60.3) | .38 |
| Disease severity before and after switch, median (IQR) | |||
| PASI | |||
| PASI at index visit | 0.2 (0.0 to 1.2) | 0.2 (0.0 to 1.2) | .77 |
| Missing, No. | 30 | 35 | NA |
| PASI at subsequent visit | 0.0 (0.0 to 1.2) | 0.2 (0.0 to 1.2) | .79 |
| Missing, No. | 68 | 69 | NA |
| ΔPASI | 0.0 (−0.3 to 0.2) | 0.0 (−0.3 to 0.2) | .63 |
| Missing, No. | 84 | 101 | NA |
| DLQI | |||
| DLQI at index visit | 0.5 (0.0 to 1.2) | 1.0 (0.0 to 2.0) | .01 |
| Missing, No. | 52 | 22 | NA |
| DLQI at subsequent visit | 0.0 (0.0 to 1.0) | 0.0 (0.0 to 2.0) | .03 |
| Missing, No. | 92 | 57 | NA |
| ΔDLQI | 0.0 (−1.0 to 0.0) | 0.0 (0.0 to 0.0) | .75 |
| Missing, No. | 108 | 81 | NA |
Abbreviations: BMI, body mass index (calculated as weight in kilograms divided by height in meters squared); DLQI, Dermatology Life Quality Index; IQR, interquartile range; NA, not applicable; PsA, psoriatic arthritis; PASI, Psoriasis Area Severity Index.
For the adalimumab biosimilar cohort, 28 patients (8.0%) stopped treatment after 12 months, of whom 12 (42.3%) stopped because of insufficient effect, 9 (32.1%) because of AEs, and 7 (25.0%) because of other reasons (Table 2). Of the patients stopping treatment, 9 switched back to adalimumab originator, of whom 4 (44.4%) stopped adalimumab biosimilar treatment because of insufficient effect and 5 (55.6%) because of AEs or other reasons. After switching back to adalimumab originator, more than 7 patients continued treatment at the censor date.
Table 2. Total Participants and Survival Functions.
| Time | Adalimumab biosimilar cohort (n = 348) | Adalimumab originator cohort (n = 378)a | Adalimumab originator sensitivity cohort (n = 403)b | |||
|---|---|---|---|---|---|---|
| Total participants/discontinuation | Survival function (SE) | Total participants/discontinuation | Survival function (SE) | Total participants/discontinuation | Survival function (SE) | |
| All causes | ||||||
| 6 mo | 348/15 | 0.957 (0.011) | 378/16 | 0.958 (0.010) | 402/21 | 0.945 (0.011) |
| 12 mo | 348/28 | 0.920 (0.015) | 376/30 | 0.921 (0.014) | 402/44 | 0.891 (0.016) |
| Insufficient effect | ||||||
| 6 mo | 339/6 | 0.983 (0.007) | 370/8 | 0.979 (0.008) | 389/8 | 0.980 (0.007) |
| 12 mo | 332/12 | 0.965 (0.010) | 362/16 | 0.957 (0.011) | 376/18 | 0.953 (0.011) |
| Adverse events | ||||||
| 6 mo | 338/5 | 0.985 (0.006) | 366/4 | 0.993 (0.005) | 389/7 | 0.982 (0.006) |
| 12 mo | 329/9 | 0.973 (0.009) | 353/7 | 0.981 (0.007) | 358/11 | 0.972 (0.008) |
Included patients with a visit between May 1, 2017, and November 1, 2017, with data censored November 1, 2018.
Included patients with a visit between November 1, 2016, and May 1, 2017 (sensitivity period), with data censored May 1, 2018.
For the adalimumab originator cohort, 30 patients (7.9%) stopped treatment after 12 months, of whom 16 (53.3%) stopped because of insufficient effect, 7 (23.3%) because of AEs, and 7 (23.3%) because of other reasons (Table 2).
No differences in time receiving treatment were observed for the adalimumab biosimilar cohort compared with the adalimumab originator cohort (Figure 3; eFigure in the Supplement). Limiting the population to only include biologic-naive patients did not alter the results. Similar results were seen for the 2 different adalimumab biosimilars (GP2017 and SB5).
Figure 3. Survival Curves for Patients Stopping Treatment With Adalimumab Originator or Adalimumab Biosimilar for All Causes of Treatment Discontinuation.

The crude HRs for drug discontinuation for the adalimumab biosimilar cohort compared with the adalimumab originator cohort were 1.02 (95% CI, 0.61-1.70; P = .94) for all causes of drug discontinuation, 0.82 (95% CI, 0.39-1.73; P = .60) for insufficient effect, and 1.41 (95% CI, 0.52-3.77; P = .50) for AEs. Adjusting for age and sex or additionally adjusting for time in adalimumab treatment, biologic exposure, concomitant methotrexate, psoriatic arthritis, and body weight did not significantly alter the results (eTable 1 in the Supplement). Overall, no changes in disease activity or Dermatology Life Quality Index were observed after index date in the adalimumab biosimilar cohort and adalimumab originator cohort.
The proportion of patients experiencing AEs was assessed in the 12-month treatment period for the adalimumab originator and adalimumab biosimilar cohorts. In total, 359 patients had available data on AEs in the adalimumab originator cohort and 320 in the adalimumab biosimilar cohort. In DERMBIO, AEs are registered in predefined categories: keratinocyte cancers, cancers other than keratinocyte cancer, cardiac, pulmonary, neurological, dermatological, infection, anaphylaxis, and other. More patients who switched to adalimumab biosimilars experienced any AEs vs patients treated with adalimumab originator (29 [9.1%] vs 18 [5.0%], P = .04) (eTable 2 in the Supplement). More patients treated with adalimumab biosimilars experienced AEs registered as other vs patients treated with adalimumab originator (21 [6.6%] vs 3 [0.8%], P < .001).
No difference was observed for patients having an increase in dose in the 2 cohorts. Of 357 patients treated with adalimumab originator, 4 (1.1%) had an increase in dose, and 5 (1.6%) of 319 treated with adalimumab biosimilar had an increase in dose (P = .74). A similar proportion of patients had a decrease in dose (11 [3.4%] in the adalimumab biosimilar cohort and 10 [2.8%] in the adalimumab originator cohort; P = .63).
Biologic-Naive Patients Initiating Adalimumab Biosimilar and Adalimumab Originator Treatment
The biologic-naive biosimilar cohort comprised 321 biologic-naive patients initiating use of adalimumab biosimilars, and the biologic-naive originator cohort comprised 389 biologic-naive patients initiating use of adalimumab originator (eTable 3 in the Supplement). Similar 1-year retentions were seen for all outcomes (eTable 4 in the Supplement). Of the patients, 189 had available data on AEs in the biologic-naive biosimilar cohort and 333 in the biologic-naive originator cohort. More patients treated with adalimumab biosimilars experienced dermatologic AEs vs patients treated with adalimumab originator (7 [3.6%] vs 0, P < .001), but no differences were observed in patients experiencing any AEs (eTable 5 in the Supplement).
Sensitivity Analyses
Moving the inclusion period and censor period for the adalimumab originator by half a year (adalimumab originator sensitivity cohort) was not associated with statistically significant differences in 1-year drug retentions compared with the adalimumab biosimilar cohort (eTables 3 to 6 in the Supplement). A higher proportion of patients experiencing any AE in the adalimumab biosimilar cohort was not observed when compared with the sensitivity cohort (eTable 2 in the Supplement). More patients experienced infections and neurologic AEs in the adalimumab originator sensitivity cohort (eTable 2 in the Supplement). In patients with less than 2 years of adalimumab exposure before the index date, 47 could be included in the adalimumab biosimilar cohort, of whom 10 stopped treatment after 1 year, and 75 in the adalimumab originator cohort, of whom 17 stopped. No differences were observed in HRs for drug treatment discontinuation (eTable 7 in the Supplement).
Discussion
This nationwide cohort study of patients with moderate to severe psoriasis undergoing a mandatory switch from adalimumab originator to adalimumab biosimilars (GP2017 or SB5) found similar 1-year retentions for adalimumab biosimilars after switching as for adalimumab originator before switching. No differences in change of disease severity were seen. However, more patients treated with adalimumab biosimilars experienced dermatologic AEs.
The phase 3 clinical trial of GP2017 assessed the equivalence of GP2017 compared with adalimumab originator and the influence of multiple switches on the efficacy.7 In that study, equivalent efficacy between GP2017 and the adalimumab originator was observed up to week 17.7 After week 17, patients were rerandomized to continue treatment or have 3 switches between drugs until week 35; thereafter, patients returned to using the original drug.7 No differences in efficacy, insufficient effect, and development of antidrug antibodies were observed.7 SB5 was assessed in patients with rheumatoid arthritis, with the phase 3 trial finding no differences in efficacy and in development of antidrug antibodies.8
In line with the phase 3 clinical trials of adalimumab biosimilars, no differences were found for the 1-year drug retention for the adalimumab biosimilars (GP2017 and SB5) compared with adalimumab originator after a mandatory switch. Overall, results for any AEs were contradicting, but certain AEs were more prevalent in the adalimumab biosimilar cohort. Both dermatologic and the AE category other were more prevalent, which could be attributable to more patients experiencing injection site reactions as a result of larger volumes and differences in excipients and syringes in the adalimumab biosimilars and the adalimumab originator.28,29,30 Other potential explanations are the nocebo effect and more awareness of AEs by practitioners and patients.31
Although biosimilars as new prescriptions might, in many cases and countries, not be of concern to the prescribing practitioner,32 switching patients between originator and biosimilars may be of concern for practitioners because of the lack of clinical data and recommendations.32,33,34 Concerns surrounding switching to biosimilars include the possibility of increased immunogenicity, safety issues, and loss of effictiveness.35 Regarding 1-year drug retentions in patients treated for 2 years or more with adalimumab before the switch, this study provides evidence that in the real world a switch to an adalimumab biosimilar is not inferior compared with continuing treatment with the adalimumab originator. Likewise, a post hoc analysis found no difference in patients treated with adalimumab for less than 2 years before the switch. Nevertheless, a small proportion of patients were switched back to adalimumab originator, mostly because of insufficient effect or AEs. The introduction of a biosimilar and consequently a switch might influence the practitioners’ and the patients’ thoughts, the response to drug, or drug retention. National differences in the use and perception of biosimilars32 might lead to different influences of a nonmedical switch with a potential nocebo effect to follow. In Denmark, all patients treated with infliximab or etanercept originator underwent a mandatory nonmedical switch to infliximab biosimilar in 2015 and etanercept biosimilar in 2016.3 In the study, noninferiority regarding effectiveness and safety was observed,3 probably leading to more open-minded and less guarded practitioners in switching patients from adalimumab originator to adalimumab biosimilars. No differences in drug retention for the adalimumab originator when changing the inclusion period were observed.
This study found that 1-year drug retention for biologic-naive patients initiating treatment with adalimumab biosimilars was similar to that for biologic-naive patients initiating treatment with adalimumab originator in a historical cohort. Taken together with the switch data, the results of this study support the interchangeability of adalimumab originator with adalimumab biosimilars. This finding is important because the lower price of biosimilars, although with national differences, can make the drug more accessible. The cost saving of adalimumab biosimilars in Denmark is evident: the quarterly expenditure on adalimumab across all indications decreased from DKK 28.8 million (€3.9 million, US $4.7 million) in the first quarter of 2018 to DKK 6.5 million (€0.9 million, US $1.1 million) in the first quarter of 2019, corresponding to an 80% reduction in the Central Region Jutland, which houses 1.3 million people.36
Strengths and Limitations
This study has strengths and limitations. Strengths include the prospective data collection and the nationwide coverage. Moreover, the mandatory nationwide switch eliminates the risk of potential confounding by indication (ie, some patients or practitioners might be more prone to switch to biosimilars if given the choice, which could overestimate or underestimate the outcomes following a switch from originator to biosimilar).
Some limitations should be considered when interpreting the results of this study. First, the study comprised only Danish patients, and because the outcome of biosimilar switch might depend on familiarity with and attitude toward biosimilars, the result might not be generalizable to countries where biosimilars are not part of the daily routine. Providing information on biosimilars to patients and practitioners might be a way to overcome this potential issue. Another limitation is that the individual AEs could not be examined. Moreover, the surveillance of AEs is not as vigilant as in clinical trials, and AEs are most likely underreported. Although no major differences were found when switching from adalimumab originator to adalimumab biosimilar versions, it was not possible to assess the performance of individual adalimumab biosimilar versions in this study. Last, some data were missing but are believed to be missing completely at random because no association was found between missingness of the data (eg, body weight) and any other parameter.
Conclusions
These results suggest that the effectiveness of adalimumab biosimilar is similar to that of adalimumab originator. A nonmedical switch from adalimumab originator to an adalimumab biosimilar does not appear to affect drug retention. However, switching to an adalimumab biosimilar might lead to more dermatologic AEs, although whether this is attributable to increased medical scrutiny remains unclear and warrants further study.
eFigure. Survival Curves for Patients Stopping Treatment Due to A) Insufficient Effect and B) Adverse Events
eTable 1. Hazard Ratios for OneYear Drug Retention Comparing ADA-Biosimilar With ADA-Originator in Patients With ≥2 Years Adalimumab Exposure Prior to Index Date
eTable 2. Adverse Events Among Patients Treated With Either ADA-Originator or ADA-Biosimilar
eTable 3. Baseline Characteristics for the Bio-Naïve Biosimilar-Cohort and the Bio-Naïve Originator-Cohort
eTable 4. Total Participants and Survival Functions for Biological-Naïve Patients Starting on Adalimumab 2007-2012 and Patients Starting on Adalimumab From 2018
eTable 5. Adverse Events Among Biological-Naïve Patients Treated With Either Adalimumab Originator (From 2007-2012) or Adalimumab Biosimilar (From 2018 and Onwards)
eTable 6. Hazard Ratios for One-Year Drug Retention Comparing Biological-Naïve Patients Treated With Adalimumab Biosimilar (From 2018 and Onwards) With Adalimumab Originator (From 2007-2012)
eTable 7. Post Hoc Analysis of Hazard Ratios for One-Year Drug Retention Comparing ADA-Biosimilar With ADA-Originator in Patients With <2 Years Adalimumab Exposure Prior to Index Date
References
- 1.Reynolds KA, Pithadia DJ, Lee EB, Han G, Wu JJ. Are biosimilars approved for use in psoriasis safe enough to replace leading biologic therapies? a review. Expert Opin Drug Saf. 2020;19(4):459-466. doi: 10.1080/14740338.2020.1737674 [DOI] [PubMed] [Google Scholar]
- 2.Constantin MM, Cristea CM, Taranu T, et al. Biosimilars in dermatology: the wind of change. Exp Ther Med. 2019;18(2):911-915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Egeberg A, Ottosen MB, Gniadecki R, et al. Safety, efficacy and drug survival of biologics and biosimilars for moderate-to-severe plaque psoriasis. Br J Dermatol. 2018;178(2):509-519. doi: 10.1111/bjd.16102 [DOI] [PubMed] [Google Scholar]
- 4.Glintborg B, Sørensen IJ, Loft AG, et al. ; all departments of rheumatology in Denmark . A nationwide non-medical switch from originator infliximab to biosimilar CT-P13 in 802 patients with inflammatory arthritis: 1-year clinical outcomes from the DANBIO registry. Ann Rheum Dis. 2017;76(8):1426-1431. doi: 10.1136/annrheumdis-2016-210742 [DOI] [PubMed] [Google Scholar]
- 5.Glintborg B, Loft AG, Omerovic E, et al. To switch or not to switch: results of a nationwide guideline of mandatory switching from originator to biosimilar etanercept. One-year treatment outcomes in 2061 patients with inflammatory arthritis from the DANBIO registry. Ann Rheum Dis. 2019;78(2):192-200. doi: 10.1136/annrheumdis-2018-213474 [DOI] [PubMed] [Google Scholar]
- 6.Papp K, Bachelez H, Costanzo A, et al. Clinical similarity of biosimilar ABP 501 to adalimumab in the treatment of patients with moderate to severe plaque psoriasis: a randomized, double-blind, multicenter, phase III study. J Am Acad Dermatol. 2017;76(6):1093-1102. doi: 10.1016/j.jaad.2016.12.014 [DOI] [PubMed] [Google Scholar]
- 7.Blauvelt A, Lacour JP, Fowler JF Jr, et al. Phase III randomized study of the proposed adalimumab biosimilar GP2017 in psoriasis: impact of multiple switches. Br J Dermatol. 2018;179(3):623-631. doi: 10.1111/bjd.16890 [DOI] [PubMed] [Google Scholar]
- 8.Weinblatt ME, Baranauskaite A, Niebrzydowski J, et al. Phase III Randomized Study of SB5, an adalimumab biosimilar, versus reference adalimumab in patients with moderate-to-severe rheumatoid arthritis. Arthritis Rheumatol. 2018;70(1):40-48. doi: 10.1002/art.40336 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Cohen SB, Alonso-Ruiz A, Klimiuk PA, et al. Similar efficacy, safety and immunogenicity of adalimumab biosimilar BI 695501 and Humira reference product in patients with moderately to severely active rheumatoid arthritis: results from the phase III randomised VOLTAIRE-RA equivalence study. Ann Rheum Dis. 2018;77(6):914-921. doi: 10.1136/annrheumdis-2017-212245 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP; STROBE Initiative . The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 2007;4(10):e296. doi: 10.1371/journal.pmed.0040296 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Gniadecki R, Kragballe K, Dam TN, Skov L. Comparison of drug survival rates for adalimumab, etanercept and infliximab in patients with psoriasis vulgaris. Br J Dermatol. 2011;164(5):1091-1096. doi: 10.1111/j.1365-2133.2011.10213.x [DOI] [PubMed] [Google Scholar]
- 12.Ahlehoff O, Skov L, Gislason G, et al. Cardiovascular outcomes and systemic anti-inflammatory drugs in patients with severe psoriasis: 5-year follow-up of a Danish nationwide cohort. J Eur Acad Dermatol Venereol. 2015;29(6):1128-1134. doi: 10.1111/jdv.12768 [DOI] [PubMed] [Google Scholar]
- 13.Ahlehoff O, Skov L, Gislason G, et al. Pharmacological undertreatment of coronary risk factors in patients with psoriasis: observational study of the Danish nationwide registries. PLoS One. 2012;7(4):e36342. doi: 10.1371/journal.pone.0036342 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Egeberg A, Iversen L, Gniadecki R, et al. Characteristics of patients receiving ustekinumab compared with secukinumab for treatment of moderate-to-severe plaque psoriasis—nationwide results from the DERMBIO registry. J Eur Acad Dermatol Venereol. 2017;31(7):1183-1187. doi: 10.1111/jdv.14200 [DOI] [PubMed] [Google Scholar]
- 15.Loft N, Skov L, Bryld LE, Gislason G, Egeberg A. Treatment history of patients receiving biologic therapy for psoriasis—a Danish nationwide study. J Eur Acad Dermatol Venereol. 2017;31(8):e362-e363. doi: 10.1111/jdv.14156 [DOI] [PubMed] [Google Scholar]
- 16.Loft ND, Skov L, Rasmussen MK, et al. Genetic polymorphisms associated with psoriasis and development of psoriatic arthritis in patients with psoriasis. PLoS One. 2018;13(2):e0192010. doi: 10.1371/journal.pone.0192010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Loft ND, Skov L, Iversen L, et al. Associations between functional polymorphisms and response to biological treatment in Danish patients with psoriasis. Pharmacogenomics J. 2018;18(3):494-500. doi: 10.1038/tpj.2017.31 [DOI] [PubMed] [Google Scholar]
- 18.Gniadecki R, Bang B, Bryld LE, Iversen L, Lasthein S, Skov L. Comparison of long-term drug survival and safety of biologic agents in patients with psoriasis vulgaris. Br J Dermatol. 2015;172(1):244-252. doi: 10.1111/bjd.13343 [DOI] [PubMed] [Google Scholar]
- 19.Hesselvig JH, Egeberg A, Loft ND, Zachariae C, Kofoed K, Skov L. Correlation between dermatology life quality index and psoriasis area and severity index in patients with psoriasis treated with ustekinumab. Acta Derm Venereol. 2018;98(3):335-339. doi: 10.2340/00015555-2833 [DOI] [PubMed] [Google Scholar]
- 20.Loft ND, Egeberg A, Rasmussen MK, et al. Patient-reported outcomes during treatment in patients with moderate-to-severe psoriasis: a Danish nationwide study. Acta Derm Venereol. 2019;99(13):1224-1230. doi: 10.2340/00015555-3331 [DOI] [PubMed] [Google Scholar]
- 21.Loft N, Egeberg A, Rasmussen MK, et al. Response to biologics during the first 6 months of therapy in biologic naïve patients with psoriasis predicts risk of disease flares: a Danish nationwide study. Acta Derm Venereol. 2021;101(1):adv00357. doi: 10.2340/00015555-3722 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Maclure M, Mittleman MA. Should we use a case-crossover design? Annu Rev Public Health. 2000;21(1):193-221. doi: 10.1146/annurev.publhealth.21.1.193 [DOI] [PubMed] [Google Scholar]
- 23.van den Reek JMPA, Kievit W, Gniadecki R, et al. Drug survival studies in dermatology: principles, purposes, and pitfalls. J Invest Dermatol. 2015;135(7):1-5. doi: 10.1038/jid.2015.171 [DOI] [PubMed] [Google Scholar]
- 24.Warren RB, Smith CH, Yiu ZZN, et al. Differential drug survival of biologic therapies for the treatment of psoriasis: a prospective observational cohort study from the British Association of Dermatologists Biologic Interventions Register (BADBIR). J Invest Dermatol. 2015;135(11):2632-2640. doi: 10.1038/jid.2015.208 [DOI] [PubMed] [Google Scholar]
- 25.Dansk Dermatologisk Selskab . Retningslinjer for behandling af psoriasis med 2. generations immunomodulatorisk behandling. 2019. Accessed January 28, 2021. https://dds.nu/wp-content/uploads/2019/12/Guideline-DDS-2.-generations-immunomodulatorisk-behandling-final-oktober-2019.pdf
- 26.Lin DY, Wei L-J. The robust inference for the Cox proportional hazards model. J Am Stat Assoc. 1989;84(408):1074-1078. doi: 10.1080/01621459.1989.10478874 [DOI] [Google Scholar]
- 27.Schafer JL. Analysis of Incomplete Multivariate Data. CRC Press; 1997. doi: 10.1201/9781439821862 [DOI] [Google Scholar]
- 28.Humira: Summary of product characteristics. Accessed September 10, 2020. https://www.ema.europa.eu/en/documents/product-information/humira-epar-product-information_en.pdf
- 29.Hyrimoz: Summary of product characteristics. Accessed September 10, 2020. https://www.ema.europa.eu/en/documents/product-information/hyrimoz-epar-product-information_en.pdf
- 30.Imraldi: Summary of product characteristics. Accessed September 10, 2020. https://www.ema.europa.eu/en/documents/product-information/imraldi-epar-product-information_en.pdf
- 31.Kristensen LE, Alten R, Puig L, et al. Non-pharmacological effects in switching medication: the nocebo effect in switching from originator to biosimilar agent. BioDrugs. 2018;32(5):397-404. doi: 10.1007/s40259-018-0306-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Cohen AD, Torres T, Boehncke W-H, et al. Biosimilars for psoriasis—experience from Europe. Curr Dermatol Rep. 2019;8(1):26-34. doi: 10.1007/s13671-019-0249-x [DOI] [Google Scholar]
- 33.Inotai A, Prins CPJ, Csanádi M, Vitezic D, Codreanu C, Kaló Z. Is there a reason for concern or is it just hype? a systematic literature review of the clinical consequences of switching from originator biologics to biosimilars. Expert Opin Biol Ther. 2017;17(8):915-926. doi: 10.1080/14712598.2017.1341486 [DOI] [PubMed] [Google Scholar]
- 34.Moots R, Azevedo V, Coindreau JL, et al. Switching between reference biologics and biosimilars for the treatment of rheumatology, gastroenterology, and dermatology inflammatory conditions: considerations for the clinician. Curr Rheumatol Rep. 2017;19(6):37. doi: 10.1007/s11926-017-0658-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Cohen HP, Blauvelt A, Rifkin RM, Danese S, Gokhale SB, Woollett G. Switching reference medicines to biosimilars: a systematic literature review of clinical outcomes. Drugs. 2018;78(4):463-478. doi: 10.1007/s40265-018-0881-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Midtjylland Region. Lægemiddelmonitorering i Region Midtjylland 2019. 2019. Accessed January 28, 2021. https://www.rm.dk/api/NewESDHBlock/DownloadFile?agendaPath=%5C%5CRMAPPS0221.onerm.dk%5CCMS01-EXT%5CESDH%20Data%5CRM_Internet%5CDagsordener%5CHospitalsudvalget%202019%5C09-09-2019%5CAaben_dagsorden&appendixId=247011
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eFigure. Survival Curves for Patients Stopping Treatment Due to A) Insufficient Effect and B) Adverse Events
eTable 1. Hazard Ratios for OneYear Drug Retention Comparing ADA-Biosimilar With ADA-Originator in Patients With ≥2 Years Adalimumab Exposure Prior to Index Date
eTable 2. Adverse Events Among Patients Treated With Either ADA-Originator or ADA-Biosimilar
eTable 3. Baseline Characteristics for the Bio-Naïve Biosimilar-Cohort and the Bio-Naïve Originator-Cohort
eTable 4. Total Participants and Survival Functions for Biological-Naïve Patients Starting on Adalimumab 2007-2012 and Patients Starting on Adalimumab From 2018
eTable 5. Adverse Events Among Biological-Naïve Patients Treated With Either Adalimumab Originator (From 2007-2012) or Adalimumab Biosimilar (From 2018 and Onwards)
eTable 6. Hazard Ratios for One-Year Drug Retention Comparing Biological-Naïve Patients Treated With Adalimumab Biosimilar (From 2018 and Onwards) With Adalimumab Originator (From 2007-2012)
eTable 7. Post Hoc Analysis of Hazard Ratios for One-Year Drug Retention Comparing ADA-Biosimilar With ADA-Originator in Patients With <2 Years Adalimumab Exposure Prior to Index Date