

Abstract
Objectives
To investigate the skeletal and dentoalveolar effects of Invisalign's G5 protocol with virtual bite ramps in the treatment of adults with skeletal deep bites.
Materials and Methods
This retrospective study was conducted on consecutively treated adults presenting with skeletal deep bites as defined by the Overbite Depth Indicator (ODI). Subjects were divided into 2 groups: Invisalign group (n = 24) treated with the Invisalign G5 protocol and a full fixed appliance (FFA) group (n = 24) treated with edgewise FFAs and matched to the Invisalign group by ODI, sex, type of malocclusion, and non-extraction treatment. Pretreatment (T1) and post–comprehensive treatment (T2) lateral cephalograms were obtained and analyzed.
Results
Both the Invisalign and FFA groups showed significant changes from T1 to T2 in ODI and other skeletal and dentoalveolar measurements. The mean change in ODI was −1.5° (P < .001) for the Invisalign group and −2.0° (P < .001) for the FFA group. The mean decrease in overbite was 1.3 mm (P < .001) and 2.0 mm (P < .001) for the Invisalign and FFA groups, respectively. The mean increase in mandibular plane angle (Sn-GoGn) was 0.65° (P = .003) for the Invisalign group and 1.15° (P < .001) for the FFA group. When the groups were compared with each other, both ODI (P = .03) and overbite (P = .003) were significantly different in addition to other measurements.
Conclusions
Although FFA treatment had more apparent skeletal changes for deep bite adult patients when compared with Invisalign, both systems were effective in opening deep bites at dentoalveolar and skeletal levels.
Keywords: Clear aligners, Adult, Fixed appliances, Deep bite
INTRODUCTION
Deep bite malocclusions are a relatively common component found in malocclusions of adolescents and adults, with overbites of greater than or equal to 5 mm occurring in 15% to 20% of the US population. Depending on whether the etiology is skeletal or dental, techniques that involve maxillary and mandibular incisor intrusion, proclination, posterior extrusion, and increasing lower anterior facial height through surgical means have been proven effective in correcting deep bite malocclusions.1,2
Clear aligners have increased in popularity because of their esthetic advantages and comfort compared with conventional fixed appliances.3 Few studies reported success in correcting malocclusions, including anteroposterior discrepancies, Class III malocclusions and, less commonly, severe deep bites.4,5 Treating deep bites with clear aligners has been perceived as difficult due to the patient's natural biting force aiding in posterior intrusion. Perhaps the only benefit initially in using aligners for deep bite treatment was that there was no waiting necessary to level the curve of Spee with mandibular incisor intrusion. This is in contrast to fixed appliances where the clinician typically waits until some of the initial leveling and aligning are corrected before placing reverse-curve arch wires. In addition, bracket interferences can also cause delays in the curve of Spee leveling with fixed appliances.6
In 2014, Align Technology (Santa Clara, CA) introduced Invisalign G5 Innovation for Deep Bite correction. This innovation included control of anterior intrusion via SmartForce pressure areas (to direct intrusion through the long axis of the tooth), optimized deep bite attachments on premolars (to serve as anchorage for incisor intrusion), and precision bite ramps that are up to 3 mm in depth (to allow posterior disocclusion).7 These bite ramps were designed to eliminate transient posterior intrusion and add intrusive forces to mandibular incisors through natural biting forces. By disoccluding the buccal segments, it is easier to successfully achieve posterior tooth extrusion. The bite ramp position is automatically adjusted to maintain anterior contact throughout all stages of treatment.7
Khosravi et al.8 evaluated the management of overbite with Invisalign. In their study, the sample consisted of adults with normal overbite, deep bite, and anterior open bite, all of whom were treated with the Invisalign appliance alone. The deep bite group was categorized on the basis of a dental deep bite only, with the inclusion criteria being an overbite of 4 mm or greater. The treatment mechanics for the deep bite patients primarily consisted of virtual bite ramps, overcorrection of the overbite, leveling of the curve of Spee, and leveling of the curve of Wilson. They found a median of 1.5 mm of bite opening in the deep bite group, with mandibular incisor proclination being the primary bite opening mechanism.8 The study, however, was completed prior to the introduction of G5. Thus, the aim of this study was to investigate the skeletal and dentoalveolar effects of Invisalign's G5 protocol with virtual bite ramps in the treatment of adults with skeletal deep bites.
MATERIALS AND METHODS
This retrospective study analyzed the effectiveness of Invisalign G5 (Align Technology) with virtual bite ramps compared with a matched control group treated with standard edgewise full fixed appliances (FFAs). The samples were collected from the private orthodontic practice of Dr. Willy Dayan in Toronto, Ontario, and the University at Buffalo Department of Orthodontics. Dr. Dayan is an experienced Invisalign provider and has been using Invisalign since its inception in 1998. Institutional review board approval was obtained from the University at Buffalo (STUDY00001130).
Sample Size Estimation
With reference to Baccetti et al.,9 an estimated sample of 24 patients per group would have a 90% power to detect an effect size of 1.15° for the Overbite Depth Indicator (ODI) measurement at an α level of 5%.
Inclusion/Exclusion Criteria
The inclusion criteria were treatment with Invisalign G5 or FFAs between January 1, 2014, and January 1, 2017; complete pretreatment and posttreatment lateral cephalograms; ODI greater than or equal to 80.5 degrees;10 malocclusions of either Class I or Class II divisions 1 and 2; nonextraction treatment; and older than the age of 18 at the start of treatment. Participants were excluded if they presented with the following: dolichocephalic growth pattern; Class III malocclusion; or treatment involving orthognathic surgery, skeletal anchorage, or single arch Invisalign treatment.
Invisalign did not introduce the G5 protocol until 2014; therefore, any patient treated prior to the implementation of G5 was not included. Of 236 patients started after 2014 with Invisalign, 74 were treated with the G5 protocol, and only 24 (women = 15, men = 9) consecutively treated patients met the inclusion criteria and were included. A total of 24 patients (women = 16, men = 8) treated with FFAs and matched to the Invisalign group by ODI, sex, type of malocclusion, and nonextraction treatment were included.
Study Procedures
Pretreatment (T1) and post–comprehensive treatment (T2) lateral cephalograms were obtained, traced, and analyzed by one investigator (D.H.) using Dolphin Imaging Software (version 11.7.5.66; Dolphin Imaging, Chatsworth, CA). The investigator was blinded to type of cephalogram and time point. A total of 9 skeletal, 8 dental, and 3 soft tissue variables were measured. Of the measurements, 10 were linear and 10 were angular.
For the Invisalign group, additional information was collected on the total amount of trays for the maxillary and mandibular arches, the tray number in which the G5 bite ramps were placed and removed, the teeth included in bite ramp extension, and the number and location of attachments as well as potential interproximal reduction plans and maxillary lingual root torque.
Treatment Protocols
A standard treatment protocol was followed for the Invisalign group. It included creating gradual reverse curves of Spee in mandibular arch aligners and precision bite ramps on the maxillary anterior teeth, adding maxillary incisor lingual root torque, and creating hard posterior contacts. Timing and length of use of Class II elastics varied based on malocclusion severity but was initiated on the first tray until Class I molar relationship was achieved.
All patients in the FFA group were treated with 0.018-inch slot brackets (Victory series; 3M, St. Paul, Minn), MBT (McLaughlin/Bennett/Trevisi) prescription with negative 6-degree torque on mandibular incisors. Mechanics involved placing reverse curve of Spee wires in the mandibular arch. The general archwire sequence was 0.016″ Nickel-titanium (NiTi), 16 × 22″ NiTi, 16 × 22″ Stainless steel, and 17 × 25″ Beta-titanium. Class II elastics were used depending on the type of malocclusion. No other appliances were used for Class II correction.
Intraexaminer Reliability
A total of 10 lateral cephalometric measurements were repeated 2 weeks following the initial measurements. The intraclass correlation coefficients for all repeated measurements were calculated.
Statistical Methods
Data were analyzed using SPSS version 23 for Windows (IBM Corporation, Chicago, Ill). Descriptive statistics were conducted to explore the data. Homogeneity of variance was assessed for all variables by Levene's test. For any measurement with unequal variances, a Mann-Whitney U-test was performed to ensure accuracy. To analyze age by gender and treatment group at baseline, a two-way analysis of variance (ANOVA) was used. To describe Angle malocclusion classification within groups, a Pearson chi-square test was used. A paired t-test was calculated to compare the cephalometric changes pre and post Invisalign and FFA treatments, and an unpaired t-test was used to compare differences between the two treatment groups. As some measurements did not follow a normal distribution, Wilcoxon signed ranks and Mann-Whitney U-tests were performed accordingly. All tests were two-tailed and analyzed at the 5% significance level.
RESULTS
Intraexaminer Reliability
The intraclass correlation coefficients for the repeated measurements were greater than 0.90, indicating that the measurements were reproducible (Table 1).
Table 1.
Intraclass Correlation Coefficients
| Variable |
ICC |
95% Confidence Interval |
P Value |
|
| Lower Bound |
Upper Bound |
|||
| SNA | 0.98 | 0.90 | 0.99 | <.001 |
| SNB | 0.98 | 0.93 | 0.99 | <.001 |
| ANB | 0.91 | 0.69 | 0.98 | <.001 |
| Facial axis | 0.94 | 0.78 | 0.99 | <.001 |
| SN–GoGn | 0.98 | 0.93 | 0.99 | <.001 |
| OP–GoGn | 0.97 | 0.90 | 0.99 | <.001 |
| ODI | 0.99 | 0.96 | 0.99 | <.001 |
| LAFH | 0.97 | 0.87 | 0.99 | <.001 |
| P:A facial height | 0.98 | 0.93 | 0.99 | <.001 |
| U1–PP | 0.98 | 0.91 | 0.99 | <.001 |
| U1–SN | 0.97 | 0.90 | 0.99 | <.001 |
| U6–PP | 0.98 | 0.90 | 0.99 | <.001 |
| L6–MP | 0.98 | 0.93 | 0.99 | <.001 |
| L1–MP | 0.93 | 0.73 | 0.98 | <.001 |
| IMPA | 0.98 | 0.94 | 0.99 | <.001 |
| OB | 0.96 | 0.85 | 0.99 | <.001 |
| OJ | 0.94 | 0.78 | 0.99 | <.001 |
| Upper lip–E-plane | 0.95 | 0.82 | 0.99 | <.001 |
| Lower lip–E-plane | 0.96 | 0.84 | 0.99 | <.001 |
| Nasolabial angle | 0.98 | 0.94 | 0.99 | <.001 |
SNAo = Sella-Nasion line to Point A; SNBo = Sella-Nasion line to Point A; ANBo = Point A-Nasion-Point B; Facial Axiso = Nasion-Basion/ Point Pt-Gnathion; SN-GoGno = Sella-Nasion/Gonion-Gnathion; OP-GoGno = Functional Occlusal Plane/Gonion-Gnathion; ODIo = Overbite Depth Indicator (A-B Plane/MP) + (FH/PP); ANS-Menton, mm = Anterior Nasal Spine-Menton; P:A Facial Height, % = Sella-Gonion/Nasion-Menton; U1-PPo = Vertical distance from U1 tip to palatal plane; U1-SNo = U1 to Sella-Nasion; U6-PP, mm = Vertical distance from U6 central groove to palatal plane; L1-MP, mm = Vertical distance from L1 tip to mandibular plane; L6-MP, mm = Vertical distance from L6 central groove to mandibular plane; IMPAo = L1 to mandibular plane; Overbite, mm = Vertical distance from U1 tip to L1 tip; Overjet, mm = Horizontal distance from facial surface of L1 to lingual surface of U1; Upper Lip- E plane, mm = Distance from upper lip to Ricketts' esthetic line; Lower Lip- E plane, mm = Distance from lower lip to Ricketts' esthetic line; Nasolabial Angle = intersection of upper lip and columella at Subnasale.
Descriptive Statistics
The mean age of the Invisalign group was 37.2 (standard deviation [SD] = 17.7) and for the FFA group was 27.1 (SD = 10.4). Two-way ANOVA to test the significance of age by gender and group indicated no significant differences between the Invisalign and FFA groups (P=0.267).
Of the Invisalign group, 58% were Class I and 42% were Class II. In the FFA group, 38% were Class I and 63% were Class II. Although the FFA group had a greater percentage of Class II patients than the Invisalign group, the results of the Pearson chi-square test revealed a P value of 0.763, indicating no significant differences.
In the Invisalign group, 15 (62.5%) patients had bite ramps from canine to canine, 8 (33.3%) had bite ramps that extended from lateral incisor to lateral incisor, and 1 (0.04%) received bite ramps only on the canines.
The mean number of trays on the maxillary arch was 33.17, whereas the mean number of mandibular trays was 31.17. A total of 22 (92%) patients began the G5 protocol and received bite ramps starting on the first tray. One (0.04%) patient started this protocol on the second tray, and one (0.04%) patient began on the third tray. Maxillary palatal root torque was added to maxillary trays in 9 patients (37.5%), whereas 15 (62.5%) did not.
Invisalign and FFA Measurements at Baseline
At T1, the median ODIs for the FFA and Invisalign groups were 83.45 degrees and 82.50 degrees, respectively, but the difference was not significant (P = .733; Table 2). In comparing the means of all other measurements between the Invisalign and FFA groups at baseline, values for the vertical distance from lower first molar central groove to mandibular plane (L6-MP), the vertical distance from upper first molar central groove to palatal plane (U6-PP), and overjet were significantly different.
Table 2.
Sample Baseline Comparisons
| Variable |
Invisalign |
FFA |
P Value |
||||
| Mean |
Median |
SD |
Mean |
Median |
SD |
||
| SNA | 83.45 | 83.00 | 2.61 | 82.89 | 83.00 | 3.45 | .53 |
| SNB | 78.52 | 77.95 | 2.62 | 77.85 | 78.65 | 3.05 | .42 |
| ANB | 4.90 | 5.40 | 1.87 | 5.04 | 5.45 | 2.00 | .81 |
| Facial axis | 90.87 | 90.30 | 2.97 | 91.58 | 92.10 | 3.93 | .59a |
| Sn–GoGn | 24.50 | 24.85 | 4.99 | 24.37 | 24.70 | 4.59 | .92 |
| OP–GoGn | 13.48 | 13.65 | 3.00 | 12.65 | 12.25 | 2.49 | .30 |
| ODI | 83.95 | 82.50 | 3.37 | 84.57 | 83.45 | 3.80 | .73a |
| ANS–Menton | 58.63 | 58.40 | 2.95 | 60.18 | 60.80 | 5.20 | .16a |
| P:A facial height | 69.25 | 70.15 | 4.01 | 70.76 | 71.20 | 5.42 | .37a |
| U1–PP | 26.88 | 27.05 | 1.67 | 28.05 | 27.55 | 2.54 | .07 |
| U1–SN | 99.81 | 101.45 | 6.03 | 99.00 | 97.75 | 7.38 | .68 |
| U6–PP | 17.90 | 17.90 | 1.60 | 20.88 | 29.90 | 2.51 | <.001 |
| L1–MP | 37.38 | 38.45 | 3.45 | 36.72 | 36.40 | 3.16 | .27a |
| L6–MP | 23.56 | 23.05 | 2.14 | 26.88 | 27.20 | 2.48 | .00a |
| IMPA | 100.92 | 101.80 | 5.72 | 98.27 | 96.60 | 7.63 | .20a |
| OB | 4.49 | 4.20 | 1.00 | 4.60 | 4.55 | 1.12 | .87a |
| OJ | 3.66 | 3.55 | 1.43 | 4.74 | 4.30 | 1.35 | .01 |
| Upper lip–E plane | −2.80 | −2.75 | 2.03 | −2.90 | −3.20 | 2.69 | .89 |
| Lower lip–E plane | −2.00 | −2.05 | 2.24 | −1.34 | −1.40 | 2.99 | .39 |
| Nasolabial angle | 110.02 | 110.15 | 8.09 | 107.09 | 106.15 | 7.52 | .20 |
Mann-Whitney U-test. Bold font indicates statistical significance at P< .05.
Within-Group Changes
The following variables showed statistically significant changes in the Invisalign group from T1 to T2: mandibular plane angle (Sn–GoGn), ANS-Menton, U1–PP, L1–MP, U6–PP, L6–MP, facial axis, overbite, overjet, ODI, SNB, upper lip to E-plane, and lower lip to E-plane (Table 3).
Table 3.
Comparisons Between Invisalign and FFA T1 to T2
| Variable |
Invisalign, T1–T2 |
FFA, T1–T2 |
Invisalign vs FFA, P Value |
||||||
| Mean |
Median |
SD |
P Value |
Mean |
Median |
SD |
P Value |
||
| SNA | 0.07 | 0.45 | 0.88 | .697 | −0.19 | −0.45 | 1.14 | .419 | .39a |
| SNB | 0.32 | 0.35 | 0.65 | .025 | 0.70 | 0.85 | 1.16 | .007 | .09a |
| ANB | −0.23 | −0.15 | 1.00 | .280 | −0.99 | −0.85 | 1.18 | <.001 | .019 |
| Facial axis | −1.30 | −1.55 | 1.46 | <.001 | −1.17 | −1.20 | 1.50 | .001 | .763 |
| Sn–GoGn | 0.65 | 0.80 | 0.98 | .003 | 1.15 | 0.95 | 0.92 | <.001 | .078 |
| OP–GoGn | 0.41 | 0.35 | 1.38 | .156 | 0.32 | 0.70 | 1.07 | .154 | .78 |
| ODI | −1.51 | −1.70 | 0.96 | <.001b | −2.03 | −2.10 | 1.07 | <.001b | .03a |
| ANS–Menton | 0.64 | 0.75 | 1.10 | .009 | 1.85 | 2.00 | 1.49 | <.001 | .003 |
| P:A face height | −0.66 | −0.65 | 1.72 | .073 | −0.91 | −0.95 | 1.50 | .007 | .594 |
| U1–PP | −0.88 | −1.00 | 0.57 | <.001 | −1.14 | −1.35 | 1.28 | <.001 | .35a |
| U1–SN | 0.59 | 1.30 | 3.07 | .359 | 4.14 | 5.30 | 5.15 | .001 | .01a |
| U6–PP | 0.35 | 0.50 | 0.57 | .007 | 0.55 | 0.90 | 1.16 | .030 | .03a |
| L1–MP | −1.30 | −1.50 | 0.90 | <.001 | −2.06 | −2.35 | 1.26 | <.001 | .00a |
| L6–MP | 0.58 | 0.55 | 0.76 | .001 | 0.75 | 0.80 | 0.87 | <.001 | .36a |
| IMPA | 0.34 | 0.05 | 2.92 | .577 | 3.50 | 4.15 | 2.96 | <.001 | .00a |
| OB | −1.33 | −1.30 | 0.61 | <.001 | −2.02 | −1.75 | 0.86 | <.001 | .003 |
| OJ | −0.79 | −0.95 | 0.92 | <.001 | −1.41 | −1.55 | 1.30 | <.001 | .063 |
| Upper lip–E plane | 0.63 | 0.55 | 1.14 | .013 | −0.72 | −0.90 | 1.41 | .020 | .001 |
| Lower lip–E plane | 0.58 | 0.80 | 1.34 | .043 | −0.51 | −0.60 | 1.76 | .167 | .019 |
| Nasolabial angle | −0.14 | −0.95 | 3.10 | .825 | 3.53 | 5.25 | 5.85 | .007 | .01a |
Between-group significance determined using the Mann-Whitney U-test.
ODI within group significance determined using Wilcoxon signed rank test. Bold font indicates statistical significance at P< .05.
For the FFA group, the following variables were statistically significant between T1 and T2: Sn–GoGn, ANS–Menton, U1–PP, L1–MP, U6–PP, L6–MP, facial axis, overbite, overjet, ODI, posterior:anterior facial height, SNB, ANB, IMPA, U1–SN, upper lip to E-plane, and nasolabial angle. The median ODI change for the FFA and Invisalign groups was −2.10 and −1.70, respectively (Figure 1).
Figure 1.
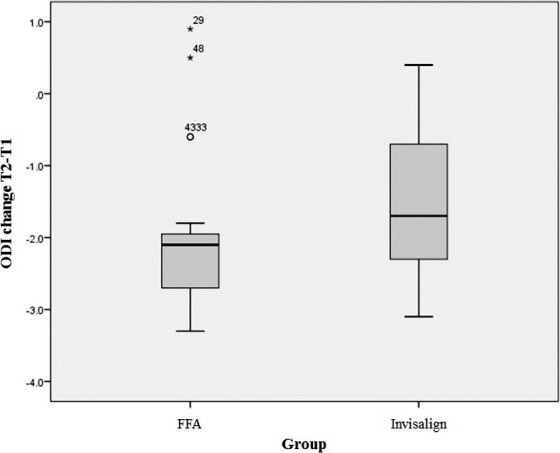
Change in ODI from T1 to T2 between the Invisalign and FFA groups.
Between-Group Changes
In comparing the means between the Invisalign and FFA groups, the following measurements were found to be statistically significant: ANS–Menton, overbite, ANB, upper lip to E-plane, lower lip to E-plane, L1–MP, U6–PP, ODI, IMPA, U1–SN, and nasolabial angle.
Comparison of Measurements by G5 Ramp Location
Among those patients in the Invisalign group, the effects of having the bite ramps located on different teeth can be seen in Table 4. No statistical significance was found on any measurement from having the bite ramps located on an upper canine to canine versus lateral incisor to lateral incisor.
Table 4.
Changes T1 to T2 for the Invisalign Group According to Bite Ramp Location
| Variable |
Ramp Location |
N |
Mean |
SD |
P Value |
| Sn–GoGn, degree | Ramp 3-3 | 15 | 0.393 | 0.960 | .084 |
| Ramp 2-2 | 8 | 1.150 | 0.938 | ||
| OB, mm | Ramp 3-3 | 15 | −1.347 | 0.722 | .870 |
| Ramp 2-2 | 8 | −1.300 | 0.438 | ||
| ODI, degree | Ramp 3-3 | 15 | −1.380 | 1.041 | .587 |
| Ramp 2-2 | 8 | −1.613 | 0.779 | ||
| IMPA, degree | Ramp 3-3 | 15 | 1.173 | 2.211 | .159 |
| Ramp 2-2 | 8 | −0.525 | 3.376 |
DISCUSSION
This study analyzed the outcomes of Invisalign G5 protocol in comparison to FFA for the correction of skeletal deep bites. At T1, three measurements showed statistically significant differences (P < .05) between the Invisalign and FFA groups: L6–MP, U6–PP, and overjet. As such, comparison of the changes in these variables between groups should be interpreted with caution.
In both the Invisalign and FFA groups, several skeletal measurements showed statistically significant intragroup changes between pretreatment and posttreatment. The Sn–GoGn angle increased in the FFA group by 1.15 degrees (P < .001), whereas it increased 0.65 degrees (P = .003) in the Invisalign group. The ODI angle decreased in the FFA group by 2.03 degrees (P < .001), whereas it decreased 1.51 degrees (P < .001) in the Invisalign group. When the ODI changes were compared between the groups, significant differences were noted (P = .030). It is possible Invisalign was not as effective as FFA in translating reverse curve arch wires into aligners as the plastic would perpetually hinder the teeth from contacting as much as they would in braces. However, the fact that there was still a statistically significant increase in the Invisalign group suggested that the G5 protocol was capable of decreasing a skeletal deep bite, possibly resulting from the effectiveness of the bite ramps in disoccluding the posterior teeth, allowing more buccal extrusion than would have otherwise been possible; in adults, this could result in mandibular rotation. This finding of vertical skeletal increase with Invisalign was similar to that of another study8 that reported a significant increase of 0.5 degrees (P = .01) in the mandibular plane angle of deep bite patients. The study was completed prior to the introduction of G5, however, so the increased skeletal change seen in the current study could be explained by this new protocol. It was also possible that more incisor intrusion11 (true intrusion) was achieved in the Invisalign group than in the FFA group.
Studies have reported that change in the lower anterior facial height for deep bite patients varies depending on the type of mechanics employed.1,11 In this study, the ANS–Menton increased significantly in both the Invisalign group (0.64 mm) and the FFA group (1.85 mm). The variability in this measurement is also seen throughout the literature. One study reported a 1.4 mm increase in ANS–Menton between pretreatment and posttreatment of adult deep bite cases for which mechanics involved leveling with conventional continuous arch wires and Class II elastics where indicated.12 However, Dake and Sinclair11 showed a statistically significant (P < .05) decrease in ANS–Menton when Ricketts intrusive mechanics were used.
In both the Invisalign and FFA groups, multiple dental measurements showed significant changes between pretreatment and posttreatment. The maxillary incisors intruded 1.14 mm (U1–PP) in the FFA group, and 0.88 mm in the Invisalign group. In the FFA group, this was achieved through a combination of intrusion arches, stepping up the wire, and placing palatal root torque. In the Invisalign group, only 9 (37.5%) patients had ClinCheck (Align Technology, CA) instructions that included palatal root torque to the maxillary incisors. Another factor that may have contributed to this change was the presence of the virtual bite ramps.
The mandibular incisors intruded (L1–MP) 2.06 mm in the FFA group and 1.30 mm in the Invisalign group. This finding was in contrast to Khosravi et al.,8 who found no significant change in mandibular incisor intrusion in deep bite adults treated with Invisalign. Rather, a key bite opening mechanism reported in their study was through mandibular incisor proclination. However, not all practitioners in their study used virtual bite ramps, and their study was completed prior to the introduction of the G5 protocol.
The significantly greater amount of L1–MP intrusion in the FFA group needs to be analyzed taking into account true versus relative intrusion. The amount of intrusion in the FFA group was similar to results reported in another study13 assessing treatment changes in adult deep bite patients where 1.8 mm of mandibular incisor intrusion was seen. The FFA group in the previous study and the current study also had significant flaring of the mandibular incisors. As the Invisalign group had a significant increase in the amount of mandibular incisor intrusion with minimal proclination, it can be concluded that the new G5 pressure areas7 were effective in intrusion mechanics.
In the current study, the change in mandibular incisor proclination was negligible in the Invisalign group. This may have been because the patients initially were considerably proclined with a mean IMPA of 100.9 degrees and the practitioner did not want to compromise the mandibular incisor position. It also could be due to interproximal enamel reduction in the mandibular arch, and this should be addressed in future studies.
In this study, the overbite decreased significantly in each of the two groups, but the decrease was greater in the FFA group (P < .001) than in the Invisalign group. Previous studies6,8,14,15 have shown that when treatment strategies with Invisalign involve virtual bite ramps, overcorrection of the overbite to 0 mm and sufficient leveling of curve of Spee, the deep overbite can be reduced. When the groups were compared against each other, the FFA group showed significantly greater bite opening than the Invisalign group.
One study released by Align Technology showed a 2.56 mm reduction in overbite with the use of the G5 protocol,6 whereas another study showed a 1.5 mm reduction in overbite.8 The current study showed a smaller bite opening of 1.33 mm. This difference can partly be explained by the previous studies being based on dental deep bites with no consideration of the skeletal vertical pattern. Previous studies10,16–18 have shown that opening deep bites in a true hypodivergent patient was more difficult than in the dental deep bite patient.
The maxillary and mandibular molars extruded significantly in both the Invisalign and FFA groups. The extrusion of the mandibular molars in the Invisalign group was consistent with that of another study that found 0.5 mm of mandibular first and second molar extrusion in deep bite patients treated with Invisalign.8 Thus, the extrusion of the mandibular first molar did not appear to be greater than Invisalign pre-G5 protocols.
The effects of having bite ramps on different teeth (maxillary canine to canine vs lateral incisor to lateral incisor) were shown not to be significantly different for all measurements studied. There is no standard protocol recommended by Invisalign with regard to placement of the virtual bite ramps. However, a general rule of thumb is that the ramps only extend to the canines in situations of extreme overjet where the ramps otherwise might not have reached to contact mandibular anterior teeth. Future studies are warranted to understand the effects of ramp location on deep bite correction.
Patient compliance was not assessed in this study. It is possible this may have affected the amount of overbite correction observed in the Invisalign group. Future studies should attempt to analyze three-dimensional study models with particular regard to crowding. Unraveling crowding has an effect on IMPA angle and thus can play a crucial role in bite opening. Future studies should also account for Class II elastic wear pattern, frequency, and forces used. This variable may have influenced the amount of bite opening reported in this study.
It is critical to note that, even with the introduction of the G5 protocol, the success of any Invisalign treatment ultimately depends on proper formulation of the ClinCheck plan. Overengineering of mandibular reverse curve of Spee mechanics on the virtual set-up by extruding posterior teeth and intruding anterior teeth to an open bite is important to achieve adequate results in adult deep bite patients.
CONCLUSIONS
Although FFA treatment has more apparent skeletal change for deep bite adult patients when compared with G5 Invisalign, both systems appear effective in opening deep bites at the dentoalveolar and skeletal levels.
REFERENCES
- 1.Parker CD, Nanda RS, Currier GF. Skeletal and dental changes associated with the treatment of deep bite malocclusion. Am J Orthod Dentofacial Orthop. 1995;107(4):382–393. doi: 10.1016/s0889-5406(95)70091-9. [DOI] [PubMed] [Google Scholar]
- 2.Nanda R. Correction of deep overbite in adults. Dent Clin North Am. 1997;41(1):67–87. [PubMed] [Google Scholar]
- 3.Djeu G, Shelton C, Maganzini A. Outcome assessment of Invisalign and traditional orthodontic treatment compared with the American Board of Orthodontics objective grading system. Am J Orthod Dentofacial Orthop. 2005;128(3):292–298. doi: 10.1016/j.ajodo.2005.06.002. discussion 98. [DOI] [PubMed] [Google Scholar]
- 4.Gracco A, Mazzoli A, Favoni O, et al. Short-term chemical and physical changes in invisalign appliances. Aust Orthod J. 2009;25(1):34–40. [PubMed] [Google Scholar]
- 5.Boyd RL. Surgical-orthodontic treatment of two skeletal Class III patients with Invisalign and fixed appliances. J Clin Orthod. 2005;39(4):245–258. [PubMed] [Google Scholar]
- 6.Invisalign. Invisalign G5 Innovations. Improved Clinical Outcomes for Deep Bite Treatment. 2016 Align Technology, Inc. www.invisalign.com/braces-for-adults-and-teens Accessed 8/1/2017.
- 7.Invisalign. Invisalign G5 Innovations for Deep Bite. San Jose, CA: Align Technology, Inc.; 2013. [Google Scholar]
- 8.Khosravi R, Cohanim B, Hujoel P, et al. Management of overbite with the Invisalign appliance. Am J Orthod Dentofacial Orthop. 2017;151(4):691–99. doi: 10.1016/j.ajodo.2016.09.022. e2. [DOI] [PubMed] [Google Scholar]
- 9.Baccetti T, Franchi L, Giuntini V, et al. Early vs late orthodontic treatment of deepbite: a prospective clinical trial in growing subjects. Am J Orthod Dentofacial Orthop. 2012;142(1):75–82. doi: 10.1016/j.ajodo.2012.02.024. [DOI] [PubMed] [Google Scholar]
- 10.Kim YH. Overbite depth indicator with particular reference to anterior open-bite. Am J Orthod. 1974;65(6):586–611. doi: 10.1016/0002-9416(74)90255-3. [DOI] [PubMed] [Google Scholar]
- 11.Dake ML, Sinclair PM. A comparison of the Ricketts and Tweed-type arch leveling techniques. Am J Orthod Dentofacial Orthop. 1989;95(1):72–78. doi: 10.1016/0889-5406(89)90138-8. [DOI] [PubMed] [Google Scholar]
- 12.McDowell EH, Baker IM. The skeletodental adaptations in deep bite correction. Am J Orthod Dentofacial Orthop. 1991;100(4):370–375. doi: 10.1016/0889-5406(91)70076-9. [DOI] [PubMed] [Google Scholar]
- 13.Kale Varlik S, Onur Alpakan O, Turkoz C. Deepbite correction with incisor intrusion in adults: a long-term cephalometric study. Am J Orthod Dentofacial Orthop. 2013;144(3):414–9. doi: 10.1016/j.ajodo.2013.04.014. [DOI] [PubMed] [Google Scholar]
- 14.Schupp W, Haubrich J, Neumann I. Class II correction with the Invisalign system. J Clin Orthod. 2010;44(1):28–35. [PubMed] [Google Scholar]
- 15.Boyd RL. Esthetic orthodontic treatment using the invisalign appliance for moderate to complex malocclusions. J Dent Educ. 2008;72(8):948–967. [PubMed] [Google Scholar]
- 16.Berg R. Stability of deep overbite correction. Eur J Orthod. 1983;5(1):75–83. doi: 10.1093/ejo/5.1.75. [DOI] [PubMed] [Google Scholar]
- 17.Engel G, Cornforth G, Damerell JM, et al. Treatment of deep-bite cases. Am J Orthod. 1980;77(1):1–13. doi: 10.1016/0002-9416(80)90220-1. [DOI] [PubMed] [Google Scholar]
- 18.Huang GJ, Bates SB, Ehlert AA, et al. Stability of deep-bite correction: a systematic review. J World Fed Orthod. 2012;1(3):e89–e86. doi: 10.1016/j.ejwf.2012.09.001. [DOI] [PMC free article] [PubMed] [Google Scholar]