

Abstract
Objectives
To compare the effects of a hybrid miniscrew-supported expander versus a conventional Hyrax (CH) expander in growing patients.
Materials and Methods
Forty patients were randomized into two groups: a hybrid Hyrax (HH) expander group using a Hyrax expander with two miniscrews and a CH expander group. The final sample had 18 subjects (8 female, 10 male; initial age of 10.8 years) in the HH group and 14 subjects (6 female, 8 male; initial age of 11.4 years) in the CH group. Cone-beam computed tomography examinations and digital dental models were obtained before expansion and 11 months postexpansion. The primary outcomes included the orthopedic transverse effects of expansion. Intergroup comparison was performed using analysis of covariance (P < .05).
Results
Significantly greater increases in the nasal cavity width, maxillary width, and buccal alveolar crest width were found for the HH group. No intergroup differences were observed for dental arch width or shape changes.
Conclusions
The HH group showed greater increases in the nasal cavity width, maxillary width, and buccal alveolar crest width. No differences were observed for intermolar, interpremolar, or intercanine widths; arch length; or arch perimeter. Arch size and shape showed similar changes in both groups.
Keywords: Orthodontics, Interceptive, Orthodontic appliance, Palatal expansion technique, Dental models, Imaging, Three-dimensional
INTRODUCTION
Rapid maxillary expansion (RME) is indicated for the treatment of maxillary constriction. Orthopedic opening of the midpalatal suture represents the main effect of an RME procedure.1 Conventional expanders are commonly used for RME. Recently, innovative expanders using skeletal anchorage for performing RME procedure have been described.2,3 Is there an increase in the orthopedic effect of RME by incorporating skeletal anchorage to conventional expanders?
The first report of skeletal-anchored RME was in a 14-year-old girl and used two small implants in the palate.4 Lee et al.2 used a miniscrew-supported RME procedure. Using four palatal miniscrews as anchorage, increases of 8.3 mm and 2.4 mm were obtained in the intermolar distance and in the maxillary basal bone, respectively, in a young adult patient.2 Miniscrew-anchored rapid palatal expansion (MARPE) seems to extend the age limit for RME.2,5 A previous study using MARPE in a sample of 69 adult patients with a mean age of 20.9 years showed a success rate of 86.96% in opening the midpalatal suture.5 An increase in the maxillary width of 2.11 mm was found after MARPE.5 The nasal cavity width and intermolar width also showed significant increases of 1.07 mm and 8.32 mm, respectively, after expansion.5
Wilmes et al.3 reported the use of a hybrid Hyrax (HH) for growing patients. The HH was anchored on the maxillary permanent first molars and on two parasutural miniscrews in the anterior region of the palate.3 The use of a HH was indicated as anchorage for maxillary protraction with facemask therapy.6 A previous study compared the periodontal and skeletal effects produced by RME using hybrid and conventional Hyrax (CH) expanders in adolescent patients in the permanent dentition.7 Similar skeletal effects were found in both groups.7 The Hyrax expander produced greater increases in the interpremolar distances as compared with the hybrid expanders.7 A greater decrease in the first premolar buccal bone plate was found for the CH expanders when compared with hybrid expanders.7
The orthopedic outcomes of miniscrew-supported maxillary expanders were more extensively studied in adult patients.2,5 The literature is limited regarding the dentoskeletal effects of the hybrid expander in growing patients. A previous study compared the dentoskeletal and periodontal effects of the hybrid and CH expanders. However, a small sample size and the amount of screw activation was not standardized.7 Further studies are necessary to more extensively compare the orthopedic effects produced by the hybrid and CH expander in growing individuals.
Objective
The aim of this study was to compare the orthopedic outcomes of hybrid and CH expanders in growing patients. The null hypothesis was that the dentoskeletal effects produced by both expanders were similar.
MATERIALS AND METHODS
Trial Design and Settings
This study was a secondary data analysis from a previous single-center randomized clinical trial (RCT). Two parallel arms and a 1:1 allocation ratio was used. Changes in participant number were made after trial commencement (Figure 1).
Figure 1.

CONSORT flow chart.
The study followed the Consolidated Standards of Reporting Trials guidelines (CONSORT). The study was approved by the Ethics in Research Committee of Bauru Dental School, University of São Paulo, Brazil (protocol No. 67610717.7.0000.5417). All patients and parents provided written informed consent before treatment.
The individuals were recruited in the Clinic of Orthodontics of Bauru Dental School, University of São Paulo, from July 2017 to March 2018. The sample consisted of 40 individuals with posterior crossbites and age varying from 9 to 13 years. The eligibility criteria included (1) both sexes, (2) late mixed or early permanent dentition, and (3) Class I and Class III malocclusions. Exclusion criteria included individuals with a history of previous orthodontic treatment and patients with special needs or syndromes.
Interventions
The HH group was treated with a premanufactured 9-mm HH expander (PecLab, Belo Horizonte, Brazil). The expander was inserted posteriorly to the third palatal rugae, supported by bands on the maxillary first permanent molars and 1-mm away from the palatal surface (Figure 2A). Two parasutural miniscrews of 1.8-mm diameter, 7-mm length, and 4-mm transmucosal length were installed in the expander slots (Figure 2A). The miniscrews were installed under local anesthesia, using a contra-angle implant driver with maximum insertion torque of 35 Ncm and 30 rotations/min. The miniscrews were installed with approximately a 45° inclination relative to the occlusal plane, following the expander slot chamfer (Figure 3).
Figure 2.

(A) Hybrid Hyrax expander group. (B) Conventional Hyrax expander group.
Figure 3.
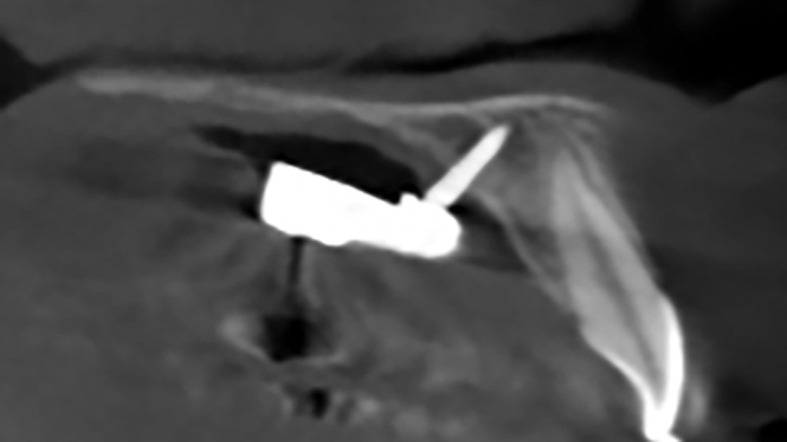
Miniscrews installed with a 45° inclination in the paramedian anterior palate in a subject using the hybrid expander.
In the CH group, the RME was performed using a CH expander (Figure 2B). Bands on the maxillary first permanent molars and bonded C-shape clasps on the maxillary canines or premolars were used to support the expander (Figure 2B). In both groups, the expander screw was activated a one-quarter turn twice a day for 14 days, achieving 5.6 mm of expansion. After the active phase, the expanders were maintained in the oral cavity for 11 months as retention until bone-anchored maxillary protraction therapy was performed for a previous study. The treatment times were 11.38 and 11.00 months for the experimental and control groups, respectively.
Cone-beam computed tomography (CBCT) and digital dental models were obtained before expansion (T1) and after the expander removal (T2). The head orientation was standardized in the sagittal view, positioning the palatal plane parallel to the horizontal plane; in the frontal view, leveling the orbital plane parallel to the horizontal plane; and, in the axial view, positioning the vertical plane simultaneously on the anterior and posterior nasal spine.
Outcomes
The primary outcomes of this RCT were the dentoskeletal changes produced by maxillary protraction that were evaluated in a previous study.
The outcomes of the current study included the dentoskeletal changes of RME measured on CBCT scans. A coronal section passing through the center of the palatal root of the right maxillary permanent first molar was used to evaluate the transverse measurements (Table 1). The variables illustrated in Figure 4A were measured using Nemoscan software (Nemotec, Madrid, Spain).
Table 1.
Variable Definitions
| Variable |
Definition |
| Transversal distances (mm) | |
| Nasal cavity width | The greater width of the nasal cavity lower third measured in parallel to the horizontal plane |
| Palatal root distance width | Dental arch width measured at the most apical level of the palatal roots parallel to the horizontal plane |
| Maxillary width | Maxillary width at the level of the hard palate parallel to the horizontal plane |
| Palatal alveolar crest width | Maxillary width at the level of the interpalatal alveolar crest parallel to the horizontal plane |
| Buccal alveolar crest width | Maxillary width at the level of the buccal alveolar crest parallel to the horizontal plane |
| Arch width | Dental arch width measured at the level of the buccal cusp points parallel to the horizontal plane |
| Tooth inclination | Angle between lines passing through the buccal and lingual cusp tips of the first molars |
| Dental model analysis (mm) | |
| 6-6 width | Intermolar width measured at the level of the cusp tips |
| 5-5 width | Inter–second premolar width measured at the level of the cusp tips |
| 4-4 width | Inter–first premolar width measured at the level of the cusp tips |
| 3-3 width | Intercanine width measured at the level of the cusp tips |
| Arch length | Arch length measured perpendicularly in the horizontal plane from a line connecting the mesial aspects of the first permanent molars to the mesial edge of the right permanent incisor |
| Arch perimeter | Arch perimeter measured by the sum of four segments connecting the mesial aspect of the right first permanent molar to the mesial aspect of the left first permanent molar |
Figure 4.

(A) Coronal slice showing the transverse measurements (Table 1). (B) Transverse measurements performed on the digital dental models (Table 1). (C) Landmarks used for arch shape analysis.
The arch widths (at the molars, premolars, and canines), arch length, and arch perimeter (Figure 4B; Table 1) were evaluated using OrthoAnalyzer 3D software (3Shape A/S, Copenhagen, Denmark). Arch size and shape were measured using the software Stratovan Checkpoint (Stratovan Corporation, Davis, Calif) and MorphoJ (Klingenberg Lab, Manchester, UK) according to a previous study (Figures 4C; Figure 5).8 Digital dental models were imported into the Stratovan Checkpoint software. Fourteen landmarks were placed on both T1 and T2 dental models (Figure 4C). The landmark coordinates (x and z) were imported into the MorphoJ software. The arch size was calculated by using the centroid size of each dental arch at T1 and T2. Generalized Procrustes analysis was used to calculate the mean arch shape at each time point and the interphase arch shape changes.
Figure 5.
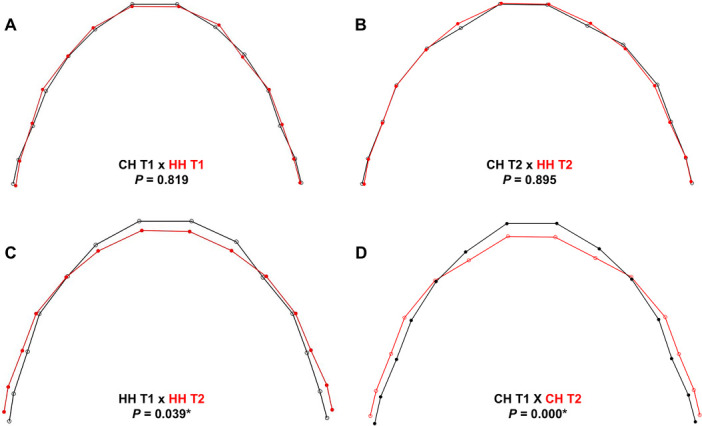
(A) Intergroup comparison of preexpansion arch shape. (B) Intergroup comparison of postexpansion arch shape. (C, D) Arch shape before (black line) and after expansion (gray) in the hybrid (C) and conventional Hyrax (D) groups.
Sample Size Calculation
Sample size calculation was performed to provide 80% test power, a significance level of .05, a standard deviation of 1.18 mm for maxillary width,9 and a minimum intergroup difference of 2.0 mm. A sample of eight patients was required for each group.
Randomization and Blinding
Randomization was performed electronically using the Randomization.com website (http://www.randomization.com). Opaque, sealed, and numbered envelopes containing the group name were organized and opened according to the sequence generated by the randomization.
All CBCT scans were deidentified before assessment to avoid bias. Only a simple blinding was performed, once both operator and patient were aware of the type of treatment performed.
Statistical Analyses
After 1 month, the same operator (F.M.) randomly selected and remeasured 30% of the sample. The intraclass correlation coefficient (ICC) was used to assess the reliability of repeated measures.
Normal distribution was verified by Kolmogorov-Smirnov tests. We used t-tests for baseline comparisons. Nonparametric tests were applied to variables without normal distribution. An analysis of covariance using the baseline data as a covariate was applied to adjust for the influence of the initial maxillary dimensions on the expansion changes. A significance level of 5% was regarded for all tests.
RESULTS
Forty growing individuals agreed to participate of the trial. Twenty patients were allocated to the HH group. One patient interrupted treatment, and one was excluded because of palatal miniscrew instability. The final sample of the HH group included 18 individuals (8 female; 10 male) with a mean age of 10.80 years. The total treatment time was 11.38 months.
Fifteen individuals were allocated to the CH group. Five were not allocated because of group interruption related to side effects observed during maxillary protraction in the original RCT. One patient quit treatment. The final sample of the CH group was composed of 14 individuals with a mean age of 11.44 years (6 female and 8 male) and 11 months of treatment time. Figure 1 contains the completed participants' flow chart.
Similar characteristics regarding sex, initial age, and treatment time were found in both groups (Table 2). Intergroup differences were found for 3 of 15 variables at T1 (Table 3). The HH group presented slightly greater transverse dimensions before treatment than the CH group did.
Table 2.
Baseline Characteristics of the Groups and Treatment Times
| Variable |
Group HH |
Group CH |
P Valuea |
| Sex, n | .928 | ||
| Male | 10 | 8 | |
| Female | 8 | 6 | |
| Total, n | 18 | 14 | |
| Mean age, y (SD) | 10.80 (1.04) | 11.44 (1.26) | .102 |
| Treatment time, m (SD) | 11.38 (3.98) | 11.00 (3.78) | .782 |
Chi-square test (sex); t-test (age and treatment time).
Table 3.
Intergroup Comparisons of the Starting Forms (t-Test and Mann-Whitney U-Test)
| Variable |
Group HH, Mean (SD) |
Group CH, Mean (SD) |
95% CI, Lower, Upper |
P Value* |
| Transversal distances (mm) | ||||
| Nasal cavity width | 28.81 (2.35) | 28.33 (2.18) | −1.18, 2.14 | .561 |
| Palatal root distance width | 34.56 (2.86) | 31.65 (3.31) | 0.64, 5.18 | .021*a |
| Maxillary width | 64.64 (3.47) | 62.59 (4.85) | −0.96, 5.05 | .175 |
| Palatal alveolar crest width | 36.32 (2.66) | 33.94 (3.97) | −0.06, 4.83 | .056 |
| Buccal alveolar crest width | 59.94 (3.40) | 57.08 (3.86) | 0.19, 5.52 | .036* |
| Arch width | 57.02 (3.12) | 54.69 (4.32) | −0.41, 5.07 | .093 |
| Premolar inclination | 162.66 (13.61) | 156.73 (9.63) | −4.38, 16.24 | .245 |
| Molar inclination | 158.26 (11.52) | 153.66 (7.03) | −2.61, 11.80 | .203 |
| Dental model analysis (mm) | ||||
| 6-6 width | 55.35 (3.27) | 52.59 (4.77) | −0.31, 5.82 | .077 |
| 5-5 width | 50.47 (2.95) | 47.57 (5.12) | −0.25, 6.05 | .070 |
| 4-4 width | 45.61 (2.72) | 42.63 (3.86) | 0.36, 5.58 | .027* |
| 3-3 width | 36.83 (2.66) | 34.78 (3.00) | −0.99, 5.08 | .170 |
| Arch length | 29.09 (3.00) | 27.66 (2.80) | −0.80, 3.66 | .201 |
| Arch perimeter | 77.64 (5.03) | 75.02 (5.52) | −1.75, 7.00 | .228 |
| Arch size | ||||
| Maxillary arch size | 91.96 (5.54) | 91.09 (5.86) | −4.00, 5.74 | .716 |
P values for Mann-Whitney U-test.
Statistically significant at P < .05, t-test.
The ICC ranged from .883 to .999 for all transverse measurements, showing good reproducibility. Landmarks assigned for arch shape analysis demonstrated ICCs ranging from .745 to .999.
All patients from both groups demonstrated a midpalatal suture split during RME. A significantly greater increase in nasal cavity and maxillary width and buccal alveolar crest width was found for the hybrid expander (Table 4). No intergroup differences were found for the other maxillary widths and tooth inclinations.
Table 4.
Intergroup Treatment Change Comparisons (Analysis of Covariance)
| Variable |
Group HH, Mean Changes (SD) |
Group CH, Mean Changes (SD) |
Difference, Mean |
95% CI, Lower, Upper |
P Value* |
| Transversal distances (mm) | |||||
| Nasal cavity width | 2.26 (1.17) | 1.11 (0.95) | 1.15 | 0.40, 1.99 | .004* |
| Palatal root distance width | 3.52 (1.04) | 2.83 (1.34) | 0.69 | −0.47, 1.48 | .301 |
| Maxillary width | 1.82 (1.47) | 0.99 (0.84) | 0.83 | 0.04, 1.89 | .041* |
| Palatal alveolar crest width | 3.67 (1.26) | 3.02 (1.24) | 0.65 | −0.15, 1.81 | .097 |
| Buccal alveolar crest width | 3.22 (1.55) | 2.03 (1023) | 1.19 | 0.19, 2.47 | .023* |
| Arch width | 2.89 (1.40) | 2.67 (1.22) | 0.22 | −0.52, 1.47 | .335 |
| Premolar inclination | 1.81 (9.80) | 9.79 (11.21) | −7.98 | −10.82, 2.41 | .200 |
| Molar inclination | 2.86 (14.16) | 7.08 (11.00) | −4.22 | −6.12, 7.59 | .827 |
| Dental model analysis (mm) | |||||
| 6-6 width | 3.5 (1.24) | 3.47 (1.21) | 0.03 | −0.75, 1.23 | .624 |
| 5-5 width | 3.18 (2.12) | 4.23 (1.23) | −1.05 | −2.19, 0.78 | .338 |
| 4-4 width | 2.62 (1.76) | 4.07 (1.19) | −1.45 | −1.99, 0.44 | .201 |
| 3-3 width | 0.94 (1.12) | 0.54 (1.55) | 0.4 | −0.85, 2.20 | .356 |
| Arch length | −1.94 (1.36) | −2.2 (1.68) | 0.26 | −0.60, 1.66 | .347 |
| Arch perimeter | 0.11 (2.31) | −0.51 (1.70) | 0.62 | −0.58, 2.71 | .195 |
| Arch size | |||||
| Maxillary arch size | 3.62 (2.48) | 3.30 (1.92) | 0.32 | -1.01, 2.12 | 0.474 |
Statistically significant at P < .05.
No intergroup differences were found for intermolar, interpremolar, or intercanine distances; arch length; or perimeter (Table 4). Arch size displayed similar increases after treatment in both groups (Table 4). Both types of expander produced similar arch shape changes after RME (Figure 5).
One of the 38 palatal miniscrews was lost in the HH group. A 97.36% stability rate was found for palatal miniscrews. One patient was excluded from the sample after palatal miniscrew instability.
DISCUSSION
This study aimed to compare the orthopedic effects of RME with hybrid and CH expanders in growing patients. Both CBCT and digital dental models provide accurate information regarding the dentoskeletal effects produced by RME.10–12 Good reproducibility was found for dimensional measurements in both types of three-dimensional images (ICC ranging from .883 to .999). Previous studies also reported good reproducibility for measures performed on digital dental models.12,13 In agreement, a previous study also reported excellent intraexaminer reproducibility by assessing bone morphology in CBCT with different voxel sizes.14 A previous study also reported good intraexaminer reproducibility for transverse dimensions of the maxilla measured after RME on CBCT.15 In this study, CBCT three-dimensional images were used for planning miniscrew installation at T1 and planning comprehensive orthodontic treatment at T2.
The hybrid expander is an innovative treatment option for maxillary constriction, which incorporated miniscrews into the expansion procedure.2,3,5 In adult patients, greater bone resistance to midpalatal suture opening requires four miniscrews as anchorage.2,5 In growing patients, previous studies used two miniscrews in the maxillary expander with skeletal anchorage.3,7 In this study, midline diastema and radiologic suture opening was observed for all patients from both groups.
Previous studies demonstrated high stability rates for the palatal miniscrews.5,16 Only 1 of 38 palatal miniscrews was lost during maxillary expansion. In agreement with these findings, a sample of 69 adult patients treated with MARPE showed a stability rate of 95% for palatal miniscrews.5 The palate is a very suitable place to receive miniscrews with high stability rates, supporting heavier forces from RME.16 The possible explanations are the favorable bone quality and quantity and the presence of extensive keratinized mucosa in the paramedian anterior palate.17 In addition, previous studies demonstrated that stability is increased by splitting two miniscrews in the palate.16
A greater increase in the nasal cavity width was found for the HH expander as compared with the conventional expanders (Table 4). The hypothesis is that the palatal miniscrews transfer the expansion forces to higher maxillary levels, increasing the orthopedic outcome of RME in the nasal cavity. Previous studies have demonstrated an increase in nasal cavity width varying from 1.2 to 2.73 mm after conventional RME.7,15,18 A previous study in adolescents corroborated the current findings, demonstrating a greater increase in the nasal cavity width with a bone-borne expander as compared with a conventional tooth-borne expander.18 On the other hand, another study demonstrated similar increases in nasal cavity width after expansion using hybrid and Hyrax expanders in growing individuals.7 The possible explanation for this discrepancy was that, in the latter study, the amount of screw expansion was not standardized, and the cusp tip relationship was individually used as a reference to determine the amount of expansion.7 Considering the ratio between nasal cavity increase and the amount of screw activation, the Hybrid and conventional expanders demonstrated an orthopedic effect of approximately 40% and 20%, respectively. The hybrid expander also demonstrated a greater increase in maxillary width as compared with the conventional expander (Table 4), demonstrating a greater orthopedic effect at the level of maxillary basal bone. A previous study also demonstrated a greater increase in maxillary width in the bone-borne expander group as compared with the conventional expander in a sample of adolescents.9 Conversely, another study reported similarity between conventional and hybrid expanders for orthopedic effects in growing individuals.7 These differences might be related to the lack of expansion standardization.7
The buccal alveolar crest width also showed a greater increase after treatment in the HH group than in the CH group (Table 4). During the active expansion phase, hybrid expanders usually demonstrated a slight posterior divergence of the screw hinges due to the expansion limitation caused by the anterior skeletal anchorage (Figure 2A). As a consequence, the expansion force might have a greater impact on the dentoalveolar region of the maxillary first molars. Another assumption was that first molar eruption was restrained during the time the HH was in the oral cavity. A relative intrusion of maxillary first molars was observed in subjects of the HH group. These side effects could have combined to increase the molar intercrestal distance. Posterior tooth inclination increased similarly in both groups (Table 4). Two previous studies were controversial when comparing the amount of buccal inclination between tooth-borne and tooth-bone-borne expanders.7,18 Variations in these outcomes might be explained by different expander designs. In addition, the current findings should be analyzed with caution because cusp tip definitions in CBCT are not adequate.
All maxillary dental arch widths increased similarly in both groups (Table 4). The arch shape changes observed in Figure 5 were also similar between groups. It was observed that the premolar region demonstrated a slightly greater expansion in the CH expander group compared with the HH group (Figure 5B), although both groups demonstrated a significant arch shape change (Figure 5C,D). Arch size also increased similarly in both groups. A previous study reported that the Hyrax expander did not produce a change in arch shape.8 However, that study was conducted in patients with bilateral complete cleft lip and palate, which might explain the discrepancy.
Limitations
One limitation of the study was the lack of a nasal airflow analysis. Considering the nasal cavity width changes, future studies should evaluate the influence of HH expanders in the respiratory function of patients with oral breathing and sleep apnea. The sample size of the CH group was also a limitation. Future studies should be conducted to compare the effects of tooth-bone-borne and bone-borne expanders.
In all, while the functional outcomes of Hybrid expanders are unknown, the indication for skeletal anchored maxillary expansion in growing patients should be restricted to subjects with deficient dental anchorage for conventional expanders (oligodontia and tooth transition), patients with periodontal bone deficiencies on the anchorage teeth, and as anchorage for bone protraction in Class III patients. The absence of an untreated control group for growth comparisons was another limitation of this study. However, using CBCT images in untreated subjects would have raised ethical concerns.
CONCLUSIONS
The hybrid Hyrax expander produced greater increases in the nasal cavity and maxillary widths as compared with the conventional Hyrax expander.
Similar dental effects were observed for hybrid and conventional expanders.
Arch size and shape changes were similar for both types of expanders.
ACKNOWLEDGMENTS
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001 and by the São Paulo Research Foundation, FAPESP (grants 2017/04141-9, 2017/24115-2 and 2019/03175-2). The authors thank PecLab (Belo Horizonte, Brazil) and Morelli (Sorocaba, Brazil) for the support.
REFERENCES
- 1.Haas AJ. The treatment of maxillary deficiency by opening the midpalatal suture. Angle Orthod. 1965;35:200–217. doi: 10.1043/0003-3219(1965)035<0200:TTOMDB>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 2.Lee KJ, Park YC, Park JY, Hwang WS. Miniscrew-assisted nonsurgical palatal expansion before orthognathic surgery for a patient with severe mandibular prognathism. Am J Orthod Dentofacial Orthop. 2010;137:830–839. doi: 10.1016/j.ajodo.2007.10.065. [DOI] [PubMed] [Google Scholar]
- 3.Wilmes B, Nienkemper M, Drescher D. Application and effectiveness of a mini-implant- and tooth-borne rapid palatal expansion device: the hybrid Hyrax. World J Orthod. 2010;11:323–330. [PubMed] [Google Scholar]
- 4.Garib DG, Navarro R, Francischone CE, Oltramari PV. Rapid maxillary expansion using palatal implants. J Clin Orthod. 2008;42:665–671. [PubMed] [Google Scholar]
- 5.Choi SH, Shi KK, Cha JY, Park YC, Lee KJ. Nonsurgical miniscrew-assisted rapid maxillary expansion results in acceptable stability in young adults. Angle Orthod. 2016;86:713–720. doi: 10.2319/101415-689.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Nienkemper M, Wilmes B, Franchi L, Drescher D. Effectiveness of maxillary protraction using a hybrid Hyrax-facemask combination: a controlled clinical study. Angle Orthod. 2015;85:764–770. doi: 10.2319/071614-497.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gunyuz Toklu M, Germec-Cakan D, Tozlu M. Periodontal, dentoalveolar, and skeletal effects of tooth-borne and tooth-bone-borne expansion appliances. Am J Orthod Dentofacial Orthop. 2015;148:97–109. doi: 10.1016/j.ajodo.2015.02.022. [DOI] [PubMed] [Google Scholar]
- 8.Pugliese F, Palomo JM, Calil LR, de Medeiros Alves A, Lauris JRP, Garib D. Dental arch size and shape after maxillary expansion in bilateral complete cleft palate: a comparison of three expander designs. Angle Orthod. 2019;90:233–238. doi: 10.2319/020219-74.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Lin L, Ahn HW, Kim SJ, Moon SC, Kim SH, Nelson G. Tooth-borne vs bone-borne rapid maxillary expanders in late adolescence. Angle Orthod. 2015;85:253–262. doi: 10.2319/030514-156.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Garib DG, Henriques JF, Janson G, Freitas MR, Coelho RA. Rapid maxillary expansion-tooth tissue-borne versus tooth-borne expanders: a computed tomography evaluation of dentoskeletal effects. Angle Orthod. 2005;75:548–557. doi: 10.1043/0003-3219(2005)75[548:RMETVT]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 11.Fleming PS, Marinho V, Johal A. Orthodontic measurements on digital study models compared with plaster models: a systematic review. Orthod Craniofac Res. 2011;14:1–16. doi: 10.1111/j.1601-6343.2010.01503.x. [DOI] [PubMed] [Google Scholar]
- 12.Grunheid T, Patel N, De Felippe NL, Wey A, Gaillard PR, Larson BE. Accuracy, reproducibility, and time efficiency of dental measurements using different technologies. Am J Orthod Dentofacial Orthop. 2014;145:157–164. doi: 10.1016/j.ajodo.2013.10.012. [DOI] [PubMed] [Google Scholar]
- 13.Stevens DR, Flores-Mir C, Nebbe B, Raboud DW, Heo G, Major PW. Validity, reliability, and reproducibility of plaster vs digital study models: comparison of peer assessment rating and Bolton analysis and their constituent measurements. Am J Orthod Dentofacial Orthop. 2006;129:794–803. doi: 10.1016/j.ajodo.2004.08.023. [DOI] [PubMed] [Google Scholar]
- 14.Sun Z, Smith T, Kortam S, Kim DG, Tee BC, Fields H. Effect of bone thickness on alveolar bone-height measurements from cone-beam computed tomography images. Am J Orthod Dentofacial Orthop. 2011;139:e117–e127. doi: 10.1016/j.ajodo.2010.08.016. [DOI] [PubMed] [Google Scholar]
- 15.Christie KF, Boucher N, Chung CH. Effects of bonded rapid palatal expansion on the transverse dimensions of the maxilla: a cone-beam computed tomography study. Am J Orthod Dentofacial Orthop. 2010;137:S79–S85. doi: 10.1016/j.ajodo.2008.11.024. [DOI] [PubMed] [Google Scholar]
- 16.Kim YH, Yang SM, Kim S, et al. Midpalatal miniscrews for orthodontic anchorage: factors affecting clinical success. Am J Orthod Dentofacial Orthop. 2010;137:66–72. doi: 10.1016/j.ajodo.2007.11.036. [DOI] [PubMed] [Google Scholar]
- 17.AlSamak S, Gkantidis N, Bitsanis E, Christou P. Assessment of potential orthodontic mini-implant insertion sites based on anatomical hard tissue parameters: a systematic review. Int J Oral Maxillofac Implants. 2012;27:875–887. [PubMed] [Google Scholar]
- 18.Celenk-Koca T, Erdinc AE, Hazar S, Harris L, English JD, Akyalcin S. Evaluation of miniscrew-supported rapid maxillary expansion in adolescents: a prospective randomized clinical trial. Angle Orthod. 2018;88:702–709. doi: 10.2319/011518-42.1. [DOI] [PMC free article] [PubMed] [Google Scholar]