

Abstract
Objectives
To compare the efficacy of orthodontic tooth movement with three aligner wear protocols: 7 day, 10 day, and 14 day.
Materials and Methods
Eighty patients were randomly allocated into three groups: group A (7-day changes), group B (10-day changes), and group C (14-day changes). The posttreatment scans were compared with the final virtual treatment simulations through digital superimposition. The differences between predicted and actual achieved treatment outcomes were computed in six angular and six linear dimensions. Differences >0.5 mm for linear measurements and >2° for angular measurements were considered clinically relevant.
Results
Within groups, and irrespective of wear protocol, all linear discrepancies in both jaws were deemed clinically insignificant (<0.5 mm) while nearly all angular discrepancies were considered clinically significant (>2.0°). When the three groups were compared, group C (14-day changes) showed significantly greater accuracy in the posterior segment for maxillary intrusion, distal-crown tip and buccal-crown torque, and mandibular intrusion and extrusion. The mean treatment duration in the 7-day aligner change group was nearly half that of the 14-day aligner change group (5 months vs 9 months).
Conclusions
Fourteen-day changes were statistically significantly more accurate in some posterior movements. However, this difference in accuracy did not exceed the threshold for clinical significance (>0.5 mm/>2.0°). Achieving a clinically similar accuracy between the 7-day protocol and 14-day protocol in half the treatment time suggests a 7-day protocol as an acceptable treatment protocol. Clinicians may consider slowing down to a 14-day protocol if challenging posterior movements are desired.
Keywords: Invisalign, Wear protocol, Aligner efficacy, Clear aligner therapy
INTRODUCTION
Clear aligner therapy (CAT) is an accepted mainstay of orthodontic mechanotherapy.1–5 Studies have evaluated the biological,2–4 esthetic,5,6 and psychological7–10 advantages that CAT may provide over conventional preadjusted edgewise appliances. Although CAT is fast gaining popularity among care seekers, there are still unanswered questions regarding the efficacy and efficiency of these appliances. Evidence-based literature on the efficacy of Invisalign (Align Technology, Santa Clara, Calif), and CAT in general, is still in its incipient stages.9,11–14 In 2009, Kravitz et al.15 evaluated the accuracy of anterior tooth movement using Invisalign by comparing the predicted and achieved tooth movement and reported a mean overall accuracy of 41%. A recent follow-up to this study by Haouili et al.16 suggested that the mean accuracy improved to 50% in 2020. In a 2017 retrospective study, Grünheid et al.3 concluded that Invisalign was able to achieve predicted tooth positions with high accuracy in nonextraction cases.
Invisalign aligners are to be worn 20–22 hours per day and to be changed sequentially every 7 days as per current protocols from the manufacturer. Previously, however, the recommended wear schedule was 14 days. In the literature, there is limited evidence to support either wear schedule. Drake et al.17 reported that more orthodontic tooth movement occurred during the first week than during the second week of aligner wear. The reduction in tooth movement seen during the second week was not related to material fatigue.
Only two published clinical trials have investigated optimal aligner wear protocol. Bollen et al.18 compared the effects of material stiffness (soft, hard) and activation time on the patient's ability to complete a prescribed series of aligners. The 2-week activation period almost doubled the likelihood for successful completion of the initial series of aligners compared with 1-week activation. A high Peer Assessment Rating (PAR) score and planned extractions substantially decreased the likelihood that the initial aligner series would be completed. This study tended to support 2-week activation time in patients who did not require premolar extractions. In the second clinical trial, Clements et al.19 measured the effects of material stiffness and activation time on the quality of treatment and dental improvement measured by changes in PAR scores and the irregularity index. The authors concluded that there was no significant difference between 1-week and 2-week aligner change frequency protocols.
The landmark studies of Bollen et al.18 and Clements et al.19 were performed in 2003 and marked the beginning of independent prospective clinical research regarding CAT and Invisalign. Invisalign has continually improved through the development of new aligner materials, modifications of attachments, and staging of tooth movements.16 The exact extent to which new aligner material influences treatment efficacy still requires investigation. According to the company's internal data, an analysis comparing tooth movement predictability in 200 cases showed no difference in predictability or refinement rates between 1- or 2-week aligner changes.
To date, no independent study has evaluated the efficacy of tooth movement with different aligner wear protocols (7 day, 10 day, 14 day). A better understanding of the optimal aligner wear protocol would help both clinicians and patients improve efficiency. Hence, the purpose of this randomized clinical study was to evaluate and compare the efficacy of different orthodontic tooth movements with different aligner wear protocols (7 day, 10 day, 14 day) by comparing the predicted treatment outcome vs actual outcome. The null hypothesis was that there would be no difference in the efficacy of orthodontic tooth movement with aligners changed every 7 days, 10 days, or 14 days.
MATERIALS AND METHODS
Trial Design
The study was a three-arm parallel randomized clinical trial with a balanced allocation ratio (1:1:1). This study was approved by the Institutional Review Board of European University College (Dubai Healthcare City, United Arab Emirates), IRB number EUC-IRB-17.2.12.
Sample
One hundred twenty consecutive patients were assessed for eligibility at a single orthodontic practice in South Riding, Virginia, USA. The orthodontist (Dr Kravitz) who prescribed all ClinCheck (Align Technology Inc, Santa Clara, Calif) treatment plans was highly skilled and experienced (Tier-Level Diamond Plus Provider [formerly Top 1% Elite] with more than 2500 Invisalign cases treated). Prospective participants for the study were informed about the research and treatment protocol and provided informed consent to participate in the study.
Patients were selected based on the following inclusion criteria: malocclusion to be treated with Invisalign aligners (SmartTrack) with a total initial sequence between 17 and 25 aligners, permanent dentition, good oral hygiene, and no extractions. Exclusion criteria included the following: use of auxiliary appliances, oral surgery, and previous orthodontic treatment or dental restorations placed during treatment. A total of 80 treated patients fit the inclusion criteria and were then randomized using the Random function in Excel (Microsoft Office 2019, Seattle, WA) with a 1:1:1 allocation ratio. The participants were randomly assigned to one of the following three groups: group A changed aligners every 7 days; group B changed aligners every 10 days; and group C changed aligners every 14 days. The records of five subjects were not adequate for data collection; hence, a final sample size of 75 was analyzed (Figure 1; Table 1).
Figure 1.
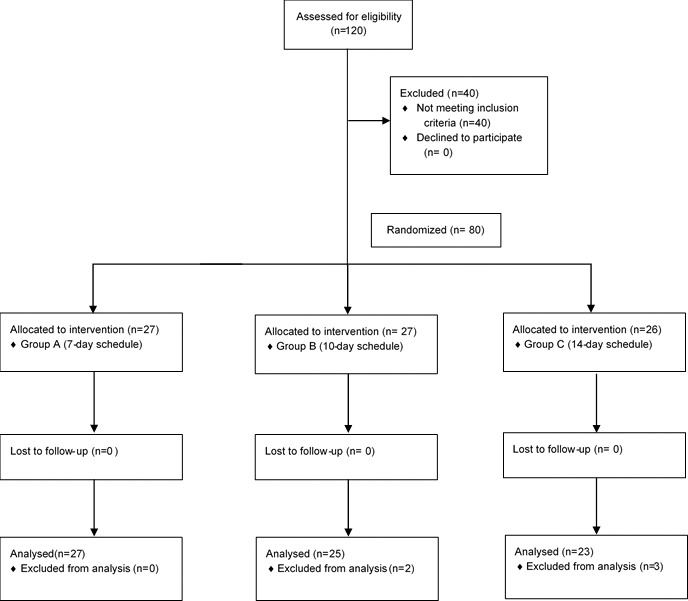
CONSORT flow chart.
Table 1.
Sample Distributiona
| 7 Days (n = 27) |
10 Days (n = 25) |
14 Days (n = 23) |
|
| Demographics | |||
| Age, y | 36.3 | 34.3 | 35.4 |
| Gender (M/F) | 7M/20F | 12M/13F | 11M/12F |
| Angle classification | |||
| Class I | 18 | 15 | 19 |
| Class II | 7 | 8 | 3 |
| Class III | 2 | 2 | 1 |
| No. of aligners | |||
| Maxilla | 21 | 22 | 20 |
| Mandible | 19 | 20 | 20 |
| Mean treatment time, mo | 5 | 8 | 9 |
F indicates female; M, male.
To reduce the risk of bias, the randomization was undertaken by an author who had not examined any of the patients; hence, the treating orthodontist was blinded to the initial allocation. Thereafter, however, blinding was not feasible for the treating doctor due to the nature of treatment. Data collectors and outcome assessors were blinded for analysis.
The stereolithography files of the final stage of each patient's virtual treatment plan were exported through ClinCheck, which represented the predicted tooth movement. The actual outcome was obtained using three-dimensional (3D) intraoral scans (Itero Element, Align Technology, San Jose, Calif) taken at final records. The digital models were deidentified and imported into eModel 9.0 Compare software (GeoDigm Corporation, Falcon Heights, Minn). The software uses a best-fit 3D superimposition algorithm allowing for calculation of differences in linear and angular dimensions for individual tooth positions between the two models. This software has been previously tested for reproducibility20 and has been used in previous studies comparing virtual treatment outcomes to achieved treatment outcomes.3,16,21–24
The virtual treatment plan models exported from ClinCheck Pro were segmented to isolate each tooth as a separate object and compared with the unsegmented intraoral scans. Corresponding dental arches were first aligned globally, and then individual teeth from a segmented model were superimposed on analogous teeth of an unsegmented model using a best-fit algorithm so that differences between tooth positions could be computed. The differences between the positions of each tooth in the two digital models were quantified in the following six dimensions: mesial-distal, buccal-lingual, occlusal-gingival, tip, torque, and rotation (Figure 2). Data from the patient's dentition were organized into four categories: maxillary and mandibular anterior and posterior dentition (posterior dentition included second molars, first molars, second premolars, and first premolars; anterior dentition included canines, lateral incisors, and central incisors).
Figure 2.

Superimposition of digital models to compute differences between predicted and achieved tooth positions. (Left) Global alignment of posttreatment model (white) and final virtual treatment plan model (orange). (Right) Superimposition of individual teeth of final virtual treatment model (green) and posttreatment model (white) using best-fit surface-based registration.
The software used for the superimpositions allowed researchers to detect differences that were too small to be clinically relevant. The threshold values were therefore chosen in reference to the American Board of Orthodontics (ABO) model grading system as described by Grünheid et al.3 According to the ABO, alignment discrepancies of 0.5 mm or greater in marginal ridges and contact points would result in point deductions. Furthermore, a marginal ridge discrepancy of 0.5 mm equated to a crown-tip deviation of 2° for an average-sized molar. Thus, clinically significant discrepancies were set at >0.5 mm for linear movements and >2° for angular movements.
Statistical Analysis
All data were collected and stored in Excel and analyzed using SPSS software (version 15.0.1, IBM, Armonk, NY). Descriptive statistics were computed for the differences between predicted and actual achieved tooth positions in each of the six directions. Interval data were tested for normal intragroup distribution using the Shapiro-Wilk test. Independent t-tests were then used to asses intragroup differences. Intergroup differences were assessed using analysis of variance and the Scheffe post hoc test. P-values <.05 were considered statistically significant.
RESULTS
A comparison of subject demographics suggested homogeneity (P > .05) of the three samples for group age and number of aligners per jaw. Heterogeneity (P < .05) was suggested for gender, Angle classification, and mean treatment time (Table 1).
In the maxillary dentition, group C (14 day) achieved significantly (P < .05) higher accuracy compared with group A (7 day) for posterior intrusion (0.3 mm vs 0.4 mm), distal crown tip (2.8° vs 3.9°) and buccal crown torque (2.8° vs 4.4°) (Table 2). In the mandibular dentition, group C achieved significantly (P < .05) higher accuracy compared with groups A and B for posterior intrusion (0.3 mm vs 0.4 mm) and extrusion (0.2 mm vs 0.3 mm) (Table 2).
Table 2.
Predicted Achieved Differences in the Maxilla and Mandiblea
| Movement |
Posterior |
Anterior |
||||||
| Mean |
ANOVA |
Mean |
ANOVA |
|||||
| 7 Day |
10 Day |
14 Day |
7 Day |
10 Day |
14 Day |
|||
| Maxilla | ||||||||
| Distal | 0.2 | 0.2 | 0.2 | NS | 0.2 | 0.2 | 0.2 | NS |
| Mesial | 0.3 | 0.2 | 0.2 | NS | 0.3 | 0.3 | 0.2 | NS |
| Lingual | 0.4 | 0.4 | 0.4 | NS | 0.2 | 0.2 | 0.2 | NS |
| Buccal | 0.3 | 0.3 | 0.2 | NS | 0.3 | 0.3 | 0.3 | NS |
| Intrusion | 0.4 | 0.4 | 0.3 | P < .05 | 0.3 | 0.3 | 0.4 | NS |
| Extrusion | 0.3 | 0.3 | 0.2 | NS | 0.4 | 0.4 | 0.4 | NS |
| Distal tip | 3.9b | 2.9b | 2.8b | P < .05 | 2.9b | 2.6b | 2.6b | NS |
| Mesial tip | 3.5b | 3.0b | 2.9b | NS | 3.5b | 3.4b | 3.4b | NS |
| Lingual torque | 2.6b | 2.6b | 2.4b | NS | 3.2b | 3.2b | 3.1b | NS |
| Buccal torque | 4.4b | 4.2b | 2.8b | P < .05 | 3.1b | 2.9b | 2.8b | NS |
| Distal rotation | 2.3b | 2.2b | 2.0b | NS | 2.9b | 2.9b | 2.9b | NS |
| Mesial rotation | 2.4b | 2.5b | 1.9 | NS | 3.5b | 3.4b | 3.3b | NS |
| B. Mandible | ||||||||
| Distal | 0.2 | 0.2 | 0.2 | NS | 0.2 | 0.1 | 0.1 | NS |
| Mesial | 0.3 | 0.3 | 0.3 | NS | 0.3 | 0.3 | 0.2 | NS |
| Lingual | 0.2 | 0.3 | 0.3 | NS | 0.2 | 0.2 | 0.2 | NS |
| Buccal | 0.4 | 0.4 | 0.3 | NS | 0.3 | 0.3 | 0.3 | NS |
| Intrusion | 0.4 | 0.4 | 0.3 | P < .05 | 0.3 | 0.2 | 0.2 | NS |
| Extrusion | 0.3 | 0.3 | 0.2 | P < .05 | 0.5 | 0.5 | 0.5 | NS |
| Distal tip | 2.1b | 2.2b | 2.0b | NS | 2.9b | 3.0b | 2.3b | NS |
| Mesial tip | 3.7b | 3.7b | 3.3b | NS | 4.1b | 3.2b | 3.3b | NS |
| Lingual torque | 2.6b | 2.8b | 2.1b | NS | 3.3b | 3.3b | 3.2b | NS |
| Buccal torque | 3.4b | 3.1b | 2.8b | NS | 2.0b | 2.7b | 1.9 | NS |
| Distal rotation | 2.2b | 2.5b | 2.0b | NS | 2.8b | 2.7b | 2.9b | NS |
| Mesial rotation | 3.0b | 3.0b | 2.4b | NS | 3.9b | 3.7b | 2.9b | NS |
ANOVA indicates analysis of variance; NS, not significant.
Clinically significant (>0.5 mm/>2.0°).
Within groups, all linear discrepancies for the posterior and anterior segments in both the maxillary and mandibular arches for all three groups were clinically insignificant (<0.5 mm). In contrast, all discrepancies for angular movements in both arches were clinically significant (>2°) except for two variables in group C: mesial rotation (1.9°) in the maxillary posterior segment and buccal crown torque (1.9°) of the mandibular anterior segment (Table 2).
DISCUSSION
In this prospective trial, the three groups (7-day, 10-day, and 14-day wear) were homogeneous for age and number of aligners. Heterogeneity (P < .05) was suggested for gender, Angle classification, and mean treatment duration. It should be noted that the amount of interproximal reduction performed or number of attachments used was decided on a patient-to-patient basis, although each arch averaged approximately six attachments and <1 mm of interproximal reduction. The mean treatment duration required to finish the initial set of aligners in the 7-day group (5 months) was, as expected—almost half compared with the 14-day group (9 months). This result was significant in lieu of the findings in this study showing no clinically relevant differences in accuracy of tooth movement among the three groups.
Within the groups, there were no clinically significant linear discrepancies between achieved and predicted tooth positions (>0.5 mm). In contrast, all angular movement discrepancies for all three groups were >2° and therefore considered clinically significant (Table 2). Hence, even with 14-day changes, clinicians must consider overcorrections to achieve the desired angular movements. These results agree somewhat with those of Simon et al.,14 who found that molar distalization, a linear movement, was predictable. Incisor torque and premolar rotations, on the other hand, were more challenging and less accurate. Although both Grünheid et al.3 and Charalampakis et al.4 found mandibular incisor intrusion to be an inaccurate movement (contrary to the findings in this study), Grünheid et al.3 also found molar torque as well as mandibular lateral incisor, canine, and first premolar rotations to be inaccurate, while Charalampakis et al.4 found maxillary canine, mandibular premolar, and canine rotations; again, all angular movements, to be most inaccurate. These findings may have been due to the flexibility of the aligner material, combined with the nonrigid nature of the aligner to tooth-surface contact, precluding torsion and tipping control. Attempting overcorrection in the digital predictions, incorporation of composite attachment designs and additional refinement aligners are possible solutions for this (Table 2).
When the differences between predicted and achieved tooth movements were compared among 7-day, 10-day, and 14-day aligner changes, there were no statistically significant differences for all linear and angular movement in the anterior segments in both arches (P > .05). With regard to the posterior segment, however, group C (14-day change) was statistically more accurate for intrusion, distal-crown tip, and buccal-crown torque in the maxillary arch as well as intrusion and extrusion movements in the mandibular arch. Although these differences were not clinically significant, the trend supported greater accuracy in the 14-day protocol, as previously found by Bollen et al.18 This could be due to the larger root surface areas of molars that require greater control for linear and angular tooth movements.25 It seemed that aligners using the same material stiffness in both anterior and posterior segments would have greater difficulty delivering loads suitable in the posterior segments.
With the use of mathematical superimposition of digital models, it has become feasible to quantify treatment changes and, as in the present study, to determine differences between virtual treatment simulations and actual treatment outcomes. The software used in this study (eModel 9.0 Compare software) was able to quantify differences between objects with respect to six degrees of freedom. The software calculated differences automatically, without being influenced by potential operator bias. However, this method measured only intra-arch discrepancies and did not measure interarch relationships, such as overbite, overjet, and occlusal contacts.
The findings in this study seemed to suggest that a 7-day protocol was generally sufficient as there was no clinically significant difference compared with a 10-day or 14-day protocol. A 7-day protocol did, however, significantly reduce treatment duration. It could be suggested that, for those cases requiring complex movement of posterior teeth, a 14-day change of aligners may be beneficial. In the near future, personalized aligner change protocols may be used to enhance aligner efficiency.26,27
Limitations
A limitation of 3D superimposition was the lack of stable anatomic structures on the predicted models, as stereolithography files exported from ClinCheck contained only the clinical crowns and virtual gingiva. In addition, the ClinCheck plan was simply a visual representation of force systems, rather than a true prediction of final tooth position; hence, the predicted tooth position may not have actually been the one desired.16 Patient compliance and inaccuracies from the clinician during attachment placement and interproximal reduction may also have affected tooth movement. This study also relied on the clinical decisions made by one (albeit experienced) orthodontic provider and may not be externally valid for all orthodontists, who vary in their preferences for tooth-movement sequencing, attachment design, and extent of overcorrections. Finally, the patients in this sample had an initial number of aligners between 17 and 25 and short treatment durations, thus indicating relatively simple treatments. The results may have differed if more difficult cases, with more challenging tooth movements, were included.
CONCLUSIONS
Within groups, all linear discrepancies demonstrated clinically insignificant differences (<0.5 mm). In contrast, nearly all angular discrepancies were clinically significant (>2.0°).
The 14-day wear protocol showed statistically greater accuracy for some posterior tooth movements: maxillary intrusion, distal-crown tip, and buccal-crown torque as well as mandibular intrusion and extrusion. None of them exceeded the clinically significant threshold (>0.5 mm or >2°).
Achieving a clinically similar accuracy between the 7-day protocol and 14-day protocol in half the treatment time suggests that a 7-day protocol is an acceptable treatment protocol.
However, if challenging posterior tooth movements or angular movements (ie, torque, tip, and rotation) are required, the 14-day protocol should be considered.
REFERENCES
- 1.Vaid NR. Lets talk ALIGNers. APOS Trends Orthod. 2016;6:177–178. doi: 10.4103/2321-1407.186428. [DOI] [Google Scholar]
- 2.Gu J, Tang JS, Skulski B, et al. Evaluation of Invisalign treatment effectiveness and efficiency compared with conventional fixed appliances using the Peer Assessment Rating index. Am J Orthod Dentofac Orthop. 2017;151:259–266. doi: 10.1016/j.ajodo.2016.06.041. [DOI] [PubMed] [Google Scholar]
- 3.Grünheid T, Loh C, Larson BE. How accurate is Invisalign in nonextraction cases? Are predicted tooth positions achieved? Angle Orthod. 2017;87:809–815. doi: 10.2319/022717-147.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Charalampakis O, Iliadi A, Ueno H, Oliver DR, Kim KB. Accuracy of clear aligners: a retrospective study of patients who needed refinement. Am J Orthod Dentofac Orthop. 2018;154:47–54. doi: 10.1016/j.ajodo.2017.11.028. [DOI] [PubMed] [Google Scholar]
- 5.Tindera M. Bracing for competition? Cheaper challengers enter Invisalign's $1.5 billion market. Forbes. 2018 Published. https://www.forbes.com/sites/michelatindera/2018/05/02/bracing-for-competition-cheaper-challengers-enter-invisaligns-1-5-billion-market/#1fb9cbf92392 Accessed January 15, 2020.
- 6.Melkos AB. Advances in digital technology and orthodontics: a reference to the Invisalign® method. Med Sci Monit. 2005;11:39–42. [PubMed] [Google Scholar]
- 7.Morton J, Derakhshan M, Kaza S, Li C. Design of the Invisalign system performance. Semin Orthod. 2017;23:3–11. doi: 10.1053/j.sodo.2016.10.001. [DOI] [Google Scholar]
- 8.Papadimitriou A, Mousoulea S, Gkantidis N, Kloukos D. Clinical effectiveness of Invisalign® orthodontic treatment: a systematic review. Prog Orthod. 2018;19:37. doi: 10.1186/s40510-018-0235-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Robertson L, Kaur H, Fagundes NCF, Romanyk D, Major P, Flores Mir C. Effectiveness of clear aligner therapy for orthodontic treatment: a systematic review. Orthod Craniofacial Res. 2020;23:133–142. doi: 10.1111/ocr.12353. [DOI] [PubMed] [Google Scholar]
- 10.Papageorgiou SN, Koletsi D, Iliadi A, Peltomaki T, Eliades T. Treatment outcome with orthodontic aligners and fixed appliances: a systematic review with meta-analyses. Eur J Orthod. Published online. 2019:1–13. doi: 10.1093/ejo/cjz094. [DOI] [PubMed]
- 11.Rossini G, Parrini S, Castroflorio T, Deregibus A, Debernardi CL. Efficacy of clear aligners in controlling orthodontic tooth movement: a systematic review. Angle Orthod. 2015;85:881–889. doi: 10.2319/061614-436.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Dasy H, Dasy A, Asatrian G, Rózsa N, Lee HF, Kwak JH. Effects of variable attachment shapes and aligner material on aligner retention. Angle Orthod. 2015;85:934–940. doi: 10.2319/091014-637.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kravitz ND, Kusnoto B, Agran B, Viana G. Influence of attachments and interproximal reduction on the accuracy of canine rotation with invisalign. Angle Orthod. 2008;78:682–687. doi: 10.2319/0003-3219(2008)078[0682:IOAAIR]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 14.Simon M, Keilig L, Schwarze J, Jung BA, Bourauel C. Treatment outcome and efficacy of an aligner technique—regarding incisor torque, premolar derotation and molar distalization. BMC Oral Health. 2014;14:1–7. doi: 10.1186/1472-6831-14-68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kravitz ND, Kusnoto B, BeGole E, Obrez A, Agran B. How well does Invisalign work? A prospective clinical study evaluating the efficacy of tooth movement with Invisalign. Am J Orthod Dentofac Orthop. 2009;135:27–35. doi: 10.1016/j.ajodo.2007.05.018. [DOI] [PubMed] [Google Scholar]
- 16.Haouili N, Kravitz ND, Vaid NR, Ferguson DJ, Makki L. Has Invisalign improved? A prospective follow-up study on the efficacy of tooth movement with Invisalign. Am J Orthod Dentofac Orthop Published online. 2020:1–6. doi: 10.1016/j.ajodo.2019.12.015. [DOI] [PubMed] [Google Scholar]
- 17.Drake CT, McGorray SP, Dolce C, Nair M, Wheeler TT. Orthodontic tooth movement with Clear Aligners. ISRN Dent. 2012;2012:1–7. doi: 10.5402/2012/657973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bollen AM, Huang G, King G, Hujoel P, Ma T. Activation time and material stiffness of sequential removable orthodontic appliances. Part 1: ability to complete treatment. Am J Orthod Dentofac Orthop. 2003;124:496–501. doi: 10.1067/S0889-5406(03)00576-6. [DOI] [PubMed] [Google Scholar]
- 19.Clements KM, Bollen AM, Huang G, King G, Hujoel P, Ma T. Activation time and material stiffness of sequential removable orthodontic appliances. Part 2: dental improvements. Am J Orthod Dentofac Orthop. 2003;124:502–508. doi: 10.1067/j.ajodo.2003.08.001. [DOI] [PubMed] [Google Scholar]
- 20.Grauer D, Cevidanes LH, Tyndall D, Styner MA, Flood PM, Proffit WR. Registration of orthodontic digital models. Craniofacial Growth Ser. 2011;48:377–391. http://www.ncbi.nlm.nih.gov/pubmed/26549917%0Ahttp://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=PMC4636130. [PMC free article] [PubMed] [Google Scholar]
- 21.Brown MW, Koroluk L, Ko CC, Zhang K, Chen M, Nguyen T. Effectiveness and efficiency of a CAD/CAM orthodontic bracket system. Am J Orthod Dentofac Orthop. 2015;148:1067–1074. doi: 10.1016/j.ajodo.2015.07.029. [DOI] [PubMed] [Google Scholar]
- 22.Grauer D, Proffit WR. Accuracy in tooth positioning with a fully customized lingual orthodontic appliance. Am J Orthod Dentofac Orthop. 2011;140:433–443. doi: 10.1016/j.ajodo.2011.01.020. [DOI] [PubMed] [Google Scholar]
- 23.Larson BE, Vaubel CJ, Grünheid T. Effectiveness of computer-assisted orthodontic treatment technology to achieve predicted outcomes. Angle Orthod. 2013;83:557–562. doi: 10.2319/080612-635.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Awad MG, Ellouze S, Ashley S, Vaid N, Makki L, Ferguson DJ. Accuracy of digital predictions with CAD/CAM labial and lingual appliances: a retrospective cohort study. Semin Orthod. 2018;24:393–406. doi: 10.1053/j.sodo.2018.10.004. [DOI] [Google Scholar]
- 25.Djeu G, Shelton C, Maganzini A. Outcome assessment of Invisalign and traditional orthodontic treatment compared with the American Board of Orthodontics objective grading system. Am J Orthod Dentofac Orthop. 2005;128:292–298. doi: 10.1016/j.ajodo.2005.06.002. [DOI] [PubMed] [Google Scholar]
- 26.Hansa I, Semaan SJ, Vaid NR. Clinical outcomes and patient perspectives of Dental Monitoring® GoLive® with Invisalign®—a retrospective cohort study. Prog Orthod. 2020;21 doi: 10.1186/s40510-020-00316-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Hansa I, Semaan SJ, Vaid NR, Ferguson DJ. Remote monitoring and “tele-orthodontics”: concept, scope and applications. Semin Orthod. 2018;24:470–481. doi: 10.1053/j.sodo.2018.10.011. [DOI] [Google Scholar]