

Abstract
Objectives
To compare the efficacy of traditional and digital communication strategies in improving compliance with fixed orthodontic therapy and to investigate the effect of gender, baseline oral hygiene habits, socioeconomics, and parents' education on orthodontic compliance.
Materials and Methods
Orthodontic patients were randomly allocated to three groups. Group 1 received traditional communication including verbal and written instructions, whereas group 2 and group 3 received, in addition to traditional communication, weekly text messages or e-mails with audiovisual links, respectively. Baseline demographics (age, gender, baseline oral hygiene habits, socioeconomics, and parents' education) as well as compliance indicators (treatment duration, failed appointments, incidence and total number of appliance breakages) were recorded. For statistical analysis, Pearson chi-square, independent t-test, and one-way analysis of variance were used (P < .05).
Results
Of 120 patients (aged 12 to 18 years) recruited, 108 completed the trial (G1 = 37, G2 = 35, G3 = 36). Weekly text messages failed to improve patient compliance. On the other hand, sending weekly e-mails with audiovisual links significantly (P = .014) reduced the incidence of appliance breakage as compared with the control group. Females had a significantly lower incidence of breakage (P = .041) and a fewer total number of breakages (P = .021). Patients from households with high income had significantly better compliance (P < .05). A higher level of parents' education was significantly associated with a lower incidence and total number of breakages (P < .01).
Conclusions
Communication with patients using link-rich e-mails and reminders could improve patient compliance with fixed orthodontic treatment. Female patients, high household income, and high parent education are associated with better compliance with fixed orthodontic treatment.
Keywords: Adherence, Compliance, Sociodemographic, Communication, RCT
INTRODUCTION
The most widely accepted definition for compliance is that by Haynes et al.,1 who stated that compliance is “the extent to which a person's behavior coincides with medical or health advice.” Other terms such as adherence or therapeutic alliance are sometimes used, because many authors believe the term compliance has an authoritarian overtone.2
Compliance in orthodontics relates to keeping appointments, following oral hygiene instructions, wearing elastics and other patient-dependent appliances, and avoiding hard sticky food that might debond the brackets and other parts of the appliance.2 Patient compliance in orthodontics is crucial for successful treatment outcomes. When patients fail to follow instructions, the treatment time will increase, and eventually the treatment results will be compromised.3
Adolescents make up the majority of orthodontic patients. It is important for health care professionals to be aware that their interpersonal communication skills and recognition of the uniqueness of this age group play a vital role in optimizing health care outcomes.4 There is no doubt that the Internet and communication technologies have had a considerable impact on the everyday life of young people. Accordingly, more adolescents have access to social media, which will inevitably influence their education and sources of information.
Previous studies attempted to predict the factors that might affect compliance during orthodontic treatment. Patient-related factors such as desire for treatment and relationship with parents were considered important factors motivating patients to comply.5,6 Verbal praise and communication were rated as important methods for improving compliance.7 On the other hand, pain and inconvenience associated with fixed orthodontic appliances were inversely correlated with compliance.8
The main aim of this randomized clinical trial was to study the effect of different methods of communication on the level of patient compliance. The second aim was to investigate the effect of baseline demographics on compliance with fixed orthodontic treatment. The null hypotheses were as follows:
Weekly text messages or weekly e-mails with audiovisual links have no effect on compliance with fixed orthodontic therapy as compared with the standard communication method.
Factors such as gender, baseline oral hygiene habits, household income, residency, school attended, and parents' education have no effect on patient compliance during fixed orthodontic treatment.
MATERIALS AND METHODS
This was a single-center randomized controlled trial. The study protocol and ethical approval were reviewed, accepted, and registered by the review board of the research committee, Faculty of Dentistry and University Hospital, University of Jordan (IRB No. 610/2013/10).
For a power of .90 and an alpha level of .05, we calculated that 29 subjects were needed in each group that was compared to detect a mean difference of 2 and a standard deviation of 3 for the different compliance indicators (ie, treatment duration in months, failed appointments, incidence of breakage, total numbers of breakages).9
The study sample included patients aged 12 to 18 years who attended the Orthodontic Department of Jordan University Hospital and were scheduled to start dual-arch multibracket orthodontic therapy. Patients with significant medical history, severe skeletal discrepancies, craniofacial syndromes and clefts, or previous history of fixed orthodontic treatment were excluded. In addition, patients with a malocclusion that required multiple stages of treatment or different appliances were excluded as well.
A computer-generated blocked-random table was used to randomize the participants, who satisfied the inclusion criteria and provided informed consent, into one of three groups in a block of 40. These three groups were G1 (the control group), G2 (the message group), and G3 (the e-mail group). Patients who were assigned to G3 and reported not having access to the Internet or not having an e-mail account were excluded from the study and were not relocated to other groups. In addition, patients with a sibling already enrolled in the study were not recruited.
Participants in all groups received verbal and written information and instructions regarding their fixed orthodontic treatment (conventional method of communication) by the first author. Participants in G2, in addition to the conventional method of communication, received weekly messages to remind them about these instructions. Participants in G3 received weekly e-mails with links to videos or photo-rich text to remind them about the instructions. The weekly messages and e-mails were sent by the clinic coordinator, and the list of participants was updated weekly.
All participants were required to complete a questionnaire before the start of the treatment. The questionnaire was constructed to record data on a number of factors as follows:
Age: recorded as a numerical value.
Gender: male or female
Brushing teeth: yes or no answer; if yes, there were three options: (1) once a day, (2) twice a day, and (3) three or more times a day.
Household income: based on life expenses and average salaries, this value was classified into low, medium, and high income10,11
Residency: (1) west area of the capital city, which is occupied by people with better socioeconomic conditions; (2) east area of the capital city; and (3) other provinces10,11
School attended: this could reflect the socioeconomic level of the patient and was classified into public or private school
Parents' education: (1) school level, (2) college level, and (3) postgraduate level
All patients were treated using the same fixed orthodontic appliances (stainless steel 0.022-inch MBT bracket system) by the first author who remained blinded to group allocations. As a standard practice for all patients under treatment by the first author, they were reviewed every 6 to 8 weeks, and comprehensive clinical notes were recorded at every visit. Therefore, the clinician was blinded to those recruited in the trial since the same records were kept for all patients. On the last working day of every month, the clinic coordinator retrieved the clinical notes for those who were enrolled in the trial and completed their treatment to record a number of variables that indicated orthodontic compliance. These variables were as follows:
Treatment duration: numerical value measured in months
Number of appointments the patient failed to attend
Number of appointments with reported appliance breakage (incidence of breakage)
Total numbers of breakage (broken brackets and/or bands)
Collected data were analyzed using SPSS version 23.0 (IBM Corp, Armonk, NY, 2015). To test the sociodemographic variables between the three communication groups, one-way analysis of variance (ANOVA) was used for age, while Pearson chi-square test was used for gender, residency, and household income. The variables reflecting the level of patient compliance were tested using independent-sample t-tests to compare two groups: gender (male, female), school attended (public, private), brushing prior to the start of treatment (yes, no). On the other hand, one-way ANOVA and post hoc tests were used when three groups were compared: communication (conventional, message, e-mail), residency (west, east, outside the capital), household income (low, medium, high), parents' level of education (high school, college, postgraduate), and frequency of tooth brushing before the start of the treatment (once, twice, three or more times a day). The level of significance was set at P < .05.
RESULTS
The participants were recruited between November 2013 and November 2017. Of the 120 consecutive patients who satisfied the inclusion/exclusion criteria, 108 patients completed the trial. Five patients moved to other provinces, and 7 patients declined to proceed with the treatment (Figure 1). Overall, there were 73 females (67.6%) and 35 males (32.4%), with an age range of 12 to 18 years (mean age = 14.8 years, SD = 1.67). Sociodemographic characteristics of the study sample are shown in Figure 2.
Figure 1.
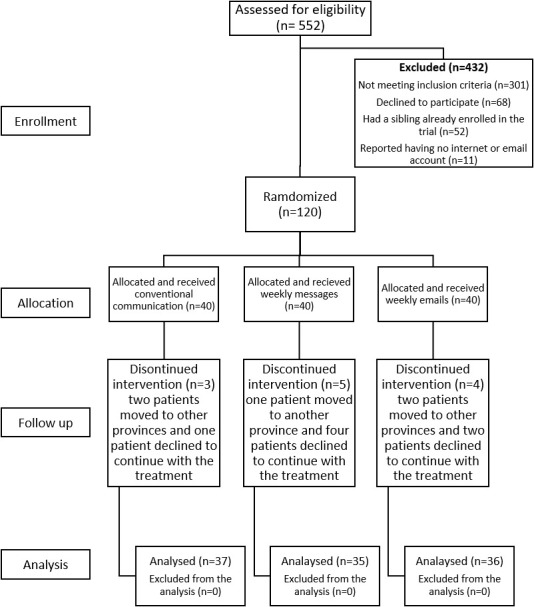
CONSORT flow chart showing patient flow during the trial.
Figure 2.

Sociodemographic characteristics of the study sample (N = 108).
Comparison Based on Methods of Communication
The number of participants in each communication group was G1 = 37, G2 = 35, and G3 = 36. The baseline demographics (age, gender, residency, household income) for the participants based on the communication groups are shown in Table 1.
Table 1.
Three Communication Groups by Age, Gender, Residency, and Household Income
| Variable |
G1, n = 37 |
G2, n = 35 |
G3, n = 36 |
P Value |
| Age, mean ± SD | 14.78 ± 1.75 | 14.51 ± 1.74 | 14.97 ± 1.52 | .514a |
| Gender | ||||
| Male, n = 35 (32.4%) | 12 (32.4%) | 11 (31.4%) | 12 (33.3%) | .985b |
| Female, n = 73 (67.6%) | 25 (67.6%) | 24 (68.6%) | 24 (66.7%) | |
| Residency | ||||
| West of the capital city, n = 48 (44.4%) | 13 (35.1%) | 16 (45.7%) | 19 (52.8%) | .414b |
| East of the capital city, n = 36 (33.3%) | 16 (43.2%) | 12 (34.3%) | 8 (22.2%) | |
| Outside the capital, n = 24 (22.2%) | 8 (21.6%) | 7 (20%) | 9 (25%) | |
| Household income | ||||
| Low, n = 33 (30.6%) | 12 (32.4%) | 13 (34.3%) | 8 (22.2%) | .097b |
| Medium, n = 57 (52.8%) | 23 (62.6%) | 16 (45.7%) | 18 (50%) | |
| High, n = 18 (16.7%) | 2 (5.4%) | 6 (17.1%) | 10 (27.8%) | |
ANOVA P value.
Pearson chi-square test.
Overall, there were no statistically significant differences between the communication groups (G1, G2, G3) at the outset with respect to age, gender, residency, and household income. The results showed a pattern of reduction in the treatment duration and total numbers of breakage from G1 to G3, but the reduction was not statistically significant, with P values of .141 and .226, respectively. The number of failed appointments on average was 1.39, with no significant differences between the groups (P = .405). The incidence of breakage between the groups showed a significant difference (P = .016), for which G1 had a significantly higher incidence of breakage compared with G3 (Table 2).
Table 2.
Three Communication Groups by Variables Indicating Compliance With Fixed Orthodontic Treatmenta
| Variables Indicating Orthodontic Compliance |
G1 (M ± SD) |
G2 (M ± SD) |
G3 (M ± SD) |
One-Way ANOVA P Value |
Groups Compared |
Mean Difference |
P Value |
95% Confidence Interval |
|
| Lower Bound |
Upper Bound |
||||||||
| Treatment duration (mo) | 24.45 ± 6.0 | 22.18 ± 7.4 | 21.27 ± 7.6 | .14 | G1 vs G2 | 2.27 | .43 | −1.74 | 6.23 |
| G1 vs G3 | 3.19 | .15 | −0.79 | 7.12 | |||||
| G2 vs G3 | 0.92 | .93 | −3.12 | 4.95 | |||||
| Number of failed appointments | 1.30 ± 1.87 | 1.71 ± 1.98 | 1.17 ± 1.46 | .41 | G1 vs G2 | −0.42 | .69 | −1.44 | 0.60 |
| G1 vs G3 | 0.13 | .99 | −0.88 | 1.14 | |||||
| G2 vs G3 | 0.55 | .48 | −0.48 | 1.57 | |||||
| Incidence of breakage | 2.92 ± 1.28 | 2.86 ± 2.33 | 1.92 ± 1.65 | .016* | G1 vs G2 | 0.06 | .99 | −1.01 | 1.14 |
| G1 vs G3 | 1.00 | .014* | 0.17 | 1.83 | |||||
| G2 vs G3 | 0.94 | .13 | −0.21 | 2.09 | |||||
| Total numbers of breakage | 4.92 ± 3.03 | 4.34 ± 4.02 | 3.47 ± 3.65 | .23 | G1 vs G2 | 0.58 | .87 | −1.47 | 2.62 |
| G1 vs G3 | 1.45 | .24 | −0.59 | 3.48 | |||||
| G2 vs G3 | 0.87 | .67 | −1.19 | 2.93 | |||||
One-way ANOVA and post hoc tests.
Significant results.
Comparison Based on Gender, Baseline Oral Hygiene Habits, and Sociodemographic Variables
The results of the comparison of the treatment compliance indicators based on gender, baseline oral hygiene habits, and sociodemographic variables are shown in Tables 3 and 4. Independent-sample t-test showed a significant difference between males and females for the incidence of breakage (P = .041) and total numbers of broken brackets (P = .021), in which females had significantly better compliance. In addition, the results suggested that the seven patients who reported not brushing their teeth at the beginning of the study had significantly greater numbers of broken brackets as compared with the rest of the patients (P = .004). However, how often the patient brushed his or her teeth did not have any significant effect on the compliance indicators.
Table 3.
Significance of Difference Between Categories of Compliance Variables (Consisting of Two Groups) and Treatment Compliance Indicators Using Independent-Sample t-Test
| Variable |
Orthodontic Compliance Indicators |
|||
| Treatment Duration (M ± SD) |
Failed Appointments (M ± SD) |
Incidence of Breakage (M ± SD) |
Total Number of Breakages (M ± SD) |
|
| Gender | ||||
| Male (n = 35) | 22.08 ± 6.68 | 1.49 ± 2.02 | 3.09 ± 1.92 | 5.40 ± 4.10 |
| Female (n = 73) | 22.92 ± 7.28 | 1.34 ± 1.67 | 2.32 ± 1.76 | 3.70 ± 3.22 |
| t-test P value | .56 | .70 | .041* | .021* |
| Mean difference | −0.85 | 0.14 | 0.77 | 1.70 |
| 95% confidence interval | −3.74 to 2.04 | −0.59 to 0.87 | 0.034 to 1.51 | 0.27 to 3.14 |
| Tooth brushing | ||||
| Yes (n = 101) | 22.77 ± 7.07 | 1.37 ± 1.82 | 2.48 ± 1.78 | 3.99 ± 3.38 |
| No (n = 7) | 20.91 ± 7.49 | 1.71 ± 1.25 | 3.86 ± 2.34 | 8.00 ± 4.80 |
| t-test P value | .503 | .620 | .054 | .004* |
| Mean difference | 1.86 | −0.35 | −1.38 | −4.01 |
| 95% confidence interval | −3.63 to 7.36 | −1.73 to 1.04 | −2.79 to 0.02 | −6.70 to −1.32 |
| School | ||||
| Public (n = 68) | 23.49 ± 6.98 | 1.37 ± 1.76 | 2.60 ± 1.80 | 4.31 ± 3.53 |
| Private (n = 40) | 21.24 ± 7.10 | 1.43 ± 1.84 | 2.50 ± 1.92 | 4.15 ± 3.75 |
| t-test P value | .11 | .87 | .78 | .83 |
| Mean difference | 2.25 | −0.06 | 0.10 | 0.16 |
| 95% confidence interval | −0.53 to 5.02 | −0.76 to 0.65 | −0.63 to 0.83 | −1.27 to 1.59 |
Statistically significant.
Table 4.
Significance of Difference Between Categories of Compliance Variables Consisting of Three Groups and Treatment Compliance Indicators Using One-Way ANOVA and Post Hoc Tests
| Compliance Variable |
Treatment Compliance Indicators |
Subgroups |
Mean ± SD |
One-Way ANOVA, P Value |
Multiple Comparisons |
||||
| Compared Groups |
Mean Difference |
P Value |
95% Confidence Interval |
||||||
| Lower Bound |
Upper Bound |
||||||||
| Frequency of tooth brushing | Treatment duration | Once (n = 64) | 22.13 ± 6.91 | .453 | Once vs twice | −1.62 | .64 | −5.30 | 2.06 |
| Twice (n = 33) | 23.75 ± 6.98 | Once vs more | −3.08 | .78 | −11.93 | 5.78 | |||
| More (n = 4) | 25.20 ± 10.69 | Twice vs more | −1.45 | .97 | −10.55 | 7.65 | |||
| Failed appointments | Once (n = 64) | 1.28 ± 1.60 | .430 | Once vs twice | −0.11 | .99 | −1.06 | 0.83 | |
| Twice (n = 33) | 1.39 ± 2.11 | Once vs more | −1.22 | .48 | −3.49 | 1.06 | |||
| More (n = 4) | 2.50 ± 2.65 | Twice vs more | −1.11 | .58 | −3.44 | 1.23 | |||
| Incidence of breakage | Once (n = 64) | 2.39 ± 1.73 | .813 | Once vs twice | −0.22 | .92 | −1.15 | 0.72 | |
| Twice (n = 33) | 2.61 ± 1.97 | Once vs more | −0.36 | .97 | −2.60 | 1.88 | |||
| More (n = 4) | 2.75 ± 0.50 | Twice vs more | −0.14 | .998 | −2.44 | 2.16 | |||
| Total numbers of breakage | Once (n = 64) | 3.97 ± 3.35 | .997 | Once vs twice | −0.06 | .996 | −1.90 | 1.78 | |
| Twice (n = 33) | 4.03 ± 3.68 | Once vs more | −0.03 | .998 | −1.59 | 1.53 | |||
| More (n = 4) | 4.00 ± 0.82 | Twice vs more | 0.03 | .999 | −1.87 | 1.93 | |||
| House hold income | Treatment duration | Low (n = 33) | 24.73 ± 6.79 | .031* | Low vs medium | 2.22 | .36 | −1.41 | 5.85 |
| Medium (n = 57) | 22.51 ± 7.23 | Low vs high | 5.39 | .024* | 0.54 | 10.25 | |||
| High (n = 18) | 19.33 ± 5.99 | Medium vs high | 3.17 | .22 | −1.19 | 7.53 | |||
| Failed appointments | Low (n = 33) | 2.24 ± 2.12 | .002** | Low vs medium | 1.12 | .030* | 0.09 | 2.15 | |
| Medium (n = 57) | 1.12 ± 1.62 | Low vs high | 1.58 | .001*** | 0.56 | 2.56 | |||
| High (n = 18) | 0.67 ± 0.84 | Medium vs high | 0.46 | .27 | −0.25 | 1.16 | |||
| Incidence of breakage | Low (n = 33) | 3.30 ± 2.07 | .000**** | Low vs medium | 0.78 | .16 | −0.24 | 1.79 | |
| Medium (n = 57) | 2.53 ± 1.64 | Low vs high | 1.97 | .000**** | 0.83 | 3.11 | |||
| High (n = 18) | 1.33 ± 1.28 | Medium vs high | 1.19 | .008** | 0.28 | 2.10 | |||
| Total numbers of breakage | Low (n = 33) | 5.42 ± 3.85 | .000**** | Low vs medium | 1.06 | .40 | −0.90 | 3.01 | |
| Medium (n = 57) | 4.37 ± 3.50 | Low vs high | 3.70 | .000**** | 1.75 | 5.65 | |||
| High (n = 18) | 1.72 ± 1.90 | Medium vs high | 2.65 | .000**** | 1.09 | 4.20 | |||
| Residency | Treatment duration | West Amman (n = 48) | 21.70 ± 6.87 | .461 | West vs east | −2.00 | .49 | −5.79 | 1.79 |
| East Amman (n = 36) | 23.70 ± 7.12 | West vs outside | −1.30 | .85 | −5.59 | 2.99 | |||
| Outside Amman (n = 24) | 23.00 ± 7.45 | East vs outside | 0.70 | .98 | −3.83 | 5.23 | |||
| Failed appointments | West Amman (n = 48) | 1.27 ± 1.55 | .305 | West vs east | −0.48 | .53 | −1.43 | 0.47 | |
| East Amman (n = 36) | 1.75 ± 2.16 | West vs outside | 0.19 | .97 | −0.89 | 1.27 | |||
| Outside Amman (n = 24) | 1.08 ± 1.56 | East vs outside | 0.67 | .40 | −0.47 | 1.80 | |||
| Incidence of breakage | West Amman (n = 48) | 2.52 ± 1.91 | .476 | West vs east | −0.31 | .83 | −1.30 | 0.67 | |
| East Amman (n = 36) | 2.83 ± 1.83 | West vs outside | 0.27 | .91 | −0.84 | 1.39 | |||
| Outside Amman (n = 24) | 2.25 ± 1.70 | East vs outside | 0.58 | .54 | −0.59 | 1.76 | |||
| Total numbers of breakage | West Amman (n = 48) | 4.13 ± 3.76 | .349 | West vs east | −0.76 | .71 | −2.69 | 1.16 | |
| East Amman (n = 36) | 4.89 ± 3.82 | West vs outside | 0.58 | .89 | −1.60 | 2.76 | |||
| Outside Amman (n = 24) | 3.54 ± 2.80 | East vs outside | 1.35 | .40 | −0.95 | 3.64 | |||
| Education of mother | Treatment duration | School (n = 29) | 24.00 ± 7.81 | .384 | School vs college | 1.68 | .63 | −2.09 | 5.44 |
| College (n = 73) | 22.32 ± 6.98 | School vs postgrad | 3.80 | .55 | −3.90 | 11.50 | |||
| Postgrad (n = 6) | 20.20 ± 2.98 | College vs postgrad | 2.12 | .86 | −5.16 | 9.41 | |||
| Failed appointments | School (n = 29) | 1.52 ± 1.77 | .441 | School vs college | 0.11 | .99 | −0.84 | 1.06 | |
| College (n = 73) | 1.41 ± 1.84 | School vs postgrad | 1.02 | .50 | −0.92 | 2.96 | |||
| Postgrad (n = 6) | 0.50 ± 0.84 | College vs postgrad | 0.91 | .55 | −0.93 | 2.75 | |||
| Incidence of breakage | School (n = 29) | 2.69 ± 1.44 | .081 | School vs college | 0.09 | .97 | −0.77 | 0.94 | |
| College (n = 73) | 2.60 ± 2.01 | School vs postgrad | 1.19 | .10 | −0.21 | 2.59 | |||
| Postgrad (n = 6) | 1.50 ± 1.05 | College vs postgrad | 1.10 | .12 | −0.28 | 2.48 | |||
| Total numbers of breakage | School (n = 29) | 4.76 ± 3.20 | .005** | School vs college | 0.51 | .77 | −1.27 | 2.30 | |
| College (n = 73) | 4.25 ± 3.81 | School vs postgrad | 2.93 | .008** | 0.75 | 5.10 | |||
| Postgrad (n = 6) | 1.83 ± 1.47 | College vs postgrad | 2.41 | .31 | −1.27 | 6.09 | |||
| Education of father | Treatment duration | School (n = 13) | 22.99 ± 5.47 | .156 | School vs college | −0.50 | .99 | −5.65 | 4.65 |
| College (n = 68) | 23.49 ± 7.41 | School vs postgrad | 2.58 | .62 | −3.16 | 8.33 | |||
| Postgrad (n = 27) | 20.40 ± 6.59 | College vs postgrad | 3.09 | .16 | −0.78 | 6.96 | |||
| Failed appointments | School (n = 13) | 0.92 ± 1.19 | .600 | School vs college | −0.55 | .68 | −1.86 | 0.77 | |
| College (n = 68) | 1.47 ± 1.87 | School vs postgrad | −0.48 | .81 | −1.95 | 0.98 | |||
| Postgrad (n = 27) | 1.41 ± 1.80 | College vs postgrad | 0.063 | .998 | −0.92 | 1.05 | |||
| Incidence of breakage | School (n = 13) | 3.15 ± 1.95 | .005** | School vs college | 0.32 | .91 | −0.98 | 1.61 | |
| College (n = 68) | 2.84 ± 1.86 | School vs postgrad | 1.56 | .03* | 0.12 | 3.00 | |||
| Postgrad (n = 27) | 1.59 ± 1.37 | College vs postgrad | 1.25 | .007** | 0.27 | 2.22 | |||
| Total numbers of breakage | School (n = 13) | 6.00 ± 4.04 | .008** | School vs college | 1.43 | .44 | −1.12 | 3.97 | |
| College (n = 68) | 4.57 ± 3.48 | School vs postgrad | 3.41 | .013* | 0.57 | 6.25 | |||
| Postgrad (n = 27) | 2.59 ± 3.13 | College vs postgrad | 1.98 | .04* | 0.07 | 3.89 | |||
P = .05; ** P = .01; *** P = .001; **** P = .0001.
The low household income group had a significantly longer treatment time and a greater incidence of failing appointments, incidence of breakage, and total number of breakages compared with the high household income group. Similarly, the low household income group had a significantly greater incidence of failure of appointments compared with the medium household income group. In addition, the medium household income group had a significantly greater incidence of breakage and higher total numbers of broken brackets as compared with the high household income group. Finally, neither residency nor school attended made any difference in the compliance indicators.
One-way ANOVA was used to compare means (treatment duration, number of failed appointments, breakage incidence, and total breakage) between different groups classified based on parents' education. Results showed that patients who had a mother with an education level of postgraduate degree had significantly a lower total number of breakages as compared with the other two groups (Table 4). Likewise, patients whose fathers had an education level of postgraduate degree had a significantly lower incidence of appliance breakage and lower total number of breakages as compared with the other two groups.
DISCUSSION
Comparison Based on Methods of Communication
The results (Table 1) showed no baseline differences between the three communication groups based on age, gender, residency, and household income. The results showed that patients who received weekly e-mails (G3) had a lower incidence of appliance breakage as compared with G1 and G2 (P = .016). A few studies tested the influence of new technology on orthodontic patient compliance, but only oral hygiene was considered as the output measure.12,13 One of these studies used WhatsApp and concluded that this app significantly improved patient compliance with the oral hygiene protocol. Other researchers investigating orthodontic compliance used different methods than the current study; nevertheless, they proved that methods aiming to enhance communication with the patient usually had a positive influence on patient compliance. Wright et al.,14 who tested the influence of supplementing conventional verbal instructions with written information, found that this reduced the number of missed appointments and the incidence of breakage but not to a significant level. Furthermore, improving patient communication using postal reminders15 or computer-generated telephone reminders16 proved to significantly reduce the rate of failed appointments in orthodontic practice. The use of regular messages was proved efficient on improving patient compliance and adherence to treatment in many chronic diseases (such as diabetes mellitus, chronic hypertension, smoking, obesity, bulimia nervosa),17,18 and the current study found that weekly messages mildly improved patient compliance but not to a significant level. In agreement with the current results, Patel et al.19 showed that computer-based visual information was a significantly better method than a written leaflet for information retention.
Comparison Based on Gender, Baseline Oral Hygiene Habit, and Sociodemographic Variables
It seems that information reported on gender and its effect on orthodontic compliance was controversial.8 The present study found that females had better compliance than males, with a significantly lower incidence as well as total number of breakages. Current findings were similar to those reported by Bukhari et al.,20 who carried out a retrospective self-reported study and found that females were more likely to attend appointments than males were (P = .038). Other studies based on questionnaires21 or a behavior modification reward system3 found that gender was not significantly related to orthodontic compliance.
The present study found that the seven patients who did not practice any oral hygiene habits before treatment initiation had significantly poorer compliance with a higher incidence of breakage and a greater total number of broken brackets/bands. Only one study was identified that investigated the relationship between baseline oral hygiene habits and orthodontic compliance,20 and in agreement with the current findings, the study reported that patients who brushed and flossed daily had better compliance in attending orthodontic appointments. On the other hand, the current study found that, among patients who used to brush their teeth prior to treatment initiation, the frequency of brushing had no influence on the degree of their compliance during treatment.
When the socioeconomic effect on patient compliance was analyzed by studying categories of residency, school attended, and household income, only household income showed a significant effect on orthodontic compliance. In previous studies, it was suggested that patients belonging to higher socioeconomic groups were usually more aware of the attractiveness of their smile and its influence on social and occupation success and therefore were more likely to develop better treatment compliance.22 This finding was further confirmed by the results of Bukhari et al.,20 who reported that non-Medicaid patients complied with attendance more consistently than Medicaid patients did (P = .022). On the other hand, other studies found that patients from middle and lower socioeconomic groups may develop better compliance.22,23 In contrast with the current results, Mandall et al.24 found that neither gender nor socioeconomic status were associated with orthodontic compliance, which was represented by completion of the treatment, incidence of breakage, and number of failed/canceled appointments. Although this was a prospective multicenter longitudinal study, an unusually high percentage of 43% of the initial sample did not complete the treatment. In addition, and unlike the current study design, patients as young as 10 years of age were included, and different appliances such as headgear, functional, removable, and fixed appliances were used; this increased the number of covariables, making it difficult to compare to the current findings.
In the current study, the effect of the level of parents' education on their child's compliance during fixed orthodontic treatment was investigated, and a significant effect was found. As parents' education background increased, patient compliance was significantly enhanced, as represented by a lower incidence of breakage and a lower number of broken brackets/bands. The level of parents' education was reported to have an effect on demand for orthodontic treatment for their children because of the awareness of the importance of oral function and esthetics.6 Nevertheless, this factor and its effect on orthodontic compliance was not previously investigated.
The strength of this study was its design as a prospective randomized controlled trial with 90% power to detect actual differences between groups. In addition, the digital method for weekly reminders used in this study for which the greatest effect was shown was the weekly audiovisual-rich e-mail method. This is a simple method, available to most of the patients with hardly any cost to the practice. Nevertheless, the present study had some limitations. There were factors identified in the study that significantly affected fixed orthodontic compliance that were impossible for practitioners to alter: for example, household income, gender of the patient, and parents' education. Therefore, these factors could be used to predict the level of compliance but not to improve it. Furthermore, the trial was carried out in one center. Therefore, the generalizability of the results could be limited, and future multicenter randomized trials could be more informative.
CONCLUSIONS
The most relevant finding of this investigation was that supplementing written and verbal information with weekly audiovisual reminders through e-mail could overcome the problem of limited retention of information in orthodontic practice and enhance patient compliance with a lower incidence of fixed appliance breakage.
In addition, the results of this study identified gender, household income, and parents' level of education as significant factors affecting compliance with fixed orthodontic treatment.
ACKNOWLEDGMENTS
This study was funded by the Deanship of Academic Research, The University of Jordan. Sincere appreciation to Ms S. Daamseh for her help in sending the weekly reminders. We also wish to show gratitude to Dr I. Al-Omari and Dr Z. Al-Bitar for their valuable ideas and suggestions.
REFERENCES
- 1.Haynes RB, Taylor DW, Sackett DL. Compliance in Health Care. Baltimore, Md: Johns Hopkins University Press; 1979. [Google Scholar]
- 2.Aljabaa A, McDonald F, Newton JT. A systematic review of randomized controlled trials of interventions to improve adherence among orthodontic patients aged 12 to 18. Angle Orthod. 2015;85:305–313. doi: 10.2319/031214-184.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Richter DD, Nanda RS, Sinha PK, Smith DW, Currier GF. Effect of behavior modification on patient compliance in orthodontics. Angle Orthod. 1998;68:123–132. doi: 10.1043/0003-3219(1998)068<0123:EOBMOP>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 4.Kim B, White K. How can health professionals enhance interpersonal communication with adolescents and young adults to improve health care outcomes? Systematic literature review. Int J Adolesc Youth. 2018;23:198–218. [Google Scholar]
- 5.Mehra T, Nanda RS, Sinha PK. Orthodontists' assessment and management of patient compliance. Angle Orthod. 1998;68:115–122. doi: 10.1043/0003-3219(1998)068<0115:OAAMOP>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 6.Tuncer C, Canigur Bavbek N, Balos Tuncer B, Ayhan Bani A, Çelik B. How do patients and parents decide for orthodontic treatment–effects of malocclusion, personal expectations, education and media. J Clin Pediatr Dent. 2015;39:392–399. doi: 10.17796/1053-4628-39.4.392. [DOI] [PubMed] [Google Scholar]
- 7.Lin F, Sun H, Ni Z, Zheng M, Yao L. A feasible method to improve adherence of Hawley retainer in adolescent orthodontic patients: a randomized controlled trial. J Patient Prefer Adherence. 2015;9:1525. doi: 10.2147/PPA.S94111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Egolf RJ, BeGole EA, Upshaw HS. Factors associated with orthodontic patient compliance with intraoral elastic and headgear wear. Am J Orthod Dentofacial Orthop. 1990;97:336–348. doi: 10.1016/0889-5406(90)70106-M. [DOI] [PubMed] [Google Scholar]
- 9.Noordzij M, Tripepi G, Dekker FW, Zoccali C, Tanck MW, Jager KJ. Sample size calculations: basic principles and common pitfalls. Nephrol Dial Transplant. 2010;25:1388–1393. doi: 10.1093/ndt/gfp732. [DOI] [PubMed] [Google Scholar]
- 10.Stud Fam Plann. Vol. 41. Department of Statistics and Macro International Inc; Calverton, Maryland, USA: 2010. Jordan 2007: results from the population and family health survey; pp. 61–66. [DOI] [PubMed] [Google Scholar]
- 11.Shahateet MI. How serious regional economic inequality in Jordan? Evidence from two national household surveys. J Am Appl Sci. 2006;3:1735–1744. [Google Scholar]
- 12.Eppright M, Shroff B, Best AM, Barcoma E, Lindauer SJ. Influence of active reminders on oral hygiene compliance in orthodontic patients. Angle Orthod. 2014;84:208–213. doi: 10.2319/062813-481.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Zotti F, Dalessandri D, Salgarello S, et al. Usefulness of an app in improving oral hygiene compliance in adolescent orthodontic patients. Angle Orthod. 2016;86:101–107. doi: 10.2319/010915-19.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wright NS, Fleming PS, Sharma PK, Battagel J. Influence of supplemental written information on adolescent anxiety, motivation and compliance in early orthodontic treatment. Angle Orthod. 2010;80:329–335. doi: 10.2319/042809-138.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Can S, MacFarlane T, O'Brien K. The use of postal reminders to reduce non-attendance at an orthodontic clinic: a randomised controlled trial. Br Dent J. 2003;195:199–201. doi: 10.1038/sj.bdj.4810443. [DOI] [PubMed] [Google Scholar]
- 16.Roth JP, Kula TJ, Jr, Glaros A, Kula K. Effect of a computer-generated telephone reminder system on appointment attendance. Semin Orthod. 2004;10:190–193. [Google Scholar]
- 17.Hussein WI, Hasan K, Jaradat AA. Effectiveness of mobile phone short message service on diabetes mellitus management; the SMS-DM study. Diabetes Res Clin Pract. 2011;94:e24–e26. doi: 10.1016/j.diabres.2011.07.025. [DOI] [PubMed] [Google Scholar]
- 18.Fjeldsoe BS, Marshall AL, Miller YD. Behavior change interventions delivered by mobile telephone short-message service. Am J Prev Med. 2009;36:165–173. doi: 10.1016/j.amepre.2008.09.040. [DOI] [PubMed] [Google Scholar]
- 19.Patel JH, Moles DR, Cunningham SJ. Factors affecting information retention in orthodontic patients. Am J Orthod Dentofacial Orthop. 2008;133:S61–S67. doi: 10.1016/j.ajodo.2007.07.019. [DOI] [PubMed] [Google Scholar]
- 20.Bukhari OM, Sohrabi K, Tavares M. Factors affecting patients' adherence to orthodontic appointments. Am J Orthod Dentofacial Orthop. 2016;149:319–324. doi: 10.1016/j.ajodo.2015.07.040. [DOI] [PubMed] [Google Scholar]
- 21.Nanda RS, Kierl MJ. Prediction of cooperation in orthodontic treatment. Am J Orthod Dentofacial Orthop. 1992;102:15–21. doi: 10.1016/0889-5406(92)70010-8. [DOI] [PubMed] [Google Scholar]
- 22.Sergl HG, Zentner A. Predicting patient compliance in orthodontic treatment. Semin Orthod. 2000;6:231–236. [Google Scholar]
- 23.Starnbach Hk, Kaplan A. Profile of an excellent orthodontic patient. Angle Orthod. 1975;45:141–145. doi: 10.1043/0003-3219(1975)045<0141:POAEOP>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 24.Mandall N, Matthew S, Fox D, Wright J, Conboy F, O'Brien K. Prediction of compliance and completion of orthodontic treatment: are quality of life measures important? Eur J Orthod. 2008;30:40–45. doi: 10.1093/ejo/cjm077. [DOI] [PubMed] [Google Scholar]