

Abstract
Elevated blood pressure is associated with an increased risk of cardiovascular illness and death. Efforts to reduce that risk have led to recommendations for a wide array of nondrug and drug therapies. Choosing the optimal first-line drug for hypertensive patients should address a hierarchy of treatment goals: decrease in morbidity and mortality associated with hypertension, decrease in blood pressure and other surrogate markers, good tolerance, dosing convenience and low cost. This article examines the evidence for angiotensin-converting-enzyme (ACE) inhibitors as a class of first-line antihypertensive drugs in light of these treatment goals. Overall, the evidence does not support the use of ACE inhibitors as first-line drugs in the management of most patients with hypertension, although they have proven benefit as second-line drugs for the treatment of congestive heart failure and left ventricular dysfunction secondary to myocardial infarction.
Published evidence indicates that low-dose thiazides are the drugs of first choice in managing hypertension.1 Evidence for &beta%-blockers as first-line agents is weak; however, there is substantial evidence of their effectiveness in hypertension as second-line agents.2 Beyond these 2 classes of drugs, the evidence for long-term health benefits is less well established. In this article I summarize the evidence for the use of angiotensin-converting-enzyme (ACE) inhibitors as first-line drugs in the management of elevated blood pressure. Captopril was the first available orally active ACE inhibitor. Many others in the class followed, and their utilization worldwide has steadily increased since their introduction in the early 1980s.
What is an ACE inhibitor?
ACE inhibitors modulate the activity of the renin angiotensin system, which has an important role in regulating blood pressure. The renin angiotensin system increases blood pressure by producing angiotensin II, which has 2 main systemic actions: it is a potent vasoconstrictor of resistance vessels, and it stimulates the adrenal cortex to release aldosterone, which increases blood pressure by increasing retention of sodium and water by the kidney. The ACE inhibitors diminish the activity of the renin angiotensin system by competitively inhibiting the enzyme responsible for converting inactive angiotensin I to active angiotensin II.
What is the evidence that ACE inhibitors reduce cardiovascular morbidity and mortality?
There are no long-term randomized trials measuring health outcomes in which ACE inhibitors used as first-line agents in the management of hypertension have been compared with placebo or an untreated control. In a meta-analysis of the outcome evidence for treating hypertension,3 none of the 17 randomized controlled trials comparing active treatment with untreated control used an ACE inhibitor as a first- or second-line drug. However, in one recently published trial,4 in which nitrendipine was the first-line drug, the ACE inhibitor enalapril was the second-line drug.
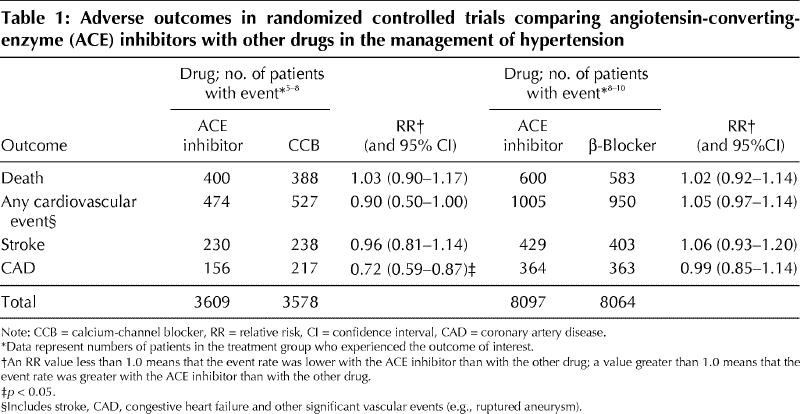
ACE inhibitors have been used as first-line agents in 6 head-to-head randomized controlled trials comparing ACE inhibitors with other antihypertensive therapies (Table 1).5,6,7,8,9,10 Four of these trials compared an ACE inhibitor with a calcium-channel blocker (CCB).5,6,7,8 These 4 trials were pooled in a meta-analysis (using Cochrane Review Manager 3.1), which showed that the ACE inhibitors were associated with significantly fewer cases of coronary artery disease than were the CCBs. Of these 4 trials, the 2 smaller ones6,7 involved patients with hypertension and type 2 diabetes; in the larger trials5,8 more than 89% of patients did not have diabetes. In the fourth and fifth of the head-to-head trials,8,9 which involved hypertensive patients mostly without diabetes, the ACE inhibitor was compared with a &beta%-blocker or a thiazide (or both). The sixth head-to-head trial10 compared captopril with a &beta%-blocker in type 2 diabetic patients with hypertension. If these last 3 trials are considered as comparisons between ACE inhibitors and &beta%-blockers, their results can be combined and compared with those of the trials comparing ACE inhibitors with CCBs (Table 1). Whereas ACE inhibitors yielded better outcomes than CCBs in terms of coronary artery disease events, patients taking ACE inhibitors fared similarly to those taking &beta%-blockers in terms of all 4 adverse-outcome categories.
Table 1
Congestive heart failure is a common complication of hypertension, so evidence related to its treatment is relevant to many hypertensive patients. A recent meta-analysis11 examined the evidence from 32 trials in which 7 different ACE inhibitors were compared with controls in the management of congestive heart failure. The meta-analysis demonstrated that the ACE inhibitors yielded a highly significant benefit in terms of reducing both total mortality and the combined outcome of mortality or admission to hospital for congestive heart failure (attributable risk reduction 10.2%, number needed to treat 10 for about 3 months). In most of these trials the patients were receiving diuretics (29 of the 32 trials) and digoxin (26 of the 32 trials) at baseline, and the ACE inhibitor or placebo was added to the treatment regimen.
There are 4 randomized controlled trials from a recent systematic review12 in which 4 different ACE inhibitors administered for 1.5 to 50 months were compared with placebo for patients with recent myocardial infarction; the selection criteria were left ventricular dysfunction, symptoms of congestive heart failure or anterior myocardial infarction, and no thrombolytic treatment. In each of these trials total mortality rate and rate of admission to hospital were significantly lower with the ACE inhibitor than with placebo. These trials do not provide evidence of the benefit of ACE inhibitors alone, as more than half of the patients were receiving other drugs (including diuretics, &beta%-blockers or CCBs) when they were assigned to the ACE inhibitor or placebo group.
Renal disease is also commonly associated with hypertension, as either a cause or a consequence of the condition. Meta-analyses have shown that ACE inhibitors are effective in preserving renal function in both diabetic13 and nondiabetic14 proteinuric nephropathy (more than 3 g/d). For diabetic patients the data are consistent with the suggestion that ACE inhibitors have an overall benefit that is greater than their effect in reducing blood pressure. However, in the UK Prospective Diabetes Study10 there was no difference between the &beta%-blocker and the ACE inhibitor in terms of blood pressure reduction, renal function or proteinuria. In a meta-analysis of nondiabetic nephropathy14 the ACE inhibitors were associated with a lower risk of end-stage renal disease than were other antihypertensive agents, but they were also associated with a greater decline in blood pressure. At present it is impossible to be sure whether the beneficial effect of ACE inhibition is due to the decline in blood pressure or to other effects.
In summary, ACE inhibitors are effective in reducing morbidity and mortality in 2 clinical settings commonly associated with hypertension: congestive heart failure and renal disease. The bulk of the evidence for their effectiveness in these settings comes from their use as second-line agents.
How efficacious are ACE inhibitors in reducing blood pressure and other surrogate markers?
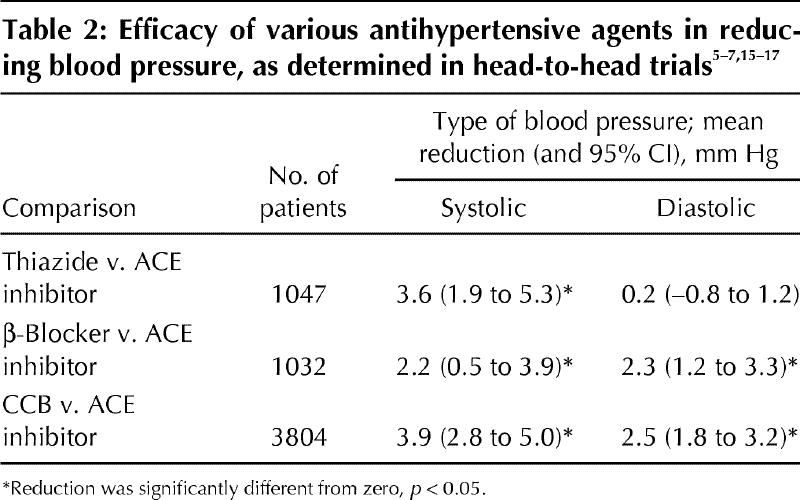
No meta-analysis has been published on the efficacy of ACE inhibitors in reducing blood pressure relative to that of other drug classes. Three randomized controlled trials15,16,17 were specifically designed to measure the antihypertensive efficacy of single-drug therapy for mild hypertension. By pooling the results from these trials, it is possible to compare ACE inhibitors with the other drug classes (Table 2). Table 2 also includes blood pressure data from 3 of the outcome trials5,6,7 comparing ACE inhibitors with CCBs. ACE inhibitors as single agents appear to be significantly less efficacious in reducing blood pressure than the other drug classes.
Table 2
A recent meta-analysis18 of 50 trials showed the following mean percent reductions (and 95% confidence intervals) in another surrogate marker, left ventricular mass index, in patients receiving various classes of antihypertensive drugs: ACE inhibitors, 12% reduction (9.0% to 14.5%); CCBs, 11% reduction (7.8% to 13.7%); diuretics, 8% reduction (3.9% to 11.1%); and &beta%-blockers, 5% reduction (1.2% to 7.3%). In this meta-analysis, &beta%-blockers were significantly less effective than ACE inhibitors and CCBs (p <% 0.05), but there were no other significant differences between drug classes.
A meta-analysis19 of 41 trials measuring protein excretion demonstrated a greater reduction in proteinuria with ACE inhibitors than with other antihypertensive drugs, despite similar reductions in blood pressure in these trials.
Do ACE inhibitors and other antihypertensive drugs differ in tolerability?
In the 3 comparative trials designed to assess this question15,16,17 patients receiving ACE inhibitors did not fare significantly worse or better than those receiving other classes of drugs in terms of withdrawal due to adverse effects or measures of quality of life. The most frequent problematic adverse effect with ACE inhibitors is a dry cough, which occurs in approximately 10% of patients; in half of these patients the cough is intolerable and necessitates discontinuation of therapy.20 Cough is a class effect, occurring with all ACE inhibitors, and there are no clear differences between the various drugs in terms of prevalence or severity of the effect.
Do ACE inhibitors have advantages in terms of convenience or cost?
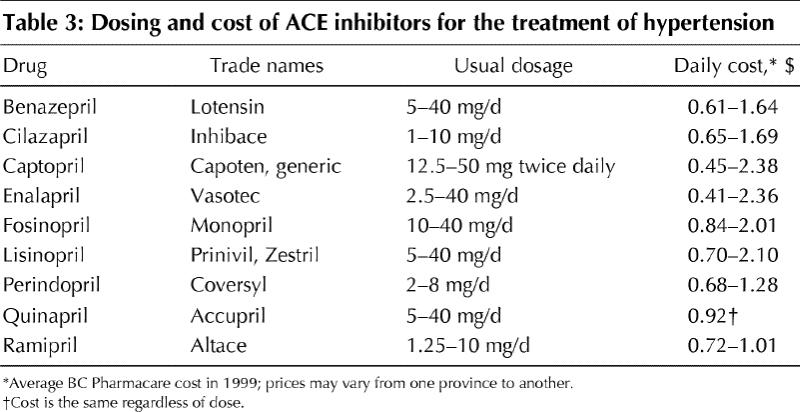
Many of the ACE inhibitors reduce blood pressure for 24 hours and are recommended to be given once daily (Table 3). This effect is similar to that of other classes for which once-daily preparations have a convenience advantage. The mean daily cost of ACE inhibitors in Canada (Table 3) is about 100 times higher than that of hydrochlorothiazide (for which the cost is 0.3 to 0.6 cents/d1).
Table 3
In which patients with elevated blood pressure is an ACE inhibitor the drug of first choice?
On the basis of the outcome evidence, there are only 2 types of patients with elevated blood pressure in whom an ACE inhibitor should be considered the drug of first choice: patients who have had myocardial infarction leading to left ventricular dysfunction in whom a &beta%-blocker is contraindicated and a diuretic is not needed, and patients with diabetic or nondiabetic nephropathy. In other settings in which an ACE inhibitor is indicated, such as hypertension with congestive heart failure, the evidence for its effectiveness is based on the drug being added to optimal diuretic therapy as a second-line agent. In all other hypertensive patients a thiazide should be considered first,1 and &beta%-blockers should be considered second.2 These 2 drug classes have a beneficial effect on morbidity and mortality that is equal to or better than that of ACE inhibitors (Table 1), they reduce blood pressure to a greater extent than ACE inhibitors (Table 2), and they cost less than ACE inhibitors1,2 (Table 3). On the basis of the significantly better head-to-head outcome evidence from randomized controlled trials comparing ACE inhibitors with CCBs, ACE inhibitors are preferable to CCBs as first-line drugs.
Are there any clinically significant differences between the different ACE inhibitors?
There are very few randomized controlled trials comparing one ACE inhibitor with another, and none of these comparative trials have measured health outcomes. Most of the small comparative trials have not shown any clinically significant differences between the various ACE inhibitors.
Conclusion
Overall, the evidence in light of the hierarchy of treatment goals does not support the use of ACE inhibitors as first-line drugs in the management of most patients with elevated blood pressure. However, there is substantial evidence for the benefit of this class of drugs when given as second-line therapy in the management of patients with congestive heart failure and left ventricular dysfunction secondary to myocardial infarction. In patients with diabetic and nondiabetic proteinuric nephropathy and elevated blood pressure, an ACE inhibitor may be appropriate as the drug of first choice. Additional randomized controlled trials measuring health outcomes are required to establish whether ACE inhibitors have any clear advantages over thiazides and other classes of drugs in different settings.
Footnotes
This article has been peer reviewed.
Competing interests: None declared.
Reprint requests to: Dr. James M. Wright, Department of Medicine, University Hospital &mdash% UBC Site, 2211 Wesbrook Mall, Vancouver BC V6T 2B5; fax 604 822-0701; jmwright@interchange.ubc.ca
References
- 1.Wright JM. Choosing a first-line drug in the management of elevated blood pressure: What is the evidence? 1: Thiazide diuretics. CMAJ 2000;163(1):57-60. Available: www.cma.ca/cmaj/vol-163/issue-1/0057.htm [PMC free article] [PubMed]
- 2.Wright JM. Choosing a first-line drug in the management of elevated blood pressure: What is the evidence? 2: b-Blockers. CMAJ 2000;163(2):188-92. Available: www.cma.ca/cmaj/vol-163/issue-2/0188.htm [PMC free article] [PubMed]
- 3.Wright JM, Lee CH, Chambers GK. Systematic review of antihypertensive therapies: Does the evidence assist in choosing a first-line drug? CMAJ 1999;161:25-32. Available: www.cma.ca/cmaj/vol-161/issue-1/0025.htm [PMC free article] [PubMed]
- 4.Staessen JA, Fagard R, Thijs L, Celis H, Arabidze GG, Birkenhager WH, et al. Randomised double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. Systolic Hypertension in Europe (Syst-Eur) Trial Investigators. Lancet 1997;350:757-64. [DOI] [PubMed]
- 5.Study Group on Long-term Antihypertensive Therapy. A 12-month comparison of ACE inhibitor and CA antagonist therapy in mild to moderate essential hypertension &mdash% the GLANT Study. Hypertens Res 1995;18:235-44. [PubMed]
- 6.Estacio RO, Jeffers BW, Hiatt WR, Biggerstaff SL, Gifford N, Schrier RW. The effect of nisoldipine as compared with enalapril on cardiovascular outcomes in patients with non-insulin-dependent diabetes and hypertension. N Engl J Med 1998;338:645-52. [DOI] [PubMed]
- 7.Tatti P, Pahor M, Byington RP, Di Mauro P, Guarisco R, Strollo G, et al. Outcome results of the Fosinopril Versus Amlodipine Cardiovascular Events Randomized Trial (FACET) in patients with hypertension and NIDDM. Diabetes Care 1998;21:597-603. [DOI] [PubMed]
- 8.Hansson L, Lindholm LH, Ekbom T, Dahlof B, Lanke J, Schersten B, et al. Randomised trial of old and new antihypertensive drugs in elderly patients: cardiovascuular mortality and morbidity. The Swedish Trial in Old Patients with Hypertension-2 Study. Lancet 1999;354:1751-6. [DOI] [PubMed]
- 9.Hansson L, Lindholm LH, Niskanen L, Lanke J, Hedner T, Niklason A, et al. Effect of angiotensin-converting-enzyme inhibition compared with conventional therapy on cardiovascular morbidity and mortality in hypertension: the Captopril Prevention Project (CAPPP) randomised trial. Lancet 1999;353: 611-6. [DOI] [PubMed]
- 10.UK Prospective Diabetes Study Group. Efficacy of atenolol and captopril in reducing risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 39. BMJ 1998;317:713-20. [PMC free article] [PubMed]
- 11.Garg R, Yusuf S. Overview of randomized trials of angiotensin-converting enzyme inhibitors on mortality and morbidity in patients with heart failure. JAMA 1995;273:1450-6. [PubMed]
- 12.Mehta RH, Eagle KA. Secondary prevention in acute myocardial infarction. BMJ 1998;316:838-42. [DOI] [PMC free article] [PubMed]
- 13.Kasiske BL, Kalil RS, Ma JZ, Liao M, Keane WF. Effect of antihypertensive therapy on the kidney in patients with diabetes: a meta-regression analysis. Ann Intern Med 1993;118:129-38. [DOI] [PubMed]
- 14.Giatras I, Lau J, Levey AS. Effect of angiotensin-converting enzyme inhibitors on the progression of non-diabetic renal disease: a meta-analysis of randomised trials. Ann Intern Med 1997;127:337-45. [DOI] [PubMed]
- 15.Materson BJ, Reda DJ, Cushman WC, Massie BM, Freis ED, Kochar MS, et al. Single-drug therapy for hypertension in men. A comparison of six antihypertensive agents with placebo. The Department of Veterans Affairs Cooperative Study Group on Antihypertensive Agents. N Engl J Med 1993;328:914-21. [DOI] [PubMed]
- 16.Neaton JD, Grimm RH Jr, Prineas RJ, Stamler J, Grandits GA, Elmer PJ, et al, for the Treatment of Mild Hypertension Study Research Group. Treatment of Mild Hypertension Study. Final results. JAMA 1993;270:713-24. [PubMed]
- 17.Philipp T, Anlauf M, Distler A, Holzgreve H, Michaelis J, Wellek S. Randomised, double blind, multicentre comparison of hydrochlorothiazide, atenolol, nitrendipine, and enalapril in antihypertensive treatment: results of the HANE study. HANE Trial Research Group. BMJ 1997;315:154-9. [DOI] [PMC free article] [PubMed]
- 18.Schmieder RE, Schlaich MP, Klingbeil AU, Martus P. Update on reversal of left ventricular hypertrophy in essential hypertension (a meta-analysis of all randomized double-blind studies until December 1996). Nephrol Dial Transplant 1998;13:564-9. [DOI] [PubMed]
- 19.Gansevoort RT, Sliuter WJ, Jemmelder MH, de Zeeuw D, de Jong PE. Antiproteinuric effect of blood-pressure-lowering agents: a meta-analysis of comparative trials. Nephrol Dial Transplant 1995;10:1963-74. [PubMed]
- 20.Overlack A. ACE inhibitor-induced cough and bronchospasm. Incidence, mechanisms and management. Drug Saf 1996;15:72-8. [DOI] [PubMed]