

Abstract
The characteristics of the optimal cuff for blood pressure (BP) measurement are still the subject of much debate. The choice of the appropriate cuff in obese individuals depends not only on the arm circumference but also on its shape because a conically shaped arm makes it difficult to fit the cuff to the arm. When a large‐size cylindrical cuff is used in conical arms, an overestimation of the true BP is likely to occur with BP discrepancies that may be as large as 10 mm Hg. With the advent of automatic oscillometric devices, the choice of the appropriate cuff became even more controversial because with oscillometric BP measurement the reference point is not the artery occlusion but the oscillometric peak signal. To overcome the problem of miscuffing in obese individuals, special cuffs that can accommodate a wide range of arm sizes have been designed. Using these cuffs, accurate oscillometric BP measurements can be obtained over a wide range of arm circumferences using a unique software algorithm. These wide‐range cuffs coupled to oscillometric devices may represent a good option for BP measurement in very obese subjects. However, their reliability should be confirmed in larger populations and different settings.
Keywords: bladder, blood pressure, cuff, device, measurement, oscillometric
1. INTRODUCTION
In the past, doctors had only one way to evaluate blood pressure (BP) of a patient: the palpation of the radial artery and empirical judgment if the systolic pulse peak was strong or weak. Around the second half of 1800, the idea of applying an inflatable cuff with a mercury manometer allowed more reliable measurements. The current mercury sphygmomanometer method is still very similar to that proposed by Riva‐Rocci in 1896. However, the characteristics of the optimal cuff have been the subject of much debate since the beginning of the 20th century, and many problems remain debated.1, 2 With the advent of automatic oscillometric devices the choice of the appropriate cuff became even more controversial because the oscillometric measurement is generated by a different sequence of events compared to the auscultatory one. In fact, with traditional auscultatory technique, the role of the cuff is to compress the artery under a defined reference pressure, whereas with oscillometric devices, the cuff is at the same time the signal sensor.2 In the auscultatory BP measurement, a complete artery occlusion is necessary as a pre‐requisite for the systolic pressure determination. In the oscillometric method, the reference point is not the artery occlusion, but the oscillometric peak signal.3 Thus, the present recommendations for standard sphygmomanometry do not necessarily apply to BP measurement performed with oscillometric devices since the role of the cuff differs between the auscultatory and the oscillometric method.
2. THE CUFF AND BLADDER
With traditional sphygmomanometry, miscuffing may lead to inaccurate BP measurements, and the use of a cuff and/or a bladder of inappropriate dimensions for the arm circumference is a serious source of error. Use of too narrow or too short bladders (undercuffing) leads to overestimation of BP, and thus to overdiagnosis of hypertension, a problem overlooked by many doctors when measuring BP in obese subjects. Conversely, use of too wide or too long bladders (overcuffing) may lead to BP underestimation, with the possibility of diagnosing hypertensive individuals as being normotensive. However, there is still no consensus about the appropriate size of cuffs and bladders in relation to the upper arm circumference. The British Hypertension Society recommends a standard cuff with a bladder measuring 12 × 26 cm for the majority of adult arms, a large cuff with a bladder measuring 12 × 40 cm for obese arms, and a small cuff with a bladder measuring 12 × 18 cm for lean adult arms and children.4 Thus, the same cuff width is suggested for all types of arms. At variance, the recommendations of the American Heart Association are mainly based on the 40% × 80% rule.5 In other words, the bladder inside the cuff should have at least a 40% width and an 80% length of arm circumference. Thus, 4 different cuffs have been recommended to be used according to the arm size: a small adult cuff with a bladder measuring 10 × 24 cm for arm circumference 22‐26 cm, an adult cuff with a bladder measuring 13 × 30 cm for arm circumference 27‐34 cm, a large adult cuff with a bladder measuring 16 × 38 cm for arm circumference 35‐44 cm, and an adult thigh cuff with a bladder measuring 20 × 42 cm for arm circumference 45‐52 cm. However, an intraarterial study in which multiple indirect measurements were made with the cuff width/arm circumference ratio varying from 30% to 55% demonstrated that the problem is much more complex and that optimum cuff width for the indirect measurement of BP is proportional to the logarithm of the arm's circumference.6 A ratio of 40% resulted in an overestimation of BP for most arms, with particularly high errors for small arms. This overestimation indicates that the choice of the optimal cuff for BP measurement with the auscultatory method remains a clinical dilemma.
3. THE OSCILLOMETRIC BP MEASUREMENT
As stated above, current recommendations for cuff size may not apply to devices based on the oscillometric BP measurement. Indeed, little is known about the relationship between cuff size and performance for oscillometric monitors. This stresses the importance of the varying software‐cuff combinations in the different measurement methods. Complete artery occlusion is not critical when BP is measured with the oscillometric method because oscillations can also be detected beyond the systolic pressure through the knocking of the pulse at the overinflated bladder wall.2 Interesting results on the biomechanical basis of oscillometric BP were provided by Han et al using a computational model of the whole upper arm.7 This study showed that the measured cuff pressure oscillations are a reflection of the entire artery volume change under the cuff thereby presenting a mixture of arterial distension in different closure states during the entire measurement process. One advantage of the oscillometric over the auscultatory measurement was that although the oscillation amplitude was smaller with stiff than with elastic arteries the stiffness variation of the brachial artery did not affect the accuracy of oscillometric BP measurement.7
4. PROBLEMS WITH BP MEASUREMENT IN THE OBESE
As mentioned above, the regular adult cuff size is too short for individuals with an arm circumference of 32 cm or larger and will lead to overestimation of BP.8 Thus, obese subjects often require the use of large‐sized cuffs. According to the AHA recommendations, for arm circumferences ranging from 35 to 44 cm, a bladder measuring 16 cm in width should be used.5 For circumferences from 45 to 52 cm the bladder width should be 20 cm, but in subjects with short upper arm length, a 16 cm wide cuff can be used. However, a large arm often cannot be correctly cuffed especially in obese women with short humerus length. Results from our laboratory showed that arm length was <20 cm in 22% of the subjects referred to our outpatient clinic and was <16 cm in 0.6% of the subjects.9
The choice of the appropriate cuff in obese individuals depends not only on the arm circumference but also on its shape because a conically shaped arm makes it difficult to fit the cuff to the arm, increasing the likelihood of inaccurate BP measurements.10 This problem has not been considered by most investigators and is disregarded by current guidelines. The recent AAMI/ISO/ESH proposals stated that there is a need for further future investigations in this field.11 Yet, the shape of the upper arm is tronco‐conical in virtually all individuals and may vary according to gender, degree of obesity, and arm circumference. According to data from our laboratory, the difference between the proximal and the distal circumferences of the upper arm ranged from 1 to 20 cm, with an average value of 8.7 cm.9 This corresponded to slant angles of the upper arm ranging from 89.2 to 82.4°. In addition, while upper arms of standard size have the shape of a single truncated cone, large‐sized arms represent the sum of 2 truncated cones with different slant angles, which further complicates adequate cuffing by cylindrical cuffs (Figure 1). When a large‐size cylindrical cuff is used in conical arms, the elbow end of the cuff will remain loose and will expand irregularly over the lower part of the arm, causing an overestimation of the true BP. In subjects with an arm circumference of 37.5 to 42.5 cm, we showed that a cylindrical cuff overestimated BP measured by comparison to the tronco‐conical cuff by 2.0/1.8 mm Hg with systolic BP differences as large as 10 mm Hg9 (Figure 2). This measurement error is more than doubled in subjects with morbid obesity and arm circumference of 42 cm or larger (Palatini P., unpublished results). The same problem may be encountered when a wide range cuff is used (see below). Indeed, it has been shown that when a cylindrical wide‐range cuff was used in obese subjects it overestimated systolic BP.12 In contrast, when a tronco‐conical cuff was used in the same subjects BP readings were accurate.
Figure 1.
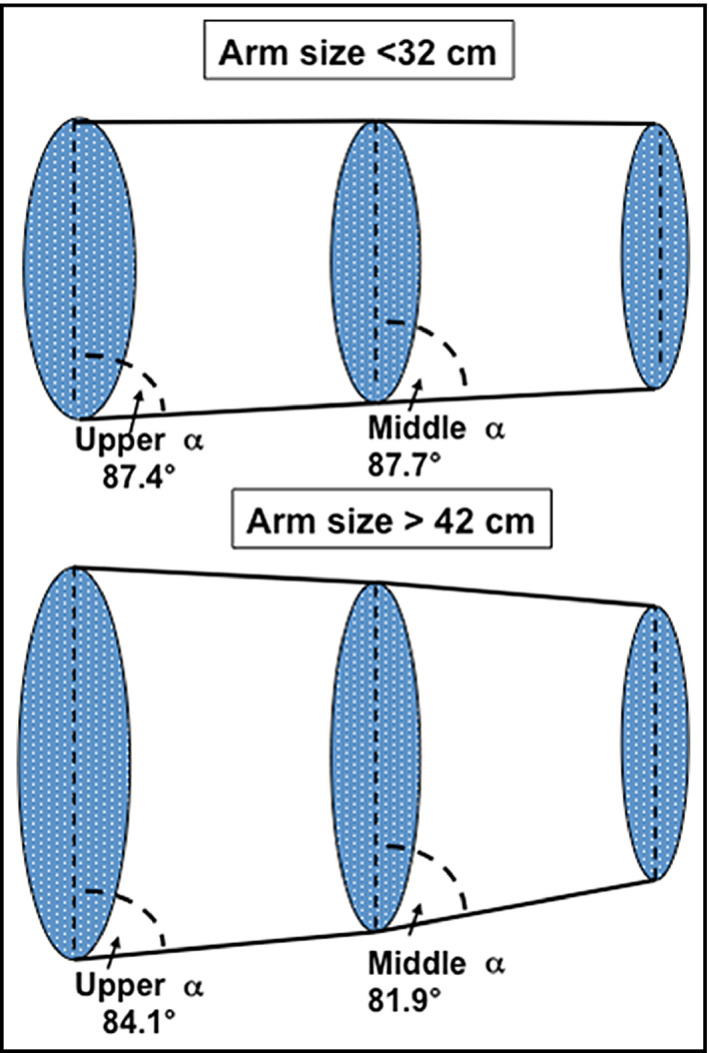
Upper arm shape in 33 subjects with arm circumference <32 cm and 33 subjects with arm circumference >42 cm. The upper arm has been divided into 2 truncated cones. Upper and middle α represents the mean slant angle for the 2 truncated cones in each group. The 2 slant angles are similar in the subjects with smaller arm whereas in the subjects with larger arm the middle slant angle is smaller than the upper angle. Data from Palatini P., unpublished results
Figure 2.
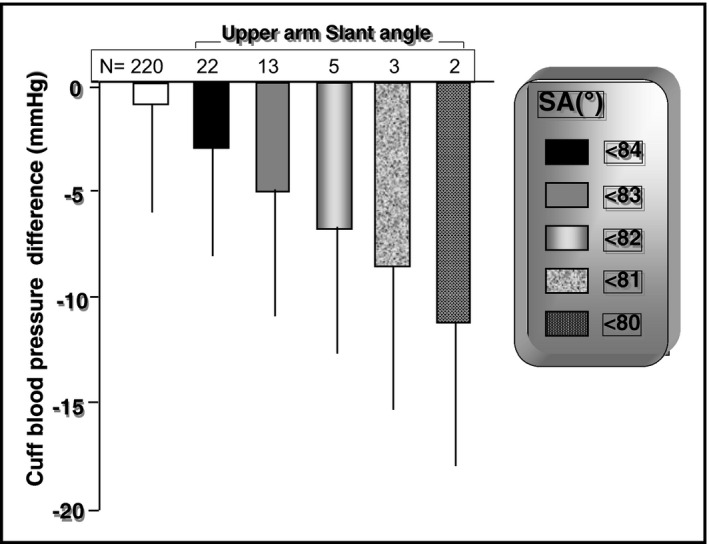
Systolic blood pressure differences between a cylindrical and a tronco‐conical cuff in a group of subjects with middle arm circumference ranging between 37.5 and 42.5 cm. Data are mean ± SEM and are adjusted for age and sex. A negative value indicates that the cylindrical cuff measurement is greater than the tronco‐conical cuff measurement. SA indicates slant angle. Adapted from Palatini et al9
Future studies in larger samples will better define the importance of bladder shape for obtaining accurate measurements in subjects with large upper arms. The use of BP measurement with wrist monitors may be a valid alternative for these subjects, especially if devices coupled to conical cuffs designed for large lower arms are used.13
5. THE WIDE RANGE CUFF
Even when recommendations are strictly followed, often a large arm cannot be correctly cuffed because an extra large cuff cannot fit on a short upper arm.14 To overcome the problem of miscuffing in these individuals, special cuffs that can accommodate a wide range of arm sizes from medium to very large have been produced by some manufacturers. Using these so‐called “wide range cuffs” containing smaller bladder than traditionally recommended, accurate BP measurements can be obtained over a wide range of arm sizes thanks to a special software algorithm.15 The software algorithm adjusts the device parameters based on the characteristics of the individual arm being measured. The correct reference pressure in the cuff is reached through a specific cuff design that can provide stable arterial occlusion and assessment of the oscillometric signal efficiency in the software algorithm through electronic gain adjustment in each measurement. Masiero et al showed that a device coupled to a single cuff with a 14.5 × 32 cm bladder could provide accurate BP readings in subjects with arm circumferences ranging from 32 to 50 cm.16 It should be noted that a tronco‐conical shape should also be adopted for wide‐range cuffs.
6. ARM AND CUFF SIZE IN VALIDATION STUDIES
Despite the important recent technological advances in BP measurement equipment, little attention has been given by scientific societies to the performance of cuffs in obese individuals. To avoid the use of inaccurate BP monitors, several international bodies developed protocols for independent validation of BP‐measurement devices worldwide with the objective of establishing minimum standards of accuracy. Currently, about 400 automatic BP measurement devices have been validated,17 mostly based on the British Hypertension Society guidelines or the International Protocol of the European Society of Hypertension.18 However, 1 limitation of these 2 protocols is that arm size is not included among the criteria used for selecting the subjects recruited for the validation studies. Given the problems outlined above, there is a need for better validation protocols to test the accuracy of BP measuring devices provided with the oscillometric technique. The introduction of wide‐range cuffs that cover a wide range of arm circumferences has made it of paramount importance to test these devices on an adequate number of subjects with large arms. To make sure that these devices are reliable up to the extreme of the declared arm size range, a balanced distribution of arm circumferences should be taken into account. Indeed, the latest AAMI/ISO81060‐2 standard specifies the limb size distribution as follows: For a sphygmomanometer intended for use with a single cuff size, at least 40% of the subjects shall have a limb circumference which lies within the upper half of the specified range of use of the cuff, and at least 40% shall have a limb circumference within the lower half.19 At least 20% of the subjects should have a limb circumference which lies within the upper quarter of the specified range of use of the cuff, and at least 20% should have a limb circumference within the lower quarter. For a sphygmomanometer intended for use with multiple cuff sizes, each cuff size shall be tested on at least 1/(2 × n) of the subjects, where n is the number of cuff sizes. These recommendations have been confirmed by a recent international initiative including AAMI, ESH, and ISO experts who developed a universal standard for device validation.11
7. PERSPECTIVES
The goal of the manufacturer is to provide a cuff with optimal size and shape in relation to the patient's arm. The shape of the cuff is crucial for obtaining reliable BP readings, especially when semi‐rigid cuffs are used; and in subjects with large arms, the shape should be tronco‐conical. However, little is known about the appropriate slant angles that should be adopted for cuffs and bladders in relation to arm sizes. The optimal slant angle should be identified based on several hundred subjects with arm size distributed over a wide range of circumferences. Cylindrical and conical bladders of different size and shape should be constructed and compared in the various arm size classes studying the influence of sex, age, adiposity, arterial stiffness, and BP level. The results obtained with wide‐range cuffs coupled to oscillometric devices look promising and may represent a good option for BP measurement in the very obese. However, the reliability of these cuffs should be confirmed in larger populations and different settings.
CONFLICT OF INTEREST
No author has a conflict of interest with the present results.
Palatini P, Asmar R. Cuff challenges in blood pressure measurement. J Clin Hypertens. 2018;20:1100–1103. 10.1111/jch.13301
REFERENCES
- 1. O'Brien E. A century of confusion: which bladder for accurate blood pressure measurement? [review]. J Hum Hypertens. 1996;10:565‐572. [PubMed] [Google Scholar]
- 2. Palatini P, Frick GN. Cuff and bladder: overlooked components of BP measurement devices in the modern era? Am J Hypertens. 2012;25:136‐138. [DOI] [PubMed] [Google Scholar]
- 3. Geddes LA, Voelz M, Combs C, Reiner D, Babbs CF. Characterization of the oscillometric method for measuring indirect blood pressure. Ann Biomed Eng. 1982;10:271‐280. [DOI] [PubMed] [Google Scholar]
- 4. O'Brien E, Petrie J, Littler WA, De Swiet M, Padfield PD, Dillon MJ. Blood pressure measurement: recommendations of the British Hypertension Society, 3rd edn. London, UK: BMJ Publishing Group; 1997. [Google Scholar]
- 5. Pickering TG, Hall JE, Appel LJ, et al. Recommendations for blood pressure measurement in humans and experimental animals: part 1: blood pressure measurement in humans: a statement for professionals From the Subcommittee of Professional and Public Education of the American Heart Association Council on High Blood Pressure Research. Circulation. 2005;111:697‐716. [DOI] [PubMed] [Google Scholar]
- 6. Marks LA, Groch A. Optimizing cuff width for noninvasive measurement of blood pressure. Blood Press Monit. 2000;5:153‐158. [DOI] [PubMed] [Google Scholar]
- 7. Lan H, Al‐Jumaily AM, Lowe A, Hing W. Effect of tissue mechanical properties on cuff‐based blood pressure measurements. Med Eng Phys. 2011;33:1287‐1292. [DOI] [PubMed] [Google Scholar]
- 8. Palatini P, Parati G. Blood pressure measurement in very obese patients: a challenging problem. J Hypertens. 2011;29:425‐429. [DOI] [PubMed] [Google Scholar]
- 9. Palatini P, Benetti E, Fania C, Malipiero G, Saladini F. Rectangular cuffs may overestimate blood pressure in individuals with large conical arms. J Hypertens. 2012;30:530‐650. [DOI] [PubMed] [Google Scholar]
- 10. Maxwell GF, Pruijt JF, Arntzenius AC. Comparison of the conical cuff and the standard rectangular cuffs. Int J Epidemiol. 1985;14:468‐472. [DOI] [PubMed] [Google Scholar]
- 11. Stergiou GS, Alpert B, Mieke S, et al. A universal standard for the validation of blood pressure measuring devices: Association for the Advancement of Medical Instrumentation/European Society of Hypertension/International Organization for Standardization (AAMI/ESH/ISO) Collaboration Statement. Hypertension. 2018;71:368‐374. [DOI] [PubMed] [Google Scholar]
- 12. Bonso E, Saladini F, Zanier A, Benetti E, Dorigatti F, Palatini P. Accuracy of a single rigid conical cuff with standard‐size bladder coupled to an automatic oscillometric device over a wide range of arm circumferences. Hypertens Res. 2010;33:1186‐1191. [DOI] [PubMed] [Google Scholar]
- 13. Hersh LT, Sesing JC, Luczyk WJ, Friedman BA, Zhou S, Batchelder PB. Validation of a conical cuff on the forearm for estimating radial artery blood pressure. Blood Press Monit. 2014;19:38‐45. [DOI] [PubMed] [Google Scholar]
- 14. O'Brien E. What to do when faced with an unmeasurable ambulatory blood pressure? J Hypertens. 2011;29:451‐453. [DOI] [PubMed] [Google Scholar]
- 15. Stergiou GS, Tzamouranis D, Nasothimiou EG, Protogerou AD. Can an electronic device with a single cuff be accurate in a wide range of arm size? Validation of the Visomat Comfort 20/40 device for home blood pressure monitoring. J Hum Hypertens. 2008;22:796‐800. [DOI] [PubMed] [Google Scholar]
- 16. Masiero S, Saladini F, Benetti E, Palatini P. Accuracy of the Microlife large‐extra large‐sized cuff (32‐52 cm) coupled to an automatic oscillometric device. Blood Press Monit. 2011;16:99‐102. [DOI] [PubMed] [Google Scholar]
- 17. Stergiou GS, Asmar R, Myers M, et al. Improving the accuracy of blood pressure measurement: the influence of the European Society of Hypertension International Protocol (ESH‐IP) for the validation of blood pressure measuring devices and future perspectives. J Hypertens. 2018;36:479‐487. [DOI] [PubMed] [Google Scholar]
- 18. O'Brien E, Atkins N, Stergiou G, Karpettas N, Parati G, Asmar R on behalf of the Working Group on Blood Pressure Monitoring of the European Society of Hypertension . European Society of Hypertension International Protocol revision for the validation of blood pressure measuring devices in adults. Blood Press Monit. 2010;2010:23‐38. [DOI] [PubMed] [Google Scholar]
- 19. Non‐invasive sphygmomanometers Part 2: Clinical investigation of automated measurement type. https://www.iso.org/standard/57977.html. Accessed February 6, 2018.