

Abstract
Measures of arterial stiffness are indicators for cardiovascular health and predictors of cardiovascular events. Arterial stiffness is responsive to acute physiologic stressors such as exercise. However, the acute effects of intensive exercise and recovery on arterial stiffness are controversial. Thirty‐seven healthy middle‐ and long‐distance runners (33 men, mean age 26.5±6.6 years) underwent evaluation of their cardiovascular stiffness at rest, after a 15‐minute warm‐up, immediately after vigorous running 3 km at the pace of their 10‐km personal best, and finally 30 minutes after terminating their workout. Peripheral and central systolic blood pressure, as well as augmentation index and pulse wave velocity (PWV), increased during exercise in comparison to baseline (P<.001, general linear model). Thirty minutes after terminating the workout, a drop in peripheral blood pressure (P<.001), central blood pressure (P<.001), and PWV (P=.001) below baseline was observed. Therefore, the authors found that exercise of either moderate or vigorous intensity causes a temporary increase in arterial stiffness in middle‐ and long‐distance runners.
Arterial compliance is the important ability of the cardiovascular tree to expand and recoil in response to cardiac load, allowing a steady and laminar blood flow.1 Impaired arterial compliance measured as increased central blood pressure (BP), augmentation index (AIx), or pulse wave velocity (PWV) is associated with the presence of cardiovascular risk factors and atherosclerotic disease. Those parameters of arterial stiffness have been identified as cardiovascular risk factors and currently serve as predictors for cardiovascular endpoints.2, 3
The fact that exercise has beneficial effects on the cardiovascular system and leads to a short‐term reduction in peripheral BP after acute exercise is also well‐known.4, 5 However, the effect of acute and chronic exercise on arterial stiffness remains controversial. Increase in arterial stiffness is reported after intensive strength training.1, 6 It remains uncertain whether resistance exercise that alters regional muscles can affect peripheral and central BP as well.7 Moreover, the influence of acute aerobic exercise is controversial.8, 9 In addition, in endurance‐trained individuals, there are inconsistent findings regarding the effects of intermittent or constant aerobic exercise on arterial stiffness.10 Laurent and colleagues11 report on higher central systolic BP and aortic stiffness in aerobically trained individuals, which is in contrast to several other studies12 that have shown beneficial effect. Moreover, there also seem to be racial differences regarding the response of arterial compliance to exercise13 as well as differences in hypertensive and normotensive patients.14
In a recent study, Nieman and colleagues15 evaluated the acute influence of a 2‐hour run on the arterial stiffness of trained runners and found no decrease in arterial stiffness parameters after exercise in an entirely male population. Therefore, this study evaluated the acute effect of a vigorous 3000‐m run on arterial stiffness in healthy middle‐ and long‐distance runners.
Patients and Methods
Study Patients
Cardiovascular stiffness was tested in 37 healthy middle‐ and long‐distance runners at rest (33 men, mean age 26.5±6.6 years). Characteristics of the study participants are displayed in Table 1. All of the participants were apparently healthy and free from acute or chronic diseases. However, four participants exhibited a systolic BP >140 mm Hg at rest after repeat measurements. In those cases, the lowest value was included into statistical analyses.
Table 1.
Study Participants
| Mean±Standard Deviation | |
|---|---|
| Women/men | 4/33 |
| Age, y | 26.5±6.6 |
| Body height, cm | 179.9±7.1 |
| Body weight, kg | 66.3±6.5 |
| Body mass index, m2/kg | 20.5±1.2 |
| Years of training | 10.5±7.4 |
| 10‐km season best, min | 33:20±2:55 |
A second measurement was performed directly after a 15‐minute aerobic warm‐up and a third measurement was taken directly after a vigorous 3000‐m run.
The pace for the 3000 m of intensive running was set equal to the individual 10‐km performance pace (min/km). For example, an individual with a seasonal personal best of 30 minutes on 10 km was running 3000 m at a pace of 3 min/km and an individual with a 35‐minute seasonal best at a pace of 3:30 min/km. This guaranteed the same intensity according to the different performance levels. Finally, after a 15‐minute cool down jog and another 10‐minute rest in the sitting position, a fourth measurement was conducted 30 minutes after termination of the intensive exercise (Figure 1).
Figure 1.
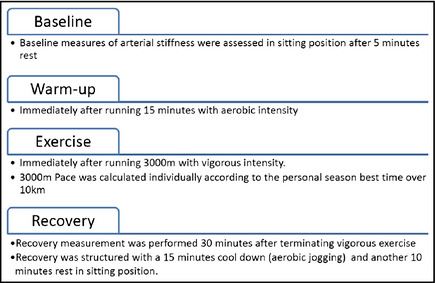
Study protocol.
The study was conducted in accordance with the Declaration of Helsinki (revision 2008). Patients gave written informed consent and agreed to the anonymous publication of their data.
Measurement of Arterial Stiffness Parameters
BP and arterial stiffness parameters were initially assessed in the supine position after 5 minutes of rest at the left brachial artery with the oscillometric Mobil‐O‐Graph device (IEM, Stolberg, Germany). Cuffs were chosen in dependence of upper‐arm circumference. For central systolic pressure, calculation and other measures of arterial stiffness an integrated transfer function (ARCSolver algorithm) was used.16, 17 In comparison to invasive central systolic pressure measurement and established radial tonometry with inbuilt generalized transfer function, the ARCSolver algorithm showed good agreement16, 17, 18
The Mobil‐O‐Graph automatically computes peripheral systolicand diastolic BP and central systolic and diastolic BP, AIx, and AIx at a heart rate of 75 beats per minute (AIx@75) as well as PWV.
Data Analyses
All descriptive data were expressed as mean±standard deviation. Arterial stiffness data at the four measuring points were analyzed using a generalized linear model with Bonferroni post‐hoc test. Associations regarding arterial stiffness, anthropometric data, and exercise history were estimated using partial correlation to control for cofounding age effects.
All analyses were performed using SPSS 21.0 software (IBM Inc, Armonk, NY). P values <.05 in a two‐sided analysis were considered significant.
Results
As seen in Table 2 and illustrated in Figure 2, there was an increase in all parameters of arterial stiffness from baseline to warm‐up and also from warm‐up to post‐exercise measurement, followed by a rapid decrease in the recovery period (P<.001 for interaction effect between groups [general linear model] and P<.05 between measurement point [Bonferroni post‐hoc]). Pressure waves according to the four measurement points are available in the online supplement (Appendix S1–S4).
Table 2.
Measures of Arterial Stiffness According to the Four Measuring Points
| Baseline | Warm‐Up | Directly After Exercise | Recovery | P Valuea | |
|---|---|---|---|---|---|
| Peripheral systolic BP, mm Hg | 129±12 | 137±11 | 161±17 | 120±10 | <.001 |
| Peripheral diastolic BP, mm Hg | 79±7 | 85±7 | 88±9 | 79±8 | <.001 |
| Central systolic BP, mm Hg | 112±10 | 118±10 | 139±16 | 105±9 | <.001 |
| Central diastolic BP, mm Hg | 81±8 | 87±8 | 90±9 | 80±8 | <.001 |
| AIx at a heart rate of 75 beats per min, % | 8±8 | 16±9 | 34±12 | 11±8 | <.001 |
| Pulse wave velocity, m/s | 5.4±0.6 | 5.7±0.6 | 6.5±0.8 | 5.2±0.6 | <.001 |
Abbreviations: AIx, augmentation index; BP, blood pressure. aOne‐way analysis of variance for repeated measurement.
Figure 2.
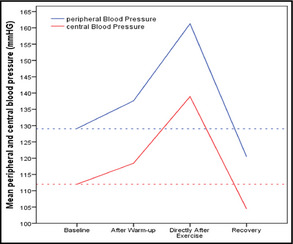
Peripheral and central systolic blood pressure according to the different time points. The dashed lines represent the baseline levels for central and peripheral blood pressure.
Both central (P<.001; Bonferroni post‐hoc) and peripheral systolic (P<.001) BP as well as PWV (P=.001) showed an augmented decrease below baseline levels in the recovery period. AIx@75 (P=.295) returned to baseline values 30 minutes after exercise.
After correction for age there was no association regarding years of training and the 10‐km seasonal best time to peripheral or central BP, as well as AIx and PWV at any of the four measuring points.
Discussion
This study shows that running at both moderate or vigorous intensity causes an increase in arterial stiffness in middle‐ and long‐distance runners. This increase is only transient and returns to baseline shortly after terminating exercise. Moreover, peripheral and central BP even showed overproportional decline below baseline level during the recovery period. However, no association of measures of arterial stiffness to years of training or fitness level could be observed.
It is widely reported that aerobic exercise has beneficial effects on arterial stiffness4, 19, 20, 21, 22 and that vigorous exercise seems to be a key element for maintaining arterial compliance in the long‐term21 because of an increase in parasympathetic activity and improvement of endothelial function as a result of enhanced arterial shear stress.21, 23 Contrary, acute exercise, either resistance or endurance, leads to a transient increase in arterial stiffness.15, 24
In our study there was a significant increase in all measured stiffness parameters after an aerobic warm‐up and a further severe increase following a vigorous 3000‐m running workout. These results were comparable to those of Nieman and colleagues,15 who also measured increased AIx in men and increased PWV in their female participants after 2 hours of running. However, the population in their study was small, at eight participants per sex. The results suggest that aerobic running for 2 hours or vigorous running for approximately 10 minutes has the same altering effects on arterial stiffness.
However, in the recovery period there was an augmented decrease in peripheral and central BP as well as in PWV below baseline levels, thus confirming several findings by Nieman and colleagues15 regarding the transient effects of stiffening under exercise and their effects on stiffness and wave reflection parameters during recovery. However, the explanatory power of their study suffered from the small population size and inability to derive significant results.
In their marathon study, Vlachopoulos and colleagues24 also measured a drop below baseline in peripheral and central BP. Albeit, in contrast to our findings, there was no deviation in PWV from baseline to post‐exercise, while AIx@75 decreased. A possible explanation for this could be the different measurement not directly but 10 to 15 minutes after finishing the workout or that long‐distance runners may, in fact, show different alterations as a result of the cardiovascular system experiencing other adaptions to different or longer exercise. However, we could not show associations between years of training or running performance to measures of arterial stiffness at baseline or the course during exercise and recovery.
Finally, a similar decrease in central systolic BP was also reported in the study by Yan and colleagues.13 These effects were present only in Caucasian participants and a decrease in AIx@75 after exercise was observed only in Caucasian women. This suggests a race‐ and sex‐specific response to exercise that should be given special attention in further studies. Moreover, Gkaliagkousi and colleagues14 outline that central hemodynamics differ with regard to exercise in hypertensive and normotensive patients. There are also fewer data available on the hemodynamic response to exercise in hypertensive patients and the interaction with antihypertensive drugs.
Study Limitations
This study investigated exercise‐related arterial compliance in highly trained athletes; therefore, arterial compliance with regard to exercise might be different in people with sedentary lifestyles. This question should be addressed in further studies. In addition, we used a different measurement device compared with other studies, perhaps causing possible bias regarding the absolute values of the measurements. However, we do not believe this affected the results as the repeated measurements in our study design were all conducted in a consistent manner.
Conclusions
These findings provide a better understanding of cardiovascular performance during different types of exercise conditions to determine cardiovascular risk during exercise. Further research is needed that focuses on the dose response of volume and intensity of exercise on arterial stiffness and wave reflection.
Supporting information
Appendix S1. Baseline.
Appendix S2. Warm‐up.
Appendix S3. Peak exercise.
Appendix S4. Recovery.
Acknowledgment and disclosures
We thank Lukas Steinheber for proofreading the manuscript. The authors declare no funding and have no conflicts of interest to disclose.
J Clin Hypertens (Greenwich). 2015;17:371–374. DOI: 10.1111/jch.12530. © 2015 Wiley Periodicals, Inc.
References
- 1. Heffernan KS, Rossow L, Jae SY, et al. Effect of single‐leg resistance exercise on regional arterial stiffness. Eur J Appl Physiol. 2006;98:185–190. [DOI] [PubMed] [Google Scholar]
- 2. Laurent S, Cockcroft J, Van Bortel L, et al. Expert consensus document on arterial stiffness: methodological issues and clinical applications. Eur Heart J. 2006;27:2588–2605. [DOI] [PubMed] [Google Scholar]
- 3. Vlachopoulos C, Aznaouridis K, Stefanadis C. Prediction of cardiovascular events and all‐cause mortality with arterial stiffness: a systematic review and meta‐analysis. J Am Coll Cardiol. 2010;55:1318–1327. [DOI] [PubMed] [Google Scholar]
- 4. Brownley KA, West SG, Hinderliter AL, Light KC. Acute aerobic exercise reduces ambulatory blood pressure in borderline hypertensive men and women. Am J Hypertens. 1996;9:200–206. [DOI] [PubMed] [Google Scholar]
- 5. Quinn TJ. Twenty‐four hour, ambulatory blood pressure responses following acute exercise: impact of exercise intensity. J Hum Hypertens. 2000;14:547–553. [DOI] [PubMed] [Google Scholar]
- 6. Cortez‐Cooper MY, DeVan AE, Anton MM, et al. Effects of high intensity resistance training on arterial stiffness and wave reflection in women. Am J Hypertens. 2005;18:930–940. [DOI] [PubMed] [Google Scholar]
- 7. Rakobowchuk M, McGowan CL, de Groot PC, et al. Effect of whole body resistance training on arterial compliance in young men. Exp Physiol. 2005;90:645–651. [DOI] [PubMed] [Google Scholar]
- 8. Casey DP, Nichols WW, Braith RW. Impact of aging on central pressure wave reflection characteristics during exercise. Am J Hypertens. 2008;21:419–424. [DOI] [PubMed] [Google Scholar]
- 9. Ranadive SM, Fahs CA, Yan H, et al. Comparison of the acute impact of maximal arm and leg aerobic exercise on arterial stiffness. Eur J Appl Physiol. 2012;112:2631–2635. [DOI] [PubMed] [Google Scholar]
- 10. Tordi N, Mourot L, Colin E, Regnard J. Intermittent versus constant aerobic exercise: effects on arterial stiffness. Eur J Appl Physiol. 2010;108:801–809. [DOI] [PubMed] [Google Scholar]
- 11. Laurent P, Marenco P, Castagna O, et al. Differences in central systolic blood pressure and aortic stiffness between aerobically trained and sedentary individuals. J Am Soc Hypertens. 2011;5:85–93. [DOI] [PubMed] [Google Scholar]
- 12. Vaitkevicius PV, Fleg JL, Engel JH, et al. Effects of age and aerobic capacity on arterial stiffness in healthy adults. Circulation. 1993;88(4 Pt 1):1456–1462. [DOI] [PubMed] [Google Scholar]
- 13. Yan H, Ranadive SM, Heffernan KS, et al. Hemodynamic and arterial stiffness differences between African‐Americans and Caucasians after maximal exercise. Am J Physiol Heart Circ Physiol. 2014;306:H60–H68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Gkaliagkousi E, Gavriilaki E, Nikolaidou B, et al. Exercise‐induced pulse wave velocity changes in untreated patients with essential hypertension: the effect of an angiotensin receptor antagonist. J Clin Hypertens (Greenwich). 2014;16:482–487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Nieman D, Dew D, Krasen P. Gender difference in the acute influence of a 2‐hour run on arterial stiffness in trained runners. Res Sports Med. 2013;21:66–77. [DOI] [PubMed] [Google Scholar]
- 16. Wassertheurer S, Kropf J, Weber T, et al. A new oscillometric method for pulse wave analysis: comparison with a common tonometric method. J Hum Hypertens. 2010;24:498–504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Weber T, Wassertheurer S, Rammer M, et al. Validation of a brachial cuff‐based method for estimating central systolic blood pressure. Hypertension. 2011;58:825–832. [DOI] [PubMed] [Google Scholar]
- 18. Salvi P. Pulse Waves: How Vascular Hemodynamics Affects Blood Pressure. Milan: Springer; 2012. [Google Scholar]
- 19. Currie KD, Thomas SG, Goodman JM. Effects of short‐term endurance exercise training on vascular function in young males. Eur J Appl Physiol. 2009;107:211–218. [DOI] [PubMed] [Google Scholar]
- 20. Tanaka H, Dinenno FA, Monahan KD, et al. Aging, habitual exercise, and dynamic arterial compliance. Circulation. 2000;102:1270–1275. [DOI] [PubMed] [Google Scholar]
- 21. van de Laar RJ, Ferreira I, van Mechelen W, et al. Lifetime vigorous but not light‐to‐moderate habitual physical activity impacts favorably on carotid stiffness in young adults: the amsterdam growth and health longitudinal study. Hypertension. 2010;55:33–39. [DOI] [PubMed] [Google Scholar]
- 22. Collier SR, Kanaley JA, Carhart R Jr, et al. Effect of 4 weeks of aerobic or resistance exercise training on arterial stiffness, blood flow and blood pressure in pre‐ and stage‐1 hypertensives. J Hum Hypertens. 2008;22:678–686. [DOI] [PubMed] [Google Scholar]
- 23. Shephard RJ, Balady GJ. Exercise as cardiovascular therapy. Circulation. 1999;99:963–972. [DOI] [PubMed] [Google Scholar]
- 24. Vlachopoulos C, Kardara D, Anastasakis A, et al. Arterial stiffness and wave reflections in marathon runners. Am J Hypertens. 2010;23:974–979. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix S1. Baseline.
Appendix S2. Warm‐up.
Appendix S3. Peak exercise.
Appendix S4. Recovery.