

In our previous editorial we discussed the beneficial cardiovascular effects of healthy lifestyle with a healthy diet and exercise.1 In this editorial we will discuss the adverse cardiovascular consequences of lack of exercise and excessive sitting. The cause of excessive sitting is the result of urbanization and technological advances, which have significantly limited mobility and increased the sitting time of people at work, in the home, and in the car commuting to work. It has been estimated that sitting time occupies about 55% of our daily waking time, excluding sleeping.2 There is increasing evidence from prospective, observational, and controlled studies that demonstrates the detrimental association between excessive sitting time and the incidence of cardiovascular disease (CVD), obesity, diabetes mellitus, and hypertension (HTN) in the United States and other developed countries.3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13 These studies show that currently, people spend an excessive amount of time sitting in front of a computer at work and in the home, watching television (TV), playing video games, speaking on the telephone, and driving the car to work. The harm of excessive sitting on cardiometabolic changes in the body is highlighted in two recent important publications. A paper by Shuval and colleagues12 from the Cooper Center in Dallas, TX, describes the adverse effects of prolonged sedentary time on cardiorespiratory fitness and cardiometabolic risk in men, whereas the paper by Kulinski and colleagues13 goes a step further by describing the adverse effects of extensive sedentary time on cardiorespiratory fitness, even if some physical activity is involved. The data from these studies add to a large number of data demonstrating that excessive sitting can be lethal. For further evidence that prolonged sitting is associated with increased CVD morbidity and mortality, a MEDLINE search of the English language literature was conducted between 2010 and 2014 and, from the 52 abstracts reviewed, 13 pertinent papers were selected. These papers together with collateral literature will be discussed in this editorial.
Studies Demonstrating an Association Between Prolonged Sitting Time and Cardiovascular Morbidity and Mortality
There are several studies that show an increased CVD risk with excessive sitting time.3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13 The data from these studies3, 4, 5, 6, 7, 8, 9 are summarized in the Table.
Table 1.
Studies Demonstrating the Cardiovascular Consequences of Prolonged Sitting
| Author | Patients, No. | Age, y | Sitting, h/d | Follow‐Up, y | CVD Deaths, No. | HR (95% CI) |
|---|---|---|---|---|---|---|
| Patel3 | 69,776 women | 50–74 | <3 | 14 | 2360 | 1.00 |
| 3–5 | 1.20 (1.1–1.32) | |||||
| ≥6 | 1.33 (1.17–1.52) | |||||
| 53,440 men | 1.00 | 4009 | ||||
| 3–5 | 1.06 (0.99–1.14) | |||||
| ≥6 | 1.18 (1.08–1.30) | |||||
| Warren4 | 7744 men | 20–89 | <11/wk | 21 | 2011 | 1.18 (0.85–1.63) |
| 23/wk | 1833 | 1.63 (1.23–2.20) | ||||
| Dunstan5 | 8800 men | ≥25 | <2 | 6.6 | 87 | 1.00 |
| 2–4 | 1.19 (0.72–1.99) | |||||
| ≥4 | 1.80 (1.00–3.25) | |||||
| Wijndaele6 | 13,197 | ≥35 | 9.5 | 9.5 | 373 | 1.08 (1.01–1.16) |
| Stamatakis7 | 4512 | ≥35 | <2 | 4.3 | 215 | 1.00 |
| 2–4 | 2.25 (1.30–3.89) | |||||
| Ford8 | 7350 | ≥20 | <1 | 8.5 | 190 | 1.00 |
| 1 | 1.42 (0.64–3.17) | |||||
| 2 | 0.82 (0.42–1.59) | |||||
| 3 | 1.42 (0.61–3.30) | |||||
| 4 | 0.84 (0.38–1.83) | |||||
| ≥5 | 1.20 (0.58–2.49) | |||||
| Matthews9 | 240,819 | 50–71 | <3 | 8.5 | 4684 | 1.00 |
| 3–4 | 0.98 (0.90–1.06) | |||||
| 5–6 | 1.02 (0.94–1.11) | |||||
| 7–8 | 0.95 (0.86–1.06) | |||||
| ≥9 | 1.16 (1.02–1.30) |
Abbreviations: CI, confidence interval; CVD, cardiovascular disease; HR, hazard ratio.
The study by Patel and colleagues3 is a large prospective study of US adults enrolled by the American Cancer Society to examine the leisure time spent on sitting and physical activity acquired by questionnaire, in relation to mortality. This study included 53,440 men aged 63 to 65 years and 69,776 women aged 61 to 63 years, free of CVD at baseline. After a follow‐up of 14 years, 11,307 (20.6%) deaths in men and 7923 (11.4%) deaths in women occurred. After adjusting for smoking, obesity, and other risk factors, sitting >6 h/d vs <3 h/d was associated with a relative risk (RR) of death of 1.17 (95% confidence interval [CI], 1.11–1.24) for men and a RR of 1.34 (95% CI, 1.25–1.44) for women. The associations were strongest for CVD mortality.
The study by Warren and colleagues4 demonstrates the association between sedentary behaviors and increased CVD mortality in men. This study included 7744 men aged 20 to 89 years who were free of CVD at baseline. Time spent watching TV and riding in a car was assessed and correlated with CVD mortality. After 21 years of follow‐up and adjusting for age, 377 CVD deaths occurred. Men who spent >23 h/wk of combined sedentary time had a 64% greater risk of dying from CVD than those who spent <11 h/wk (P trend <.001). Regardless of sedentary behavior, older individuals with normal weight and normal BP and being physically active had reduced CVD mortality.
The study by Dunstan and colleagues5 examined the association of prolonged TV viewing time with all‐cause mortality, CVD mortality, cancer, and non‐CVD mortality. This study included 8800 adults 25 years and older participating in the Australian Diabetes, Obesity, and Lifestyle Study (AusDiab). During 6.6 years of follow‐up there were 284 deaths, of which 87 were caused by CVD. After multiple adjustments for CVD risk factors, for viewing TV time 2 to 4 h/d the CVD, the hazard ratio (HR) for CVD mortality was 1.19 (95% CI, 0.72–1.99) and for ≥4 h/d the HR was 1.80 (95% CI, 1.04–2.05). For similar viewing TV time, the HRs for all‐cause mortality were 1.13 (95% CI, .87–1.36) and 1.46 (95% CI, 1.04–2.05), respectively.
The study by Wijndaele and colleagues6 examined the association between TV viewing time and incidence of fatal and nonfatal CVD in 12,608 men and women, mean age 61.4±9 years, who were free of CVD at baseline. After a mean follow‐up of 6.9±1.9 years and after adjusting for CVD risk factors, TV viewing time was associated with an increased total CVD mortality 2620 of 12,608 (20.8%) and HR of 1.06 (95% CI, 1.03–1.08), nonfatal CVD 2134 of 12,608 (16.9%) and HR of 1.06 (95% CI, 1.03–1.09), and coronary heart disease (CHD) 940 of 12,608 (0.07%) and HR of 1.08 (95% CI, 1.03–1.13). Adjustment for several CVD risk factors only partially mediated these associations.
The study by Stamatakis and colleagues7 examined the independent relationships of TV viewing and other screen‐based entertainment with all‐cause mortality and clinically confirmed CVD events. The study also examined the effect of screen time on cholesterol, high‐density lipoprotein (HDL), and inflammatory markers as mediators of CVD events. The study included 4512 patients (1945 men, 2567 women) 35 years and older, who were followed for 4.3 years. During the follow‐up period there were 215 CVD events and 325 all‐cause deaths. After adjustment for CVD risk factors, the HR for all‐cause mortality was 1.52 (95% CI, 1.06–2.16) and for CVD events was 2.30 (95% CI, 1.33–3.96) for ≥4 h/d screen time. Adjusting for physical activity only slightly attenuated the findings.
The study by Ford8 examined the association between total screen time (TV+computer) and all‐cause mortality. This study included 7350 adults aged 20 years and older who participated in the National Health and Nutrition Examination Survey (NHANES) and were followed for a medium of 5.8 years. After extensive adjustments, the HR for all‐cause mortality for the highest category was 1.30 (95% CI, 0.82–2.05). There was no significant trend between screen time exposure and circulatory diseases.
The study by Matthews and colleagues9 examined the association of prolonged sitting time and moderate to vigorous physical activity (MVPA) with mortality in 240,818 adults aged 50 to 71 years who participated in the National Institutes of Health‐American Association of Retired Persons (NIH‐AARP) Diet and Health Study who were free of CVD, respiratory disease, or cancer at baseline. In participants reporting the longest TV viewing time (≥7 vs <1 h/d), the HRs for all‐cause mortality and CVD mortality were HR 1.61 (95% CI, 1.47–1.76) and HR 1.85 (95% CI, 1.56–2.20), respectively. After adjusting for MVPA (>7 h/wk) and TV viewing time (≥7 h/d) the HRs for all‐cause and CVD mortality were 1.47 (95% CI, 1.20–1.79) and 2.00 (95% CI, 1.33–3.00), respectively. This study demonstrated that prolonged sitting is associated with significant all‐cause and CVD mortality and participation in MVPA did not mediate the risks.
Similar results have also been reported by two recent reviews of several prospective studies,10, 11 demonstrating the health risks of too much sitting time. The two recent studies by Shuval and colleagues12 and Kulinski and colleagues13 examined the effects of sedentary behavior on the cardiometabolic changes in the body and on physical fitness to delineate the mechanism by which physical inactivity increases the risk for the development of CVD morbidity and mortality. The prospective study by Shuval and colleagues12 included 1269 men aged 46.2±8.9 years from the Cooper Center Longitudinal Study who were followed for a mean of 9.3±7.4 years. The study found that sedentary time ≥9 h/wk compared with ≤9 h/wk was significantly associated with higher triglyceride levels, higher triglyceride/HDL‐C ratios, higher BMI, and higher waist circumference and body fat percentage (P trend <.05). The association between prolonged sedentary time and cardiometabolic biomarkers was less pronounced when taking physical fitness into account. The study by Kulinski and colleagues13 examined the association between cardiorespiratory fitness and sedentary behavior, independent of exercise activity in 2223 patients aged 12 to 49 years from the NHANES 2003–2004 without heart disease at baseline. The study used an accelerometer to ascertain daily sedentary time as counts per minute. Cardirespiratory fitness was assessed by a submaximal exercise by a treadmill test. An additional hour of daily activity time was associated with a 0.88 (CI, 0.37–1.39) metabolic equivalent (MET) higher fitness for men (P<.001) and 1.37 (CI, 0.43–2.31) MET higher fitness for women (P=.004). In contrast, an additional hour of sedentary time was associated with –0.12 (CI, −0.02 to −0.22) MET (P=.03) and −0.24 (CI, −0.10 to −0.38) MET (P<.001) for men and women, respectively. This study showed that sedentary behavior has an inverse association with fitness. Objectively measured leisure time with an accelerometer has shown that people spend a large part of their time in sedentary behaviors (Figure).
Figure 1.
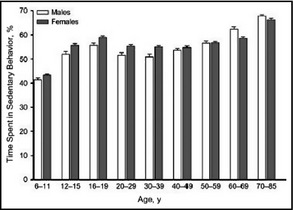
The percentage of time spent in sedentary behaviors by US men and women measured by accelerometer (mean±standard error). The sedentary time increases as people age. Constructed from data provided by Matthews and colleagues.2
Possible Mechanisms for the Adverse Cardiovascular Effects of Prolonged Sitting
The precise pathophysiologic mechanism(s) by which sedentary behaviors lead to CVD morbidity and mortality is not clear at present. It has been suggested from animal as well as human studies that metabolic changes linked to prolonged sitting could be responsible for the development of CVD.14, 15 There is evidence that the activity of lipoprotein lipase (LPL) is reduced by 80% to 90% during sitting compared with standing or ambulating.14 LPL is a critical enzyme for the catabolism of triglyceride (TG)‐rich lipoproteins in the vascular endothelium leading to decreased TG uptake by the nonexercising large muscles and increased levels of plasma TGs, which, in combination with low HDL cholesterol, lead to the development of atherosclerosis. Metabolically, excessive sitting and low energy expenditure lead to obesity, the metabolic syndrome, insulin resistance, type 2 diabetes mellitus, and HTN, all significant risk factors for CVD.15 A further important mechanism might be related to a decreased expression of endothelial nitric oxide synthase that is caused by the reduced local shear stress as a result of lower blood flow in the limbs from prolonged sitting.7 The direct effect of sitting idle is that the work performed by the large skeletal muscles of the legs, back, and trunk required for upright movement comes to a halt, leading to precipitous fall of LPL activity with the known adverse metabolic consequences. However, at present, we do not know how prolonged sitting impacts the metabolic processes and underlying mechanisms establishing a plausible cause‐effect explanation for the findings of observational studies. The most direct evidence for this important area of sedentary behaviors will, hopefully, come from future experimental studies providing a cause‐effect relationship between excessive sitting and metabolic risk factors.
Discussion
The industrial revolution and technological advances have attracted a large number of people from the country and their farming activities to large urbanized cities and have limited their mobility. Today, people spend more than 60% of their 16‐hour waking time sitting before computers at work and home, watching TV, speaking on the phone, and commuting to work sitting in a car on congested highways. Children do not walk to a neighborhood school, but are transported by bus or car to more distant schools. After school, instead of playing with their friends outside the home, they spend enormous amounts of time playing video games or talking on the phone. Adults do not go to the stores to shop for the things they need, instead order them through the Internet delivered to their front door. Therefore, it is not a surprise that the Homo erectus has now become Homo sedentarius. Technological changes in people's homes, work places, and communities, together with societal trends that contribute to the progression of human inactivity, continue to appear worldwide and it is naive to assume that we have reached the pinnacle of physical inactivity. Data from a previous NHANES report show that only 28% of Americans are physically active by meeting the minimal exercise recommendations for 30 min/d 5 d/wk.2, 16 Employed persons in many Western countries spend up to half a day being sedentary.17 It is time to stem this unhealthy trend. From the data presented here, it has become clear that too much sitting can be lethal. The American College of Sports Medicine (ACSM) has already issued a recent statement for professional care providers to recommend daily exercises for their patients.18 According to this statement, adults should engage in moderate‐intensity cardiorespiratory exercise training for ≥30 min/d for ≥5 d/wk for a total of ≥150 min/wk or vigorous‐intensity cardiorespiratory exercise training for ≥20 min/d for ≥3 d/wk for a total of ≥75 min/wk. In addition to exercising regularly, the ACSM also recommends that there are health benefits in concurrently reducing the total time spent in sedentary pursuits and by increasing frequent, short bouts of standing and physical activity, even in physically active adults. Two recent cross‐sectional studies have also demonstrated an association between the number of breaks and various cardiometabolic parameters after accounting for moderate to vigorous physical activity.19, 20 In addition, the development and increasing popularity of wearable health monitoring devices that provide a wealth of information to the wearer may help to change the current unhealthy lifestyle into a healthier one.21
Disclosures
The authors declare no conflicts of interest and no funds were received for the preparation of this manuscript.
References
- 1. Chrysant SG, Chrysant GS. A healthy lifestyle could reduce the onset of first heart attack by 80%. J Clin Hypertens (Greenwich). 2014;17:168–171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Matthews CE, Chen KY, Freedson PS, et al. Amount of time spent in sedentary behaviors in the United States 2003–2004. Am J Epidemiol. 2008;167:875–881. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Patel AV, Bernstein L, Deka A, et al. Leisure time spent sitting in relation to total mortality in a prospective cohort of US adults. Am J Epidemiol. 2010;172:419–429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Warren TY, Barry V, Hooker SP, et al. Sedentary behaviors increase risk of cardiovascular disease mortality in men. Med Sci Sports Exerc. 2010;42:879–885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Dunstan DW, Barr EL, Healy GN, et al. Television viewing time and mortality. The Australian Diabetes, Obesity and Lifestyle Study (AusDiab). Circulation. 2010;121:384–391. [DOI] [PubMed] [Google Scholar]
- 6. Wijndaele K, Brage S, Besson H, et al. Television viewing and incident cardiovascular disease: prospective associations and mediation analysis in the EPIC Norfolk Study. PLoS One. 2011;6:e20058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Stamatakis E, Hamer M, Dunstan DW. Screen‐based entertainment time, all‐cause mortality, and cardiovascular events. J Am Coll Cardiol. 2011;57:292–299. [DOI] [PubMed] [Google Scholar]
- 8. Ford ES. Combined television viewing and computer use and mortality from all‐causes and diseases of the circulatory system among adults in the United States. BMC Public Health. 2012;12:70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Matthews CE, George SM, Moore SC, et al. Amount of time spent in specific behaviors and cause‐specific mortality in US adults. Am J Clin Nutr. 2012;95:437–445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Ford ES, Caspersen CJ. Sedentary behavior and cardiovascular disease: a review of prospective studies. Int J Epidemiol. 2012;41:1338–1353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Dunstan DW, Howard B, Healy GN, Owen N. Too much sitting‐a health hazard. Diabetes Res Clin Pract. 2012;97:368–376. [DOI] [PubMed] [Google Scholar]
- 12. Shuval K, Finley CE, Barlow CE, et al. Sedentary behavior, cardiorespiratory fitness, physical activity, and cardiometabolic risk in men: the Cooper Center Longitudinal Study. Mayo Clin Proc. 2014;89:1052–1062. [DOI] [PubMed] [Google Scholar]
- 13. Kulinski JP, Khera A, Ayers CR, et al. Association between cardiorespiratory fitness and accelerometer‐derived physical activity and sedentary time in the general population. Mayo Clin Proc. 2014;89:1063–1071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Zderic TW, Hamilton MT. Physical inactivity amplifies the sensitivity of skeletal muscle to lipid‐induced downregulation of lipoprotein lipase activity. J Appl Physiol. 2006;100:249–257. [DOI] [PubMed] [Google Scholar]
- 15. Hamilton MT, Hamilton DG, Zderic TW. Role of low energy expenditure and sitting in obesity, metabolic syndrome, type 2 diabetes, and cardiovascular diseases. Diabetes. 2007;56:2655–2667. [DOI] [PubMed] [Google Scholar]
- 16. Kruger J, Yore MM, Kohl HW 3rd. Leisure‐time physical activity patterns by weight control status: 1999–2002 NHANES. Med Sci Sports Exerc. 2007;39:788–795. [DOI] [PubMed] [Google Scholar]
- 17. Van Uffern JG, Wong J, Chau JY, et al. Occupational sitting and health risks: a systematic review. Am J Prev Med. 2010;39:379–388. [DOI] [PubMed] [Google Scholar]
- 18. Garber CE, Blissmer B, Deschenes MR, et al. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidelines for prescribing exercise. Med Sci Sports Exerc. 2011;43:1334–1359. [DOI] [PubMed] [Google Scholar]
- 19. Healy GN, Dunstan DW, Salmon J, et al. Breaks in sedentary time: beneficial associations with metabolic risk. Diabetes Care. 2008;31:661–666. [DOI] [PubMed] [Google Scholar]
- 20. Healy GN, Matthews CE, Dunstan DW, et al. Sedentary time and cardiometabolic risk. Eur Heart J. 2011;32:590–597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Patel MS, Asch DA, Volpp KG. Wearable devices as facilitators, not drivers of hralth behavior change. JAMA. http://jama.jamanetwork.com. Accessed January 08, 2015. [DOI] [PubMed] [Google Scholar]