

Summary:
We report a rare case of absent thumb IP joint flexion in bilateral thumbs due to anomalous tendon slips of the flexor pollicis longus. Cutting the anomalous insertions failed to improve active flexion of the IP joints. Successful treatment was achieved by evaluating the musculotendinous units of the original flexor pollicis longus and the anomalous flexor pollicis longus tendon during a wide-awake surgery.
Absent thumb IP joint flexion due to an anomalous tendon slip of the flexor pollicis longus (FPL) is rare and the treatment is difficult, because the FPL musculotendinous unit may be hypoplastic and accompanied by other abnormalities. In particular, operations conducted under general anesthesia cannot reveal whether procedures have been sufficient because the surgeon can confirm active mobility of the thumb only after the patient awakens from anesthesia.
Wide-awake surgery is useful for tendon reconstruction because the surgeons can observe muscle-tendon excursion and active mobility of the fingers during and after the procedure.1–3 We have previously reported that the voluntary active contraction distance of musculotendinous units can be determined only during wide-awake surgery. Active contraction distance of musculotendinous units is a useful index to evaluate the function of the musculotendinous unit.4 We report a rare case of absent thumb IP joint flexion in bilateral thumbs due to anomalous tendon slips of the FPL, in which treatment was successful using this evaluation of musculotendinous units during wide-awake surgery.
Case Report
A 10-year-old boy complained of inability to flex the interphalangeal (IP) joints of both thumbs. No finger creases were observed on either palmar or dorsal sides of the IP joint, and no active motion was present. (See Video 1 [online], which displays a 0- to 60-degree passive range of motion of the bilateral thumbs at the IP joint with no active flexion.)
Video 1. Video 1 from “Wide-awake Surgery for Congenital Thumb Flexion Anomaly in a Child”.
No other complicating anomalies were identified, and there was no family history of congenital anomalies. The passive range of motion of both thumbs at the IP joint was 0–60 degrees with no active flexion. The metacarpophalangeal and carpometacarpal joints appeared normal. X-rays of the thumbs were normal. Three-dimensional computed tomography and magnetic resonance imaging showed the presence of a thin FPL tendon. Because the patient had hoped to undergo treatment under local anesthesia, we performed a wide-awake surgery, with subcutaneous infiltration of 20 ml lidocaine (1%) with 10 µg/ml of epinephrine. Exploration of the right thumb revealed a thin FPL tendon at the level of the proximal phalanx, and the FPL muscle-tendon is divided into 2 at the level of the forearm. One tendon following the normal course and appearing hypoplastic seemed to be the original FPL tendon; the other inserted into the thenar muscle and seemed to represent an anomalous FPL tendon (Fig. 1A). When we asked the patient to the flex the IP joint, the FPL muscle was contracting, but the force to flex the IP joint was not being transmitted because it was interfered by the anomalous insertion. On the other hand, the IP joint could be flexed when the FPL tendon was distracted proximally. The anomalous insertion was then cut (Fig. 1B), and although active flexion range of the IP joint improved slightly, it still remained limited. We thought the hypoplastic original FPL muscle-tendon was weak. To evaluate muscular strength during the wide-awake surgery, we measured the active voluntary distance and passive distraction distance from the original FPL and anomalous FPL muscle-tendons. Active contraction distance of the hypoplastic original FPL muscle-tendon was 12 mm, compared with 22 mm for the anomalous FPL muscle-tendon. (See Video 2 [online], which displays that when the patient is asked to flex the thumb with maximum power, the voluntary muscle-tendon contraction to the proximal side is observed. The active contraction distance is measured from the resting position to the maximum proximal point. Active contraction distance of the hypoplastic original FPL muscle-tendon was 12 mm.) (See Video 3 [online], which displays that active contraction distance of the anomalous FPL muscle-tendon was 22 mm.)
Fig. 1.
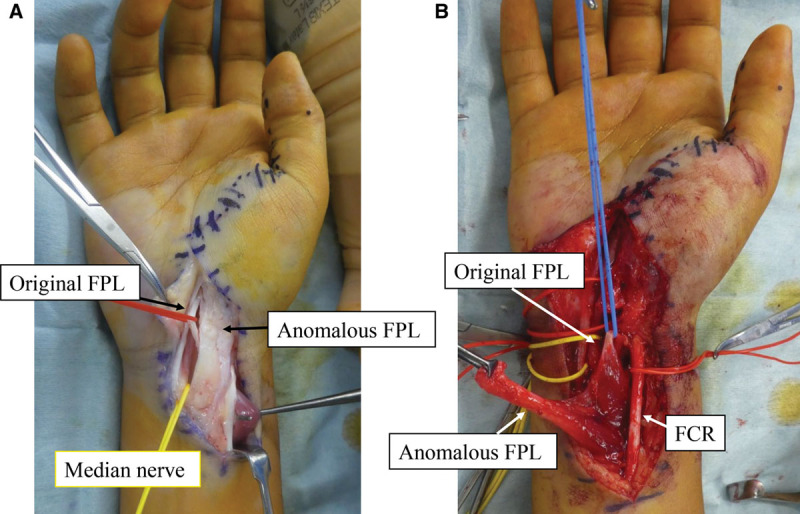
Intraoperative view of the patient’s right hand. A, The original FPL tendon is following the normal course but is hypoplastic. The anomalous FPL tendon is attached to the thenar muscle. B, When the anomalous FPL tendon insertion is cut, the original FPL and the anomalous FPL are seen to have the same muscle origins.
Video 2. Video 2 from “Wide-awake Surgery for Congenital Thumb Flexion Anormaly in a Child”.
Video 3. Video 3 from “Wide-awake Surgery for Congenital Thumb Flexion Anomaly in a Child”.
Active contraction distance of the anomalous FPL muscle-tendon was greater than that on the original FPL muscle-tendon. End-to-side suturing of the anomalous FPL tendon slip to the original FPL tendon was thus performed to maintain the dynamic strength and power of the tendon, without reducing its output power as the source (Fig. 2). Active flexion range of the IP joint improved without flexion lag after end-to-side suturing. Postoperatively, early active motion exercises were performed to prevent tendinous adhesions. Based on the wishes of the patient, similar surgery was performed on the left hand. One year later, improvements in pinch strength (Rt. 2.6 kg, Lt. 2.4 kg) and active flexion range of the IP joint (Rt. Ext 0 degree/flex 40 degree, Lt. Ext 0 degree/flex 40 degree) had been maintained. (See Video 4 [online], which displays active range of motion of the right thumb at 1 year after surgery.) This case report was approved by the institutional review board committee of Toyama University, and informed consent was obtained from the patient and from his parents. The parents agreed to the publication of this surgical case report.
Fig. 2.
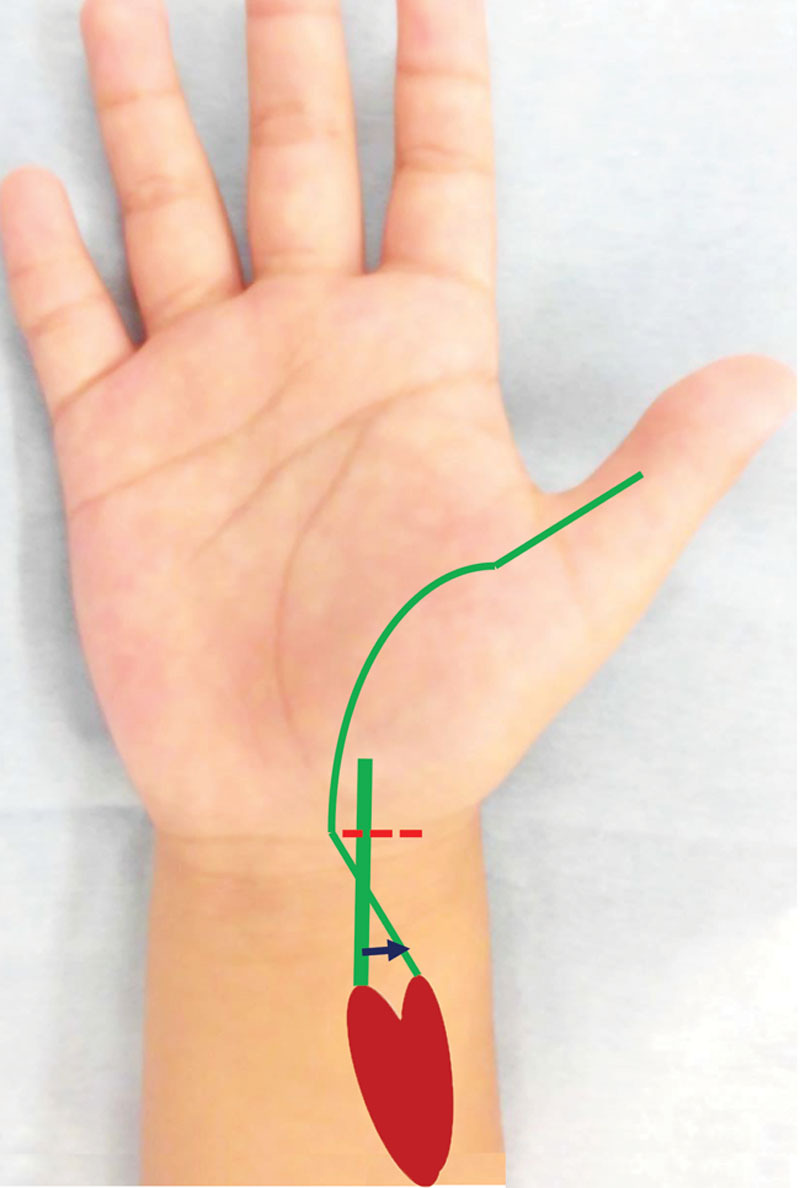
Surgical schema. After cutting the anomalous FPL tendon insertion (the dashed line), end-to-side suturing (arrow) of the anomalous FPL tendon slip to the original FPL tendon was performed to maintain the dynamic strength and power of the tendon, without reducing its output power as the source.
Video 4. Video 4 from “Wide-awake Surgery for Congenital Thumb Flexion Anomaly in a Child”.
Discussion
Several types of congenital FPL abnormality have been reported. Nakamura et al reviewed the literature on congenital abnormalities of FPL (Table 1). They showed that these abnormalities can be divided into 5 different groups5: (1) conjunction with radial deficiency; (2) conjunction with hypoplasia of the thumb; (3) conjunction with absence of the median innervated intrinsic muscles; (4) conjunction with absence of the flexor pollicis brevis; or (5) simple abnormalities of the FPL alone. Abnormalities of the FPL can be further divided into 4 subgroups: (i) absence; (ii) abnormal connection; (iii) anomalous insertion, or (iv) abnormal course. Our case fit into group 5—simple FPL abnormalities showing anomalous insertion.
Table 1.
The Classifications of FPL Anomalies
| Five groups |
| 1. Conjunction with radial deficiency |
| 2. Conjunction with hypoplasia of the thumb |
| 3. Conjunction with absence of the median innervated intrinsic muscles |
| 4. Conjunction with absence of the flexor pollicis brevis |
| 5. Simple abnormalities of the flexor pollicis longus alone |
| Four subgroups |
| i. Absence |
| ii. Abnormal connection |
| iii. Anomalous insertion |
| iv. Abnormal course |
There were similar reports of congenitally absent thumb IP joint flexion in the thumbs due to anomalous tendon slips of the FPL.5–9 The methods for such operation remain controversial. One report suggested that only cutting the anomalous insertion improves flexion of the thumb,5 whereas another reported that tendon transfer might be needed because thumb flexion disturbance recurred 19 years after cutting only the anomalous insertion.9 This is because the function of the FPL muscle is unknown. We, therefore, tried to assess the function of the FPL muscle during the wide-awake surgery. We referred to the active contraction distance of the FPL and active range of motion of the thumb. We have previously reported that if the active contraction distance of the FPL is >15 mm, the muscle should be considered available for motoring.10 Accordingly, we judged the original FPL muscle as weak, and performed end-to-side suturing of the anomalous FPL tendon slip to the original FPL tendon. Iwase et al reported successful results using the same procedures, but performed under general anesthesia.11 In addition, in this wide-awake surgery case, the immediate results favored patient satisfaction and postoperative compliance. Wide-awake surgery may allow clarification of the pathophysiology as well as proving clinically useful.
There are no previous reports of wide-awake surgeries in children. In this case, the patient understood and was interested in surgery, and enjoyed the 100-minute surgery without oral medication, but not all children can tolerate local anesthesia surgery. This indication needs to be considered carefully.
Footnotes
Published online 8 April 2021.
Disclosure: The authors have no financial interest to declare in relation to the content of this article.
Related Digital Media are available in the full-text version of the article on www.PRSGlobalOpen.com.
References
- 1.Lalonde DH, Wong A. Dosage of local anesthesia in wide awake hand surgery. J Hand Surg Am. 2013; 38:2025–2028 [DOI] [PubMed] [Google Scholar]
- 2.Tang JB. Wide-awake primary flexor tendon repair, tenolysis, and tendon transfer. Clin Orthop Surg. 2015; 7:275–281 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bezuhly M, Sparkes GL, Higgins A, et al. Immediate thumb extension following extensor indicis proprius-to-extensor pollicis longus tendon transfer using the wide-awake approach. Plast Reconstr Surg. 2007; 119:1507–1512 [DOI] [PubMed] [Google Scholar]
- 4.Zukawa M, Osada R, Makino H, et al. Evaluation of the active voluntary contraction of the ruptured muscle-tendon during the wide-awake tendon reconstruction. Plast Reconstr Surg Glob Open. 2017; 5:e1597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Nakamura J, Kubo E. Bilateral anomalous insertion of flexor pollicis longus. J Hand Surg Br. 1993; 18:312–315 [DOI] [PubMed] [Google Scholar]
- 6.Miura T. Congenital anomaly of the thumb–unusual bifurcation of the flexor pollicis longus and its unusual insertion. J Hand Surg Am. 1981; 6:613–615 [DOI] [PubMed] [Google Scholar]
- 7.Hagan HJ, Idler RS. Limitation of thumb flexion due to an unusual insertion of the flexor pollicis longus. J Hand Surg Br. 1988; 13:474–476 [DOI] [PubMed] [Google Scholar]
- 8.Blair WF, Omer GE. Anomalous insertion of the flexor pollicis longus. J Hand Surg Am. 1981; 6:241–244 [DOI] [PubMed] [Google Scholar]
- 9.Kozuki K, Sakamoto K, Shakya I. Dysfunction in active flexion in the bilateral thumb IP joints due to congenital difference in the flexor pollicis longus. J Jpn Pediatric Orthop Soc. 2007; 16:48–51 [Google Scholar]
- 10.Zukawa M, Osada R, Makino H, et al. Wide-awake flexor pollicis longus tendon reconstruction with evaluation of the active voluntary contraction of the ruptured muscle-tendon. Plast Reconstr Surg. 2019; 143:176–180 [DOI] [PubMed] [Google Scholar]
- 11.Iwase Y, Kusunose K, Tomita Y. Observation of the improvement in the active range of motion by a short-term active thumb flexion exercise is helpful in the diagnosis of flexion disturbance in bilateral thumbs due to anomalous tendon slip of flexor pollicis longus: congenital flexion disturbance in bilateral thumbs: a case report. J Juntendo Med. 2015; 61:149–152 [Google Scholar]