

Abstract
Objective
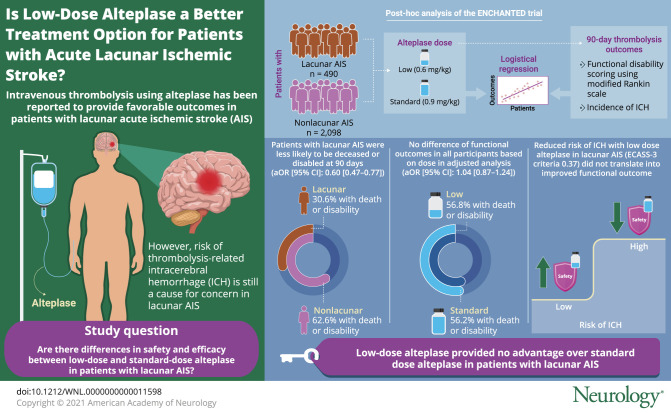
To determine any differential efficacy and safety of low- vs standard-dose IV alteplase for lacunar vs nonlacunar acute ischemic stroke (AIS), we performed post hoc analyzes from the Enhanced Control of Hypertension and Thrombolysis Stroke Study (ENCHANTED) alteplase dose arm.
Methods
In a cohort of 3,297 ENCHANTED participants, we identified those with lacunar or nonlacunar AIS with different levels of confidence (definite/according to prespecified definitions based on clinical and adjudicated imaging findings. Logistic regression models were used to determine associations of lacunar AIS with 90-day outcomes (primary, modified Rankin Scale [mRS] scores 2–6; secondary, other mRS scores, intracerebral hemorrhage [ICH], and early neurologic deterioration or death) and treatment effects of low- vs standard-dose alteplase across lacunar and nonlacunar AIS with adjustment for baseline covariables.
Results
Of 2,588 participants with available imaging and clinical data, we classified cases as definite/probable lacunar (n = 490) or nonlacunar AIS (n = 2,098) for primary analyses. Regardless of alteplase dose received, lacunar AIS participants had favorable functional (mRS 2–6, adjusted odds ratio [95% confidence interval] 0.60 [0.47–0.77]) and other clinical or safety outcomes compared to participants with nonlacunar AIS. Low-dose alteplase (versus standard) had no differential effect on functional outcomes (mRS 2–6, 1.04 [0.87–1.24]) but reduced the risk of symptomatic ICH in all included participants. There were no differential treatment effects of low- vs standard-dose alteplase on all outcomes across lacunar and nonlacunar AIS (all pinteraction ≥0.07).
Conclusions
We found no evidence from the ENCHANTED trial that low-dose alteplase had any advantages over standard dose for definite/probable lacunar AIS.
Classification of Evidence
This study provides Class II evidence that for patients with lacunar AIS, low-dose alteplase had no additional benefit or safety over standard-dose alteplase.
Clinical Trial Registration
Clinicaltrials.gov identifier NCT01422616.
In routine clinical practice, patients with lacunar acute ischemic stroke (AIS) are eligible to receive IV thrombolysis, given comparable favorable outcomes to other common AIS pathologic subtypes.1–3 These results were confirmed in a recent subgroup analysis of the Efficacy and Safety of Magnetic Resonance Imaging–Based Thrombolysis in Wake-Up Stroke (WAKE-UP) trial, where the safety and efficacy of standard-dose IV alteplase were comparable between lacunar and nonlacunar subtypes defined on baseline MRI.4 Similar consistency of effect of IV alteplase between lacunar and nonlacunar AIS, defined by the Oxfordshire Community Stroke Project (OCSP) syndromic classification, was found in the third International Stroke Trial (IST-3).5 Despite this evidence, some clinical concern persists over whether the modest risk of thrombolysis-related intracerebral hemorrhage (ICH) could offset the modest benefits of IV thrombolysis for lacunar AIS, where the natural course is generally more benign compared to other AIS subtypes6 from there being no or small thrombotic lytic target on the presumption of a single penetrating artery occlusion.7,8
In the alteplase-dose arm of the Enhanced Control of Hypertension and Thrombolysis Stroke Study (ENCHANTED),9 a lower dose (0.6 mg/kg) of IV alteplase was shown to have a lower risk of ICH compared to standard dose (0.9 mg/kg) in thrombolysis-eligible patients with AIS. Whether it is the same for lacunar AIS is unclear. Herein, we report further analyses of the efficacy and safety of low- vs standard-dose IV alteplase in the ENCHANTED participants with lacunar (versus nonlacunar) AIS who were identified by the combination of clinical and adjudicated imaging findings.
Methods
Primary Research Question and Evidence Level
Is there are any differential efficacy and safety of low- vs standard-dose IV alteplase between participants with lacunar and nonlacunar AIS in the alteplase dose arm of the ENCHANTED trial? This study provides Class II evidence that for patients with lacunar AIS, low-dose alteplase has no additional benefit or safety over standard-dose alteplase.
Design and Participants
ENCHANTED was an international, multicenter, 2 × 2 quasifactorial, prospective, randomized, open-label, blinded-endpoint trial that assessed the effectiveness of low-dose (0.6 mg/kg; 15% as bolus, 85% as infusion during 1 hour) vs standard-dose (0.9 mg/kg; 10% as bolus, 90% as infusion during 1 hour) IV alteplase, and more intensive vs guideline-recommended control of blood pressure (BP) in adult participants with AIS. The study design, participant characteristics, and main results of the alteplase-dose arm have been reported9–11 for 3,310 patients with AIS recruited from 111 centers in 13 countries. Key demographic and clinical characteristics were recorded at the time of enrollment, with clinical severity defined according to the NIH Stroke Scale (NIHSS) at baseline, 24 hours, and at day 7 (or on discharge from hospital if earlier). A final clinical diagnosis of AIS subtypes based upon the opinion of site investigations, generally according to the Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification system,12 was made at day 7, postrandomization (or on discharge from hospital, if earlier).
Standard Protocol Approvals, Registrations, and Participant Consents
The study protocol was approved by the appropriate ethics committee at each participating center and written informed consent was obtained from participants or an appropriate legal surrogate according to the Declaration of Helsinki. The ENCHANTED trial was registered at ClinicalTrials.gov (Unique identifier: NCT01422616).
Imaging Analysis
Uncompressed digital images of all baseline and follow-up digital CT, MRI, and angiographic images were uploaded into the study brain imaging database in Digital Imaging and Communications in Medicine (DICOM) format identified only by the participant's unique study identification number. Images were analyzed centrally for any ICH by a trial adjudication panel, blind to clinical data, treatment, date, and sequence of scan. Assessors graded any identified symptomatic ICH (sICH) using a range of standard definitions from the Safe Implementation of Thrombolysis in Stroke–Monitoring Study (SITS-MOST), National Institute of Neurologic Disease and Stroke (NINDS), the European–Australian Cooperative Acute Stroke Study II (ECASS), ECASS III, and IST-3 (additional Methods I, doi.org/10.5061/dryad.t1g1jwt0s).
The ENCHANTED Imaging Analysis Project was established in August 2016, with the aim of defining the presence, extent, and severity of, and swelling from, acute ischemic changes (including arterial territory, border zone, small subcortical and brainstem/cerebellar infarcts), coexisting old vascular lesions and their subtypes, white matter lesions, and brain volume loss on all collected images by an imaging analysis team of trained individuals, blind to all clinical data, using an electronic scoring system modified from IST-3.13 All observed infarct lesions on baseline (prerandomization) CT or MRI were coded according to the IST-3 criteria for infarct site and size. Separately and subsequent to primary scan reads, a neuroradiologist (Z.Z.) and neurosurgeon (X.C.) sought the ischemic lesion on 24-hour follow-up images while viewing the baseline images for those with no infarct lesion identified at baseline. They also assessed large vessel occlusion (LVO) on baseline CT angiography (CTA) or magnetic resonance angiography (MRA) according to a modified Thrombolysis in Cerebral Infarction (TICI) score for an abnormal artery in IST-3.14 All the imaging data were cross-checked (Z.Z.) and a final rating made before unmasking the clinical data and randomization code for analyses.
Definitions of Lacunar and Nonlacunar AIS
Different levels of confidence (definite/probable/possible) were used around the definitions of lacunar and nonlacunar AIS based on adjudicated imaging findings, clinical severity, and clinical diagnosis (additional Methods II, doi.org/10.5061/dryad.t1g1jwt0s). In brief, definite lacunar AIS was defined when all 4 criteria were met: (1) the presence of acute infarct lesion (maximum diameter ≤20 mm) in the territory of penetrating arteries, with a rounded, ovoid, or tubular shape on axial CT or diffusion-weighted imaging/apparent diffusion coefficient map (typical examples are shown in figure 1)15; (2) no LVO adjudicated centrally (on CTA/MRA) or reported by site investigators (on CTA/MRA/digital subtraction angiography); (3) the final diagnosis was reported as “small vessel or perforating vessel ‘lacunar’ disease” according to the TOAST criteria that involved any of the standard clinical lacunar syndromes with the lack of large vessel atheroma or cerebral cortical dysfunction; and (4) infarct side on images is consistent with that reported by site investigators. Definite nonlacunar AIS was defined as having acute infarct lesion with maximum diameter >20 mm or LVO on angiography. Participants were classified as nonlacunar if they had lacunar and nonlacunar infarcts.
Figure 1. Examples of Lacunar Ischemic Stroke at Different Locations From ENCHANTED.

Lacunar stroke at (A) left lentiform (red arrow) identified on 24-hour follow-up CT; (B) left internal capsule (red arrow) identified on 24-hour follow-up MRI; (C) right centrum semiovale (red arrow) identified on baseline and 24-hour follow-up MRI; (D) left internal border zone (red arrow) identified on baseline MRI; (E) right thalamus (red arrow) identified on baseline and 24-hour follow-up CT; and (F) brainstem (red arrow) identified on 24-hour follow-up MRI. DWI = diffusion-weighted imaging; ENCHANTED = Enhanced Control of Hypertension and Thrombolysis Stroke Study.
Given that the clinical diagnosis of lacunar syndrome plus baseline NIHSS score <7 had a high specificity to predict imaging-confirmed lacunar stroke in IST-3,16 probable lacunar and nonlacunar AIS were discriminated mainly by baseline NIHSS scores and final diagnosis in the situation that there was no acute infarct lesion identified on images or the images were not collected from the sites. For those with conflicting clinical and adjudicated imaging information that compromised the confidence of discrimination, we classified as possible lacunar or nonlacunar AIS according to the clinical diagnosis and LVO status.
Outcomes
The primary outcome of these analyses was the composite endpoint of disability or death (modified Rankin Scale [mRS] scores 2–6) at 90 days postrandomization. Secondary efficacy outcomes included major disability or death (mRS 3–6), death (mRS 6), and ordinal shift of the full range of mRS scores at 90 days. Secondary safety outcomes were sICH defined according to several criteria from other studies, fatal ICH within 7 days, ICH identified by central adjudicators, and any ICH adjudicated centrally or reported by site investigators. Other clinical outcomes included early neurologic deterioration (END) (≥4-point increase in NIHSS scores) or death within 24 hours or 7 days.
Statistical Analysis
Continuous or categorical variables at baseline were presented as mean (SD), median (interquartile range), or number (percentage). Baseline differences between participants with lacunar and nonlacunar AIS were evaluated using analysis of variance, χ2 test, or Wilcoxon signed-rank test, as appropriate. Associations of lacunar AIS with 90-day function, safety, and other secondary outcomes were estimated in logistic regression models with adjustment for randomized treatment and key prognostic covariates (age, sex, ethnicity, baseline NIHSS score, time from symptom onset to randomization, premorbid function [mRS score 0 or 1], prior use of antithrombotic agents, history of diabetes or cardiovascular disease, and assigned to intensive blood pressure–lowering group). The treatment effect of low- vs standard-dose alteplase was determined in logistic regression models and the heterogeneity of alteplase dose effect across participants with lacunar and nonlacunar AIS was estimated by adding an interaction term to statistical models. Proportional odds regression models were used to analyze ordinal mRS scores. The primary analyses pertain to participants with definite/probable lacunar and nonlacunar AIS after excluding those with a possible diagnostic classification. Sensitivity analyses of the treatment effects of low- vs standard-dose alteplase were performed in participants with definite lacunar/nonlacunar AIS and in all participants with possible lacunar/nonlacunar AIS. We also performed an exploratory analysis of the treatment effects in a subset of lacunar AIS identified at baseline (infarct size ≤15 mm and no adjudicated LVO). Data were reported as odds ratios (ORs) and 95% confidence intervals (CIs) and a 2-sided p < 0.05 was considered statistically significant. All analyses were performed using SAS version 7.1 and Stata version 12.0.
Data Availability
Additional methods (I and II) and data (supplementary tables 1–3) are available from Dryad (doi.org/10.5061/dryad.t1g1jwt0s). Individual de-identified participant data used in this analysis will be shared by request from any qualified investigator via the Research Office of The George Institute for Global Health.
Results
Baseline Characteristics
Among 3,297 AIS participants in the ENCHANTED alteplase dose arm, 2,588 (78.5%) were classifiable (definite lacunar, n = 195; probable lacunar, n = 295; definite nonlacunar, n = 1,697; and probable nonlacunar, n = 401 AIS) for inclusion in the primary analysis (figure 2). Compared to the 709 excluded participants, they were more likely to be older, have higher baseline NIHSS scores, be Asian, have a history of cardiovascular disease, and have a final diagnosis of LVO, but they also had shorter time interval from symptom onset to randomization (supplementary table 1, doi.org/10.5061/dryad.t1g1jwt0s). Table 1 shows that all the baseline clinical characteristics were significantly different between definite/probable lacunar and nonlacunar AIS except for sex, history of diabetes, and prior use of statin/other lipid-lowering agents. Participants with lacunar (versus nonlacunar) AIS were younger and had milder neurologic impairment, higher baseline BP, and a lower proportion with conventional cardiovascular risk factors except smoking. In keeping with the lacunar pattern of stroke, few participants had multiple lesions in both anterior and posterior circulation, but they were more likely to have a lesion only in the posterior circulation. They were also less likely to have brain atrophy or a hyperdense vessel sign on CT or hyperintense arteries on MRI.
Figure 2. Flowchart of Participants Included in Analyses.
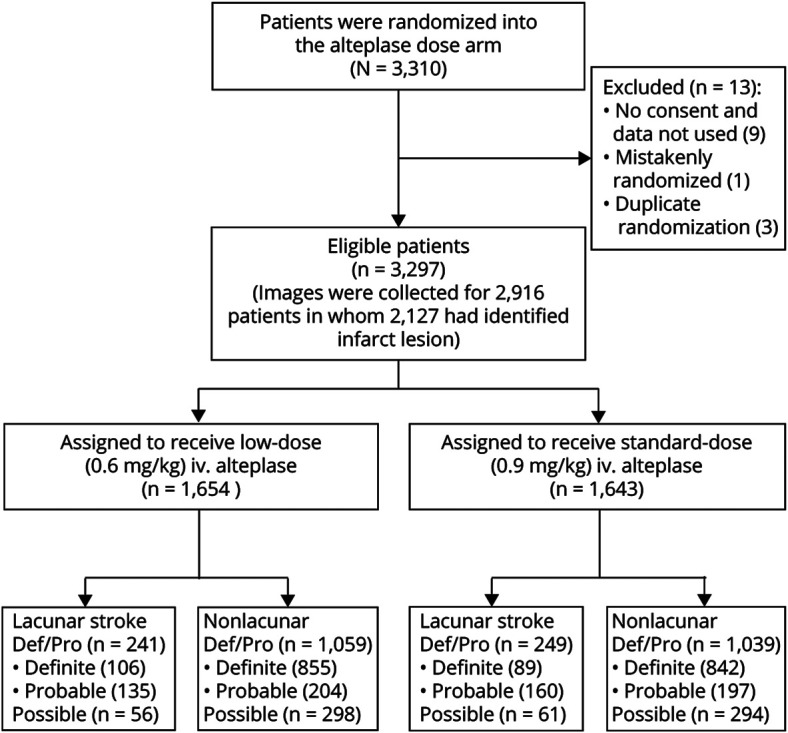
Def/Pro = definite or probable.
Table 1.
Baseline Characteristics of Participants With Definite/Probable Lacunar and Nonlacunar Stroke

Lacunar AIS and Outcomes
Compared to participants with definite/probable nonlacunar AIS, those with definite/probable lacunar AIS had better 90-day functional outcomes, whether defined by the outcome of mRS scores 2–6 (unadjusted OR 0.26, 95% CI 0.21–0.33), mRS scores 3–6 (0.20, 0.15–0.26), ordinal shift in the full range of scores (0.27, 0.23–0.33), or death alone (0.04, 0.01–0.12) (table 2). They were also less likely to have ICH and END or death after IV thrombolysis. The findings persisted with adjustment of baseline covariables and randomized alteplase dose.
Table 2.
Thrombolysis Outcomes in Definite/Probable Lacunar Versus Nonlacunar Stroke

Lacunar AIS and Alteplase Dose
The overall treatment effects of low- vs standard-dose alteplase on function, safety, and other outcomes in these 2,588 participants were comparable to the main results of the ENCHANTED trial, that low-dose vs standard-dose alteplase reduced the risk of sICH (SITS-MOST criteria, adjusted OR 0.39, 95% CI 0.21–0.73; NINDS criteria, 0.67, 0.50–0.89; ECASS II criteria, 0.56, 0.39–0.80; ECASS III criteria, 0.37, 0.21–0.67; IST-3 criteria, 0.54, 0.33–0.87) but with no difference in effect on functional outcomes (mRS 2–6, adjusted OR 1.04, 95% CI 0.87–1.24; mRS 3–6, 1.01, 0.85–1.21). There was no heterogeneity of treatment effects on all outcomes for definite/probable lacunar vs nonlacunar AIS after adjustment for baseline covariables (all pinteraction ≥0.07) (figures 3 and 4). Similar results were seen in the sensitivity analyses for definite lacunar and nonlacunar AIS (all pinteraction ≥0.16) (figures 4 and 5) and definite/probable/possible lacunar and nonlacunar AIS (all pinteraction ≥0.12) (data available on request).
Figure 3. Thrombolysis Outcomes in Participants With Definite/Probable Lacunar and Nonlacunar Stroke by Randomized Treatment.

*Adjusted for key prognostic covariates (age, sex, ethnicity, baseline NIH Stroke Scale [NIHSS] score, time from stroke onset to randomization, premorbid function [modified Rankin Scale (mRS) scores 0 or 1], prior use of antithrombotic agents [aspirin, other antiplatelet agent, or warfarin], history of diabetes or cardiovascular disease [stroke, atrial fibrillation, coronary artery disease, valvular or other heart disease], assigned to intensive blood pressure–lowering group) for functional outcomes. Adjusted for minimization and key prognostic covariates (age, baseline NIHSS score, time from stroke onset to randomization, and assigned to intensive blood pressure–lowering group) for safety outcomes and neurologic deterioration within 24 hours or 7 days.†Site reported or adjudicated centrally. CI = confidence interval; ECASS = European–Australian Cooperative Acute Stroke Study; END = early neurologic deterioration; ICH = intracerebral hemorrhage; IST-3 = third International Stroke Trial; NINDS = National Institutes of Neurologic Diseases and Stroke; sICH = symptomatic intracerebral hemorrhage; SITS-MOST = Safe Implementation of Thrombolysis in Stroke–Monitoring Study.
Figure 4. Randomized Treatment Effects on the Ordinal Modified Rankin Scale (mRS) Score by Lacunar and Nonlacunar Stroke.

*Adjusted for key prognostic covariates (age, sex, ethnicity, baseline NIH Stroke Scale [NIHSS] score, time from stroke onset to randomization, premorbid function [mRS scores 0 or 1], prior use of antithrombotic agents [aspirin, other antiplatelet agent, or warfarin], history of diabetes or cardiovascular disease [stroke, atrial fibrillation, coronary artery disease, valvular or other heart disease], assigned to intensive blood pressure–lowering group).
Figure 5. Thrombolysis Outcomes in Participants With Definite Lacunar and Nonlacunar Stroke by Randomized Treatment.

*Adjusted for key prognostic covariates (age, sex, ethnicity, baseline NIH Stroke Scale [NIHSS] score, time from stroke onset to randomization, premorbid function [modified Rankin Scale (mRS) scores 0 or 1], prior use of antithrombotic agents [aspirin, other antiplatelet agent, or warfarin], history of diabetes or cardiovascular disease [stroke, atrial fibrillation, coronary artery disease, valvular or other heart disease], assigned to intensive blood pressure–lowering group) for functional outcomes. Adjusted for minimization and key prognostic covariates (age, baseline NIHSS score, time from stroke onset to randomization, and assigned to intensive blood pressure–lowering group) for safety outcomes and neurologic deterioration within 24 hours or 7 days. †Site reported or adjudicated centrally. CI = confidence interval; ECASS = European–Australian Cooperative Acute Stroke Study; END = early neurologic deterioration; ICH = intracerebral hemorrhage; IST-3 = third International Stroke Trial; NINDS = National Institutes of Neurologic Diseases and Stroke; sICH = symptomatic intracerebral hemorrhage; SITS-MOST = Safe Implementation of Thrombolysis in Stroke–Monitoring Study.
Specifically, in the definite subgroup of lacunar AIS, there were no significant differences on the primary efficacy outcome (mRS 2–6) (33.7% vs 32.9%, adjusted OR 0.96, 95% CI 0.49–1.87) or major disability or death (mRS 3–6) (20.2% vs 15.3%, adjusted OR 1.31, 95% CI 0.54–3.19) between low-dose and standard-dose alteplase groups (figure 5). There was one case of sICH (0.9%) meeting NINDS and IST-3 criteria in participants with definite lacunar AIS treated by low-dose alteplase, but no case of sICH was observed after use of standard-dose alteplase. In participants with definite lacunar AIS who received low-dose alteplase, 3 (2.8%) had adjudicated ICH and 1 more had ICH reported by a site investigator, while any ICH occurred in 2 (2.2%) participants with definite lacunar AIS assigned to the standard-dose group. In a smaller subset of definite lacunar AIS identified at baseline with size <15 mm and no adjudicated LVO, 4 of the 9 participants (44.4%) in the low-dose group and 2 of the 7 participants (28.6%) in the standard-dose group had mRS 2–6 at 90 days postrandomization, and no ICH occurred in either treatment group (supplementary table 2, doi.org/10.5061/dryad.t1g1jwt0s).
Discussion
In these post hoc analyzes of the ENCHANTED trial, we did not identify any benefit, nor any harm, from the use of low-dose alteplase vs standard-dose alteplase to treat patients with lacunar AIS compared to those with other subtypes of AIS. As well as having a range of significantly different characteristics, the 90-day outcomes were better for those with lacunar than nonlacunar AIS, which provided some internal consistency for the classifications used in our study. However, given the low event rate of sICH, with fewer than 5 events in the primary analysis for definite or probable lacunar AIS, we are limited in the conclusions that can be drawn as to whether a lower dose of IV alteplase should be preferred because of the good prognosis for lacunar AIS.
Our results on thrombolysis outcomes for lacunar AIS are consistent with prior observational studies.2,17–21 However, the net benefit of thrombolysis for lacunar AIS is still debated, mainly because the evidence is drawn from subgroup analyzes of trials, such as WAKE-UP4 and IST-3,5 where there is low statistical power. In addition, accurate identification of lacunar AIS is challenging, especially in the absence of an acute lesion on the initial CT, and even MRI (in nearly one third of patients with nondisabling stroke).22 The pragmatic approach of applying a lacunar syndrome classification system in studies has moderate diagnostic sensitivity and specificity,15 which may potentially mix patients with nonlacunar AIS with the target population of lacunar AIS, and nondifferentially bias results towards IV thrombolysis.
We were unable to confirm in ENCHANTED participants any benefit of low-dose over standard-dose alteplase in lacunar AIS. The fact that there were few cases of sICH in the low-dose alteplase group, and no sICH in the standard-dose group, highlights the potential for chance and imprecise estimates of treatment effects when there are few events. Even with current imaging techniques and clinical criteria, it is difficult to discriminate lacunar AIS due to occlusion of a deep penetrating arteriole presumed caused by progressive lipohyalinosis from thrombosis related to atherosclerosis or embolus. Platelet activation triggered by disintegration of the endothelium from intrinsic cerebral small vessel disease (CSVD) may also be relevant in this type of AIS.8 It is possible, therefore, that IV thrombolysis may have a differential effect dependent on the cause of lacunar stroke, being more effective when there is underlying thromboembolism. In lacunar AIS, we noted a significant imbalance in the frequency of background white matter lesions between the low-dose and standard-dose alteplase groups (41.8% vs 30.7%), which could partly account for more ICH in the former (supplementary table 3, doi.org/10.5061/dryad.t1g1jwt0s).23 Again, however, due to the few sICH events in patients with lacunar AIS, we cannot confirm whether the increase in sICH by low-dose alteplase was confounded by CSVD.
Some strengths of our study include the large, prospective, multicenter cohort of patients with AIS who had systematic, complete, and high-quality data collected prospectively, where we were able to adjust for multiple covariables in statistical models. Furthermore, the imaging assessment was completed blind to clinical features and other data, using a rigorously defined approach developed for the IST-3 study. However, we acknowledge limitations that include insufficient statistical power and inevitable selection bias from the data being derived from a clinical trial where a large number of participants were from Asia and had mild to moderate stroke. Moreover, given the pragmatic nature of ENCHANTED, few participants had a baseline brain MRI, and the identification of lacunar AIS required analysis of follow-up images with comparison to those obtained at baseline. Whereas this approach may have altered the imaging appearances of acute ischemic lesions after use of IV thrombolysis24 and limited the identification of all true lacunar AIS, our results are comparable with previous work showing that nearly one-third of patients with nondisabling AIS lack an infarct lesion on acute MRI (median 4 days poststroke).22 In the ENCHANTED alteplase arm, 27.1% (789/2,916) of participants had no infarct lesion on either the baseline or 24-hour follow-up images. Thus, we had to use a combination of clinical and adjudicated imaging data to classify as many cases as possible into lacunar and nonlacunar AIS, which likely closely represents that used in routine practice. Relatively small samples in lacunar AIS compromised the power of a reliable assessment of any interaction, especially for sICH. Moreover, regarding the outcomes of major disability or death, a pinteraction of 0.07 might have been due to chance rather than true differential treatment effects of low- vs standard-dose alteplase across definite/probable lacunar and nonlacunar AIS. Future research in systematic reviews and clinical registries may be required to confirm or refute these findings.
We found no clear evidence that low-dose IV alteplase was any better or safer than standard-dose alteplase in the ENCHANTED participants who had lacunar AIS. According to standard eligibility criteria, patients with lacunar AIS should receive standard dose IV alteplase as with other AIS subtypes.
Acknowledgment
The authors thank the investigators, study teams, and patients for participating in the ENCHANTED trial. The research team acknowledges the support of the National Institute for Health Research Clinical Research Network (NIHR CRN) for conduct of the trial in England. Z.Z. received overseas visiting funding from Ren Ji Hospital, School of Medicine, Shanghai Jiao Tong University (2016–2018) and a Scientia PhD Scholarship from the University of New South Wales, Sydney (2018–2022) during the conduct of the study. C.S.A. holds an NHMRC Senior Investigator Fellowship.
Glossary
- AIS
acute ischemic stroke
- BP
blood pressure
- CI
confidence interval
- CSVD
cerebral small vessel disease
- CTA
CT angiography
- DICOM
Digital Imaging and Communications in Medicine
- ECASS
European–Australian Cooperative Acute Stroke Study
- ENCHANTED
Enhanced Control of Hypertension and Thrombolysis Stroke Study
- END
early neurologic deterioration
- ICH
intracerebral hemorrhage
- IST-3
the third International Stroke Trial
- LVO
large vessel occlusion
- MRA
magnetic resonance angiography
- mRS
modified Rankin Scale
- NIHSS
NIH Stroke Scale
- NINDS
National Institutes of Neurological Diseases and Stroke
- OCSP
Oxfordshire Community Stroke Project
- OR
odds ratio
- sICH
symptomatic intracerebral hemorrhage
- SITS-MOST
the Safe Implementation of Thrombolysis in Stroke–Monitoring Study
- TICI
Thrombolysis in Cerebral Infarction
- TOAST
Trial of Org 10172 in Acute Stroke Treatment classification
- WAKE-UP
Efficacy and Safety of MRI-based Thrombolysis in Wake-Up Stroke trial
Appendix. Authors

Footnotes
Class of Evidence: NPub.org/coe
Infographic: http://links.lww.com/WNL/B346
Study Funding
This study is supported by grants from the National Health and Medical Research Council (NHMRC) of Australia (project grant numbers 1020462 and 1101113), the Stroke Association of the UK (TSA 2012/01 and 2015/01), the Ministry of Health and the National Council for Scientific and Technological Development of Brazil (CNPQ: 467322/2014-7, 402388/2013-5), the Ministry for Health, Welfare and Family Affairs of the Republic of Korea (HI14C1985) (for the alteplase-dose arm), and a research grant from Takeda for conduct of the study in China.
Disclosure
Dr. Xia received a scholarship from China Scholarship Council (CSC). Prof. Hackett reports a fellowship and research grants from the National Health and Medical Research Council (NHMRC) of Australia. Prof. Woodward reports a National Health and Medical Research Council Investigator Grant (APP1174120) and Program Grant (APP1149987) and is a consultant to Amgen, Freeline, and Kyowa Hakko Kirin. Prof. Chalmers reports research grants and honoraria from Servier for the ADVANCE trial, outside the submitted work. Prof. Robinson reports grants from The Stroke Association, UK, and was a National Institute for Health Research (NIHR) Senior Investigator during the conduct of the study. Prof. Parsons reports personal fees from serving on Advisory Board for Boehringer Ingelheim (which markets alteplase outside of North America) during the conduct of the study. Prof. Demchuk reports personal fees from Medtronic, personal fees from Daiichi Sankyo, and a patent to Circle NVI issued outside the submitted work. Prof. Lindley reports grants from NHMRC of Australia during the conduct of the study. Dr. Mair reports grants from The Stroke Association, UK, during the conduct of the study. Prof. Wardlaw reports grants from The Stroke Association, UK, the Fondation Leducq, the British Heart Foundation, The European Union, the Row Fogo Charitable Trust, the Alzheimer's Society, Alzheimer's Research UK, and UK Medical Research Council during the conduct of the study. Prof. Anderson reports receiving honorarium from Takeda during the conduct of the study. Other authors have nothing to disclose for the present study. Go to Neurology.org/Nhttps://n.neurology.org/lookup/doi/10.1212/WNL.0000000000011598 for full disclosures.
References
- 1.Hsia AW, Sachdev HS, Tomlinson J, et al. Efficacy of IV tissue plasminogen activator in acute stroke: does stroke subtype really matter? Neurology 2003;61:71–75. [DOI] [PubMed] [Google Scholar]
- 2.Fuentes B, Martínez-Sánchez P, Alonso de Leciñana M, et al. Efficacy of intravenous thrombolysis according to stroke subtypes: the Madrid Stroke Network data. Eur J Neurol 2012;19:1568–1574. [DOI] [PubMed] [Google Scholar]
- 3.Mustanoja S, Meretoja A, Putaala J, et al. Outcome by stroke etiology in patients receiving thrombolytic treatment: descriptive subtype analysis. Stroke 2011;42:102–106. [DOI] [PubMed] [Google Scholar]
- 4.Barow E, Boutitie F, Cheng B, et al. Functional outcome of intravenous thrombolysis in patients with lacunar infarcts in the WAKE-UP trial. JAMA Neurol 2019;76:641–649. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lindley RI, Wardlaw JM, Whiteley WN, et al. Alteplase for acute ischemic stroke: outcomes by clinically important subgroups in the third International Stroke Trial. Stroke 2015;46:746–756. [DOI] [PubMed] [Google Scholar]
- 6.Bamford J, Sandercock P, Jones L, et al. The natural history of lacunar infarction: the Oxfordshire Community Stroke Project. Stroke 1987;18:545–551. [DOI] [PubMed] [Google Scholar]
- 7.Norrving B. Lacunar infarcts: no black holes in the brain are benign. Pract Neurol 2008;8:222–228. [DOI] [PubMed] [Google Scholar]
- 8.Regenhardt RW, Das AS, Lo EH, Caplan LR. Advances in understanding the pathophysiology of lacunar stroke: a review. JAMA Neurol 2018;75:1273–1281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Anderson CS, Robinson T, Lindley RI, et al. Low-dose versus standard-dose intravenous alteplase in acute ischemic stroke. N Engl J Med 2016;374:2313–2323. [DOI] [PubMed] [Google Scholar]
- 10.Huang Y, Sharma VK, Robinson T, et al. Rationale, design, and progress of the Enhanced Control of Hypertension and Thrombolysis Stroke Study (ENCHANTED) trial: an international multicenter 2 × 2 quasi-factorial randomized controlled trial of low- vs. standard-dose rt-PA and early intensive vs. guideline-recommended blood pressure lowering in patients with acute ischaemic stroke eligible for thrombolysis treatment. Int J Stroke 2015;10:778–788. [DOI] [PubMed] [Google Scholar]
- 11.Anderson CS, Woodward M, Arima H, et al. Statistical analysis plan for evaluating low- vs. standard-dose alteplase in the Enhanced Control of Hypertension and Thrombolysis Stroke Study (ENCHANTED). Int J Stroke 2015;10:1313–1315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Adams HP Jr, Bendixen BH, Kappelle LJ, et al. Classification of subtype of acute ischemic stroke: definitions for use in a multicenter clinical trial: TOAST: Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993;24:35–41. [DOI] [PubMed] [Google Scholar]
- 13.Wardlaw JM, Sandercock P, Cohen G, et al. Association between brain imaging signs, early and late outcomes, and response to intravenous alteplase after acute ischaemic stroke in the third International Stroke Trial (IST-3): secondary analysis of a randomised controlled trial. Lancet Neurol 2015;14:485–496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Mair G, von Kummer R, Adami A, et al. Arterial obstruction on computed tomographic or magnetic resonance angiography and response to intravenous thrombolytics in ischemic stroke. Stroke 2017; 48:353–360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Wardlaw JM, Smith EE, Biessels G, et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol 2013;12:822–838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Arba F, Mair G, Phillips S, et al. Improving clinical detection of acute lacunar stroke: analysis from the IST-3. Stroke 2020;51:1411–1418. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Matusevicius M, Paciaroni M, Caso V, et al. Outcome after intravenous thrombolysis in patients with acute lacunar stroke: an observational study based on SITS international registry and a meta-analysis. Int J Stroke 2019;14:878–886. [DOI] [PubMed] [Google Scholar]
- 18.Zivanovic Z, Gubi M, Vlahovic D, et al. Patients with acute lacunar infarction have benefit from intravenous thrombolysis. J Stroke Cerebrovasc Dis 2019;28:435–440. [DOI] [PubMed] [Google Scholar]
- 19.Eggers CCJ, Bocksrucker C, Seyfang L, et al. The efficacy of thrombolysis in lacunar stroke: evidence from the Austrian Stroke Unit Registry. Eur J Neurol 2017;24:780–787. [DOI] [PubMed] [Google Scholar]
- 20.Shobha N, Fang J, Hill MD. Do lacunar strokes benefit from thrombolysis? Evidence from the registry of the Canadian Stroke Network. Int J Stroke 2013;8(suppl A100):45–49. [DOI] [PubMed] [Google Scholar]
- 21.Fluri F, Hatz F, Rutgers MP, et al. Intravenous thrombolysis in patients with stroke attributable to small artery occlusion. Eur J Neurol 2010;17:1054–1060. [DOI] [PubMed] [Google Scholar]
- 22.Makin SD, Doubal FN, Dennis MS, et al. Clinically confirmed stroke with negative diffusion-weighted imaging magnetic resonance imaging: longitudinal study of clinical outcomes, stroke recurrence, and systematic review. Stroke 2015;46:3142–3148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Pantoni L, Fierini F, Poggesi A. Thrombolysis in acute stroke patients with cerebral small vessel disease. Cerebrovasc Dis 2014;37:5–13. [DOI] [PubMed] [Google Scholar]
- 24.Nagaraja N, Forder JR, Warach S, et al. Reversible diffusion-weighted imaging lesions in acute ischemic stroke: a systematic review. Neurology 2020;94:571–587. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Additional methods (I and II) and data (supplementary tables 1–3) are available from Dryad (doi.org/10.5061/dryad.t1g1jwt0s). Individual de-identified participant data used in this analysis will be shared by request from any qualified investigator via the Research Office of The George Institute for Global Health.