

Abstract
Purpose of Review
To review the latest evidence concerning the epidemiology, clinical implications, and management of psychiatric disorders in epilepsy.
Recent Findings
People with epilepsy have a 2–5 times increased risk of developing any psychiatric disorder, and 1 in 3 patients with epilepsy have a lifetime psychiatric diagnosis. Psychiatric comorbidities represent a poor prognostic marker as they have been associated with a poor response to treatment (drugs and surgery), increased morbidity, and mortality. Validated screening instruments are available for mood and anxiety disorders in adults as well as attention-deficit hyperactivity disorder in children with epilepsy.
Summary
All patients with epilepsy should be routinely screened for psychiatric disorder at the onset and at least once a year. Patients with epilepsy and their relatives should be informed of the risk of mental health problems and the implications.
Psychiatric disorders affect 1 in 3 people with epilepsy and are due to psychosocial and biological factors. Epilepsy is still a stigmatized condition, leading to discrimination and social withdrawal. In addition, major social limitations (e.g., loss of driving license) and the unpredictability of seizures can lead to poor self-esteem and depression. From a neurobiological perspective, neuroimaging studies in people with primary psychiatric conditions such as depression or schizophrenia have shown abnormalities in brain networks overlapping with those involved, for example, in temporal lobe epilepsy (TLE), particularly in the amygdala and the hippocampi. People with epilepsy, however, can also present with psychiatric symptoms peri-ictally, before, during, or after a seizure, or as a consequence of the treatment like antiseizure medications or epilepsy surgery.
Psychiatric problems could be due to shared neurobiological mechanisms, a consequence of having epilepsy or simply due to the unfortunate occurrence of 2 conditions in the same individual. Nevertheless, the management of these people can be challenging regardless of the causes. For this reason, physicians must identify comorbid psychiatric disorders and incorporate them into the comprehensive individual management. Accordingly, a multidisciplinary approach is required. This entails the need for health care professionals in other disciplines such as psychiatrists, clinical psychologists, neuropsychologists psychiatric nurses, and social workers to ensure that the individual receive the best management.
Focusing primarily on the last 5 years, we review current evidence about the epidemiology and clinical aspects of psychiatric disorders in epilepsy.
Epidemiology
Data from cross-sectional studies show that all psychiatric disorders seem to occur in a higher proportion of adults and children with epilepsy than in those without epilepsy.
In adults, a meta-analysis of 14 population-based studies including over 1,000,000 subjects showed an overall prevalence of active (current or last 12 months) depression in epilepsy of 23.1% (95% confidence interval [CI] 20.6%–28.3%; I2 = 97.7%) with an increased overall risk of 2.7 (95% CI 2.09–3.6; I2 = 85.1%) compared with the general population.1 These estimates, however, varied considerably across studies depending on the ascertainment source (i.e., self-report vs screening tools vs structured clinical interviews), countries, regions, and settings. Regarding anxiety disorders, a meta-analysis of 27 studies in over 3,000 people with epilepsy showed a pooled prevalence of 20.2% (95% CI 15.3–26.0; I2 = 92.1), with generalized anxiety disorder being most common (10.2%; 95% CI 7.7%–13.5%).2 Another meta-analysis of 57 studies of psychosis and related disorders, including more than 40,000 subjects, showed a pooled prevalence of 5.6% (95% CI 4.8%–6.4%; I2 > 70%) in unselected individuals increasing to 7% (95% CI 4.9%–9.1%; I2 > 70%) in people with mesial TLE, with a pooled odds ratio (OR) for risk of psychosis compared with the general population of 7.8 (95% CI 2.8–21.8; I2 > 70%).3 The pooled prevalence of psychogenic nonepileptic seizures (PNES) in people with epilepsy in a meta-analysis was 12% (95% CI 10%–14%; I2 = 92.7%), whereas the prevalence of epilepsy in those with PNES was 22% (95% CI 20%–25%; I2 = 95.5%).4
Data from children with epilepsy are not different despite an obvious emphasis on developmental disorders. A population-based study in 85 children and adolescents (aged 5–15) with active epilepsy in England reported a prevalence of attention-deficit hyperactivity disorder (ADHD) of around 33%, autism spectrum disorder of 21%, depression of 7%, and anxiety of 13%.5 A nationwide Norwegian registry study in an unselected pediatric population of over 1,000,000 children reported developmental and psychiatric comorbidities in 43% of children with epilepsy, with overall ORs (compared with the general child population) of 10.7 (95% CI 9.5–12.1) for autism, 5.4 (95% CI 4.8–5.9) for ADHD, 2.3 (95% CI 1.8–3.0) for anxiety disorders, and 1.8 (95% CI 1.4–2.5) for depression.6 The use of the International Classification of Diseases (ICD) codes to identify psychiatric disorders in many of these studies introduces an important limitation as ICD codes have low sensitivity for psychiatric conditions, leading to possible underestimation of their occurrence. Still, the majority of studies included in these meta-analyses come from high-resource countries, whereas less than 10% are from medium- and low-resource countries. This is, however, a global issue in mental health as highlighted by the Mental Health Action Plan 2013–2020 developed by the World Health Organization.
Cross-sectional epidemiologic studies provide estimates of the size of the problem but do not help to clarify the nature of the association. Data from prospective observational studies clearly indicate that the relationship between epilepsy and psychiatric disorders is bidirectional. This notion was established over 10 years ago, and the majority of studies on this subject were published before 2013. More recent studies have further confirmed this observation. A large UK observational cohort study involving over 10,000,000 subjects found that depression was associated with a 2.5-fold (95% CI 2.49–2.60) increased risk of developing epilepsy.7 Suicide risk was increased 2.9 fold (95% CI 2.5–3.4) even before the diagnosis of epilepsy.8 All these findings suggest the presence of shared pathogenic mechanisms between epilepsy and all major psychiatric disorders. In the case of depression, potential mechanisms include hyperactivity of the hypothalamic-pituitary-adrenal axis as high cortisol levels can modulate the expression and composition of gamma-aminobutyric acid receptor A receptors, thereby increasing brain excitability and ultimately leading to epileptogenesis.9 It is also tempting to speculate that psychiatric disorders, in some cases, may represent the premorbid phase of some epileptic syndromes. This specific scenario may have major implications in terms of future treatments and the development of disease-modifying agents.
Implications for Clinical Practice
In epilepsy, treatment and prognosis are dependent on the accurate definition of the epilepsy syndrome. It would then be reasonable to apply the same model for psychiatric comorbidities (e.g., psychiatric disorders being more common in TLE compared with generalized syndromes). The relative contribution of syndrome-specific variables is still unclear, and clinical evidence suggests that psychiatric comorbidities do not necessarily respect such borders. It is now evident that psychiatric comorbidities have to be considered when informing people about the prospects of long-term prognosis of the epilepsy itself.
In people with epilepsy, psychiatric comorbidities have been historically associated with poor quality of life, but there are now data suggesting their role as a prognostic indicator. A population-based cohort study involving 10,595,709 people from the United Kingdom showed that depression is associated with high comorbidity rates, as measured by the Charlson Comorbidity Index, and that the severity of the depression itself (based on the type of treatment received) correlates with lower odds of achieving seizure remission in a Canadian cohort.7 Psychiatric comorbidities are associated with a high risk of side effects, especially cognitive complaints and psychiatric side effects.10 In fact, psychiatric comorbidities, particularly depression, represent an important cause of cognitive complaint.
Psychiatric comorbidities are associated with a 4-fold increased risk of drug resistance in focal11 and generalized epilepsies.12
The impact of psychiatric comorbidities in terms of seizure outcome and psychiatric outcome, in epilepsy surgery, is complex and yet to be established. Some studies have found a lower probability of achieving seizure freedom after temporal lobectomy,13 whereas others have refuted these findings.14 The same holds true for psychiatric outcomes, as some studies showed an increased risk of recurrence of depression or anxiety during the first year after surgery, whereas other studies showed long-term improvement.
Psychiatric comorbidities are associated with premature mortality in epilepsy.15 This may be due to a variety of reasons, including increased risk of substance or alcohol abuse, increased risk of injury, poor adherence to medications, and increased suicide rates. Data from a population-based study of over 57,000 people in Sweden showed that females with epilepsy and psychiatric comorbidities had a 5-fold increased risk of sudden unexpected death in epilepsy compared with those without such comorbidities.16
Last, it is evident that psychiatric comorbidities increase the global burden of epilepsy from a public health perspective with increased health costs. People with epilepsy and psychiatric disorders have high health resource utilization, including increased emergency department admissions and outpatient visits. Data from a US nationwide study assessing almost 400,000 hospital admissions showed that psychiatric comorbidities, depression, and psychosis, in particular, increase length of stay and inpatient costs for people with epilepsy.17
Screening for Psychiatric Comorbidities
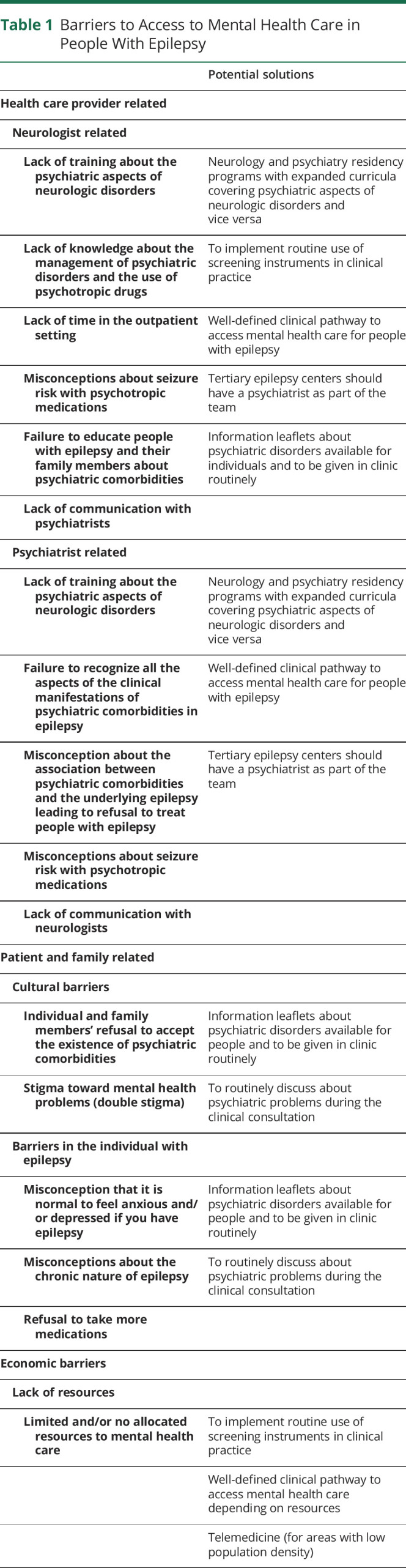
Despite robust evidence about the frequency and clinical implications of psychiatric disorders in epilepsy, these problems are still underdiagnosed and undertreated. Barriers to diagnosis and management of psychiatric comorbidities are complex and multifactorial. These include, among other factors, cultural barriers to mental health issues, lack of training of neurologists and psychiatrists about these comorbidities, and lack of allocated resources for a multidisciplinary approach (table 1).
Table 1.
Barriers to Access to Mental Health Care in People With Epilepsy
In the general population, a few screening tools are available in primary and secondary care settings for almost all major psychiatric conditions. These tools have been shown to be cost-effective because they are short, standardized against Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria, and less resource intensive than a full clinical interview. In the past, the validity of these instruments in people with epilepsy was a major barrier to their use in routine clinical practice. As described in this section, there are now good data on the validity of clinical instruments for depression and anxiety in adults and for ADHD in children.
A systematic review of studies validating 16 screening tools for depression in adults with epilepsy showed that the Neurological Disorders Depression Inventory for Epilepsy (NDDI-E), validated in 13 languages, is the most efficient and practical screening instrument for a major depressive episode in a variety of settings.18 The NDDI-E has also been validated for suicidality with good sensitivity and specificity,19 and this should allow the development of well-defined clinical pathways for suicide prevention.
Other well-known, self-rating scales such as the Beck Depression Inventory II (BDI-II) and the Patient Health Questionnaire 9 (PHQ-9) have also been shown to be valid in epilepsy but require use of cutoff scores higher than those adopted in the general population (general population BDI-II = 10, PHQ-9 = 5; epilepsy BDI-II = 15, PHQ-9 = 10).18 This can be partially explained by the heterogeneity of clinical presentations of depression in epilepsy, but also highlights the need to adapt these questionnaires to the specific needs of people with epilepsy to maximize their sensitivity and specificity.
The Hamilton Depression Rating Scale has been used as an outcome measure in clinical trials of depression outside epilepsy, and it has also been validated in epilepsy.20 This will allow the development of outcome studies of depression in people epilepsy whose results will be comparable to those from the general population.
Two main clinical instruments have been validated for symptoms of anxiety in adults with epilepsy: the Hospital Anxiety and Depression Scale (HADS) and the Generalized Anxiety Disorder 7 (GAD-7). Although studies on the validity of the HADS in epilepsy provide conflicting results, the validity and cost-effectiveness of the GAD-7 seem to be well established.21 Discrepancies among studies are due to the fluctuating nature of anxiety symptoms and the nonconforming phenomenology of psychiatric symptoms in epilepsy.
Data on screening instruments in children with epilepsy are still limited. A systematic review on the management of ADHD in epilepsy reported good evidence for the use of the Strength and Difficulties Questionnaire.22 Data on clinical instruments for depression and anxiety in the pediatric population are scant. A 12-item, self-report screening tool for depression in people with epilepsy aged 12–17 years, called NDDI-E-Youth, has been developed,23 but further studies in this area are needed.
Diagnostic Issues
After a positive screen, it is important to confirm the diagnosis, as psychiatric symptoms can be seen in a variety of clinical scenarios including peri-ictal symptoms, side effects of drugs, or comorbid psychiatric disorders. The boundaries between these scenarios are often blurred, and, as already discussed, people with a psychiatric comorbidity are also more likely to present with psychiatric side effects from antiseizure medications.
Historically, psychiatric symptoms in epilepsy have been categorized according to their temporal relationship with seizures, and the practicality of this is well known as they define different clinical scenarios, which are summarized in table 2.
Table 2.
Classification of Psychiatric Symptoms According to Their Temporal Relation With Seizures

The prevalence and pathophysiology of peri-ictal symptoms are largely unknown, and data come from adult samples. Postictal psychoses are probably the most frequently described and investigated symptom pattern, and a meta-analysis reported a point prevalence of 2% (95% CI 1.2%–2.8%).3 Postictal psychoses are typically seen in people with TLE, and they are characterized by higher rates of violent behaviors and suicide attempts than interictal psychoses.24 Conversely, nonpsychotic postictal psychiatric symptoms are often not recognized, in large part because they are short-lasting and clinicians fail to investigate their presence. In a systematic study of people with drug-resistant focal epilepsy, 43% had postictal symptoms of depression, 45% postictal anxiety, and 7% psychotic symptoms. These occurred in more than half of their seizures and lasted for a median of 24 hours.25
Psychiatric symptoms as side effects of antiseizure medications are frequently reported. A retrospective analysis of medical notes of a large unselected sample from the United States including 4,085 adults recently started on antiseizure medications showed that 1 in 6 individuals with epilepsy develops drug-related psychiatric side effects.26 Sodium channel blockers seem to be less frequently associated with psychiatric side effects,26 but there are no robust head-to-head trials providing strong evidence for that. For this reason, clinicians should bear in mind that psychiatric side effects can happen with any drug in predisposed individuals, such as those with psychiatric comorbidities. Forced normalization is an intriguing phenomenon characterized by the emergence of psychiatric disturbances following the establishment of seizure control or reduction in the epileptic activity in a patient with previous uncontrolled epilepsy. The pathophysiology remains uncertain, but a recent systematic review pointed out that antipsychotic drug use does not predict complete resolution of psychiatric symptoms in comparison with antiepileptic drug withdrawal suggesting a connection with the mechanism underlying seizure control.27
The Food and Drug Administration has issued a black box warning on all antiseizure medications for increased suicidality rates. An International League Against Epilepsy (ILAE) document has discussed limitations of the Food and Drug Administration meta-analysis on which the black box warning was based, and it has emphasized the need for continuous screening and identification of high-risk individuals to develop prevention strategies.28 Psychiatric side effects of antiseizure medications reported with a prevalence higher than 1% are summarized in table 3.
Table 3.
Common Psychiatric Side Effects of Antiseizure Medications
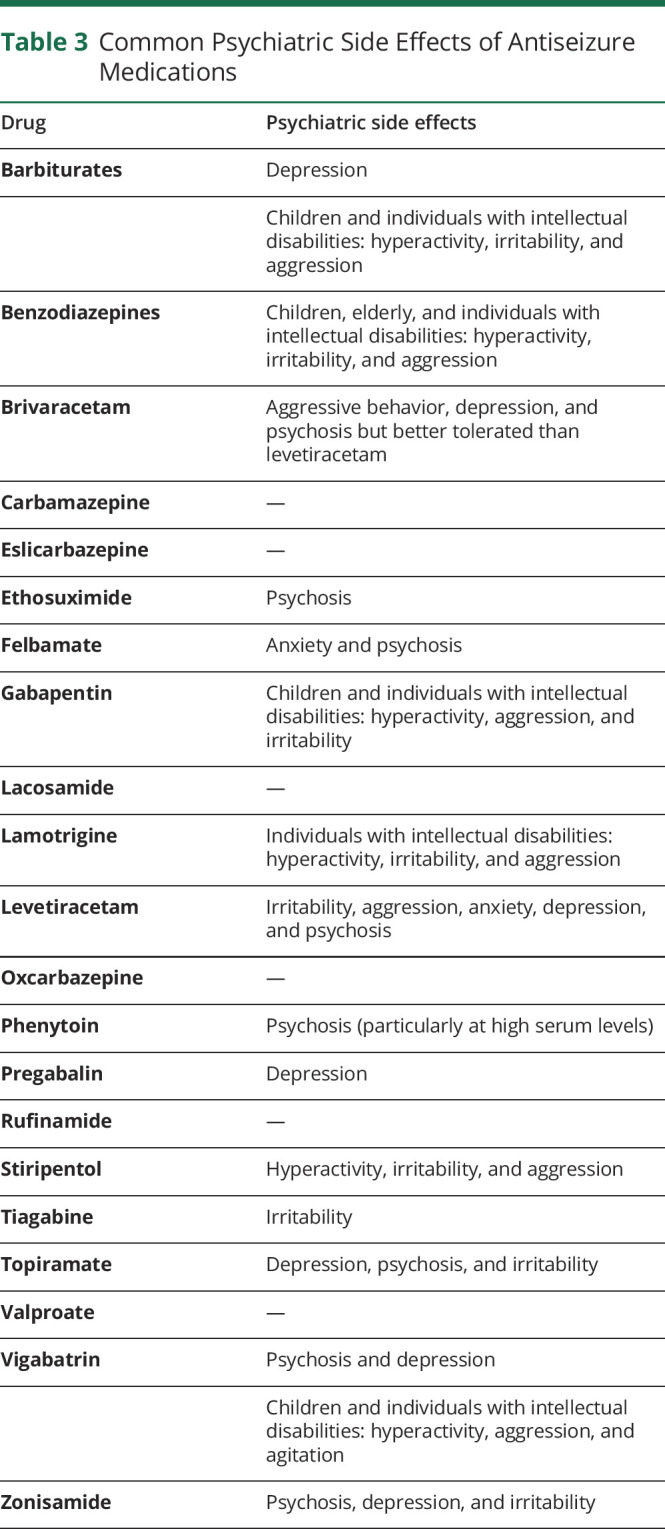
Last, the clinical presentation of psychiatric comorbidities has itself been a matter of debate.29 In fact, people with epilepsy can develop psychiatric disorders clinically identical to those of individuals without epilepsy, but it is also established that some develop psychiatric syndromes characterized by unusual features nonadequately captured by classificatory systems such as DSM and ICD (table 2). Psychiatric presentations can be atypical and sometimes challenging in people with intellectual disabilities, where also the pattern of psychiatric side effects of antiseizure medications can be different (table 3).
Treatment Issues
Full remission should always be the ultimate goal of the treatment of any psychiatric comorbidity in epilepsy. As discussed in this section, current evidence on the management of psychiatric comorbidities in epilepsy is limited. There is, however, no reason to consider that guidelines of treatment for psychiatric disorders may not be valid in epilepsy. It seems reasonable, therefore, to follow standard practice bearing in mind the individualities of people with epilepsy, especially drug interactions and risk of seizures (table 4).
Table 4.
Management of Psychiatric Comorbidities in Epilepsy

Psychological Interventions
In the general population, psychological interventions are the first-line treatment for all anxiety disorders and for mild to moderate depression. It is reasonable to apply this guidance also to people with epilepsy, but the evidence is still limited. A recent ILAE report supported psychological interventions, especially cognitive behavioral therapy, in people with epilepsy and mild to moderate depressive symptoms, although again the evidence level is moderate.30
Psychoeducation and psychological interventions still represent first-line treatments for PNES.31 No studies have specifically addressed the management of PNES in people with epilepsy, but it is obvious that explaining the diagnosis and educating individuals and caregivers about the differences between epilepsy and PNES are extremely important.
Pharmacologic Treatments
In the general population, antidepressants are used in moderate to severe depression and in all anxiety disorders in combination with psychological interventions. A Cochrane review on antidepressants in epilepsy has, however, shown a low level of evidence due to the poor quality of studies.32 There are only 2 placebo-controlled trials and several open studies of antidepressants including sertraline, citalopram, fluoxetine, reboxetine, and mirtazapine.33 These studies clearly suggest that selective serotonin reuptake inhibitors (SSRIs) and newer antidepressants are safe and effective in epilepsy, but they are limited by the relatively small size and the inclusion of people with different epilepsy types (from newly diagnosed to those with drug-resistant epilepsy). These limitations probably explain the heterogeneous response rates, ranging from 24% to 97%.33 Citalopram and sertraline are usually considered first-line treatments for depression in the context of a chronic health condition, and given available data, this is a sound option in people with epilepsy and depression.
There seem to be no studies examining the effectiveness of drug treatments for anxiety disorders in epilepsy, but SSRIs are usually considered first-line treatment when a pharmacologic treatment is needed.
Regarding antipsychotics, the evidence is also scant. Risperidone, olanzapine, and quetiapine are usually considered first-line treatments in first-episode psychosis.34 Postictal psychoses represent an epilepsy-specific problem, and for this reason, evidence is less compelling, and it is not possible to apply evidence from elsewhere. Historically, a combination of benzodiazepines (i.e., clobazam) and atypical antipsychotics is often used.34
There are no studies on the use of antipsychotics in people with challenging behavior, autism, and epilepsy. Trials in persons with intellectual disabilities and challenging behavior or autism without epilepsy seem to favor risperidone.35
The level of evidence is higher for treatment of ADHD in epilepsy than for other psychiatric comorbidities, despite the limited number of studies. A systematic review showed response rates for methylphenidate in children with ADHD and epilepsy between 65% and 83%.22 Data on atomoxetine and amphetamines are available only at the anecdotal level.
Interactions
Old antiseizure medications such as carbamazepine, phenytoin, and barbiturates induce drug-metabolizing enzymes such as the cytochromes P450 and the uridine 5'-diphospho-glucuronosyltransferase systems, whereas valproate is an inhibitor. Among newer drugs, oxcarbazepine is a weak inducer and topiramate is an inducer at daily doses over 200 mg, whereas other newer drugs are less likely to be culprits for drug interactions.36,37
Antidepressants are extensively metabolized by multiple systems, and this can potentially lead to interactions.36 Regarding tricyclics, dosage adjustments with inducers should be considered on an individual basis, and this is due to a number of pharmacokinetic reasons including the large therapeutic window of this class of antidepressants and the concomitant increase in the free fraction due to a concomitant protein binding displacement interaction.37 Inducers reduce the levels of SSRIs by around a quarter, but again systematic dose adjustments in routine clinical practice are not needed.37 Fluoxetine, fluvoxamine, and, to a lesser extent, sertraline inhibit the CYP2C9, and this can possibly increase the levels of phenytoin and, to a lesser extent, valproate.36,37 Inducers like carbamazepine decrease the blood levels of bupropion by 90% making this interaction clinically relevant.36
All enzyme-inducing drugs reduce antipsychotic blood levels, but this is markedly important for quetiapine; for instance, its use with carbamazepine is associated with undetectable levels of the antipsychotic drug even at a dose of 700 mg.37 There is no evidence that antipsychotics affect the blood levels of epilepsy medications.
Data on potential interactions of methylphenidate are limited to older compounds, but there is no evidence of clinically relevant interactions.
Pharmacodynamic interactions are rarely systematically investigated, but they can affect adherence and successful response to treatment. They are usually classified into positive and negative interactions. Positive interactions include synergistic or additive treatment effects such as the combination of SSRIs and pregabalin in some anxiety disorders.38 Negative interactions include, for example, the amplification of potential side effects by the combination of 2 medications, and these can be sedation, weight gain, sexual dysfunction, hyponatremia, osteopenia, and heart problems. For these reasons, neurologists need to familiarize themselves with the spectrum of side effects of psychotropic medications, in particular antidepressants.36
Seizure risk
Historically, psychotropic drugs were thought to be associated with an increased risk of seizures, and this is reported in the information leaflet of many psychotropic medications from antidepressants to antipsychotics. This, however, has never been based on any robust clinical evidence. Conversely, the analysis of seizure incidence in phase II–III studies of psychotropic drugs approved by the Food and Drug Administration between 1985 and 2004 involving over 75,000 individuals showed that seizure incidence was not different from that of placebo. The only exception was for high-dose clomipramine (>150 mg), which showed a standardized incidence ratio of 4 (95% CI 2.6–6.0).39
Regarding psychostimulants, a Swedish study involving more than 21,000 children with seizures showed no increased risk of seizures from ADHD medications,40 and this has been also endorsed by a recent ILAE consensus report.22
Regarding antipsychotic drugs, clozapine has the highest risk of seizures compared with placebo with a standardized incident ratio of 9.5 (95% CI 7.2–12.2).39 Olanzapine and quetiapine carry also some risk but to a lesser extent, whereas all other antipsychotics are no different from placebo.39
The risk of seizures with clozapine is dose and titration dependent, although in people with epilepsy, seizure aggravation can be observed even at low doses.
Nonetheless, it is still unknown whether all these data coming from the psychiatric realm can be directly transferred to people with epilepsy and psychiatric comorbidities. The few available open studies in epilepsy previously mentioned do not suggest deterioration in seizure frequency on a stable epilepsy drug regime.
Drug-related seizures are a complex problem, and it is not just restricted to psychotropic medications. There is no doubt, however, that the incorrect overestimation of the risk of seizures with psychotropic medications has had a deleterious impact on access to proper treatment in people with epilepsy and psychiatric comorbidities.
Psychiatric disorders are a relatively frequent comorbidity in people with epilepsy, and they need to be an integral part of the management. For this reason, epilepsy clinics should have a clear pathway for access to mental health care. There are now several screening instruments, which can be adopted in routine clinical practice even in resource-poor settings. In the absence of epilepsy-specific guidelines, internationally adopted guidelines concerning the treatment and management of primary psychiatric disorders should be adopted, taking into account the peculiarities of people with epilepsy.
Future studies need to clarify whether these disorders are mediators or moderators of seizure outcome; that is, are psychiatric disorders merely indicators of poor prognosis or can their early identification and prompt treatment have an impact on the prognosis of the epilepsy itself?
High-quality outcome studies for major psychiatric comorbidities such as mood, anxiety disorders, and psychoses in people with epilepsy are needed to develop evidence-based treatment strategies.
Acknowledgment
N. Jetté receives research grant funding from the NINDS (NIH U24NS107201 and NIH IU54NS100064) and PCORI paid to her center for work unrelated to this article. J.W. Sander is based at NIHR University College London Hospitals Biomedical Research Centre, which receives a proportion of funding from the UK Department of Health's Research Centres funding scheme. He also receives research support from the Marvin Weil Epilepsy Research Fund, the UK Epilepsy Society, and the Christelijke Vereniging voor de Verpleging van Lijders aan Epilepsie, The Netherlands. M. Mula and A.M. Kanner report no additional funding.
Appendix. Authors
References
- 1.Fiest KM, Dykeman J, Patten SB, et al. Depression in epilepsy: a systematic review and meta-analysis. Neurology 2013;80:590–599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Scott AJ, Sharpe L, Hunt C, Gandy M. Anxiety and depressive disorders in people with epilepsy: a meta-analysis. Epilepsia 2017;58:973–982. [DOI] [PubMed] [Google Scholar]
- 3.Clancy MJ, Clarke MC, Connor DJ, Cannon M, Cotter DR. The prevalence of psychosis in epilepsy; a systematic review and meta-analysis. BMC Psychiatry 2014;14:75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kutlubaev MA, Xu Y, Hackett ML, Stone J. Dual diagnosis of epilepsy and psychogenic nonepileptic seizures: systematic review and meta-analysis of frequency, correlates, and outcomes. Epilepsy Behav 2018;89:70–78. [DOI] [PubMed] [Google Scholar]
- 5.Reilly C, Atkinson P, Das KB, et al. Neurobehavioral comorbidities in children with active epilepsy: a population-based study. Pediatrics 2014;133:e1586–e1593. [DOI] [PubMed] [Google Scholar]
- 6.Aaberg KM, Bakken IJ, Lossius MI, et al. Comorbidity and childhood epilepsy: a nationwide registry study. Pediatrics 2016;138:e20160921. [DOI] [PubMed] [Google Scholar]
- 7.Josephson CB, Lowerison M, Vallerand I, et al. Association of depression and treated depression with epilepsy and seizure outcomes: a multicohort analysis. JAMA Neurol 2017;74:533–539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hesdorffer DC, Ishihara L, Webb DJ, Mynepalli L, Galwey NW, Hauser WA. Occurrence and recurrence of attempted suicide among people with epilepsy. JAMA Psychiatry 2016;73:80–86. [DOI] [PubMed] [Google Scholar]
- 9.MacKenzie G, Maguire J. Chronic stress shifts the GABA reversal potential in the hippocampus and increases seizure susceptibility. Epilepsy Res 2015;109:13–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Stephen LJ, Wishart A, Brodie MJ. Psychiatric side effects and antiepileptic drugs: observations from prospective audits. Epilepsy Behav 2017;71:73–78. [DOI] [PubMed] [Google Scholar]
- 11.Nogueira MH, Yasuda CL, Coan AC, Kanner AM, Cendes F. Concurrent mood and anxiety disorders are associated with pharmacoresistant seizures in patients with MTLE. Epilepsia 2017;58:1268–1276. [DOI] [PubMed] [Google Scholar]
- 12.Stevelink R, Koeleman BPC, Sander JW, Jansen FE, Braun KPJ. Refractory juvenile myoclonic epilepsy: a meta-analysis of prevalence and risk factors. Eur J Neurol 2019;26:856–864. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bell GS, de Tisi J, Gonzalez-Fraile JC, et al. Factors affecting seizure outcome after epilepsy surgery: an observational series. J Neurol Neurosurg Psychiatry 2017;88:933–940. [DOI] [PubMed] [Google Scholar]
- 14.Altalib HH, Berg AT, Cong X, et al. Presurgical depression and anxiety are not associated with worse epilepsy surgery outcome five years postoperatively. Epilepsy Behav 2018;83:7–12. [DOI] [PubMed] [Google Scholar]
- 15.Fazel S, Wolf A, Långström N, Newton CR, Lichtenstein P. Premature mortality in epilepsy and the role of psychiatric comorbidity: a total population study. Lancet Lond 2013;382:1646–1654. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Sveinsson O, Andersson T, Carlsson S, Tomson T. The incidence of SUDEP: a nationwide population-based cohort study. Neurology 2017;89:170–177. [DOI] [PubMed] [Google Scholar]
- 17.Patel RS, Elmaadawi A, Mansuri Z, Kaur M, Shah K, Nasr S. Psychiatric comorbidities and outcomes in epilepsy patients: an insight from a nationwide inpatient analysis in the United States. Cureus 2017;9:e1686. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Gill SJ, Lukmanji S, Fiest KM, Patten SB, Wiebe S, Jetté N. Depression screening tools in persons with epilepsy: a systematic review of validated tools. Epilepsia 2017;58:695–705. [DOI] [PubMed] [Google Scholar]
- 19.Mula M, McGonigal A, Micoulaud-Franchi JA, May TW, Labudda K, Brandt C. Validation of rapid suicidality screening in epilepsy using the NDDIE. Epilepsia 2016;57:949–955. [DOI] [PubMed] [Google Scholar]
- 20.Mula M, Iudice A, La Neve A, et al. Validation of the Hamilton Rating Scale for depression in adults with epilepsy. Epilepsy Behav 2014;41:122–125. [DOI] [PubMed] [Google Scholar]
- 21.Fiest KM, Patten SB, Jetté N. Screening for depression and anxiety in epilepsy. Neurol Clin 2016;34:351–361. [DOI] [PubMed] [Google Scholar]
- 22.Auvin S, Wirrell E, Donald KA, et al. Systematic review of the screening, diagnosis, and management of ADHD in children with epilepsy. Consensus paper of the Task Force on Comorbidities of the ILAE Pediatric Commission. Epilepsia 2018;59:1867–1880. [DOI] [PubMed] [Google Scholar]
- 23.Wagner JL, Kellermann T, Mueller M, et al. Development and validation of the NDDI-E-Y: a screening tool for depressive symptoms in pediatric epilepsy. Epilepsia 2016;57:1265–1270. [DOI] [PubMed] [Google Scholar]
- 24.Hilger E, Zimprich F, Pataraia E, et al. Psychoses in epilepsy: a comparison of postictal and interictal psychoses. Epilepsy Behav 2016;60:58–62. [DOI] [PubMed] [Google Scholar]
- 25.Kanner AM, Soto A, Gross-Kanner H. Prevalence and clinical characteristics of postictal psychiatric symptoms in partial epilepsy. Neurology 2004;62:708–713. [DOI] [PubMed] [Google Scholar]
- 26.Chen B, Choi H, Hirsch LJ, et al. Psychiatric and behavioral side effects of antiepileptic drugs in adults with epilepsy. Epilepsy Behav 2017;76:24–31. [DOI] [PubMed] [Google Scholar]
- 27.Calle-López Y, Ladino LD, Benjumea-Cuartas V, Castrillón-Velilla DM, Téllez-Zenteno JF, Wolf P. Forced normalization: a systematic review. Epilepsia 2019;60:1610–1618. [DOI] [PubMed] [Google Scholar]
- 28.Mula M, Kanner AM, Schmitz B, Schachter S. Antiepileptic drugs and suicidality: an expert consensus statement from the Task Force on Therapeutic Strategies of the ILAE Commission on Neuropsychobiology. Epilepsia 2013;54:199–203. [DOI] [PubMed] [Google Scholar]
- 29.Mula M. The interictal dysphoric disorder of epilepsy: legend or reality? Epilepsy Behav 2016;58:7–10. [DOI] [PubMed] [Google Scholar]
- 30.Michaelis R, Tang V, Goldstein LH, et al. Psychological treatments for adults and children with epilepsy: evidence-based recommendations by the international league against epilepsy psychology task force. Epilepsia 2018;59:1282–1302. [DOI] [PubMed] [Google Scholar]
- 31.Gasparini S, Beghi E, Ferlazzo E, et al. Management of psychogenic non-epileptic seizures: a multidisciplinary approach. Eur J Neurol 2019;26:205–e15. [DOI] [PubMed] [Google Scholar]
- 32.Maguire MJ, Weston J, Singh J, Marson AG. Antidepressants for people with epilepsy and depression. Cochrane Database Syst Rev 2014:CD010682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Mula M, Sander JW. Current and emerging drug therapies for the treatment of depression in adults with epilepsy. Expert Opin Pharmacother 2019;20:41–45. [DOI] [PubMed] [Google Scholar]
- 34.Agrawal N, Mula M. Treatment of psychoses in patients with epilepsy: an update. Ther Adv Psychopharmacol 2019;9:2045125319862968. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Kerr M, Linehan C, Brandt C, et al. Behavioral disorder in people with an intellectual disability and epilepsy: a report of the Intellectual Disability Task Force of the Neuropsychiatric Commission of ILAE. Epilepsia Open 2016;1:102–111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Italiano D, Spina E, de Leon J. Pharmacokinetic and pharmacodynamic interactions between antiepileptics and antidepressants. Expert Opin Drug Metab Toxicol 2014;10:1457–1489. [DOI] [PubMed] [Google Scholar]
- 37.Mula M. The pharmacological management of psychiatric comorbidities in patients with epilepsy. Pharmacol Res 2016;107:147–153. [DOI] [PubMed] [Google Scholar]
- 38.Baldwin DS, Anderson IM, Nutt DJ, et al. Evidence-based pharmacological treatment of anxiety disorders, post-traumatic stress disorder and obsessive-compulsive disorder: a revision of the 2005 guidelines from the British Association for Psychopharmacology. J Psychopharmacol 2014;28:403–439. [DOI] [PubMed] [Google Scholar]
- 39.Alper K, Schwartz KA, Kolts RL, Khan A. Seizure incidence in psychopharmacological clinical trials: an analysis of Food and Drug Administration (FDA) summary basis of approval reports. Biol Psychiatry 2007;62:345–354. [DOI] [PubMed] [Google Scholar]
- 40.Brikell I, Chen Q, Kuja-Halkola R, et al. Medication treatment for attention-deficit/hyperactivity disorder and the risk of acute seizures in individuals with epilepsy. Epilepsia 2019;60:284–293. [DOI] [PMC free article] [PubMed] [Google Scholar]
Study Funding
No targeted funding declared.
Disclosure
M. Mula reports personal fees from UCB, Eisai, Bial, and Elsevier, outside the submitted work; in addition, he also has intellectual property rights with Springer and Elsevier, and he is Associate Editor of Epilepsy & Behavior. A.M. Kanner reports personal fees from Eisai and Frontline Medical Communications, outside the submitted work. N. Jetté received an annual honorarium for her work as Associate Editor of Epilepsia and is a member of the Editorial Board of Neurology. J.W. Sander reports personal fees from Eisai, UCB, and Zogenix and grants from Eisai, UCB, NEF, and GW Pharma, outside the submitted work; he is a member of the Editorial Board of the Lancet Neurology. Full disclosure form information provided by the authors is available with the full text of this article at Neurology.org/cp.