

Abstract
Aging into later life is often accompanied by social disconnection, anxiety, and sadness. Negative emotions are self-focused states with detrimental effects on aging and longevity. Awe—a positive emotion elicited when in the presence of vast things not immediately understood—reduces self-focus, promotes social connection, and fosters prosocial actions by encouraging a “small self.” We investigated the emotional benefits of a novel “awe walk” intervention in healthy older adults. Sixty participants took weekly 15-minute outdoor walks for eight weeks; participants were randomly assigned to an awe walk group, which oriented them to experience awe during their walks, or to a control walk group. Participants took photographs of themselves during each walk and rated their emotional experience. Each day, they reported on their daily emotional experience outside of the walk context. Participants also completed pre- and post-intervention measures of anxiety, depression, and life satisfaction. Compared to participants who took control walks, those who took awe walks experienced greater awe during their walks and exhibited an increasingly “small self” in their photographs over time. They reported greater joy and prosocial positive emotions during their walks and displayed increasing smile intensity over the study. Outside of the walk context, participants who took awe walks reported greater increases in daily prosocial positive emotions and greater decreases in daily distress over time. Post-intervention anxiety, depression, and life satisfaction did not change from baseline in either group. These results suggest cultivating awe enhances positive emotions that foster social connection and diminishes negative emotions that hasten decline.
Keywords: social connection, compassion, positive emotion, exercise, outdoors
Positive emotions not only feel good but also promote social connection, a crucial component of successful aging (Cacioppo & Cacioppo, 2014; Ong, Uchino, & Wethington, 2016). Although aging has been associated with affective advantages including elevated positivity and better emotion regulation (Carstensen et al., 2011; Mather & Carstensen, 2005; Shiota & Levenson, 2009), these benefits often stabilize, and then decline, beginning in the seventh decade of life (Carstensen et al., 2011). After age 75, negative states such as sadness, fear, anxiety, and loneliness rise in robust fashion and can supplant positive emotions in daily life (Hawkley, Wroblewski, Kaiser, Luhmann, & Schumm, 2019). Sustained negative emotions are especially detrimental for older adults and are associated with higher rates of social isolation, depression, cognitive impairment, cardiovascular disease, and mortality (Cacioppo & Cacioppo, 2018; Cacioppo & Hawkley, 2009; Golden et al., 2009; Kassem et al., 2017; Kubzansky & Kawachi, 2000; Luo, Hawkley, Waite, & Cacioppo, 2012; Mehta et al., 2007; Valtorta, Kanaan, Gilbody, & Hanratty, 2018). These studies suggest that in aging, a paucity of positive emotions and reduced feelings of social connection can hasten cognitive impairment, physical decline, and even death (Byers, Yaffe, Covinsky, Friedman, & Bruce, 2010; Cacioppo et al., 2002; de Koning, Richards, & Stathi, 2019; O’Luanaigh et al., 2012).
What might counter these trends in later life? One candidate is awe. Awe is a positive emotion that people feel when they are in the presence of something vast that they cannot immediately understand (Keltner & Haidt, 2003). The sources of awe are myriad and include nature, art, music, collective action (e.g., a ceremony, political march, or concert), and the courage and magnanimity of others (Bai et al., 2017; Gordon et al., 2017). Individuals who readily experience awe tend to be more curious (Anderson, Dixson, Monroy, & Keltner, 2019) and more open to new ideas (Danvers & Shiota, 2017; Stancato & Keltner, 2019) than those who are less awe-prone. Even brief experiences of awe yield a host of benefits including an expanded sense of time and enhanced feelings of generosity, well-being, and humility (Anderson, Monroy, & Keltner, 2018; Piff, Dietze, Feinberg, Stancato, & Keltner, 2015; Rudd, Vohs, & Aaker, 2012; Stellar et al., 2018). The physical and emotional benefits of spending time outdoors—which include reductions in anxiety, depression, cortisol, inflammation, and cardiovascular risk (Mao et al., 2017; Stellar et al., 2015; Williams, 2017)—may also be mediated, in part, by experiences of awe (Anderson et al., 2018).
In addition to shaping the subjective experience of individuals, awe also has powerful effects on social relationships. Feelings of awe help us to put our problems into perspective and to prioritize the needs of the collective above our own. By shifting attention away from the self and onto the outside world, awe diminishes feelings of self-importance and makes people feel smaller, yet more connected, to a larger community and purpose (Horberg, Oveis, & Keltner, 2011; Keltner & Haidt, 2003; Piff et al., 2015). Elevated feelings of social connection, in turn, may help to elevate prosocial positive emotions such as compassion, admiration, and gratitude, emotions that draw us toward others, encourage interpersonal engagement, and foster empathy (Algoe, Fredrickson, & Gable, 2013; Goetz, Keltner, & Simon-Thomas, 2010). Elevating prosocial positive emotions in people as they age by promoting awe may help to counteract the feelings of isolation and disconnection that often shape the later years of life.
In the present study, we developed a novel intervention to promote experiences of awe in healthy older adults via “awe walks.” Previous intervention studies designed to increase positive emotions have used a variety of approaches, including loving kindness meditation (Fredrickson, Cohn, Coffey, Pek, & Finkel, 2008), gratitude journals (Emmons & McCullough, 2003), and acts of kindness (Buchanan & Bardi, 2010). These studies have shown that even simple experimental manipulations can elevate positive feelings and enhance well-being and mood, among other advantageous outcomes (Bolier et al., 2013). Typically, the mental and physical health improvements these interventions yield emerge over time and increase with practice (Fredrickson et al., 2008). We expected that awe, just like other positive states, could be nurtured and cultivated and be associated with other benefits.
We recruited healthy older adults and randomly assigned them to either an “awe walk” or a “control walk” group. All participants were instructed to take weekly 15-minute outdoor walks for eight weeks. Whereas participants in the control walk group received no additional instructions, those in the awe walk group were taught how to orient their walks to experience awe by tapping into their sense of wonder and walking in new locales, if possible. Although we anticipated both groups might experience benefits from regular exercise (Colcombe & Kramer, 2003; Voss et al., 2013), we expected that participants who took awe walks would, by design, experience greater awe during their walks than those who took control walks. We further tested whether elevated awe during the walks would be accompanied by a “small self” (Bai et al., 2017; Piff et al., 2015), which we operationalized here as the extent to which they filled photographs that they submitted from their walks with their own face and body versus the background scenery. We also examined whether other positive emotions increased during the walks and whether these gains would be reflected in greater smile intensity, which we coded in participants’ facial expressions in the photographs. Our primary hypotheses were that awe walks would produce momentary alterations in emotional experience during the walks and would also encourage beneficial affective shifts outside of the walk context. Given that awe fosters social connection, humility, and kindness (Piff et al., 2015; Stellar et al., 2018), we anticipated that participants who took awe walks would experience greater increases in their daily experience of prosocial positive emotions, such as compassion (Goetz et al., 2010), and report greater feelings of connectedness with the world around them than those who took control walks. We also expected that participants in the awe walk group might experience greater decreases in daily negative emotions, such as sadness and fear, over the study than those in the control walk group.
Methods
Power Analyses
Standard power analyses were performed with GLIMMPSE (Kreidler et al., 2013), a program recommended for repeated measures power analyses (Guo, Logan, Glueck, & Muller, 2013), to detect the effects of interest at 80% power (α=.05). Our primary analysis examined whether there was a group by time interaction on daily prosocial positive emotions. To provide estimates for the effect size and standard deviation of this measure, we referred to Fredrickson et al. (2008), a positive emotion intervention study with a similar design and time course. Although there are some differences between our studies that could have influenced expected effect sizes (e.g., they used a waitlist control where we used an active walk control condition), we thought this study offered a reasonable estimate for a group by time interaction effect size, which they reported as 0.026 with a standard deviation of 0.15 units. We anticipated a similar effect size for the group by time interaction in our study and, thus, entered expected mean values for daily prosocial positive emotions in the awe walk group that increased by 0.026 units each week (with the mean of the control walk group staying constant across the weeks). Previous studies have found a moderate degree of consistency in self-reported experience over time, and, therefore, we entered 0.6 as the within-subject correlation for emotional experience, which is in the range of previous experience sampling studies (Seidlitz, Fujita, & Duberstein, 2000). We entered eight repeated measures because we anticipated participants would complete a minimum of one daily survey per week of the eight-week study (in actuality, participants completed an average of 46 daily surveys over the study with a range of 9 – 59). The values we entered in the power analysis, therefore, were an underestimation of our actual number of repeated measures. The power analysis for daily prosocial positive emotions revealed that a total sample size of 42 (21 per group) was needed to detect a significant interaction. Thus, we recruited 60 participants to ensure adequate power while accounting for potential attrition during the study. It should be noted that during the study design phase, we initially conducted a different power analysis that was based on a more complex data analytic strategy and a more conservative estimate of the number of repeated measures that we would collect; this initial power analysis also indicated a sample of comparable size would provide us with adequate power to detect the desired effects in our variables of interest over time. After we completed our data collection, we conducted an additional post hoc power analysis to test whether we had adequate power to detect between-group differences with the 52 participants included in our analyses. This power analysis indicated that with 24 participants in the awe walk group and 28 participants in the control walk group, we had 80% power (α=.05) to detect a large effect size (Cohen’s d=.92) between the groups using a two-sample t-test.
Participants
Healthy older participants between the ages of 60 and 90 were invited to participate in a study about health and emotions. Participants were volunteers recruited from the community who were followed by the Hillblom Healthy Aging Network at the University of California, San Francisco (UCSF). Participants underwent an extensive interdisciplinary diagnostic work-up that included a neurological exam, neuropsychological testing (Kramer et al., 2003), magnetic resonance imaging, and informant interview (Morris, 1993). Based on this assessment, all participants were determined to be cognitively intact, functionally normal, and free of current and previous neurological and psychiatric disorders.
The study procedures were approved by the UCSF Committee on Human Research. The study was registered as a clinical trial: https://www.clinicaltrials.gov/ct2/show/NCT03550144?term=awe&rank=1, and no methodological changes were made once the study commenced. We have reported all measures, conditions, and data exclusions in this study. The participants were financially compensated for completing each survey. Participants received $20 for completing the pre- and post-intervention questionnaires and $2 for each daily survey. Data generated by the UCSF Memory and Aging Center are available upon request.
Procedure
During the pre-intervention baseline assessment, participants completed questionnaires and an in-person laboratory-based assessment of emotion at UCSF (these data were not analyzed here). Participants completed these questionnaires again three and six months after completing the eight-week walk study, but these data were not included in the present study.
At UCSF, the study coordinator used Google’s random number generator to assign each participant randomly to the awe walk group or the control walk group. Participants were blind to their group assignment and did not know the instructions provided to the other group. The study coordinator explained the instructions to each participant and provided a summary handout to take home (see Supplemental Information).
Participants in both groups were instructed to take weekly 15-minute walks for eight weeks. In contrast to a waitlist control, which is a common comparison for positive emotion intervention studies (Bolier et al., 2013), we used a walk as our comparison condition, which was a tight, active control that allowed us to isolate the benefits that awe walks conferred above and beyond walks in general. All participants were asked to take the walks alone in any outdoor setting (urban or rural) and to maintain a light to moderate pace (Borg, 1982). They were encouraged to refrain from using their phones during the walks except to take photographs. To facilitate experiences of awe, participants in the awe walk group were also told that “with the right outlook, awe can be found almost anywhere, but it is most likely to occur in places that involve two key features: physical vastness and novelty.” They were asked to tap into their sense of wonder and to go somewhere new each week, if possible (see Supplemental Information for detailed instructions for both groups).
Measures
Walk Surveys.
Participants completed a brief “walk survey” about each walk.
Emotional Experience.
After each walk, participants reported on the emotions they experienced during the walk. They rated their experience of a wide range of emotions (i.e., awe, wonder, amazement, admiration, amusement, anger, annoyance, appreciation, anxiety, calm, compassion, contentment, fear, gratitude, happiness, joy, pride, sadness, relaxed, and warmth) on a 7-point Likert scale (1=not at all, 4=a little, 7=a lot). They were also asked the following questions: “To what extent did you feel part of something larger than yourself during your walk?”; “To what extent did you feel small during your walk?”; “To what extent did you feel in the presence of something vast during your walk?”; “To what extent did you feel as if your worries and concerns were insignificant during your walk?”. They responded on a 7-point Likert scale (1=not at all, 4=a little, 7=a lot).
Walk Characteristics.
Participants recorded the duration and distance of each walk and rated how urban (1=not urban to 5=very urban), beautiful (1=aesthetically unpleasant to 7=aesthetically pleasant), and strenuous (6=very, very light to 20=very, very hard) they perceived the walk to be. They also recorded if they had walked with other people (and, if so, how many and how much emotional support they had received from them) or pets, and they responded to the following open-ended questions: “Please describe where you walked” and “What did you think about during your walk today?”.
Walk Photographs.
When completing each walk, participants took three photographs of themselves (before, during, and after each walk). They also took a photo of the most awe-inspiring thing they saw on their walk (for the awe walk group) or the most interesting thing they saw on their walk (for the control walk group); these scenery photographs, however, were not analyzed as a part of the present study. Later, they uploaded their photographs online when completing the walk survey. We used the photographs that participants took of themselves to extract two behavioral measures that were relevant to our study hypotheses.
Self-Size.
We first used the photographs to extract a measure of “self-size,” the proportion of space participants filled with their own face and body in the photographs, which would allow us to look for additional evidence of a “shrinking” self in the awe walk group. To quantify self-size, we outlined the participant’s silhouette in each photograph. Photographs were then imported into Matlab (version 2017b) with the Image Processing Toolbox and binarized into black (“self”) and white (“non-self”) pixels. Self-size was quantified by dividing the number of “self” pixels by the total number of pixels in the image.
Smile Intensity.
We next coded participants’ smiles in their photographs with the goal of finding convergent, objective evidence of greater positive emotional gains in the awe walk group. Coders certified in the Facial Action Coding System (Ekman & Friesen, 1978) and blind to the study aims, hypotheses, design, and group assignment coded smile intensity in the photographs. They rated the degree to which Action Unit 12, a facial behavior in which the lip corners are pulled up into a smile, was engaged on a scale ranging from 1 (trace) to 5 (maximum). If Action Unit 12 was not present, no intensity code was given. Multiple coders coded 21% of the photographs to assess reliability. The coding system was highly reliable (Cronbach’s α=.89).
Daily Surveys.
Each afternoon of the eight-week study, participants received an email with a link to an online “daily survey.” Using the 7-point Likert scale, they rated their experience of the emotions listed above (see the “Walk Surveys” section for the full list of emotions) to indicate how they felt that day. There were also asked the following questions: “To what extent did you feel part of something larger than yourself today?”; “To what extent did you feel small today?”; “To what extent did you feel in the presence of something vast today?”; “To what extent did you feel your life was terrible today?”; “To what extent did you feel your life was terrific today?”; “How much did you engage in acts today that involved helping someone else or doing something for a good cause?”. They responded on a 7-point Likert scale (1=not at all, 4=a little, 7=a lot).
Pre-and Post-Intervention Anxiety, Depression, and Life Satisfaction.
At the baseline assessment (i.e., pre-intervention) and eight weeks later (i.e., post-intervention), participants completed the Generalized Anxiety Disorder 7-Item Scale, a measure of anxiety (Spitzer, Kroenke, Williams, & Lowe, 2006); the Center for Epidemiological Studies Depression Scale (Radloff, 1977), a measure of depression; and the Satisfaction with Life Scale, a measure of well-being (Diener, Emmons, Larsen, & Griffin, 1985), among other measures not analyzed in the present study (see Supplemental Table 1). We focused on these measures here because prior studies have found associations between experiences of awe and improvements in anxiety, mood, and well-being (Gordon et al., 2017; Piff et al., 2015; Rudd, Vohs & Aakers, 2012).
Data Analyses
Statistical analyses were conducted in R (R Core Team, 2017); no interim analyses were conducted.
Inclusion Criteria.
We included participants in our analyses who took at least two walks over the course of the study, which we considered to be a “minimum effective dose” of the intervention and a liberal inclusion cut-off, and completed the pre- and post-intervention measures (n=52).
Cluster Scores.
For each walk survey and each daily survey, we averaged participants’ intensity ratings of relevant emotions to compute four emotional experience cluster scores: an “awe” cluster (awe, amazement, and wonder), a “prosocial positive emotions” cluster (compassion, admiration, amusement, appreciation, and gratitude), a “joy” cluster (joy, happiness, warmth, contentment, relaxation, calm, and pride), and a “distress” cluster (sadness, anger, anxiety, fear, and annoyance). Across days, the emotions reported in these cluster scores were highly correlated (see Supplemental Table 2); the cluster scores had an average alpha coefficient of .95 (awe cluster: α=.98, prosocial positive emotions cluster: α=.96, joy cluster: α=.93, distress cluster: α=.92), which suggested they were a reliable reflection of participants’ day-to-day emotional experience.
Impact of Awe Walks on Emotional Experience, Self-Size, and Smile Intensity During the Walks.
As a manipulation check, we first used a t-test to determine whether, over the course of the study, the groups differed in their overall experiences of awe during the walks. We next ran a series of linear mixed effects models using the nlme package in R to compare within-subject changes in outcomes between the awe walk and control walk groups. In all models, we specified random intercepts for participant, to account for individual variation in emotional experience, and fixed effects for group (0=control walk group, 1=awe walk group), to test for differences in emotional experience. To capture the passage of time, we computed a “time” variable, which reflected the number of days elapsed since day one of the study (range: 0 – 55). Because we expected emotional experience might have different trajectories in the two groups across the study, we also included time and a group by time interaction in all models (Gelman & Stern, 2006). In all analyses, we used the emotional experience cluster scores as our dependent variables. To follow up on statistically significant group by time interactions that emerged using the emotional experience cluster scores, we next ran linear mixed effects models for each of the individual emotions that were included in significant clusters, which allowed us to determine whether any results were driven by changes in certain emotions more than others. We then ran models with the same structure to examine whether the groups had different trajectories in self-size and smile intensity, behavioral variables that were extracted from the photographs. For each walk, we computed mean measures of self-size and smile intensity by averaging across participants’ photographs from that walk. The mean self-size and smile intensity measures were used as our dependent variables in the linear mixed effects models. We ran several additional models with this same structure to investigate whether awe walks also affected the extent to which participants felt a part of something larger than themselves, in the presence of something vast, and small, sentiments that pertain to social connection and are relevant to experiences of awe.
Finally, we conducted an additional set of analyses to examine whether taking more walks yielded greater benefits. We computed a “cumulative walks” variable, which represented a running total of the number of walks each participant had taken by each day of the study. In these analyses, we included the cumulative walks variable as a fixed effect instead of time, which allowed us to investigate whether participants who took more walks experienced more substantial emotional gains than participants who took fewer walks. We kept group in our model to examine whether the number of walks played a role in the gains that participants experienced above and beyond the experimental condition to which they were assigned. We planned to focus these analyses on the emotional experience clusters and behavioral measures (i.e., self-size and smile intensity) that were significant in our primary analyses.
Impact of Awe Walks on Daily Emotional Experience.
To test our hypothesis that awe walks would also give rise to emotional benefits outside of the walk context (using the emotional experience cluster scores), we ran a series of linear mixed effects models to investigate the impact of awe walks, passage of time, and the number of awe walks on daily emotional experience. All models were structured as described in the previous section. We conducted follow-up analyses, as described above, to decompose significant interactions, investigate the impact of awe walks on individual emotions in significant cluster scores, and examine whether more walks led to greater benefits using the “cumulative walks” variable instead of time.
Pre-and Post-Intervention Anxiety, Depression, and Life Satisfaction.
We used t-tests to compare the groups on pre- and post-intervention measures of anxiety, depression, and life satisfaction. Change scores for each measure (i.e., post-intervention minus pre-intervention) were also computed and compared with t-tests.
Results
Participants Included in the Analyses
Across the sample, 87% of the recruited participants were included in the analyses. Of those, 65% were female, and they had a median age of 75 years. Of the total recruited participants who did not meet criteria to be included in the analyses, 63% were female and the median age was 73 years, which suggested that lower engagement in the intervention did not appear related to these demographic factors. Over the course of the study, participants included in the analyses submitted a total of 2,341 daily surveys, 691 walk surveys, and 1,184 photographs (30 photographs were later excluded from the self-size analyses, and 35 were excluded from the smiling analyses for insufficient quality).
Group Characteristics
The awe walk and control walk groups had similar demographic profiles and no significant differences in cognitive functioning at the pre-intervention baseline, which indicated that the randomization successfully balanced the two groups on variables of interest (see Table 1). There was a trend for the control walk group to have a greater mean body mass index (p=.05). There were no statistically significant differences between the groups on the Generalized Anxiety Disorder 7-Item Scale, the Center for Epidemiological Studies Depression Scale, or the Satisfaction with Life Scale at the pre-intervention assessment. A difference between the groups in baseline anxiety approached significance (p=.11), but scores were very low on average and in the range of minimal anxiety. Further examination revealed one participant in the awe walk group whose baseline anxiety was more than five standard deviations above the mean of that group and in the level of mild to moderate anxiety.
Table 1:
Participant Demographics and Characteristics
| Awe Walk Group M(SD) | Control Walk Group M(SD) | Statistic | P | |
|---|---|---|---|---|
| N | 24 | 28 | ||
| Age | 75.5 (4.4) | 74 (4.4) | 1.20 | .24 |
| Sex (male / female) | 9 / 15 | 9 / 19 | 0.01 | .91 |
| Body Mass Index | 23.3 (3.1) | 25.1 (3.6) | −1.98 | .05 |
| Education | 17 (1.8) | 17.7 (2.1) | −1.32 | .19 |
| Race/Ethnicity (number) | ||||
| White | 23 | 25 | ||
| Black | 1 | 0 | ||
| Hispanic | 0 | 1 | ||
| Asian | 0 | 2 | ||
| Clinical Dementia Rating Scale Total | 0 (0) | 0 (0) | n/a | |
| Clinical Dementia Rating Scale -Sum of the Boxes | 0 (0) | 0 (0) | n/a | |
| Mini-Mental State Examination | 29.6 (0.8) | 29.1 (1.3) | 1.50 | .14 |
| CVLT-2 Long Form 10-minute Recall (/16) | 11.9 (3.4) | 11 (3.7) | 0.71 | .48 |
| Benson Figure Copy 10-minute Recall (/17) | 11.6 (1.8) | 11.5 (1.9) | 0.22 | .83 |
| Modified Trails (correct lines per minute) | 46.5 (19.0) | 41.2 (11.0) | 1.01 | .32 |
| Modified Trails Errors | 0.1 (0.5) | 0.1 (0.2) | 0.66 | .51 |
| Phonemic Fluency (# correct in 60 seconds) | 17.6 (3.6) | 16.1 (4.2) | 1.15 | .26 |
| Semantic Fluency (# correct in 60 seconds) | 23 (4.8) | 22.5 (3.7) | 0.40 | .69 |
| Design Fluency Correct (# correct in 60 seconds) | 12.1 (3.5) | 12.6 (3.9) | −0.39 | .70 |
| Design Fluency Repetitions | 1.9 (1.7) | 1.7 (1.5) | 0.41 | .68 |
| Digits Backward | 5.7 (1) | 5.6 (1.5) | 0.20 | .85 |
| Benson Figure Copy (/17) | 15.6 (0.6) | 15.8 (0.5) | −1.14 | .26 |
| Boston Naming Test Spontaneous Correct (/15) | 14.7 (0.6) | 14.6 (0.8) | 0.44 | .66 |
| Pre-Intervention Generalized Anxiety Disorder-7 Item Scale (/21) | 1.4 (2.3) | 0.6 (0.8) | 1.62 | .11 |
| Post-Intervention Generalized Anxiety Disorder-7 Item Scale (/21) | 1.4 (1.8) | 1.3 (1.7) | 0.18 | .86 |
| Pre-Intervention Satisfaction with Life Scale (/35) | 27.0 (5.2) | 29.2 (6.2) | −1.31 | .20 |
| Post-Intervention Satisfaction with Life Scale (/35) | 27.8 (5.9) | 29.6 (5.0) | −1.18 | .25 |
| Pre-Intervention Center for Epidemiological Studies Depression Scale | 3.4 (3.3) | 2.8 (2.1) | 0.91 | .37 |
| Post-Intervention Center for Epidemiological Studies Depression Scale | 3.5 (3.3) | 2.6 (2.1) | 1.13 | .27 |
T-tests or chi-square tests, when appropriate, were used to compare the groups. Means (M) and standard deviations (SD) are presented unless otherwise noted. n/a=not applicable.
Did Participants in the Awe Walk and Control Walk Groups Take Similar Walks?
Participants in the awe walk and control walk groups took walks that were of comparable speed, t(50)=1.02, p=.31. There were no statistically significant differences in the duration, t(50)=−1.61, p=.11, or distance, t(50)= −1.39, p=.17 of their walks, but there were trends that participants in the control walk group took walks of a somewhat longer duration and distance than those in the awe walk group. These potential differences appeared to be accounted for by a handful of participants in the control walk group who took a few longer walks (see Supplemental Figure 1). The groups also did not differ in how urban, t(50)= −.13, p=.89; beautiful, t(50)=.03, p=.98; or strenuous, t(50)= −.96, p=.34, they perceived their walks to be. In general, few participants took walks with companions, and there were no differences between the groups in the proportions of walks in which participants were accompanied by another person, t(50)= −1.07, p=.29, or by a pet, t(50)= −.67, p=.51. When joined by others on their walks, the groups did not differ in the average number of people who accompanied them, t(24)=.07, p=.94, but there was a trend for participants in the awe walk group to perceive receiving greater emotional support from their walk companions, t(24)=1.94, p=.06. Taken together, these results suggest many of the “objective” characteristics of the walks were similar in the two conditions (see Table 2).
Table 2:
Walk Characteristics of the Awe Walk and Control Walk Groups
| Awe Walk Group M(SD) | Control Walk Group M(SD) | T | P | |
|---|---|---|---|---|
| Total Number of Walks Taken | 7.5 (2.8) | 18.9 (14.1) | −3.89 | <.001 |
| Walk Duration (minutes) | 38.0 (14.1) | 46.6 (22.8) | −1.61 | .12 |
| Walk Distance (miles) | 1.4 (0.3) | 1.6 (0.8) | −1.39 | .17 |
| Walk Speed (estimated miles per hour) | 2.4 (0.7) | 2.2 (0.7) | 1.02 | .31 |
| Subjective Urban Setting of Walk (1–5) | 3.2 (1.1) | 3.2 (1.1) | −0.13 | .89 |
| Subjective Beauty of Walk (1–7) | 5.2 (0.8) | 5.1 (1.0) | 0.03 | .98 |
| Subjective Strenuousness of Walk (6–20) | 10.8 (1.0) | 11.0 (1.1) | −0.96 | .34 |
| Percentage of Walks Taken with Another Person | 12.0 (18.0) | 18.5 (24.7) | −1.07 | .29 |
| Number of People on Those Walks | 1.8 (1.3) | 1.8 (1.4) | 0.07 | .94 |
| Emotional Support Received (1–7) | 5.3 (1.5) | 4.0 (1.7) | 1.94 | .06 |
| Percentage of Walks Taken with Pets | 2.1 (10.2) | 4.6 (16.1) | −0.67 | .51 |
Means (M) and standard deviations (SD) are presented for each group. T-tests or chi-square tests, when appropriate, were used to compare the groups.
Unexpectedly, participants in the control walk group took significantly more walks than those in the awe walk group, t(50)= −3.89, p<.001 (see Table 2 and Supplemental Figure 1). Because they took more walks, they also completed more walk surveys, t(50)= −3.89, p<.001 (awe walk group: M=7.5, SD=2.8, control walk group: M=18.9, SD=14.1) and submitted more photographs, t(39)= −2.93, p=.01 (awe walk group: M=28.0, SD=12.0, control walk group: M=52.8, SD=36.6). Both groups, however, completed a similar number of daily surveys, t(50)=−1.16, p=.25 (awe walk group: M=43.7, SD=15.7, control walk group: M=47.9, SD=10.1). On a day-to-day basis, this pattern was also reflected in their self-reported daily exercise, which did not significantly differ between the groups but was higher in the control walk group on average (see Table 3).
Table 3:
Walk and Daily Survey Questions
| Awe Walk Group M(SD) | Control Walk Group M(SD) | T | P | |
|---|---|---|---|---|
| Walk Surveys | ||||
| To what extent did you feel part of something larger than yourself during your walk? | 4.6 (1.3) | 3.4 (1.8) | 2.75 | .01 |
| To what extent did you feel small during your walk? | 2.5 (1.3) | 1.9 (1.0) | 1.92 | .06 |
| To what extent did you feel in the presence of something vast during your walk? | 3.7 (1.6) | 3.1 (1.9) | 1.35 | .18 |
| To what extent did you feel as if your worries and concerns were insignificant during your walk? | 4.8 (1.6) | 4.0 (2.0) | 1.6 | .12 |
| Daily Surveys | ||||
| How many minutes did you exercise today? | 37.3 (23.1) | 48.0 (31.3) | −1.38 | .17 |
| To what extent did you feel part of something larger than yourself today? | 4.0 (1.4) | 3.5 (1.8) | 1.11 | .27 |
| To what extent did you feel small today? | 2.3 (1.2) | 1.9 (1.1) | 1.29 | .20 |
| To what extent did you feel in the presence of something vast today? | 3.3 (1.4) | 3.1 (1.9) | 0.49 | .63 |
| To what extent did you feel as if your worries and concerns were insignificant today? | 4.4 (1.6) | 4.0 (2.0) | 0.80 | .43 |
| To what extent did you feel your life was terrible today? | 1.3 (0.5) | 1.2 (0.3) | 1.16 | .25 |
| To what extent did you feel your life was terrific today? | 4.7 (1.3) | 5.1 (1.6) | −1.02 | .31 |
| How much did you engage in acts today that involved helping someone else or doing something for a good cause? | 4.1 (1.1) | 3.9 (1.4) | 0.76 | .45 |
Participants responded to these questions on 7-point Likert scales (1=not at all, 4=a little, 7=a lot). Means (M) and standard deviations (SD) are presented for each group. T-tests were used to compare the groups.
Did Experiences of Awe Increase During Awe Walks?
Emotional Experience.
A t-test comparing the groups on mean awe experienced during the walks across the study revealed significantly higher awe in those who took awe walks compared to those who took control walks, t(50)=2.67, p=.01, which indicated the awe walk instructions were effective (see Figure 1 and Supplemental Table 3 for group comparisons of the mean levels of emotional experience reported across the study). Linear mixed effects models revealed the main effect of group was not significant, but there was a significant main effect of time and a significant group by time interaction on awe experience during the walks. This suggested awe experience during the walks increased more over the study for participants who took awe walks than for those who took control walks (see Table 4). Follow-up analyses of the individual emotions in the awe cluster showed significant group by time interactions on awe but not on amazement or wonder (see Supplemental Table 4). An analysis that examined the impact of the number of cumulative walks also revealed a significant group by total cumulative walks interaction: participants who took more awe walks reported greater increases in awe during their walks than those who took more control walks, b=.07, CI95%=[.002, .14], p=.04.
Figure 1.
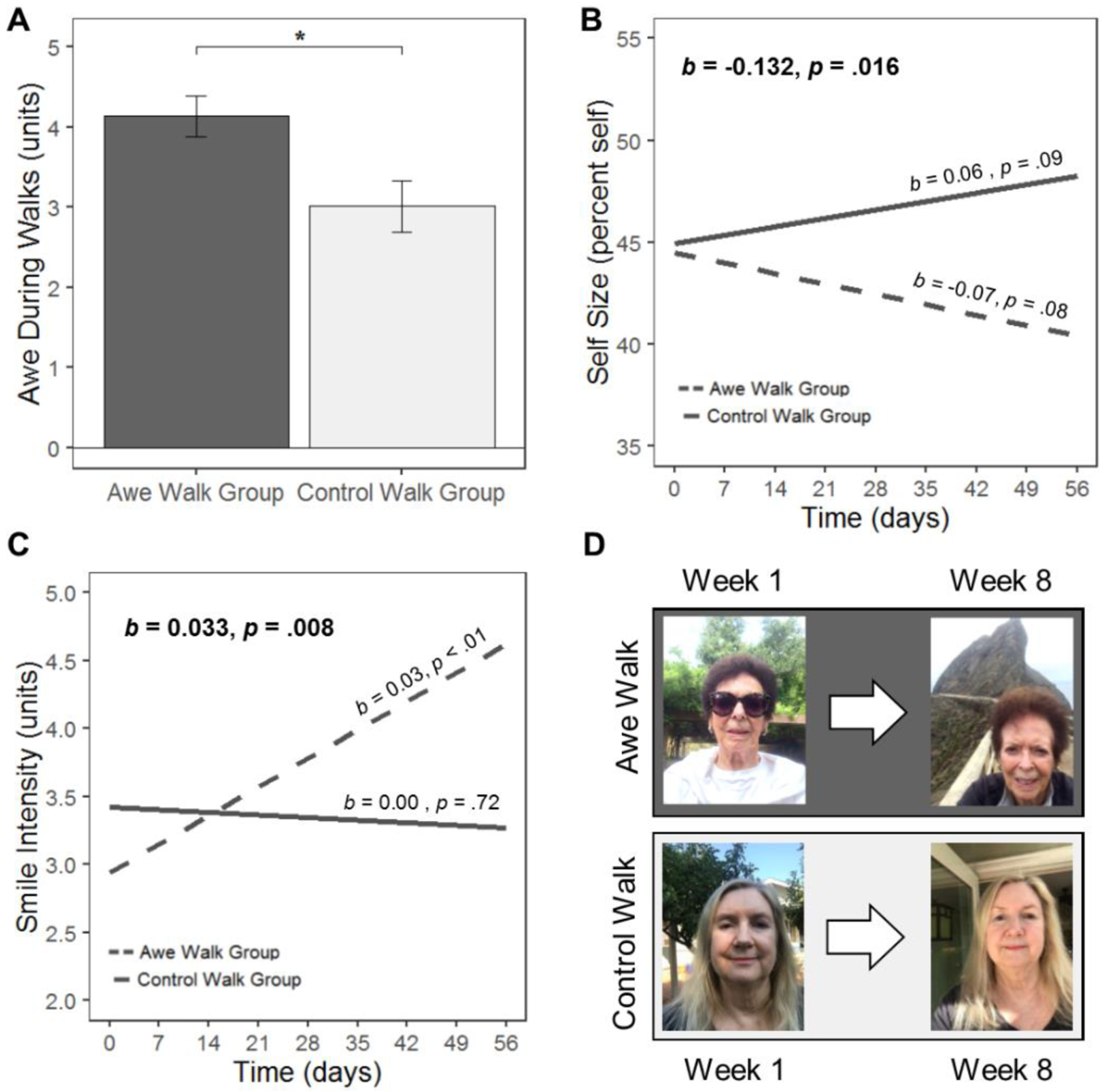
(A) Over the course of the study, participants who took awe walks experienced greater awe during their walks than participants who took control walks. Significant group by time interactions indicated that participants in the awe walk group and the control walk group had different trajectories in (B) self-size and (C) smile intensity. We also report the simple slopes and their significance levels in each group. (D) To illustrate the effects of awe walks on self-size and smile intensity, photographs are shown for two participants—one from the awe walk group and one from the control walk group— at the beginning (week 1) and end (week 8) of the study. These participants provided consent to publish their photographs.
Table 4:
Impact of Intervention Group, Time, and Their Interaction on Emotional Experience During the Walks
| b | CI 95% | SE | P | |
|---|---|---|---|---|
| Awe Cluster | ||||
| Intercept | 3.224 | [2.643, 3.804] | 0.296 | <.001 |
| Group | 0.782 | [−0.123, 1.688] | 0.451 | .09 |
| Time (days) | −0.009 | [−0.015, −0.002] | 0.003 | .01 |
| Group × Time | 0.015 | [0.002, 0.027] | 0.006 | .02 |
| Prosocial Positive Emotions Cluster | ||||
| Intercept | 3.907 | [3.388, 4.426] | 0.264 | <.001 |
| Group | −0.022 | [−0.822, 0.779] | 0.398 | .96 |
| Time (days) | −0.004 | [−0.008, 0.001] | 0.002 | .13 |
| Group × Time | 0.016 | [0.007, 0.026] | 0.005 | .001 |
| Joy Cluster | ||||
| Intercept | 4.411 | [3.955, 4.868] | 0.232 | <.001 |
| Group | −0.031 | [−0.740, 0.677] | 0.353 | .93 |
| Time (days) | −0.004 | [−0.009, 0.001] | 0.002 | .10 |
| Group × Time | 0.011 | [0.001, 0.020] | 0.005 | .03 |
| Distress Cluster | ||||
| Intercept | 1.442 | [1.248, 1.635] | 0.099 | <.001 |
| Group | 0.032 | [−0.285, 0.350] | 0.158 | .84 |
| Time (days) | 0.002 | [−0.001, 0.005] | 0.002 | .24 |
| Group × Time | −0.003 | [−0.009, 0.004] | 0.003 | .45 |
The unstandardized beta (b), 95% confidence interval (CI95%), standard error of the mean (SE), and p value are presented for each fixed effect of interest (and their interactions) in the mixed effects models that predicted emotional experience during the walks. We included the following variables in the models: group (0=control walk group, 1=awe walk group), time (the number of days elapsed since day one of the study), and their interaction.
Participants’ responses to the open-ended question about their walks echoed these findings and illustrated the ways in which awe walks shifted their attention to the details of the world around them and encouraged wonder. For example, one participant in the awe walk group wrote, “The beautiful fall colors and the absence of them amidst the evergreen forest. Thought about how the leaves were no longer crunchy underfoot because of the rain and how the walk was more spongy now… Thought about the wonder that a small child feels as they explore their expanding world.” In contrast, a participant from the control walk group wrote, “I thought about our vacation in Hawaii coming up this next Thursday. Thought about all the things I had to do before we leave.”
Self-Size.
Using the measure of self-size from the photographs, linear mixed effects models showed that, although there was no main effect of group, b=−.44, CI95%=[−8.24, 7.35], p=.91, or time, b=.06, CI95%=[−.01, .13], p=.09, on self-size, the group by time interaction was significant, b=−.13, CI95%=[−.24, −.03], p=.02. This indicated that participants in the awe walk group included increasingly less of themselves and increasingly more of the background scenery in their photographs over the course of the study when compared to participants in the control walk group (see Figure 1). An analysis of participants’ cumulative walks revealed this effect scaled with the number of walks participants took (i.e., there was a significant group by total cumulative walks interaction) such that those who took more awe walks had an even smaller self than those who took more control walks, b=−.26, CI95%=[−.41, −.12], p<.001.
These results were mirrored in the participants’ responses to questions about being connected to the larger world. On average, participants in the awe walk group reported significantly greater feelings of being part of something larger than themselves during their walks (see Table 3). Linear mixed effects models that further examined responses to this question revealed that, despite there being no significant main effect of group, b=.76, CI95%=[−.20, 1.72], p=.12, there was a significant main effect of time, b=−.01, CI95%=[−.02, −.01], p<.001, and a significant group by time interaction, b=.02, CI95%=[.005, .03], p=.01, which indicated that, over time, participants in the awe walk group reported greater increases in feeling a part of something larger than themselves during their walks than those in the control walk group. On average, the groups did not differ in the extent to which they felt in the presence of something vast during their walks (see Table 3). Linear mixed effects models that further examined responses to this question also found no main effect of group, b=.05, CI95%=[−.98, 1.08], p=.93, but the main effect of time, b=−.01, CI95%=[−.02, −.003], p=.01, and the group by time interaction were significant, b=.02, CI95%=[.01, .04], p<.001, such that, over time, participants who took awe walks reported greater increases in feeling in the presence of something vast during their walks than those who took control walks. The groups did not differ in their average feelings of smallness during their walks, though the means were in the expected directions. Neither the main effect of group, b=.61, CI95%=[−.08, 1.31], p=.08, nor time, b=.00, CI95%=[−.002, .01], p=.20, nor their interaction, b=.00, CI95%=[−.01, .01], p=.81, was significant.
Did Experiences of Other Positive Emotions Increase During Awe Walks?
Emotional Experience.
Linear mixed effects models of emotional experience during the walks revealed no significant fixed effects of group or time but did show significant group by time interactions on prosocial positive emotions and joy (see Table 4). During the walks, positive emotions—both prosocial and non-prosocial—increased more over time in participants who took awe walks than in those who took control walks. Follow-up analyses of individual emotions showed significant group by time interactions on compassion, admiration, and appreciation from the prosocial positive emotions cluster (amusement and gratitude approached significance) and on joy and pride from the joy cluster (warmth and relaxed approached significance) but not on other positive emotions in those clusters (see Supplemental Table 4). Analyses that examined the impact of the number of cumulative walks also revealed significant group by total cumulative walks interactions: participants who took more awe walks reported greater increases in prosocial positive emotions, b=.11, CI95%=[.06, .16], p<.001, and joy, b=.06, CI95%=[.01, .11], p=.02, during their walks than those who took more control walks. There was no significant difference between the groups in the extent to which they felt their worries and concerns were insignificant during their walks (see Table 3).
Smile Intensity.
A linear mixed effects model found no main effect of group, b=−.48, CI95%=[−1.95, .99], p=.51, or time, b=.00, CI95%=[−.02, .01], p=.72, on smile intensity, but their interaction was significant, b=.03, CI95%=[.01, .06], p=.01. Participants who took awe walks displayed greater increases in smile intensity over the course of the study than those who took control walks (see Figure 1). An analysis that examined the impact of the number of cumulative walks revealed a significant group by total cumulative walks interaction: participants who took more awe walks displayed greater increases in smile intensity, b=.04, CI95%=[.02, .07], p<.001, during their walks than those who took more control walks.
Did Experiences of Negative Emotions Decrease During Awe Walks?
The linear mixed effects models found no significant main effects of group or time and no significant group by time interaction on distress (see Table 4). This suggested participants in the awe walk and control walk groups experienced comparable levels of distress during the walks and that differences in walk-related distress did not emerge between the groups over time.
Did Awe Walks Increase Daily Experiences of Awe?
Next, we investigated whether awe walks shifted emotional experiences outside of the walk context, as captured in the daily surveys. For daily awe experience, a linear mixed effects model found neither the main effect of group nor time (time was at trend level) nor their interaction was significant (see Table 5 and Figure 2). This suggested that daily experiences of awe—outside of the walk context—did not increase more for participants who took awe walks than for those who took control walks.
Table 5:
Impact of Intervention Group, Time, and Their Interaction on Daily Emotional Experience
| b | CI 95% | SE | P | |
|---|---|---|---|---|
| Awe Cluster | ||||
| Intercept | 2.753 | [2.203, 3.303] | 0.281 | <.001 |
| Group | 0.344 | [−0.487, 1.179] | 0.414 | .41 |
| Time (days) | 0.004 | [−0.000, 0.008] | 0.002 | .05 |
| Group × Time | 0.002 | [−0.004, 0.008] | 0.003 | .471 |
| Prosocial Positive Emotions Cluster | ||||
| Intercept | 4.052 | [3.525, 4.578] | 0.268 | <.001 |
| Group | 0.137 | [−0.657, 0.932] | 0.396 | .73 |
| Time (days) | 0.002 | [−0.001, 0.004] | 0.001 | .15 |
| Group × Time | 0.004 | [0.000, 0.008] | 0.002 | .03 |
| Joy Cluster | ||||
| Intercept | 4.443 | [4.014, 4.872] | 0.219 | <.001 |
| Group | −0.026 | [−0.674, 0.622] | 0.322 | .94 |
| Time (days) | −0.001 | [−0.004, 0.001] | 0.001 | .27 |
| Group × Time | −0.000 | [−0.004, 0.004] | 0.002 | .97 |
| Distress Cluster | ||||
| Intercept | 1.754 | [1.476, 2.033] | 0.142 | <.001 |
| Group | 0.252 | [−0.169, 0.673] | 0.210 | .24 |
| Time (days) | 0.002 | [−0.001, 0.004] | 0.001 | .18 |
| Group × Time | −0.004 | [−0.008, −0.000] | 0.002 | .03 |
The unstandardized beta (b), 95% confidence interval (CI95%), standard error of the mean (SE), and p value are presented for each fixed effect of interest (and their interactions) in the mixed effects models that predicted daily emotional experience. We included the following variables in the models: group (0=control walk group, 1=awe walk group), time (the number of days elapsed since day one of the study), and their interaction.
Figure 2.
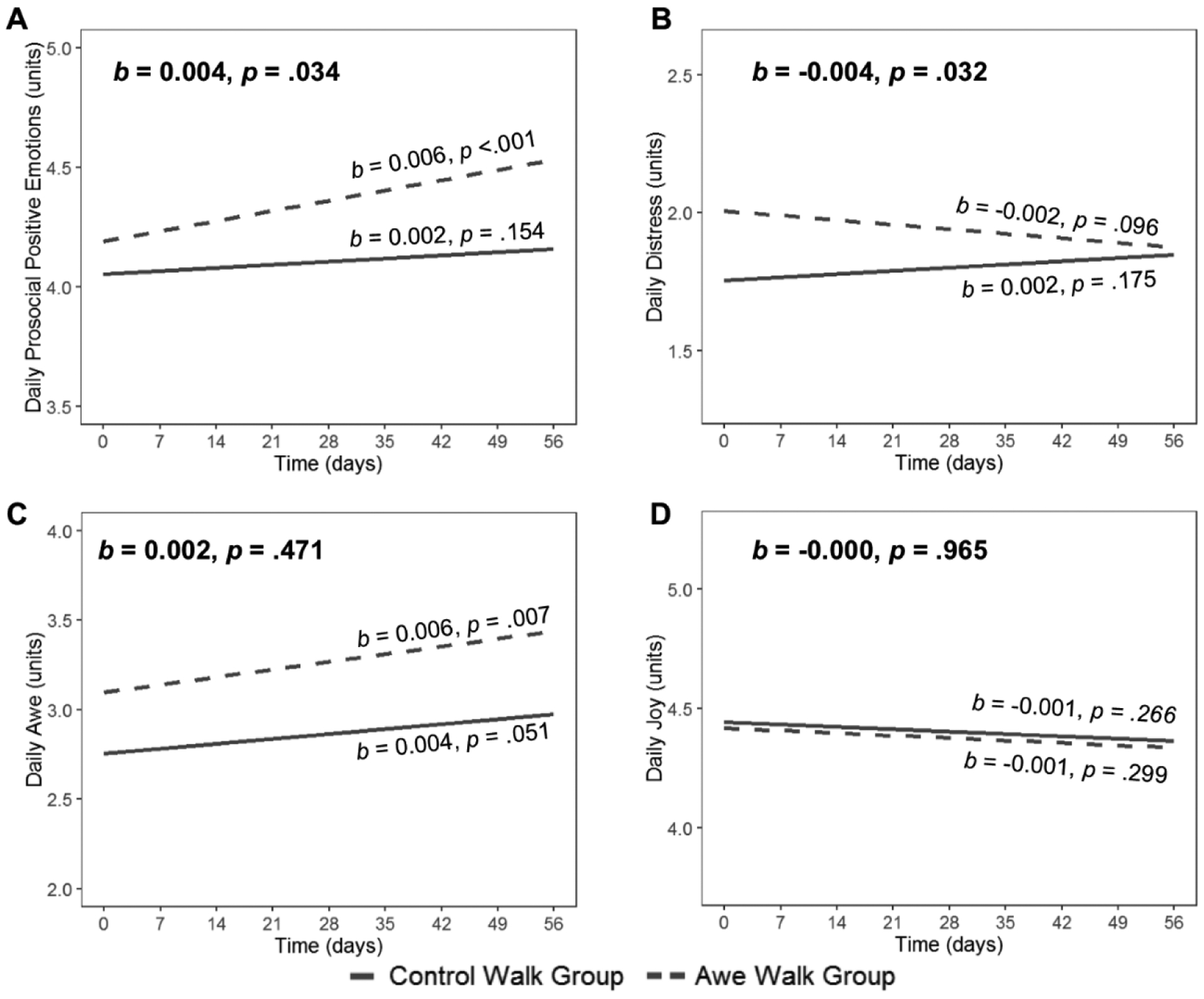
The awe walk group and control walk group had different trajectories (significant group by time interactions) in their daily experiences of (A) prosocial positive emotions and (B) distress but not in their daily experiences of (C) awe or (D) joy. We also report the simple slopes and their significance levels in each group.
Across the study, the groups also did not differ in their overall daily ratings of feeling part of something larger than themselves, in the presence of something vast, or small (see Table 3). Linear mixed effects models that further examined their responses to these questions, however, revealed significant differences between the groups over time. For the question that asked participants whether they felt a part of something larger than themselves on a daily basis, there was no significant main effect of group, b=.02, CI95%=[−.91, .95], p=.97, but there was a significant main effect of time, b=−.01, CI95%=[−.02, −.01], p<.001, and a significant group by time interaction, b=.02, CI95%=[.01, .02], p<.001. This indicated that, over time, participants in the awe walk group reported greater increases in day-to-day feelings of being a part of something larger than themselves than those in the control walk group. For the question that asked participants to rate the extent to which they felt in the presence of something vast on a daily basis, there was no main effect of group, b=−.16, CI95%=[−1.11, .80], p=.74, but the main effect of time, b=−.01, CI95%=[−.01, −.01], p<.001, and the group by time interaction were significant, b=.01, CI95%=[.01, .02], p<.001, such that, compared to participants who took control walks, participants who took awe walks reported greater increases over time in day-to-day feelings of being in the presence of something vast. For the question that asked participants to rate their daily feelings of smallness, a similar pattern emerged. Despite no main effect of group, b=.12, CI95%=[−.54, .79], p=.71, there was a significant effect of time, b=−.003, CI95%=[−.01, −.00], p=.03, and a significant group by time interaction, b=.01, CI95%=[.01, .02], p<.001, which suggested that over time, participants in the awe walk group reported greater increases in daily feelings of smallness than those in the control walk group.
Did Awe Walks Increase Daily Experiences of Other Positive Emotions?
We next examined whether there was a main effect of group or a group by time interaction on participants’ daily experiences of prosocial positive emotions. There were no main effects of group or time on daily prosocial positive emotions, but their interaction was significant such that, compared to participants in the control walk group, those who took awe walks experienced greater increases in daily prosocial positive emotions over the course of the study (see Table 5 and Figure 2). Follow-up analyses of the individual emotions in the prosocial positive emotions cluster showed significant group by time interactions on compassion, admiration, and amusement (see Supplemental Table 5). Analyses that investigated the impact of the number of cumulative walks revealed a significant group by total cumulative walks interaction: participants who took more awe walks reported greater increases in daily prosocial positive emotions, b=.05, CI95%=[.03, .08], p<.001, than those who took more control walks. Follow-up exploration of this effect in the awe walk group only showed each awe walk was associated with a .05 unit increase in daily prosocial positive emotions, b=.05, CI95% [.03, .07], p<.001. To further examine and visualize the daily prosocial positive emotional gains that were related to each awe walk, we computed change scores by subtracting participants’ average daily prosocial positive emotions reported on the first day of the study from their average levels on each day of the study on which they took an awe walk. These change scores suggested a dose-like relationship between awe walks and enhanced daily prosocial positive emotions (see Figure 3).
Figure 3.
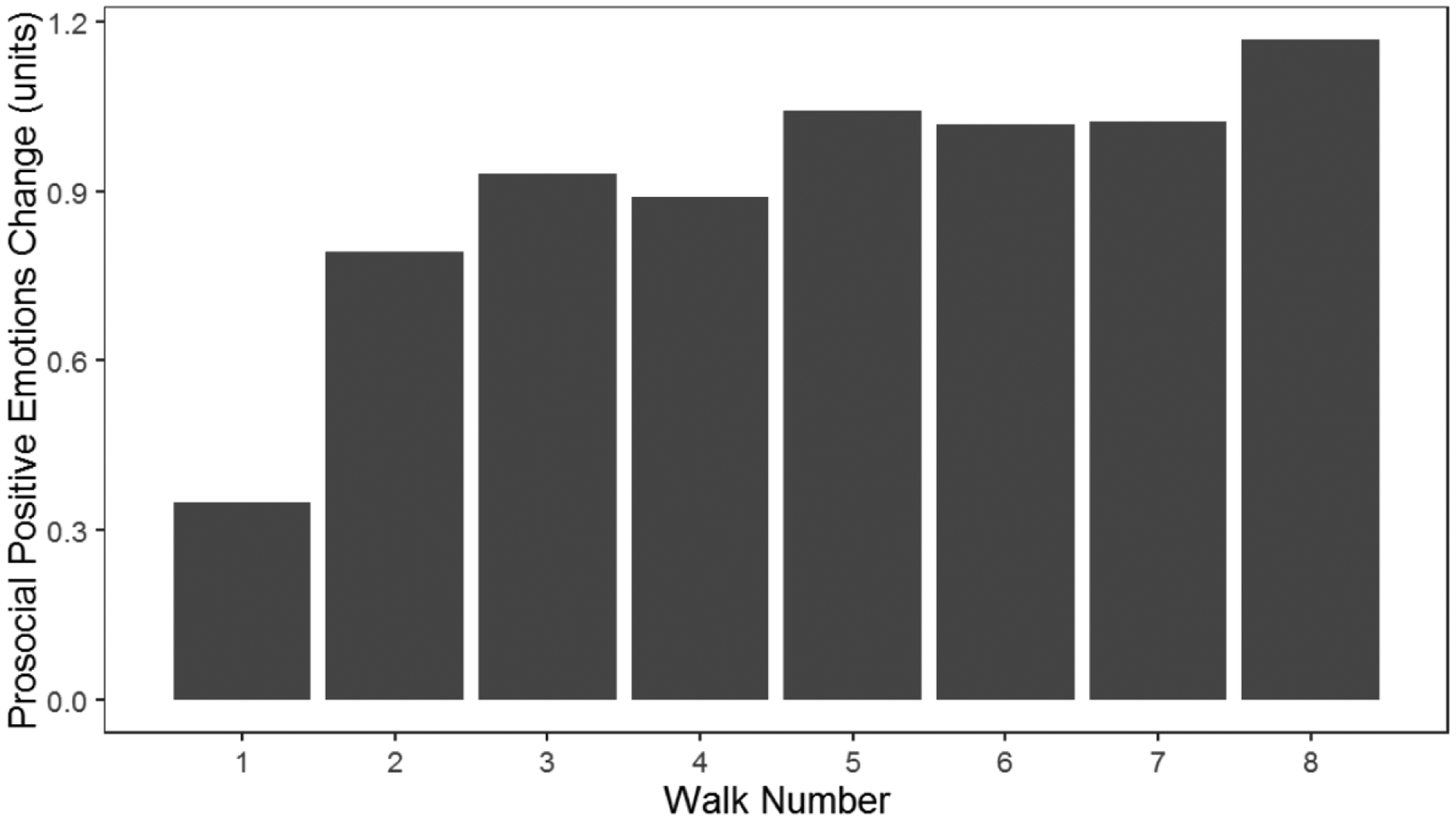
Participants who took more awe walks experienced greater emotional gains than those who took fewer awe walks. We computed change scores for daily prosocial positive emotions by subtracting participants’ average daily prosocial positive emotions on the first day of the study from their average levels on each day they took an awe walk. Each awe walk resulted in a small increase in participants’ daily experience of prosocial positive emotions (compared to their self-reported experience on the first day of the study). This suggested there was a dose-like relationship between awe walks and prosocial positive emotions experienced on a day-to-day basis, outside of the walk context.
The greater day-to-day prosocial positive emotional gains experienced by participants in the awe walk group relative to those in the control walk group did not extend to non-prosocial positive emotions, however, as the main effects of group, time, and the group by time interaction on daily joy were not significant (see Table 5 and Figure 2).
Did Awe Walks Decrease Daily Experiences of Negative Emotions?
We next examined whether awe walks impacted participants’ daily negative emotional experience. The linear mixed effects models found the main effects of group and time on daily distress were not significant, but their interaction was (see Table 5 and Figure 2). This suggested divergence between the groups in their day-to-day experiences of distress over the course of the study and indicated that distress declined more over time in participants who took awe walks than in those who took control walks. Investigation of the individual emotions in the distress cluster showed that participants who took awe walks experienced significantly greater decreases in daily sadness and fear but not in daily anger, anxiety, or annoyance over the study than those who took control walks (see Supplemental Table 5).
Did Awe Walks Impact Post-Intervention Anxiety, Depression, or Life Satisfaction?
The awe walk and control walk groups did not differ in their post-intervention scores on the Generalized Anxiety Disorder 7-Item Scale, the Center for Epidemiological Studies Depression Scale, or the Satisfaction with Life Scale (see Table 1). Given the relative stability of these measures across the two time points, the groups also did not show different amounts of change (i.e., post-intervention minus pre-intervention) in anxiety, t(49)= −1.39, p=.17 (awe walk group: M=0.0, SD=1.5; control walk group: M=0.6, SD=1.5); depression, t(49)=0.47, p=.64 (awe walk group: M=0.2, SD=3.1; control walk group: M=−0.1, SD=1.7); or life satisfaction, t(49)=0.04, p=.96 (awe walk group: M=0.5, SD=4.1; control walk group: M=0.4, SD=3.8) over the study.
Discussion
The present study revealed that a simple, brief intervention can increase awe, a positive emotion evoked by perceptual vastness (Keltner & Haidt, 2003). By attending to the details of the world around them and tapping into their sense of wonder, participants who took awe walks experienced greater awe during their walks than those who took control walks. Over time, participants who took awe walks also expressed greater feelings of social connection (feeling that one was part of something larger in the world) and exhibited a smaller self (as measured in the photographs they submitted from their walks) during their walks than those who took control walks. In addition to elevated feelings of awe, participants who took awe walks reported greater increases in other positive emotions, including prosocial positive emotions and joy, during their walks over the course of the study than those who took control walks. The accumulating positive feelings that participants in the awe walk group reported during their walks were also reflected in their photographs. Over time, participants who took awe walks displayed greater smile intensity, a behavioral measure of well-being that shapes social interactions in beneficial ways (Harker & Keltner, 2001), than those who took control walks. Outside of the walk context, awe walks also impacted day-to-day emotional experience. Although daily experiences of awe did not differ between the groups or increase more over time in participants who took awe walks, participants who took awe walks did report greater increases in daily prosocial positive emotions and greater decreases in daily distress over the course of the study than those who took control walks. Daily feelings of joy did not differ between the groups over time. Compared to those who took control walks, participants who took awe walks also reported greater feelings of social connection, being in the presence of something vast, and smallness on a daily basis over the study.
Even brief experiences of awe can shift how people view themselves in a social context (Keltner, Kogan, Piff, & Saturn, 2014). By moving attention away from the self and onto larger entities, awe expands existing cognitive frameworks and promotes behaviors that prioritize others, such as kindness and humility (Keltner & Haidt, 2003; Piff et al., 2015; Stellar et al., 2018). Compared to participants who took control walks, those who took awe walks experienced greater increases in prosocial positive emotions (during their walks and on a daily basis) and felt more intensely that they were a part of something larger than themselves, a prosocial orientation considered to be a key element of wisdom (Bangen, Meeks, & Jeste, 2013). Consistent with prior studies, experiences of awe helped participants to feel like they were in the presence of vast things and encouraged a sense of smallness (Bai et al., 2017; Campos, Shiota, Keltner, Gonzaga, & Goetz, 2013), a sentiment captured most notably by the photographs that participants took of themselves. As the study progressed, participants who took awe walks displayed a “shrinking self” (Shiota, Keltner, & Mossman, 2007), filling proportionately less of the photographs with themselves and more with the background scenery than those who took control walks. On self-report measures, although participants in the awe walk group more strongly endorsed daily feelings of smallness over time, this pattern was not evident when we examined reported feelings of smallness during the awe walks themselves. Unlike prior studies of awe, we did not find increases in post-intervention life satisfaction in participants who experienced more awe (Gordon et al., 2017; Rudd et al., 2012).
Positive emotions are brief events that shift us momentarily away from trait-like levels of baseline affect (Diener, Lucas, & Scollon, 2009). In addition to greater gains in awe and prosocial positive emotional experience during their walks, participants who took awe walks also reported greater increases in joy during their walks than those who took control walks. These elevated positive feelings were mirrored in their photographs, which revealed that participants who took awe walks displayed bigger, more intense smiles during their walks over time than those in the control walk group. The only positive emotions that endured beyond the awe walk setting, however, were the prosocial positive emotions (not awe or joy). Participants who took awe walks did not report greater awe on a daily basis and, unlike experiences of awe during the walks, which increased over time, daily experiences of awe also did not grow over the course of the study. Thus, although our intervention instructions were successful and enhanced participants’ experiences of awe during awe walks, elevations in awe did not persist outside of the walk context. Experiences of prosocial positive emotions, in contrast, were greater during awe walks than during control walks and also increased more over time for participants who took awe walks than for those who took control walks when they were measured on a daily basis, outside of the walk setting. Prosocial positive emotions prioritize the needs of others and encourage us to connect with and care for others (Algoe et al., 2013; Goetz et al., 2010), and these results are consistent with findings showing that experiences of awe potentiate emotions and actions that focus on other people (Piff et al., 2015). We did not find evidence that increasing prosocial positive feelings translated into greater prosocial actions, however, as the groups did not differ in the extent to which they reported engaging in helpful acts or doing something for a good cause. Taken together, our findings suggest that enhanced experiences of awe during the awe walks may have conferred a beneficial affective shift in the moment and may also have had more lasting effects on prosocial positive emotions outside of the walk setting.
Our results suggest cultivating awe may also help to counter negative emotions, which may have long-term health benefits (Lyubomirsky, King, & Diener, 2005). Although negative emotions were not lessened during the awe walks themselves, participants who took awe walks did report greater reductions in daily distress over time than those who took control walks. A few caveats are warranted about this result, however. Daily distress was somewhat higher in the awe walk group at the beginning of the study for unknown reasons, making it possible that distress levels regressed to the mean more in those who took awe walks than in those who took control walks for reasons other than their group assignment. In addition, trait-like measures of anxiety and depression did not change in the awe walk or control walk group when post-intervention levels were compared to pre-intervention levels. In general, daily levels of negative emotional experience as well as pre- and post-intervention measures of anxiety and depression were very low in this sample, which may have limited our ability to explore the impact of awe walks on chronic negative states. It is also possible, however, that awe walks were not potent enough to shift more enduring aspects of anxiety and mood in older adults. Nonetheless, our results suggest that, compared to participants who took control walks, those who took awe walks experienced greater increases in daily positive emotions and greater decreases in daily negative emotions, a modification in affective experience that may benefit older adults (Brown, Nesse, Vinokur, & Smith, 2003).
We expected that awe, like other positive emotions, could be nurtured over time with some instruction and effort. Whereas it might be easy to imagine how certain positive emotions, such as gratitude, could be easy to cultivate with practice, it may be more difficult to see how awe, an emotion that is facilitated by novelty and wonder, might grow with time or effort. An alternative hypothesis for the present study, therefore, could have been that as participants took more awe walks, they would habituate to the awe-walk practice and no longer find new details in the world to appreciate, thereby causing awe to dissipate. We did not find any evidence to support this alternative model, however, and rather found that awe did not wane but bloomed the more awe walks participants took. Participants who took more awe walks during the study not only experienced greater gains in awe during their walks but experienced larger increases in prosocial positive emotions and joy than those who took fewer awe walks. An examination of the impact that each awe walk had on other types of emotional experience showed a dose-like relationship between awe walks and daily prosocial positive emotions and suggested that each awe walk yielded a small yet incremental increase in daily prosocial positive emotions, gains that mounted over time. This pattern was not apparent in the control walk group. Although participants in the control walk group took more walks than those in the awe walk group, they did not experience increases in any positive emotions or decreases in negative emotions overall or in relation to the number of walks they took. The fact that participants in the control walk group took more walks than those in the awe walk group was an unexpected result, and we speculate this happened because participants in the control walk group assumed the study was about exercise or, perhaps, because they recorded more casual walks in their daily lives as being study-relevant given that the walks this group took required no particular type of focus or effort. This possibility, it should be noted, worked against our hypothesis because more walks in the control group gave those participants more opportunities to experience walk-related benefits, which made it more difficult for us to find unique benefits of awe walks. Despite this difference between the groups, the walks taken by participants in both groups were remarkably similar in terms of their locations, strenuousness, and beauty. Participants in the awe walk group were encouraged to go to new places for their walks, if possible, which likely helped them to continue to foster experiences of awe.
The present study has several noteworthy limitations. First, we did not test whether the effects of the awe walk intervention persisted beyond the eight-week study. Our results showed that over time, daily experiences of prosocial positive emotions progressively increased, and daily experiences of daily distress decreased, more in the awe walk group than in the control walk group, which suggested that awe walks brought about affective benefits that accumulated over time. Given that participants in the awe walk group did not experience greater improvements in more stable measures of anxiety, depression, or life satisfaction, however, it is unlikely that differences in these measures would emerge at later time points. Although participants who stop using awe-promoting strategies may experience fewer long-term benefits, our results suggested that those who continue to seek out awe may experience progressive affective gains, at least on a day-to-day basis. Second, most participants in our sample were Caucasian and highly educated, which may limit the generalizability of our findings. Future studies that examine whether awe has similar effects in other cultural and demographic contexts will be necessary to understand how positive emotions impact health in various populations. Third, despite being in a period of life often characterized by illness and decline, our participants were physically and cognitively healthy. Given the very low levels of anxiety and other mental health related symptoms in our sample, it is possible that our results underestimate the beneficial impact awe walks might have in groups facing greater stress and emotional challenges. Future studies of older adults with more significant health problems will help to determine whether awe can improve outcomes in those individuals. Prior studies have shown that awe improves wellbeing and reduces stress in other at-risk populations, including at-risk teens and veterans (Anderson et al., 2018), suggesting that awe walks may also ameliorate health outcomes in other populations. Fourth, our study was powered to detect group by time interactions that leveraged the repeated measures in our sample. Thus, the null findings that we report when directly comparing the groups should be interpreted with caution. It is possible that some between-groups differences would emerge, or even disappear, in larger samples.
Although some people flourish as they age into their later years, in the mid-seventies many experience elevated sadness and fear, negative states that undermine health and hasten cognitive and physical decline. Building upon recent evidence linking outdoor experiences of awe to improved mental health (Anderson et al., 2018), the results of the present study suggest that cultivating experiences of awe can bring about small affective shifts that benefit vulnerable populations such as older adults. While the effects of each awe walk may be modest, even incremental gains in well-being may be advantageous for health and longevity, especially in older adults (Chida & Steptoe, 2008). Whereas other positive emotion interventions often require training, the present study found that cultivating experiences of awe via a simple set of instructions can have beneficial effects in older adults that help to counter the detrimental effects of negative emotions that are common in aging. The more participants practiced experiencing awe via walks, the more they benefitted, which suggests that experiences of awe and other prosocial positive emotions may continue to expand with practice.
Supplementary Material
Acknowledgements
We are grateful to the volunteers who participated in our study. This work was supported by funding from the Global Brain Health Institute.
References
- Algoe SB, Fredrickson BL, & Gable SL (2013). The social functions of the emotion of gratitude via expression. Emotion, 13(4), 605–609. doi: 10.1037/a0032701 [DOI] [PubMed] [Google Scholar]
- Anderson CL, Dixson DD, Monroy M, & Keltner D (2019). Are awe-prone people more curious? The relationship between dispositional awe, curiosity, and academic outcomes. Journal of Personality. doi: 10.1111/jopy.12524 [DOI] [PubMed] [Google Scholar]
- Anderson CL, Monroy M, & Keltner D (2018). Awe in nature heals: Evidence from military veterans, at-risk youth, and college students. Emotion. doi: 10.1037/emo0000442 [DOI] [PubMed] [Google Scholar]
- Bai Y, Maruskin LA, Chen S, Gordon AM, Stellar JE, McNeil GD, … Keltner D (2017). Awe, the diminished self, and collective engagement: Universals and cultural variations in the small self. Journal of Personality and Social Psychology, 113(2), 185–209. doi: 10.1037/pspa0000087 [DOI] [PubMed] [Google Scholar]
- Bangen KJ, Meeks TW, & Jeste DV (2013). Defining and assessing wisdom: a review of the literature. American Journal of Geriatric Psychiatry, 21(12), 1254–1266. doi: 10.1016/j.jagp.2012.11.020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bolier L, Haverman M, Westerhof GJ, Riper H, Smit F, & Bohlmeijer E (2013). Positive psychology interventions: a meta-analysis of randomized controlled studies. BMC Public Health, 13, 119. doi: 10.1186/1471-2458-13-119 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borg GA (1982). Psychophysical bases of perceived exertion. Medicine and Science in Sports and Exercise, 14(5), 377–381. [PubMed] [Google Scholar]
- Brown SL, Nesse RM, Vinokur AD, & Smith DM (2003). Providing social support may be more beneficial than receiving it: results from a prospective study of mortality. Psychol Sci, 14(4), 320–327. doi: 10.1111/1467-9280.14461 [DOI] [PubMed] [Google Scholar]
- Buchanan KE, & Bardi A (2010). Acts of kindness and acts of novelty affect life satisfaction. Journal of Social Psychology, 150(3), 235–237. doi: 10.1080/00224540903365554 [DOI] [PubMed] [Google Scholar]
- Byers AL, Yaffe K, Covinsky KE, Friedman MB, & Bruce ML (2010). High occurrence of mood and anxiety disorders among older adults: The National Comorbidity Survey Replication. Archives of General Psychiatry, 67(5), 489–496. doi: 10.1001/archgenpsychiatry.2010.35 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cacioppo JT, & Cacioppo S (2014). Social Relationships and Health: The Toxic Effects of Perceived Social Isolation. Soc Personal Psychol Compass, 8(2), 58–72. doi: 10.1111/spc3.12087 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cacioppo JT, & Cacioppo S (2018). The growing problem of loneliness. Lancet, 391(10119), 426. doi: 10.1016/s0140-6736(18)30142-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cacioppo JT, & Hawkley LC (2009). Perceived social isolation and cognition. Trends Cogn Sci, 13(10), 447–454. doi: 10.1016/j.tics.2009.06.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cacioppo JT, Hawkley LC, Crawford LE, Ernst JM, Burleson MH, Kowalewski RB, … Berntson GG (2002). Loneliness and health: potential mechanisms. Psychosomatic Medicine, 64(3), 407–417. [DOI] [PubMed] [Google Scholar]
- Campos B, Shiota MN, Keltner D, Gonzaga GC, & Goetz JL (2013). What is shared, what is different? Core relational themes and expressive displays of eight positive emotions. Cogn Emot, 27(1), 37–52. doi: 10.1080/02699931.2012.683852 [DOI] [PubMed] [Google Scholar]
- Carstensen LL, Turan B, Scheibe S, Ram N, Ersner-Hershfield H, Samanez-Larkin GR, … Nesselroade JR (2011). Emotional experience improves with age: evidence based on over 10 years of experience sampling. Psychol Aging, 26(1), 21–33. doi: 10.1037/a0021285 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chida Y, & Steptoe A (2008). Positive psychological well-being and mortality: a quantitative review of prospective observational studies. Psychosom Med, 70(7), 741–756. doi: 10.1097/PSY.0b013e31818105ba [DOI] [PubMed] [Google Scholar]
- Colcombe S, & Kramer AF (2003). Fitness effects on the cognitive function of older adults: a meta-analytic study. Psychol Sci, 14(2), 125–130. doi: 10.1111/1467-9280.t01-1-01430 [DOI] [PubMed] [Google Scholar]
- Danvers AF, & Shiota MN (2017). Going off script: Effects of awe on memory for script-typical and -irrelevant narrative detail. Emotion, 17(6), 938–952. doi: 10.1037/emo0000277 [DOI] [PubMed] [Google Scholar]
- de Koning J, Richards S, & Stathi A (2019). Loneliness, Social Isolation, and Objectively Measured Physical Activity in Rural-Living Older Adults. J Aging Phys Act, 1–11. doi: 10.1123/japa.2019-0027 [DOI] [PubMed] [Google Scholar]
- Diener E, Emmons RA, Larsen RJ, & Griffin S (1985). The Satisfaction With Life Scale. J Pers Assess, 49(1), 71–75. doi: 10.1207/s15327752jpa4901_13 [DOI] [PubMed] [Google Scholar]
- Diener E, Lucas RE, & Scollon CN (2009). Beyond the hedonic treadmill: Revising the adaptation theory of well-being. In The science of well-being (pp. 103–118): Springer. [DOI] [PubMed] [Google Scholar]
- Ekman P, & Friesen WV (1978). Facial action coding system: A technique for the measurement of facial movement. In. Palo Alto, CA: Consulting Psychologists Press. [Google Scholar]
- Emmons RA, & McCullough ME (2003). Counting blessings versus burdens: an experimental investigation of gratitude and subjective well-being in daily life. J Pers Soc Psychol, 84(2), 377–389. [DOI] [PubMed] [Google Scholar]
- Fredrickson BL, Cohn MA, Coffey KA, Pek J, & Finkel SM (2008). Open hearts build lives: positive emotions, induced through loving-kindness meditation, build consequential personal resources. J Pers Soc Psychol, 95(5), 1045–1062. doi: 10.1037/a0013262 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gelman A, & Stern H (2006). The difference between “significant” and “not significant” is not itself statistically significant. The American Statistician, 60(4), 328–331. [Google Scholar]
- Goetz JL, Keltner D, & Simon-Thomas E (2010). Compassion: an evolutionary analysis and empirical review. Psychol Bull, 136(3), 351–374. doi: 10.1037/a0018807 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Golden J, Conroy RM, Bruce I, Denihan A, Greene E, Kirby M, & Lawlor BA (2009). Loneliness, social support networks, mood and wellbeing in community-dwelling elderly. International Journal of Geriatric Psychiatry, 24(7), 694–700. doi: 10.1002/gps.2181 [DOI] [PubMed] [Google Scholar]
- Gordon AM, Stellar JE, Anderson CL, McNeil GD, Loew D, & Keltner D (2017). The dark side of the sublime: Distinguishing a threat-based variant of awe. Journal of Personality and Social Psychology, 113(2), 310–328. doi: 10.1037/pspp0000120 [DOI] [PubMed] [Google Scholar]
- Guo Y, Logan HL, Glueck DH, & Muller KE (2013). Selecting a sample size for studies with repeated measures. BMC Med Res Methodol, 13, 100. doi: 10.1186/1471-2288-13-100 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harker L, & Keltner D (2001). Expressions of positive emotion in women’s college yearbook pictures and their relationship to personality and life outcomes across adulthood. Journal of Personality and Social Psychology, 80(1), 112–124. [PubMed] [Google Scholar]
- Hawkley LC, Wroblewski K, Kaiser T, Luhmann M, & Schumm LP (2019). Are U.S. older adults getting lonelier? Age, period, and cohort differences. Psychology and Aging, 34(8), 1144–1157. doi: 10.1037/pag0000365 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Horberg EJ, Oveis C, & Keltner D (2011). Emotions as Moral Amplifiers: An Appraisal Tendency Approach to the Influences of Distinct Emotions upon Moral Judgment. Emotion Review, 3(3), 237–244. doi: 10.1177/1754073911402384 [DOI] [Google Scholar]
- Kassem AM, Ganguli M, Yaffe K, Hanlon JT, Lopez OL, Wilson JW, & Cauley JA (2017). Anxiety symptoms and risk of cognitive decline in older community-dwelling men. International Psychogeriatrics, 29(7), 1137–1145. doi: 10.1017/s104161021700045x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keltner D, & Haidt J (2003). Approaching awe, a moral, spiritual, and aesthetic emotion. Cognition and Emotion, 17, 297–314. [DOI] [PubMed] [Google Scholar]
- Keltner D, Kogan A, Piff PK, & Saturn SR (2014). The sociocultural appraisals, values, and emotions (SAVE) framework of prosociality: core processes from gene to meme. Annu Rev Psychol, 65, 425–460. doi: 10.1146/annurev-psych-010213-115054 [DOI] [PubMed] [Google Scholar]
- Kramer JH, Jurik J, Sha SJ, Rankin KP, Rosen HJ, Johnson JK, & Miller BL (2003). Distinctive neuropsychological patterns in frontotemporal dementia, semantic dementia, and Alzheimer disease. Cognitive and Behavioral Neurology, 16(4), 211–218. [DOI] [PubMed] [Google Scholar]
- Kreidler SM, Muller KE, Grunwald GK, Ringham BM, Coker-Dukowitz ZT, Sakhadeo UR, … Glueck DH (2013). GLIMMPSE: Online Power Computation for Linear Models with and without a Baseline Covariate. J Stat Softw, 54(10). doi: 10.18637/jss.v054.i10 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kubzansky LD, & Kawachi I (2000). Going to the heart of the matter: do negative emotions cause coronary heart disease? Journal of Psychosomatic Research, 48(4–5), 323–337. [DOI] [PubMed] [Google Scholar]
- Luo Y, Hawkley LC, Waite LJ, & Cacioppo JT (2012). Loneliness, health, and mortality in old age: a national longitudinal study. Soc Sci Med, 74(6), 907–914. doi: 10.1016/j.socscimed.2011.11.028 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lyubomirsky S, King L, & Diener E (2005). The benefits of frequent positive affect: does happiness lead to success? Psychological Bulletin, 131(6), 803–855. doi: 10.1037/0033-2909.131.6.803 [DOI] [PubMed] [Google Scholar]
- Mao G, Cao Y, Wang B, Wang S, Chen Z, Wang J, … Dong J (2017). The salutary influence of forest bathing on elderly patients with chronic heart failure. International journal of environmental research and public health, 14(4), 368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mather M, & Carstensen LL (2005). Aging and motivated cognition: the positivity effect in attention and memory. Trends Cogn Sci, 9(10), 496–502. doi: 10.1016/j.tics.2005.08.005 [DOI] [PubMed] [Google Scholar]
- Mehta KM, Yaffe K, Brenes GA, Newman AB, Shorr RI, Simonsick EM, … Covinsky KE (2007). Anxiety symptoms and decline in physical function over 5 years in the health, aging and body composition study. Journal of the American Geriatrics Society, 55(2), 265–270. doi: 10.1111/j.1532-5415.2007.01041.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morris JC (1993). The Clinical Dementia Rating (CDR): Current version and scoring rules. Neurology, 43(11), 2412–2414. [DOI] [PubMed] [Google Scholar]
- O’Luanaigh C, O’Connell H, Chin AV, Hamilton F, Coen R, Walsh C, … Lawlor BA (2012). Loneliness and cognition in older people: the Dublin Healthy Ageing study. Aging Ment Health, 16(3), 347–352. doi: 10.1080/13607863.2011.628977 [DOI] [PubMed] [Google Scholar]
- Ong AD, Uchino BN, & Wethington E (2016). Loneliness and Health in Older Adults: A Mini-Review and Synthesis. Gerontology, 62(4), 443–449. doi: 10.1159/000441651 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piff PK, Dietze P, Feinberg M, Stancato DM, & Keltner D (2015). Awe, the small self, and prosocial behavior. J Pers Soc Psychol, 108(6), 883–899. doi: 10.1037/pspi0000018 [DOI] [PubMed] [Google Scholar]
- R Core Team. (2017). R: A language and environment for statistical computing. In. Vienna, Austria: R Foundation for Statistical Computing [Google Scholar]
- Radloff LS (1977). The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurement, 1, 385–401. [Google Scholar]
- Rudd M, Vohs KD, & Aaker J (2012). Awe expands people’s perception of time, alters decision making, and enhances well-being. Psychological Science, 23(10), 1130–1136. [DOI] [PubMed] [Google Scholar]
- Seidlitz L, Fujita F, & Duberstein PR (2000). Emotional experience over time and self-reported depressive symptoms. Personality and Individual Differences, 28(3), 447–460. [Google Scholar]
- Shiota MN, Keltner D, & Mossman A (2007). The nature of awe: Elicitors, appraisals, and effects on self-concept. Cognition and Emotion, 21(5), 944–963. [Google Scholar]
- Shiota MN, & Levenson RW (2009). Effects of aging on experimentally instructed detached reappraisal, positive reappraisal, and emotional behavior suppression. Psychol Aging, 24(4), 890–900. doi: 10.1037/a0017896 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spitzer RL, Kroenke K, Williams JB, & Lowe B (2006). A brief measure for assessing generalized anxiety disorder: the GAD-7. Archives of Internal Medicine, 166(10), 1092–1097. doi: 10.1001/archinte.166.10.1092 [DOI] [PubMed] [Google Scholar]
- Stancato DM, & Keltner D (2019). Awe, ideological conviction, and perceptions of ideological opponents. Emotion. doi: 10.1037/emo0000665 [DOI] [PubMed] [Google Scholar]
- Stellar JE, Gordon A, Anderson CL, Piff PK, McNeil GD, & Keltner D (2018). Awe and humility. Journal of Personality and Social Psychology, 114(2), 258–269. doi: 10.1037/pspi0000109 [DOI] [PubMed] [Google Scholar]
- Stellar JE, John-Henderson N, Anderson CL, Gordon AM, McNeil GD, & Keltner D (2015). Positive affect and markers of inflammation: discrete positive emotions predict lower levels of inflammatory cytokines. Emotion, 15(2), 129–133. doi: 10.1037/emo0000033 [DOI] [PubMed] [Google Scholar]
- Valtorta NK, Kanaan M, Gilbody S, & Hanratty B (2018). Loneliness, social isolation and risk of cardiovascular disease in the English Longitudinal Study of Ageing. Eur J Prev Cardiol, 25(13), 1387–1396. doi: 10.1177/2047487318792696 [DOI] [PubMed] [Google Scholar]
- Voss MW, Heo S, Prakash RS, Erickson KI, Alves H, Chaddock L, … Kramer AF (2013). The influence of aerobic fitness on cerebral white matter integrity and cognitive function in older adults: results of a one-year exercise intervention. Human Brain Mapping, 34(11), 2972–2985. doi: 10.1002/hbm.22119 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams F (2017). The Nature Fix: Why Nature Makes Us Happier, Healthier, and More Creative. New York, NY: W. W. Norton & Company, Inc. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.