

INTRODUCTION/BACKGROUND
Among older adults, persistent musculoskeletal pain is highly prevalent, with rates ranging from 40% to 60%.1 Multisite pain contributes to significant disability among older adults.2 Persistent pain is defined as pain that extends beyond the usual period of healing, typically for longer than 3 to 6 months. Musculoskeletal disorders are recognized as a significant threat to maintaining health in older age3 and have been associated with falls, frailty, depression, anxiety, sleep disturbance, reduced mobility, and impaired cognitive function.4–8 Additionally, medical treatments for pain have been estimated to cost the United States about $300 billion annually, and this burden continues to increase.9 Unfortunately, pain may be undertreated or inappropriately managed in older adults for several reasons, including lack of identification of pain, false belief that pain is part of the aging process, cognitive impairment with variable pain presentations, patient underreporting, and limited time in clinical practice to address pain among multiple comorbid conditions.10,11 This highlights the importance of understanding the special considerations in the assessment and management of persistent musculoskeletal pain in older adults.
Persistent pain should be considered in the context of geriatric syndromes. For example, falls, frailty, cognitive decline/dementia, and sleep disturbance are often linked to persistent pain.12 Studies have shown a relationship between moderate to severe pain and accelerated memory decline and impairments in attention and executive function in community-dwelling older adults.8,13 Given the multitude of contributing factors and its close relationship with geriatric syndromes, persistent pain in older adults is regarded by some experts as a geriatric syndrome.14
Older adults are particularly prone to living with multiple illnesses, which affects treatment considerations. Defined as the presence of more than two comorbid conditions, multimorbidity is estimated to exist in at least half the geriatric population.15 Consequently, polypharmacy, often described as being prescribed five medications or more, is also common; it has been linked with falls, increased mortality, and longer hospital stays.16 This highlights the need for careful review of relative risks and benefits of medications in older adults when treating pain, because the unintended adverse effects on comorbid conditions, and polypharmacy could nullify potential benefits of another added medication.
Mental health should be carefully considered in the context of pain. The relationship between persistent pain and depression and anxiety is well-established and complex, with contributions including augmentation of functional impairment, neuroinflammatory changes, impaired social engagement, and maladaptive coping.17,18 Further-more, there seems to be a reciprocal relationship between pain and depression in older adults, with pain and depression being independent risk factors for one another.19 This association underscores the complexity of the pain experience in older adults and re-emphasizes a comprehensive biopsychosocial approach to managing persistent pain.
Within a comprehensive approach, the clinician should consider the age-related changes in organ function that have significant impact on the pharmacodynamics and pharmacokinetics of medications.20 Normal age-related decline in renal and liver function may affect drug processing, reducing clearance rates and changing efficacy. Decreased muscle mass and increased adiposity can also affect the volume of distribution of medications in older adults, affecting tolerability and efficacy of medications. These changes emphasize the importance of avoiding a “one size fits all” approach when prescribing medications to older adults.
Patients have unique pain experiences, which are heavily influenced by the type of pain, physical perception of pain, emotional state and reaction to pain, ability to cope with pain, and the patient’s personal beliefs about pain. When approaching persistent pain in older adults, it is critical to engage in collaborative care to assess and address these multiple unique contributing factors. In this review, we encourage a comprehensive assessment followed by a multidisciplinary approach to pain management that emphasizes rehabilitation and nonpharmacologic modalities, particularly appropriate for complex older adults.
GENERAL APPROACH
Assessment: History
The assessment of pain in older adults begins with obtaining a complete history that characterizes the type of pain and then further quantifies the impact the pain has on function, interference with daily activities, pain-related behaviors, and effect on psychological and social well-being. Older adults may have differing perspectives and beliefs about pain as compared with younger adults, which may affect pain reporting. Stoicism and potential fear or embarrassment about pain may contribute to underreporting of pain in this patient group.21,22 A comprehensive evaluation that includes all dimensions of the pain experience is the first step to effectively manage pain, because this information guides treatment.
The ideal source of pain history is the patient (self-report). However, for patients with cognitive impairment, dementia, and limited ability to communicate about pain, obtaining an accurate firsthand account of pain may not be feasible. As a result, several observer-based pain scales incorporate pain-based behaviors of facial response, vocalization, or body posture to characterize the pain being experienced by the patient according to level of cognitive ability.23 These tools, however, have variable interrater reliability and test-retest reliability.24 Obtaining collateral information from loved ones and caregivers (proxy-reports) is beneficial. Proxy-reporting is useful to help identify, characterize, and monitor pain for patients who are not able to communicate their pain symptoms.
Characterization of pain should include specific locations, quality, aggravating or relieving factors, and time course. With consideration of nociceptive, neuropathic, or central sensitization of pain, identification of cause when possible is useful for tailoring medical treatments, although sometimes a definitive cause cannot be identified. More than one cause may be present. Prior trials of treatments often dictate what a patient is willing to try next; therefore, clinicians should document how previous pharmacologic therapies, nonpharmacologic therapies, and prior pain-related surgeries were or were not effective. Similarly, understanding the pain in the context of other medical conditions, and how the patient prioritizes the importance of these, is also critical when deciding on a management plan. A comprehensive approach to assessment of chronic low back pain (cLBP) is found in several publications of the 2014 “Report of the Task Force on Research Standards for Chronic Low Back Pain,” where musculoskeletal pain experts and leaders convened to recommend a minimal dataset to help guide clinicians and researchers on important domains to measure when managing persistent pain.25 Using this minimal dataset as an outline, Box 1 provides a list of appropriate domains to assess for chronic musculoskeletal pain in older adults.
Box 1. Domains relevant for assessing chronic musculoskeletal pain in older adults.
Location of pain
Duration of pain (in months and years)
Characterization of pain: acute, subacute, chronic
Frequency and interference of pain
Pain intensity with numerical rating scale, based on recall from past 7 days Referred pain or radicular symptoms
Other sites of pain: gastrointestinal, headaches, widespread, etc
Prior surgeries: type, date, response
Prior treatment modalities used for pain management
Lifestyle changes
Psychological/behavioral
Physical therapy and rehabilitation
Complementary, alternative, and mind-body approaches
Pharmacotherapy
Physical function: doing chores (eg, vacuuming, yard work), climbing stairs, walking for at least 15 minutes, running errands
Mental health: depression, anxiety, post-traumatic stress disorder (as appropriate)
Sleep disturbance
Alcohol use
Tobacco use
Demographics: age, gender, race/ethnicity, employment status, highest educational attainment, body mass index
These domains and categories were adapted based on the Minimal Dataset from the 2014 Report of the NIH Task Force on Research Standards for Chronic Low Back Pain.
Adapted from Deyo RA, Dworkin SF, Amtmann D, et al. Report of the NIH Task Force on Research Standards for Chronic Low Back Pain. J Pain. 2014;15(6):569–585; with permission.
An important and often overlooked portion of the comprehensive pain assessment is understanding the patient’s expectations for what defines therapeutic success. The history facilitates this conversation, because understanding the daily impact of pain often can help identify specific areas of pain the patient would like to focus on. Although “pain-free” may not be a realistic goal, it is likely that with multimodal approaches, the patient will be able to manage the pain and associated symptoms while improving function. Anchoring conversations about pain management in patient-identified values and realistic goals of care is central, because individual-specific experiences, such as engagement in social activities, ability to enjoy favorite hobbies, and more restful sleep, all contribute to the pain experience.
Physical Examination
The physical examination for persistent pain includes visual inspection, palpation of painful sites, and quantification of strength and range of motion of the affected painful areas. When applicable, the clinician should also examine the joint contralateral to the affected joint to assess for symmetric joint involvement. Joints proximal and distal to the site of pain should be examined, specifically considering sources of referred pain, such as in the presentation of knee pain presenting with contributing hip, iliotibial band, and/or ankle pathology. Gait should be assessed for abnormalities, which can hint at underlying core issues, such as deficiencies in strength, sensation, or coordination. The Timed Up and Go Test is an efficient and valuable tool to evaluate mobility and is often used as part of a frailty assessment.26 Examination of the patient’s behaviors and reactions to elicited pain are especially useful for those with cognitive impairment, because it can help to better stratify pain intensity. Outside of these core principles, the provider should tailor the examination with location-specific maneuvers.
Imaging
Abnormal imaging findings are common in older adults. Such findings as degenerative changes of the spine or hips do not necessarily contribute meaningfully to the assessment of pain or disability. The key to interpreting imaging for musculoskeletal pain is determining whether the clinical picture correlates with the findings seen on imaging. Plain film radiography can help to assess degree of joint degeneration or investigate for other possible cause of symptoms. Findings often do not reliably correlate with pain frequency or intensity, and use of imaging often does not lead to improved outcomes.27 Because of its frequently limited utility, imaging can put unnecessary extra psychological and financial burden on a patient.28 Imaging should be considered on a case-by-case basis, especially when “red-flag” symptoms suggest an urgent issue to be assessed.
MANAGEMENT APPROACHES
The Team
The management of persistent pain in the older adult involves multiple modalities (nonpharmacologic, rehabilitative, pharmacologic, and possibly surgical) as depicted in Fig. 1. Therefore, it is important to enlist the help of a diverse team to address the various domains of pain and related comorbidities, also listed in Fig. 1. Naturally, if an older patient has multiple comorbid conditions, the number of subspecialists can become overwhelming. Clear communication, especially in large teams, is key. Each member of the team is vitally important and builds the therapeutic relationship with the patient. Counseling on the expected course of persistent pain and providing reassurance are keys to progress in therapy.
Fig. 1.
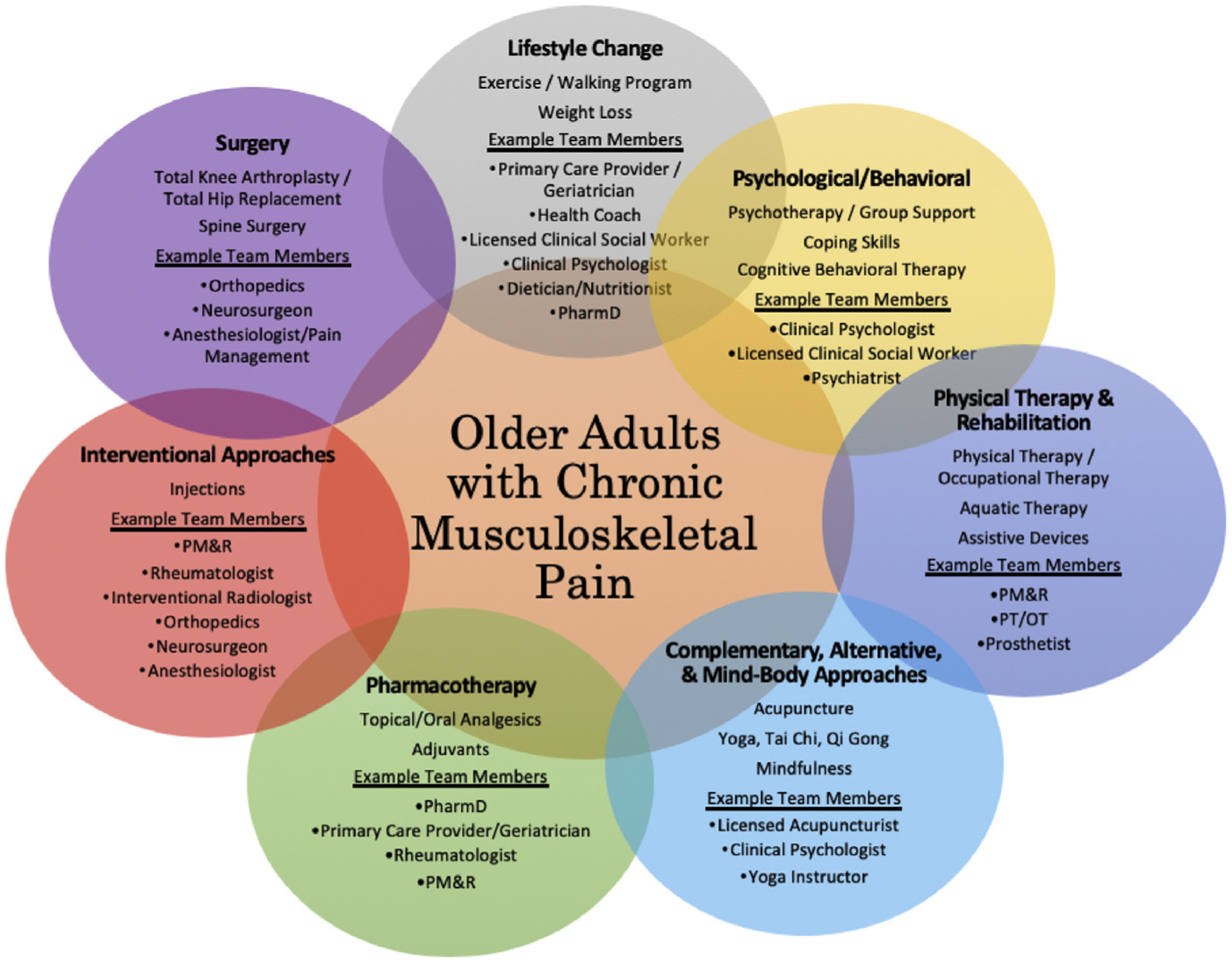
Components of multimodal interdisciplinary management of older adults with chronic musculoskeletal pain. PM&R, physical medicine and rehabilitation; PT/OT, physical therapists/occupational therapists.
Nonpharmacologic Modalities: First-Line
A comprehensive and effective treatment regimen uses multiple modalities for treatment with preference for nonpharmacologic therapies. Although these are considered first-line therapies in guidelines,29 they are unfortunately often offered after multiple trials of pharmacologic therapies and more invasive modalities. Nonpharmacologic therapies are particularly attractive for use in older adults because of the ratio of effectiveness versus safety. Nonpharmacologic modalities include physical therapy, occupational therapy, exercise (including walking) programs, psychological interventions (cognitive behavioral therapy, acceptance, pain coping skills training, cognitive restructuring, and commitment therapy),30 and complementary, alternative, and mind-body approaches and are tailored to a patient’s explicit abilities, preferences, and goals of treatment. Physical activity is consistently recommended to be a key component of any treatment plan for persistent pain in older adults.28,29,31 Exercise can reduce mortality, improve function, increase strength, reduce risk of cardiovascular disease, promote social interaction, and relieve pain. It has also been shown that providing specific physical activity advice, a plan of action, and a plan for follow-up are important in uptake and maintenance of an exercise program in older adults.32 In many patients, behavioral and psychological interventions for persistent pain are effective. For example, mindfulness programs have short- and long-term pain reduction and short-term functional improvements.33 Mindfulness and meditation therapies hold promise for improvements in pain and function, although more studies are needed to better understand their effect.34 These interventions should be considered in the context of feasibility, availability, access, cost, and patient motivation to participate.
Pharmacologic Options
When considering pharmacologic therapies, the mantra is often “start low and go slow,” titrating medications while observing for adverse effects. Table 1 outlines the classes of medications typically used in the management of persistent pain in older adults. Sometimes, an augmented pain-relieving effect is achieved when combining medications from two different drug classes. Opioids are not recommended in guidelines for managing osteoarthritis (OA). As mentioned, one must carefully consider the comorbidities and risks associated with each selected medication.
Table 1.
Common pharmacologic approaches for older adults with musculoskeletal pain
| Treatment | Indications | Safety Considerations | Recent Guidelines |
|---|---|---|---|
| Topical agents | |||
| Capsaicin | Minor muscle/joint pain (backache, strains, sprains, arthritis, bruises, cramps, muscle stiffness or soreness); neuropathic pain associated with diabetic neuropathy or postherpetic neuralgia | Wash hands with soap and water immediately after applying (unless hands are part of the treatment area) or apply with gloves Do not use within 1 h before a bath or immediately after a bath Avoid concurrent use with other topical agents or heating pad |
Conditionally recommended for knee OA Conditionally recommended against hand OA Insufficient data on hip OA35 |
| Methyl salicylate and menthol | Minor muscle/joint pain and aches (backache, strains, sprains, arthritis, bruises) | Do not apply to face, wounds, rashes, damaged skin, mucous membranes, or immediately after a bath Avoid concurrent use with other topical agents or heating pad |
Apply patch for up to 8 h (max: 2 patches/24 h) |
| Lidocaine | Postherpetic neuralgia, minor localized pain | Use lowest effective dose for pain relief for shortest duration of time (prolonged exposure increases risk for systemic absorption, potentially leading to CNS and cardiac effects) Avoid contact with water or external heat sources |
Insufficient data in OA Apply patch for up to 12 h (max: 1 patch/24 h) |
| NSAIDs | Osteoarthritis in knee and hand; may also be used for ankle, elbow, foot, or wrist; acute pain (strains, sprains, bruises) | Use lowest effective dose for pain relief for shortest duration of time (known to increase risk of adverse GI side effects and may compromise existing renal function) Do not apply to wounds, eyes, or mucous membranes |
Strongly recommended for knee OA Conditionally recommended for hand OA Insufficient data on hip OA Apply up to 4 times a day, fewer if patient is on anticoagulants or has chronic kidney disease |
| Oral medications | |||
| Acetaminophen | Minor pain and aches | Consider all sources, not to exceed 3 g/d Monitor liver function |
Conditionally recommended for knee, hip, and hand OA Limited efficacy for cLBP and not recommended for routine use36 |
| NSAIDs | Inflammatory diseases including tendinitis; mild to moderate osteoarthritis pain | Use lowest effective dose for pain relief for shortest duration of time Monitor for potential adverse GI, cardiovascular, and renal side effects |
Beer criteria recommends avoiding chronic use of NSAIDs and completely avoiding use of indomethacin and ketorolac in older patients37 Use should only be considered if there are no viable alternatives, and the patient can lower their risk of GI bleeding with use of a proton pump inhibitor or misoprostol37 |
| Tramadol | Severe pain for which nonopioid analgesics are inadequate | Monitor sodium concentration (potential risk of SIADH or hyponatremia) and respiratory depression Complex effect on cytochrome P-450 3A4 inducers, 3A4 inhibitors, or 2D6 inhibitors |
Beer criteria recommends to avoid extended release formulations and to reduce the dose of immediate release formulations37 Conditionally recommended for knee, hip, and hand OA |
| Opioids | Acute or chronic moderate to severe pain for which nonopioid analgesics are inadequate | Use lowest effective dose for pain relief for shortest duration of time Monitor for respiratory depression (particularly in patients on benzodiazepines or gabapentinoid medications concurrently) Potential effect on cytochrome P-450 3A4 inducers or 3A4 inhibitors |
Conditionally recommended against knee, hip, and OA, except when alternatives have been exhausted |
| Duloxetine | Neuropathic pain, central sensitization to pain, other persistent pain | Monitor serum sodium Risk of hyponatremia |
Conditionally recommended for knee/hip/hand OA35 Recommended for fibromyalgia38 Consider for use in cLBP |
| Gabapentin/pregabalin | Neuropathic pain, central sensitization to pain | Can have sedating effects and cause dizziness Potential to have adverse effects on mood |
Recommended for fibromyalgia38 |
Regular follow-up is critical when managing persistent pain in older adults.29 Follow-up visits assess for effectiveness of the management approach, provide an opportunity for encouragement to sustain pain-reducing behavioral changes, and allow for monitoring of adverse effects of treatments. These visits can also serve to build trust and strengthen the therapeutic alliance between the patient and provider.
COMMON MUSCULOSKELETAL CONDITIONS IN OLDER ADULTS
The principles outlined previously are a general approach to assessment and management of persistent musculoskeletal pain in older adults. The next sections outline specific considerations to consider organized by common musculoskeletal conditions in older adults.
Osteoarthritis
OA is the most common type of arthritis, and about half of all adults older than the age of 65 in the United States have doctor-diagnosed OA.39 Age is one of the strongest risk factors for OA, with others being gender (women have higher rates and report more severe symptoms), overweight/obesity, joint misalignment (varus or valgus deformity), and prior trauma.40 Although historically described as “wear and tear” of the joints, the pathophysiology of OA is appreciated as a complex interplay of inflammation, prior trauma, biochemical reactions, and metabolic derangements.41 OA most commonly affects the knees, lower vertebrae, hand, and hips. Clinically, patients present with pain, impaired joint mobility, enlarging joints, swollen joints, crepitus, and locking or clicking of the joint.
The diagnosis of OA is usually based on history and examination. Identifying functional impairment should be part of routine assessment, and one should consider use of assistive devices and orthotics when appropriate to help preserve function and improve pain. Recent guidelines do not recommend laboratory data or routine radiographs to diagnose or monitor classic presentations of OA, although it is useful in atypical presentations.
Current evidenced-based guidelines of OA recommend a comprehensive approach that emphasizes nonpharmacologic therapies.35 As highlighted in Fig. 1, exercise is also a core component of OA management. Exercise combined with dietary change yield a synergistic effect on improvement in pain and function, and it seems that the benefits in pain and function increase as the amount of weight loss increases in overweight and obese adults.42 The specific exercises must be tailored to the individual’s abilities and preferences, although a joint-preserving strategy should be used, with consideration for low-impact activities. Other nonpharmacologic options include behavior-based therapies (eg, cognitive behavioral therapy) and complementary, alternative, and mind-body approaches (eg, tai chi).
Pharmacologic treatment, listed in Table 1, includes offering topical therapies before oral therapies given the relative safety and side effect profile.35 Topical nonsteroidal anti-inflammatory drugs do not carry the high risk for renal and gastrointestinal sequelae like their systemic counterparts.43 Glucosamine and chondroitin products have limited utility for OA pain.35 Intra-articular steroid injections are used safely on an as-needed basis, although frequent dosing regimens of every 3 months have not been shown to improve pain over placebo and are also associated with increased decline of knee cartilage volume on MRI.44 There is mixed evidence of the efficacy of hyaluronic acid and hyaluronan polymer injections for the knee.45 Whenever performing an injection, one should also inquire about concurrent use of anticoagulants and take measures to minimize bleeding risk.
Surgical arthroplasty of an affected joint is considered in select patients with OA-related functional impairments who have failed conservative therapies. Older adults experience a higher rate of postoperative complications compared with younger patients but have similar benefits in quality of life,46 which highlights the need for evaluation on an individual level with shared decision-making between patient and physician.
Chronic Low Back Pain
cLBP is exceedingly common in older adults with prevalence estimates ranging between 10% and 20% in adults greater than or equal to 65 years old worldwide.47 Most cLBP does not have one definitive cause. Rather, cLBP can be thought of as a common final phenotypic pathway that is a result of several possible contributors, including spinal stenosis, hip OA, sacroiliac joint pathology, leg-length discrepancy, myofascial pain, maladaptive coping, anxiety, and depression.14 Assessment follows the domains listed in Box 1 and must rule out infection, malignancy, and cord compression in a patient who presents with red-flag symptoms. The physical examination and imaging for cLBP should be used to investigate for sources of pain including the hips, sacroiliac joints, and vertebrae (see series on Deconstructing Back Pain in Older Adults for distinct algorithms based on major presenting signs and symptoms).48–50
Successful management of cLBP involves various therapeutic modalities to optimize function, and begins with nonpharmacologic and rehabilitative modalities as depicted in Fig. 1. Physical therapy referrals should be recommended early and often. Referral to surgical specialties for spine is appropriate with any concern for central neurologic compromise or when neurologic deficits correlate with radiographic findings and/or conservative therapies have failed to provide significant improvement.
Crystal Arthritis: Gout and Pseudogout
Gout is a form of crystal arthritis characterized by an inflammatory reaction to monosodium urate in the joint. It is the most common inflammatory arthropathy in older adults and continues to increase in prevalence, likely caused by the relationship of hyperuricemia with hypertension, metabolic syndrome, renal insufficiency, and diuretic use.51 Conventionally thought of as a disease affecting middle-aged men, elderly-onset gout (EOG) is also common and can present with unique features. Notably in EOG, women are affected at higher rates by gout older than the age of 80.52 Unlike traditional gout, an initial gout flare in older adults more often presents with tophi, collections of uric acid in joints and skin. Conversely, podagra, painful swelling of the first metatarsal phalangeal joint, is less common in EOG. EOG is more likely to affect smaller joints of the hands and multiple joints at once, which can make differentiating gout from rheumatoid arthritis (RA) in older patients more difficult. When evaluating for gout, one should keep OA, RA, pseudogout, and infection in the differential diagnosis.
The diagnosis of presumed gout is often made clinically, based on the episodic nature of acute flares, although elevated inflammatory markers and serum uric acid are helpful. The diagnostic gold standard remains identification of negatively birefringent needle-like monosodium urate crystals on polarized light microscopy of synovial fluid from an affected joint. Plain film radiography can help support the diagnosis of gout, specifically erosive changes and overhanging edges of joints with preservation of joint space.
For gout flares, colchicine or corticosteroids are considered for treatment in the context of the risks to the patient and their comorbidities. Indomethacin should be avoided in older adults.37 Intra-articular steroids are a viable treatment of flares involving a few joints and pose lower risk of side effects compared with systemic steroids. Longer-term preventative therapy includes lifestyle modifications and urate-lowering therapy in certain circumstances. Patients should be counseled to reduce or eliminate intake of alcohol, shellfish, and organ meats. Urate-lowering therapy is indicated for patients who suffer from more than two flares per year, have nephrocalcinosis, or present with tophi or erosions on imaging.53 The goal uric acid level should be less than 6 mg/dL, and the initial choice of urate-lowering therapy should be allopurinol. In patients with chronic kidney disease, one can initiate allopurinol at the lowest dose and titrate to a target uric acid level while monitoring for adverse reactions.54 Febuxostat, an alternative xanthine oxidase inhibitor, may be associated with increased cardiovascular adverse effects based on data from a single clinical trial.55 When starting urate-lowering therapy, a patient should be on a prophylactic low dose of either corticosteroids or colchicine to prevent a “mobilization flare,” which is when initiation of urate-lowering therapy can paradoxically trigger an acute gout attack. Gout can typically be managed by a patient’s primary care physician, although one should consider referral to a rheumatologist if the patient continues to experience significant signs or symptoms of gout despite being on appropriate therapy, unclear source of hyperuricemia, difficulty in reaching goal serum uric acid level, or multiple and/or serious adverse effects from pharmacologic urate-lowering therapy.53
Similar to gout, calcium pyrophosphate deposition disease, or “pseudogout,” is a form of crystal arthritis characterized by an inflammatory reaction to deposition of calcium pyrophosphate into cartilaginous structure of the joint. Pseudogout has prevalence rates of about 5% to 15% for adults older than 60 years old.56 Age is a strong risk factor for pseudogout, and secondary causes include hypomagnesemia, hypercalcemia, hyperparathyroidism, and hemochromatosis. Acute pseudogout commonly presents as intermittent arthritis of the knee, wrist, or hand, although the axial skeleton can be affected. Like gout, the definitive diagnosis of pseudogout involves identification of crystals on synovial fluid microscopy; calcium pyrophosphate crystals appear as weakly positively birefringent rhomboid crystals in polarized light. Plain films are useful to aid in diagnosis when a patient is symptomatic, because chondrocalcinosis is often identified, although this can be an incidental finding in asymptomatic patients. Treatment of pseudogout flares similarly involves use of a course of steroids or colchicine. There is no medication specifically targeted to reduce the occurrence of calcium pyrophosphate deposition disease attacks but one should address reversible causes.
Rheumatoid Arthritis
RA is an autoimmune inflammatory arthritis characterized by progressive damage of synovial-lined joints and can include extra-articular manifestations. The prevalence of RA in adults greater than 60 years of age is about 2%, and incidence of RA peaks in the eighth decade of life.57 Elderly-onset RA (EORA), defined as RA with onset after the age of 65, has several unique features, including equal gender distribution; greater incidence of larger joint involvement, such as the shoulders and hips; and lower rates of rheumatoid factor positivity. EORA may follow a more indolent clinical course, although this is not always the case. Patients usually present with multiple painful and swollen joints in a symmetric distribution.
Diagnosis of RA is based on history and physical examination with laboratory data and imaging used to confirm clinical suspicion. One should investigate for extra-articular manifestations, including rheumatoid nodules, vasculitis, and interstitial lung disease, as these portend a worse prognosis. Laboratory work-up should include rheumatoid factor, anti-cyclic citrullinated peptide (CCP) antibody, inflammatory markers, complete blood count, and complete metabolic panel. Joint arthrocentesis is not essential for diagnosis but is useful to help rule out crystal arthritis or infection. Classic radiographic findings of RA include decreased joint space width, juxta-articular osteopenia or osteoporosis, and erosions. There are no specific diagnostic criteria for EORA; however, the American College of Rheumatology (ACR) and the European League Against Rheumatism (EULAR) diagnostic criteria for RA are used.58
A cornerstone of treatment of RA is disease-modifying antirheumatic drugs (DMARDs), used in a treat-to-target approach, aiming to reduce the activity of disease and prevent deformity. Depending on severity of the presenting disease, patients are started on monotherapy or combination DMARD therapy, which often includes methotrexate, hydroxychloroquine, sulfasalazine, and leflunomide. Biologic therapies are often used after a trial of nonbiologic DMARDS and now include different targets (eg, tumor necrosis factor-a, interleukin-6, JAK, CD20).59 DMARDS must be monitored closely for adverse effects including atypical infections and reactivation (tuberculosis or viral hepatitis). Corticosteroids are sometimes used at a low dose for a short period for active RA but should be avoided as a long-term treatment. Cardiovascular events are the leading cause of death in patients with RA, including older patients with RA. A patient with suspected RA should be referred to a rheumatologist as soon as possible for early, aggressive management and monitoring of the disease.
Polymyalgia Rheumatica
Polymyalgia rheumatica (PMR) is an inflammatory illness classically associated with aching and morning stiffness of the shoulders, upper arms, hips, neck, and torso. It almost exclusively affects adults older than the age of 50 and has peak incidence in the eighth to ninth decade of life with a prevalence of approximately 1% to 2% for adults older than the age of 50.60 Women are affected at about twice the rate than men. Patients can experience a symmetric polyarthritis of the hands, wrists, and knees, which makes differentiating PMR from RA challenging. PMR is a clinical diagnosis, and the ACR and EULAR have proposed classification criteria for PMR.61 Because of its overlap with giant cell arteritis (GCA), every patient with PMR should be screened for GCA. Laboratory studies typically show elevated inflammatory markers with negative autoantibodies. Imaging is not required to make a diagnosis of PMR. The mainstay of treatment of PMR is low-dose systemic glucocorticoids. Physical therapy is useful to maintain function for patients with disabling stiffness and pain.
Giant Cell Arteritis
GCA is a vasculitis affecting large-vessel and cranial arteries with a peak age incidence in the 70s. Its prevalence is estimated at 0.7%, with similar higher rates in women like that of in PMR.62 A reported 10% of patients with PMR develop GCA.63 Common symptoms include jaw claudication, changes in vision, and dysphagia, and the feared consequence of untreated GCA is irreversible blindness. The gold standard for diagnosing GCA is a temporal artery biopsy of a section at least 1 cm long with multiple sites examined. MRI, PET/computed tomography, and ultrasound can reliably identify affected vessels but cannot definitively diagnose the disease. The mainstay of treatment is high-dose systemic steroids, which should be started empirically even before confirming the diagnosis with biopsy; diagnostic yield of biopsy remains high, even if the sample is collected after initiation of steroids. The Food and Drug Administration has recently approved the interleukin-6 biologic inhibitor tocilizumab for treatment of GCA, providing a steroid-sparing option. GCA requires expedient evaluation and management by a rheumatologist and often ophthalmologist. PMR can often be managed by the primary care provider unless there are more atypical circumstances, such as substandard response to steroids, unusual presentation, or difficulty tapering steroids.
Fibromyalgia
Fibromyalgia, also referred to as central pain syndrome, is a disease characterized by increased sensitivity to pain and often presents with fatigue, mental fogginess, and sleep disturbances among other symptoms. It is identified as a centralized pain state, where individuals have abnormalities in pain processing, although changes in peripheral pain processing also have been implicated. There is no singular cause of fibromyalgia; it is the result of a complex interplay of biopsychosocial factors. Estimates of prevalence in older adults is 2% to 4%, with women being affected two times as frequently as men.64 The diagnosis of fibromyalgia is made clinically and follows the 2011 ACR diagnostic survey criteria, wherein a patient identifies widespread pain in addition to other symptoms including fatigue, depression, headache, and cramps.38 Because of the widespread distribution of pain, the differential diagnosis of fibromyalgia is expansive and may be particularly challenging in older adults with multimorbidity. One must be careful to evaluate for other causes of pain, while understanding that fibromyalgia commonly coexists in the setting of other rheumatic dieases (systemic lupus erythematosus, OA, PMR, crystal arthritis, RA), myopathy, hypothyroidism, and vitamin D deficiency.
The recommended approach to treatment of fibromyalgia is similar to the approach depicted in Fig. 1. Although pharmacologic therapies may not improve function, they may improve pain, mood, and sleep. The class of medication demonstrating the greatest efficacy is antidepressants, and it is suspected that this is caused by the pain-modifying effect of increased norepinephrine and serotonin in central pain inhibitory pathways. Duloxetine and milnacipran, both serotonin-norepinephrine reuptake inhibitors, have Food and Drug Administration approval for pain relief associated with fibromyalgia. However, potential adverse effects include sedation, orthostatic hypotension, and urinary hesitancy. Pregabalin can also help improve pain symptoms and can be considered, although starting at a low dose given at nighttime and titrating slowly. Although tramadol and tricyclic antidepressants may help relieve symptoms, their use in older adults is not encouraged because of the adverse effects on cardiovascular and urinary systems.37 Fibromyalgia is managed effectively by a primary care provider with a multidisciplinary, multimodal approach reflected in this review.38 A rheumatologist may be referred if there is concern for inflammatory arthritis or underlying autoimmune disease.
SUMMARY
Persistent musculoskeletal pain in older adults is common, resulting in tremendous disability and cost to the individual and society. Later-life pain has its own unique challenges in assessment and management; however, it is a manageable condition with a multitargeted, multimodal, and multidisciplinary approach. There are still gaps in the literature to better understand and treat pain in older adults,28,65 including broadening the evidence base for clinical trials for nonpharmacologic and pharmacologic treatments for musculoskeletal pain in older adults, because they are often excluded from these trials.66 Another issue is access to evidence-based nonpharmacologic therapies. For example, cost and accessibility of physical activity programs or mind-body modalities have been identified as significant barriers to participation in an exercise program in older adults.67 Taking the time to understand your older patient’s pain experience (including diverse domains of sleep, social isolation, fatigue), by using a comprehensive assessment/evaluation, provides the underpinnings for an effective multimodal management plan and a strong, trusting therapeutic relationship. Listening to the patient and how they respond to therapies over time is the most valuable tool.
KEY POINTS.
Musculoskeletal pain in older adults contributes to physical disability and impairments in psychosocial domains of health including social isolation, depression, and anxiety.
The manifestations of persistent pain in older adults are frequently a result of multiple contributing factors.
A comprehensive musculoskeletal pain assessment includes pain location, intensity, interference with daily life, and pain-related behaviors with attention given to how these affect and interact with comorbidities, function, mood, and cognition.
A wide array of nonpharmacologic and pharmacologic therapies exists for the treatment of persistent pain, and they can be tailored to the patient’s specific comorbidities, functional ability, preferences, and treatment goals.
Because of the inherent complexity of musculoskeletal pain in older adults, management should be multidisciplinary, multimodal, and emphasize a strong therapeutic alliance while addressing domains of pain, functionality, mental health, and social engagement.
CLINICS CARE POINTS.
Obtaining a thorough history of a patient’s level of pain, functionality, social engagement, and life at home from self-report or via proxy is central to evaluating possible contributors to pain and assessing resources available to aid the patient’s therapy.
Identifying referral processes and patterns with a diverse interdisciplinary team (as shown in Fig. 1) yields best results for complex older adults with musculoskeletal pain.
Physical activity remains a cornerstone of persistent pain management. No specific exercise type has significant superiority over the other, which means that choice of exercise can be tailored to the patient’s specific abilities and interests.
A strong therapeutic relationship between patient and provider for effective pain management is defined by commitment by both parties, realistic goal setting, and availability of both parties.
Using quantifiable metrics and goals, such as amount of time spent enjoying a (patient-identified) hobby per week, helps to gauge progress with pain-related therapies and can also help encourage the patient to engage and continue practicing therapies that are effective.
DISCLOSURE
Dr. Makris is supported by a VA HSR&D Career Development Award at the Dallas VA (IK2HX001916).
REFERENCES
- 1.Redfield RR,Mac Kenzie WR, Kent CK, et al. Prevalence of chronic pain and high-impact chronic pain among adults—United States, 2016. Morb Mortal Wkly Rep 2018;67(36):1–6. Available at: https://www.cdc.gov/nchs/nhis/index.htm. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Rundell SD, Patel KV, Krook MA, et al. Multi-site pain is associated with long-term patient-reported outcomes in older adults with persistent back pain. Pain Med 2019;20(10):1898–906. [DOI] [PubMed] [Google Scholar]
- 3.Briggs AM, Cross MJ, Hoy DG, et al. Musculoskeletal health conditions represent a global threat to healthy aging: a report for the 2015 World Health Organization World Report on ageing and health. Gerontologist 2016;56:S243–55. [DOI] [PubMed] [Google Scholar]
- 4.Lohman MC, Whiteman KL, Greenberg RL, et al. Incorporating persistent pain in phenotypic frailty measurement and prediction of adverse health outcomes. Eur J Pain 2017;72(2):216–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Blyth FM, Rochat S, Cumming RG, et al. Pain, frailty and comorbidity on older men: the CHAMP study. Pain 2008;140(1):229–35. [DOI] [PubMed] [Google Scholar]
- 6.Chen Q, Hayman ÃLL, Shmerling ÃRH, et al. Characteristics of chronic pain associated with sleep difficulty in older adults: the maintenance of balance, independent living, intellect, and zest in the elderly (MOBILIZE) Boston study. J Am Geriatr Soc 2011;59(8):1385–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Karttunen N, Lihavainen K, Sipilä S, et al. Musculoskeletal pain and use of analgesics in relation to mobility limitation among community-dwelling persons aged 75 years and older. Eur J Pain 2012;16(1):140–9. [DOI] [PubMed] [Google Scholar]
- 8.Whitlock EL, Diaz-Ramirez LG, Glymour MM, et al. Association between persistent pain and memory decline and dementia in a longitudinal cohort of elders. JAMA Intern Med 2017;177(8):1146–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gaskin DJ, Richard P, Institute of Medicine (US) Committee on Advancing Pain Research, Care, and Education. Relieving pain in America: a blueprint for transforming prevention, care, education, and research. Washington, DC: National Academies Press; 2011. [PubMed] [Google Scholar]
- 10.Chodosh J Quality indicators for pain management in vulnerable elders. Ann Intern Med 2001;135(8_Part_2):731. [DOI] [PubMed] [Google Scholar]
- 11.Gibson SJ, Helme RD. Age-related differences in pain perception and report. Clin Geriatr Med 2001;17(3):433–56. [DOI] [PubMed] [Google Scholar]
- 12.Blyth FM, Noguchi N. Chronic musculoskeletal pain and its impact on older people. Best Pract Res Clin Rheumatol 2017;31(2):160–8. [DOI] [PubMed] [Google Scholar]
- 13.Murata S, Sawa R, Nakatsu N, et al. Association between chronic musculoskeletal pain and executive function in community-dwelling older adults. Eur J Pain 2017;21(10):1717–22. [DOI] [PubMed] [Google Scholar]
- 14.Weiner DK. Deconstructing chronic low back pain in the older adult: shifting the paradigm from the spine to the person. Pain Med 2015;16(5):881–5. [DOI] [PubMed] [Google Scholar]
- 15.Marengoni A, Angleman S, Melis R, et al. Aging with multimorbidity: a systematic review of the literature. Ageing Res Rev 2011;10(4):430–9. [DOI] [PubMed] [Google Scholar]
- 16.Masnoon N, Shakib S, Kalisch-ellett L, et al. What is polypharmacy? A systematic review of definitions. BMC Geriatr 2017;17(1):230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Zis P, Daskalaki A, Bountouni I, et al. Clinical Interventions in Aging Dovepress Depression and chronic pain in the elderly: links and management challenges. Clin Interv Aging 2017;12:12–709. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Blazer DG. Depression in late life: review and commentary. J Gerontol A Biol Sci Med Sci 2003;58(3):249–65. 10.1093/gerona/58.3.m249. [DOI] [PubMed] [Google Scholar]
- 19.Chou KL. Reciprocal relationship between pain and depression in older adults: evidence from the English Longitudinal Study of Ageing. J Affect Disord 2007; 102(1–3):115–23. [DOI] [PubMed] [Google Scholar]
- 20.Ickowicz E Pharmacological management of persistent pain in older persons. J Am Geriatr Soc 2009;57(8):1331–46. [DOI] [PubMed] [Google Scholar]
- 21.Guidance on the management of pain in older people. Age Ageing 2013; 42(suppl 1):i1–57. [DOI] [PubMed] [Google Scholar]
- 22.Kaye AD, Baluch A, Scott JT. Pain management in the elderly population: a review. Ochsner J 2010;10(3):179–87. [PMC free article] [PubMed] [Google Scholar]
- 23.Achterberg W, Lautenbacher S, Husebo B, et al. Pain in dementia. Pain Rep 2019;145(3):1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Zwakhalen SM, Hamers JP, Abu-Saad HH, et al. Pain in elderly people with severe dementia: a systematic review of behavioural pain assessment tools. BMC Geriatr 2006;6(1):3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Deyo RA, Dworkin SF, Amtmann D, et al. Report of the NIH Task Force on research standards for chronic low back pain. J Pain 2014;15(6):569–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Savva GM, Donoghue OA, Horgan F, et al. Using timed up-and-go to identify frail members of the older population. J Gerontol A Biol Sci Med Sci 2013;68(4): 441–6. [DOI] [PubMed] [Google Scholar]
- 27.Jarvik JG, Gold LS, Comstock BA, et al. Association of early imaging for back pain with clinical outcomes in older adults. JAMA 2015;313(11):1143–53. [DOI] [PubMed] [Google Scholar]
- 28.Reid MC, Eccleston C, Pillemer K. Management of chronic pain in older adults. BMJ 2015;350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Makris UE, Abrams RC, Gurland B, et al. Management of persistent pain in the older patient: a clinical review. JAMA 2014;312(8):825–36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Niknejad B, Bolier R, Henderson CR, et al. Association between psychological interventions and chronic pain outcomes in older adults: a systematic review and meta-analysis. JAMA Intern Med 2018;178(6):830–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Abdulla A, Bone M, Adams N, et al. Evidence-based clinical practice guidelines on management of pain in older people. Age Ageing 2013;42(2):151–3. [DOI] [PubMed] [Google Scholar]
- 32.Taylor D Physical activity is medicine for older adults. Postgrad Med J 2014; 90(1059):26–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Morone NE, Greco CM, Moore CG, et al. A mind-body program for older adults with chronic low back pain a randomized clinical trial. JAMA Intern Med 2016; 15213:329–37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Hilton L, Hempel S, Ewing BA, et al. Mindfulness meditation for chronic pain: systematic review and meta-analysis. Ann Behav Med 2017;51(2):199–213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Kolasinski SL, Neogi T, Hochberg MC, et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Care Res (Hoboken) 2020;72(2):149–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Marcum ZA, Duncan NA, Makris UE. Pharmacotherapies in geriatric chronic pain management. Clin Geriatr Med 2016;32:705–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Investigation C. American Geriatrics Society 2019 Updated AGS Beers Criteria. J Am Geriatr Soc 2019;67(4):1–21. [DOI] [PubMed] [Google Scholar]
- 38.Clauw DJ. Fibromyalgia: a clinical review. JAMA 2014;311(15):1547–55. [DOI] [PubMed] [Google Scholar]
- 39.Barbour KE, Helmick CG, Boring M, et al. Vital signs: prevalence of doctor-diagnosed arthritis and arthritis-attributable activity limitation—United States, 2013–2015. Morb Mortal Wkly Rep 2017;66(9):246–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Zhang Y, Jordan JM. Epidemiology of osteoarthritis yuqing. Clin Geriatr Med 2011;26(3):355–69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Mora JC, Przkora R, Cruz-Almeida Y. Knee osteoarthritis: pathophysiology and current treatment modalities. J Pain Res 2018;11:2189–96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Messier SP, Resnik AE, Beavers DP, et al. Intentional weight loss in overweight and obese patients with knee osteoarthritis: is more better? Arthritis Care Res (Hoboken) 2018;70(11):1569–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Makris U Adverse effects (AEs) of topical NSAIDs in older adults with osteoarthritis (OA): a systematic review of the literature. J Rheumatol 2010;37(6): 1236–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Mcalindon TE, Lavalley MP, Harvey WF, et al. Effect of intra-articular triamcinolone vs saline on knee cartilage volume and pain in patients with knee osteoarthritis a randomized clinical trial. JAMA 2017;02111(19):1967–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Hunter DJ. Viscosupplementation for osteoarthritis of the knee. N Engl J Med 2015;372(11):1040–7. [DOI] [PubMed] [Google Scholar]
- 46.Fang M, Noiseux N, Linson E, et al. The effect of advancing age on total joint replacement outcomes. Geriatr Orthop Surg Rehabil 2015;6(3):173–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Meucci RD, Fassa AG, Xavier Faria NM. Prevalence of chronic low back pain: systematic review. Rev Saude Publica 2015;49:1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Weiner DK, Fang M, Gentili A, et al. Deconstructing chronic low back pain in the older adult—step by step evidence and expert-based recommendations for evaluation and treatment: part I: hip osteoarthritis. Pain Med 2015;16(5):886–97. [DOI] [PubMed] [Google Scholar]
- 49.Lisi AJ, Breuer P, Gallagher RM, et al. Deconstructing chronic low back pain in the older adult-step by step evidence and expert-based recommendations for evaluation and treatment: part II: myofascial pain. Pain Med 2015;16(7):1282–9. [DOI] [PubMed] [Google Scholar]
- 50.Fritz JM, Rundell SD, Dougherty P, et al. Deconstructing chronic low back pain in the older adult—step by step evidence and expert-based recommendations for evaluation and treatment. Part VI: lumbar spinal stenosis. Pain Med 2016;17(3): 501–10. [DOI] [PubMed] [Google Scholar]
- 51.De Leonardis F, Govoni M, Colina M, et al. Elderly-onset gout: a review. Rheumatol Int 2007;28(1):1–6. [DOI] [PubMed] [Google Scholar]
- 52.Agudelo CA, Wise CM. Crystal-associated arthritis in the elderly. Rheum Dis Clin North Am 2000;26(3):527–46. [DOI] [PubMed] [Google Scholar]
- 53.Khanna D, Fitzgerald JD, Khanna PP, et al. 2012 American College of Rheumatology Guidelines for Management of Gout Part I: systematic nonpharmacologic and pharmacologic therapeutic approaches to hyperuricemia. Arthritis Care Res (Hoboken) 2013;64(10):1431–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Stamp LK, Chapman PT, Barclay M, et al. The effect of kidney function on the urate lowering effect and safety of increasing allopurinol above doses based on creatinine clearance: a post hoc analysis of a randomized controlled trial. Arthritis Res Ther 2017;19(1):1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Cuenca JA, Balda J, Palacio A, et al. Febuxostat and cardiovascular events: a systematic review and meta-analysis. Int J Rheumatol 2019;2019:11–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Richette P, Bardin T, Doherty M. An update on the epidemiology of calcium pyrophosphate dihydrate crystal deposition disease. Rheumatology 2009;48(7): 711–5. [DOI] [PubMed] [Google Scholar]
- 57.Crowson CS, Matteson EL, Myasoedova E, et al. The lifetime risk of adult-onset rheumatoid arthritis and other inflammatory autoimmune rheumatic diseases. Arthritis Rheum 2011;63(3):633–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Aletaha D, Neogi T, Silman AJ, et al. Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum 2010;62(9):2569–81. [DOI] [PubMed] [Google Scholar]
- 59.Singh JA, Saag KG, Bridges SL, et al. 2015 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis. Arthritis Rheumatol 2016; 68(1):1–26. [DOI] [PubMed] [Google Scholar]
- 60.Partington RJ, Muller S, Helliwell T, et al. Incidence, prevalence and treatment burden of polymyalgia rheumatica in the UK over two decades: a population-based study. Ann Rheum Dis 2018;77(12):1750–6. [DOI] [PubMed] [Google Scholar]
- 61.Dasgupta B, Cimmino MA, Kremers HM, et al. Provisional classification criteria for polymyalgia rheumatica: a European League Against Rheumatism/American College of Rheumatology collaborative initiative. Arthritis Rheum 2012;64(4):943–54. [DOI] [PubMed] [Google Scholar]
- 62.Crowson CS, Matteson EL. Contemporary prevalence estimates for giant cell arteritis and polymyalgia rheumatica, 2015. Semin Arthritis Rheum 2017;47(2): 253–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Narváez J, Estrada P, López-Vives L, et al. Prevalence of ischemic complications in patients with giant cell arteritis presenting with apparently isolated polymyalgia rheumatica. Semin Arthritis Rheum 2015;45(3):328–33. [DOI] [PubMed] [Google Scholar]
- 64.Vincent A, Lahr BD, Wolfe F, et al. Prevalence of fibromyalgia: a population-based study in Olmsted County, Minnesota, utilizing the Rochester Epidemiology Project. Arthritis Care Res (Hoboken) 2013;65(5):786–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Makris UE, Misra D, Yung R. Gaps in aging research as it applies to rheumatologic clinical care. Clin Geriatr Med 2017;33(1):119–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Bowen E, Nayfe R, Milburn N, et al. Do decision aids benefit patients with chronic musculoskeletal pain? A systematic review. Pain Med 2020;21(5):951–69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Bethancourt HJ, Rosenberg DE, Beatty T, et al. Barriers to and facilitators of physical activity program use among older adults. Clin Med Res 2014;12(1–2):10–20. [DOI] [PMC free article] [PubMed] [Google Scholar]