

Abstract
Rural children from Benin, west Africa were evaluated with the Mullen Scales of Early Learning (MSEL) at one year of age and then at six years with the Kaufman Assessment Battery for Children (KABC-II), the visual computerized Tests of Variables of Attention (TOVA), and the Bruininks-Oseretsky Test (BOT-2) of motor proficiency (N=568). Although both the MSEL and KABC-II were available to the assessors in French, instructions to the mother/child were in local language of Fon. Mothers were evaluated with the Edinburgh Postpartum Depression Scale (EPDS), Caldwell HOME Scale, educational level and literacy, and a Socio-Economic Scale – also in their local language (Fon). After adjusting for maternal factors, MSEL cognitive composite was correlated with KABC-II with moderate effect sizes, but not with TOVA scores. Overall eta-squared effect for the multivariate models were moderately to strongly correlated (.07 to .37). Neurodevelopmental assessments in early childhood adapted cross-culturally are predictive of school-age neuropsychological cognitive ability.
Keywords: Child development, neurocognition, Mullen Scales of Early Learning, Kaufman Assessment Battery for Children, Tests of Variables of Attention, Africa
The principal purpose of this study is to relate a western-based neurodevelopmental assessment in early childhood to neuropsychological performance as they reach school-age, and we propose to do so in a longitudinal assessment of a cohort of children in a rural resource-constrained area of Benin, West Africa. This cohort was originally assessed at one-year of age with the Mullen Scales of Early Learning (MSEL), a developmental assessment much like the Bayley Scales of Infant Development but designed to be more feasible in resource-constrained settings (Kammerer, Isquith, & Lundy, 2013; Mullen, 1995). In this study, rural Benin infants’ gender (female), quality of the developmental milieu in the home as assessed by the Caldwell HOME scale, maternal education and nonverbal cognitive ability (Raven’s Progressive Matrices) were associated with a higher performance on the infant’s MSEL cognitive composite.
The Caldwell HOME and family wealth were also associated with the MSEL Gross Motor development of the infant (Bodeau-Livinec, Cot, Koura, & Boivin, 2013), and these findings were confirmed with a subgroup of this cohort when assessed with MSEL at 3 to 4 yrs of age (Bodeau-Livinec et al., 2019). Our group has also documented that maternal helminth infection and anemia during pregnancy (Mireku, Boivin, et al., 2015; Mireku et al., 2016; Mireku, Davidson, et al., 2015b), as well as delayed growth (Mireku, Cot, Massougbodji, & Bodeau-Livinec, 2020) were also predictive of poor MSEL cognitive performance at one-year of age in this cohort.
Because of the paucity of neurocognitive testing developed and normed in sub-Saharan African countries (Semrud-Clikeman et al., 2016), several tests assessing child neurodevelopment developed in Western countries have been used in this region (Bangirana, John, et al., 2009a). The principal objective of the present study was to compare the predictive correlation of a neurodevelopmental performance-based assessment previously validated with one-year old children in Benin Africa at one year of age (Koura et al., 2013; Mireku et al., 2020), with a western-based neuropsychological battery used to assess that same children at 6 years of age, after being piloted at our present study site (Bodeau-Livinec et al., 2019; Amanda Garrison et al., 2021).
When attempting to establish the validity of the construct domains for a neurodevelopmental or neuropsychological assessment in a new cultural context (e.g., in sub-Sahara Africa), it is necessary to consider a range of factors (Gladstone et al., 2008; Holding et al., 2016; Kammerer et al., 2013). Such validation should involve not only convergent or predictive validity (i.e., to demonstrate that the construct correlates with things that it should correlate with), but also divergent/discriminant validity (i.e., to demonstrate that the construct does not correlate with things that it should not correlate with).
To illustrate, a multi-trait multi-method matrix is often utilized to assess these factors (Gladstone, Jones, Mtitimila, Maleta, Ashorn, & Smyth, 2006; Gladstone, Jones, Mtitimila, Maleta, Ashorn, Smyth, et al., 2006; Gladstone et al., 2008) such as what was done with the Malawi Developmental Assessment Tools (MDAT) in a cohort of cerebral malaria survivors and their non-malarial counterparts in Malawi (Boivin, Mohanty, et al., 2019). Likewise, the factor validation of the KABC has been documented for school-age children in the Democratic Republic of Congo (DRC) (Giordani et al., 1996), with Ugandan cerebral malaria (CM) survivors at school age (Bangirana, Musisi, et al., 2009), and with children affected by HIV in South Africa and throughout the sub-Sahara (Chernoff et al., 2018; van Wyhe, van de Water, Boivin, Cotton, & Thomas, 2017). Boivin and colleagues have also validated the KABC and the TOVA with rural and urban children in Laos (SE Asia), in terms of both factor and construct validity (Boivin, Chounramany, Giordani, Xaisida, & Choulamountry, 1996).
In the Boivin et al (2019) Malawi study, the MDAT at preschool age was significantly correlated with all of the KABC-II global performance domains at school age in a cohort of cerebral malaria (CM) survivors. However, they did not obtain these significant predictive correlations between the MDAT and the KABC-II in the non-malarial control cohort of children, except for the global domain of planning/reasoning (P<0.01). Boivin and Sikorskii (2013) completed a similar longitudinal analysis in Ugandan CM survivors, evaluating the predictive validity of the Mullen Scales of Early Learning (MSEL) at preschool-age with KABC-II and Tests of Variables of Attention (TOVA) performance several years later at school-age. The MSEL was significantly predictive of all KABC-II and TOVA global performance outcomes (P<0.01) after controlling for age at school-age testing, SES, gender, and anthropometric measures of growth (M. Boivin & Sikorskii, 2013).
In the present study we will evaluate if our neurodevelopmental assessment at one year of age (MSEL) corresponds to neuropsychological performance for this same cohort of rural West African children at six years of age (KABC-II & TOVA). We expect to obtain significant predictive correlations between the MSEL (preschool) and the KABC-II and TOVA at school age in a cohort of African children not highly at risk for brain/behavior injury (CM or HIV). Findings supporting this hypothesis would have important implications for the longitudinal neurodevelopmental and neuropsychological evaluation of sub-Saharan children from early through middle childhood.
One implication is that western-based tests could be adapted to the cultural context of sub-Saharan African children to evaluate how early factors of risk and/or resilience can impact on neuropsychological trajectory throughout the developmental lifespan (Boivin & Giordani, 2013). Such findings with western-based longitudinal assessment assessments would also help gauge the long-term benefits of early medical and behavioral interventions with neurologically at risk children, such as with CM, HIV, and other CNS infections (Boivin, Ruisenor-Escudero, & Familiar-Lopez, 2016).
Finally, should western-based neurodevelopmental and neuropsychological assessments effectively longitudinally assess such brain/behavior developmental trajectories in rural West African children, it would have important implications for the science of child development. We propose that the valid application of such western-based assessments with West African children would support that such assessments can capture and characterize the integrity of a foundational brain/behavior omnibus perhaps universal to neurocognitive function in children (Boivin, Dobias, & Giordani, 2013; Boivin & Giordani, 2009).
METHODS
Human Subject Research Approvals:
This study was conducted in accordance with the ethical guidelines of the APA, with IRB approval for the initial evaluation of children at 1 year of age for a study entitled “Anemia in Pregnancy in Benin and Impact on Cognitive Function in Childhood” from New York University School of Medicine School of Medicine IRB (Protocol 09–1253), Michigan State University (BIRB #10–525), and the University of Abomey-Calavi’s School of Medicine institutional review boards (IRB). For the follow-up assessment at 6 yrs of age, IRB approval was for the protocol entitled “EXposition au PLomb et au manganèse et Risques pour l’Enfant: effet sur le développement neurocognitif et physique de l’enfant à six ans au Bénin” (Projet EXPLORE) from University of Abomey-Calavi Medical School, the Committee of Ethical Research of the Applied Biomedical Sciences Institute (CER-ISBA) and the French Institut de Recherche pour le Développement’s (IRD) Consultative Ethics Committee. The present manuscript is primarily an observational study pertaining to the predictive correlation of early childhood neurodevelopmental assessment with neuropsychological assessment of these same children at school age. The study took place with rural mothers and their children in Benin, West Africa. Written consent was obtained from the parent(s) of each child in this study.
Study Site and Population.
The study population included children born of mothers enrolled from 2009 through 2010 in a trial comparing 2 intermittent preventive treatments for malaria and for helminth infection as part of the MiPPAD (Malaria in Pregnancy Preventive Alternative Drugs) study in Benin, West Africa. Mothers were also instructed for good antenatal care practices as per Benin Ministry of Health prenatal care guidelines (Jennings, Yebadokpo, Affo, & Agbogbe, 2010). In accordance with Benin Ministry of Health guidelines for prenatal care, during pregnancy all women in the present study were prophylactically treated for helminth infection and provided with iron and folic acid supplements. Pregnant women were followed from the second trimester of pregnancy through delivery, and offspring were followed from birth to 12 months of life. Of these, 747 offspring were assessed with the Mullen Scales of Early Learning (MSEL). within the TOVI project at one year of age (Koura et al., 2013). The aim of the overall project was to assess the impact of maternal hemoglobin concentration during pregnancy on offspring development (Mireku et al., 2016; Mireku, Davidson, et al., 2015a) and anemia from poor nutrition on subsequent growth and cognitive development (Mireku et al., 2020).
The study was conducted in the district of Allada, a semi-rural area located 50 km north of Cotonu, the capital of Benin. The study participants were recruited in three health centers: Attogon, Sékou, and Allada (see Table 1). Risk factors pertaining to gestational maternal anemia, malaria, helminth infection, food insecurity, maternal illiteracy and impoverishment as they pertain to MSEL child development outcomes have been well described in the present population of children in prior published work from the present study sites in rural Benin just north (40 to 60 km) of the capital Cotonou (Bodeau-Livinec et al., 2013; Bodeau-Livinec et al., 2019; Mireku, Boivin, et al., 2015; Mireku et al., 2020; Mireku et al., 2016; Mireku, Davidson, et al., 2015a; Mireku et al., 2018). The most recent characterization of the maternal and child risk factors for the present study population involves an evaluation of the relationship between child lead exposure and malaria risk (A. Garrison et al., 2019). Our group also has evaluated the relationship between early helminths exposure and other risk factors on subsequent neurodevelopmental and neuropsychological outcomes used in the present study within the present cohort of children (Amanda Garrison et al., 2021).
Table 1.
Descriptive characteristics are presented with the mean followed by the standard deviation (StDev). Frequencies followed by percentage by category for these measures. Measures are for child participant at one year of age unless otherwise noted.
| Characteristic | Mean (StDev) or N (%) |
|---|---|
| Child’s sex | |
| Male | 270 (52%) |
| Female | 251 (48%) |
| Child age in months at Mullen Scales Early Learning Test | 12.12 (0.68) |
| Child age in months at KABC/TOVA/BOT Tests | 74.93 (4.91) |
| Interval in months between 1 yr and 6 yr old assessments | 62.81 (4.93) |
| Child in school at the age of KABC/TOVA/BOT Tests | |
| Yes | 354 (68%) |
| No | 162 (31%) |
| Missing | 5 (1%) |
| Home Observation for Measurement of the Environment (HOME) Inventory | 26.93 (2.22) |
| Maternal Edinburg Postpartum Depression Scale (EPDS) | 7.98 (4.05) |
| Socio-economic status (SES) score | 5.79 (2.49) |
| Maternal education | |
| No Schooling | 333 (64%) |
| Partial Primary Schooling | 110 (21%) |
| Primary Schooling Complete | 22 (4%) |
| Secondary Schooling and more | 56 (11%) |
| Maternal marital status | |
| Single/Divorced/Widowed | 33 (6%) |
| Married (monogamous) | 243 (47%) |
| Married (polygamous) | 235 (45%) |
| Missing | 10 (2%) |
| Child evaluation clinic | |
| Attogon | 354 (68%) |
| Sekou | 131 (25%) |
| Allada | 36 (7%) |
| Child history of severe malaria | |
| Yes | 114 (22%) |
| No | 401 (77%) |
| Missing | 6 (1%) |
Data Collection Procedure.
Although both the MSEL and KABC-II were available to the assessors in French, instructions to the mother/child were in local language of Fon. Mothers were evaluated with the Edinburgh Postpartum Depression Scale (EPDS), Caldwell HOME Scale, educational level and literacy, and a Socio-Economic Scale – also in their local language (Fon).
At enrollment when the child was about a year of age (Figure 1), a questionnaire on socioeconomic status, and the Edinburgh Postnatal Depression Scale (EPDS). for the mother (Cox, Holden, & Sagovsky, 1987a) and the Home Observation for the Measurement of the Environment (HOME) Inventory were administered (Caldwell, 2003). Between June 2016 and October 2018 when the cohort of children approached six years of age, child development was assessed by research psychologists and nurses trained specifically in the use of the Kaufman Assessment Battery in Children – 2nd edition (KABC-II) at local health centers. The MSEL and KABC-II instructions were spoken in Fon, the local language. Study nurses and the coordinator psychologist (RZ) were specifically trained by a native speaking pediatrician (JA), the lead author (MJB), and the principal investigator (FB-L) to administer the MSEL, the KABC-II, and the HOME.
Figure 1.

Diagram of mother/child enrollments at birth, one year, and at six years studies in rural Benin.
Measures
Mullen Scales of Early Learning (MSEL).
The MSEL covers various domains to assess childhood development (Mullen, 1995). The five Mullen Scales are Gross Motor, Fine Motor, Visual Reception, Receptive Language, and Expressive Language. After scoring all items and computing raw scores, these raw scores are converted into a standardized score (T score) for each of the five Mullen Scales according to American norms. T scores from the Fine Motor, Visual Reception, Receptive Language, and Expressive Language scales are converted into the Early Learning Composite score, which provides the general cognitive factor underlying all cognitive performance. With copyright permission from the publisher the MSEL was translated into French (and back translated to ensure accuracy of translation) for the benefit of the research assistants, who then spoke scripted instructions to child and mother in the local language of Fon, as described previously (Amanda Garrison et al., 2021; Koura et al., 2013; Mireku, Boivin, et al., 2015; Mireku et al., 2016; Mireku, Davidson, et al., 2015a)
Kaufman Assessment Battery for Children, second edition (KABC-II).
The 2nd edition of this test was published in 2004. In addition to simultaneous processing and sequential processing, and compared with the original KABC, it includes the global domain measures of learning and planning (reasoning). This test was already available in French (by Les Editions du Centre des Psychologie Apliquee (ECPA); French translation published and distributed exclusively by ECPA with the permission of AGS Publishing, Pearson Products Inc.) normed on a population of children in France and previously used as such in (Bodeau-Livinec et al., 2019). The French version of the KABC-II was also used for the present study, and quality assurance (QA) was maintained with the independent evaluation of each tester on a monthly basis (Bodeau-Livinec et al., 2019; Amanda Garrison et al., 2021). Each tester each month submitted a videotape of his/her KABC-II administration to an evaluative team in Uganda as part of a QA process described elsewhere (Ruisenor-Escudero et al., 2019). Spoken instructions to the child by the examiner were in the local language of Fon.
The KABC has been previously validated in francophone Africa (Giordani et al., 1996) and the KABC-II has been validated in Uganda (Bangirana, Musisi, et al., 2009) and in a multi-site study across six study sites in four different sub-Saharan countries (Chernoff et al., 2018). A comprehensive review of the validity of the KABC use in pediatric HIV in South Africa is also available (van Wyhe et al., 2017). In this study the KABC-II Luria model was used to assesses global cognitive abilities using the Mental Processing Index (MPI) standardized for age using norms from children in France. For 6-year old children, the MPI is a composite indicator of cognitive ability from the domains of 1) Sequential Processing (short-term memory), 2) Simultaneous Processing (visual-spatial processing and problem solving), 3) and Learning (immediate and delayed memory). Additional KABC-II measures of Delayed Recall (based on the Learning subtests), and Nonverbal (NVI) performance on language independent subtests were also used in the present analyses. Subtests were administered even if out of age-range for the purpose of future analyses by age-band, but only scaled if within appropriate age-ranges.
Test of Variables of Attention, version 8 (TOVA).
The TOVA (www.tovatest.com). is a computerized test measuring key component of attention and self-control, variability (consistency), response time (speed), commissions (impulsivity), and omissions (focus and vigilance) (Greenberg, 1993). Scoring is based on establishing whether response times and attention is at the normal range for the sex and age of the child with ADHD scores more negative than −1.8 considered suggestive of ADHD for USA norms. It has previously been validated with school-age children in a six site/four country in sub-Sahara Africa (Chernoff et al., 2018).
Bruininks-Oseretsky Test of Motor Proficiency, 2nd edition (BOT-2), Brief Form.
The BOT-2 is a standardized test comprehensively assessing gross and fine motor skills in children ages 4–21 years through eight subtests: Fine Motor Precision, Fine Motor Integration, Manual Dexterity, Bilateral Coordination, Balance, Running Speed and Agility, Upper Limb Coordination, and Strength (Bruininks & Bruininks, 2005). The Brief form of the BOT-2 has 12 items, each a game-like task. Composite scores include Fine Manual Control, Manual Coordination, Body Coordination, Strength and Agility and Total Composite Score. Total scores (0–72) are standardized to US norms by age. It has previously been adapted for use in gauging neuromotor disease effects in sub-Sahara Africa in the context of pediatric HIV (Boivin et al., 2018; Boivin, Chernoff, et al., 2019; Boivin et al., 2010; Ruel et al., 2012).
Socioeconomic status.
We used two variables to assess family socioeconomic status family wealth and maternal education when the child was assessed at one year of age. The family wealth scale has been described elsewhere (Koura et al., 2013). Briefly, it was assessed using a scoring instrument incorporating a checklist of material possessions (radio, television, bike, motorbike, and car), possession of cows and access to electricity. Maternal education included as schooled or unschooled at the primary school level at least.
Child’s history of severe malaria illness, requiring hospitalization for treatment either of severe malaria anemia or cerebral malaria (Bangirana et al., 2016; Paul Bangirana et al., 2014; Boivin et al., 2007; John et al., 2008) was collected.
The Home Observation for the Measurement of the Environment (HOME) (Caldwell & Bradley, 1979).
This evaluation of the quality of the developmental environment and quality of caregiving by the mother was done in the home of the children and their mother when the child was assessed at one year of age, when it was adapted and piloted for this setting (Koura et al., 2013).
Edinburgh Postpartum Depression Scale (EPDS).
This maternal questionnaire has been used to assess depressive symptoms when the child was assessed at one year of age (Cox, Holden, & Sagovsky, 1987; Hanlon et al., 2008; Kakyo, Muliira, Mbalinda, Kizza, & Muliira, 2012). Scores derived from the EPDS were analyzed as a continuous variable. The EPDS, already available in French, but any spoken instructions to the mother were in Fon by our study psychologist and several nurses as a team, in that they knew the local dialect spoken my mothers in at our two study sites (Koura et al., 2013).
Statistical analysis.
Maternal and child measures were summarized with means and standard deviations for continuous variables and counts and percentage for categorical variables. Composite cognition scores and gross motor scores from the MSEL were related to the KABC-II, TOVA, and BOT-2 scores at six years of age using regression analysis. Following unadjusted analyses with one predictor (MSEL composite or gross motor), multivariable general linear models were fit controlling for maternal socio-demographic measures, depression, child’s sex, history of malaria illness, time between two tests, HOME, and test site. These factors were selected a priori based on subject matter expertise and literature documenting these factors as potentially important for neuropsychological outcomes. In addition to statistical significance of the explanatory variables, we evaluated the effect sizes for the variance explained by these factors. Effect sizes were estimated as eta squared, with .01 being small, .09 medium, and .25 large effect sizes. All statistical tests were two-sided at .05 level of significance. All the analyses were performed with SAS 9.4 software.
RESULTS
Comparability of mother/child dyads assessed throughout present study and those lost to follow-up.
As noted in Figure 1, 568 of the 1027 mother/child dyads of singleton births enrolled in the at birth following maternal prenatal care were followed through both the neurodevelopmental assessment at 1 year and neuropsychological assessment at 6 years of age in the present study. Of these, 521 (270 boys, 251 girls) had complete assessments on all test performance and covariates for inclusion in the final multiple regression analyses (Table 1).
Mothers of children followed to six years compared to those not enrolled or lost to follow-up tended to be almost a year younger in age (p=0.04), monogamous in marriage (p=0.04), and of lower SES (p=0.01) (see Supplemental Table 1). However, mothers of children lost to follow-up between 1 and 6 years of age were significantly more likely to have had prior pregnancies before the birth of the target child (p<0.001) (See Supplemental Table 2). They were also significantly disproportionately more likely to have been enrolled at the Sekou Clinic (p<0.001), and to come from the lowest SES quartile (p<0.001) (see Supplemental Table 3).
The two groups of mothers (those of children assessed through 6 years versus lost to follow-up between 1 and 6 years) were comparable on number of prior pregnancies before target child, weight and height at enrollment, prior schooling (yes/no), and the gestational age of the target child at birth (Supplemental Table 1). They were also comparable on child gender, child gestational weight and age at birth, maternal anemia and/or malaria during pregnancy, maternal blood lead level, and HOME caregiving quality total (Supplemental Table 2) and maternal depression (Supplemental Table 3).
Descriptive statistics for the study sample.
The sample had slightly more (52%). males than females (49%). (Table 1). Majority of mothers were married and did not have formal schooling, and the summary statistics for the MSEL, KABC-II, TOVA, and BOT-2 are in Table 2.
Table 2.
Descriptive statistics (Mean followed by standard deviation (StDev)) for developmental outcomes at 1 year of age (Mullen Scales of Early Learning, (MSEL)) and 6 years of age (Kaufman Assessment Battery for Children, 2nd edition (KABC-II); Test of Variables of Attention (TOVA) visual test; Bruininks-Oseretsky Test, 2nd edition (BOT-2) of motor proficiency. MSEL is standardized (cognitive composite index) and scaled (gross motor, fine motor, visual reception, receptive language, expressive language) for age and gender using American norms, and the KABC-II composite indices (MPI, NVI) and global domains (Sequential Processing, Simultaneous Processing, Learning, Delayed Recall) are standardized for age using French norms. The TOVA index calculated based on age and gender using American normative mean of 0, range from −10.0 (poor). to +10.0 (good). TOVA D’prime signal detection standard measure calculated from American norms for age, gender. BOT-2 total standard score for short version is based on American norms for age and gender (M-50, SD=10).
| Outcome | Mean (St Dev) |
|---|---|
| MSEL – cognitive composite standardized score | 98.65 (13.54) |
| MSEL scaled gross motor score | 51.27 (14.13) |
| MSEL scaled fine motor score | 50.16 (9.54) |
| MSEL scaled visual reception score | 50.49 (10.46) |
| MSEL scaled expressive language score | 49.30 (10.48) |
| MSEL scaled receptive language score | 46.55 (6.69) |
| KABC-II standardized mental processing index (MPI) | 60.93 (11.73) |
| KABC-II standardized sequential processing global score | 80.62 (14.41) |
| KABC-II standardized simultaneous processing global score | 55.67 (9.46) |
| KABC--II standardized learning global score | 77.46 (12.19) |
| KABC-II standardized delayed recall global score | 78.52 (11.73) |
| KABC-II standardized non-verbal index (NVI) | 52.20 (7.60) |
| TOVA percent omission errors | 29.95 (18.94) |
| TOVA percent commission errors | 22.92 (20.04) |
| TOVA correct response time in msec | 771.29 (123.89) |
| TOVA correct response time variability in msec | 318.94 (68.38) |
| TOVA ADHD index | −2.63 (2.75) |
| TOVA D’prime | 1.51 (0.90) |
| TOVA D’prime standardized score | 70.88 (17.38) |
| BOT-2 scaled total score | 39.75 (8.96) |
Associations of measures at 1 years of age with measures at 6 years of age.
In the unadjusted analyses, the MSEL composite and gross motor scores were statistically significant predictors of the KABC-II (Figure 2) and BOT-2 (Figure 3) scores, but not of the TOVA scores (Table 3). The effect sizes reflected by partial eta squared were small to medium and ranged from .02 to .04 for the correlation of all KABC-II (except for simultaneous processing) and BOT-2 scores by the MSEL. For the TOVA, the effects of the MSEL were below the cut-point of .01 for small effect size (Table 3). These results did not change in an appreciable way in the adjusted analyses. For the multivariable models for the KABC-II and BOT-2 scores, the overall percent of the variance explained (R-squared or eta-squared) was moderate to high (.08 to .38), with high eta-squared observed for the correlation of the BOT-2 scores by the MSEL composite or gross motor score. Much of the variance in BOT-2 was explained by child’s sex (eta-squared=.245, Table 4). Other factors had small to moderate (clinic site, time between tests, SES, and HOME scores) or very small (maternal education, depression, child’s history of malaria illness) contributions to the explained variance of the BOT-2 scores (Table 4). For the KABC MPI scores, child’s sex had very small effects consistent with its standardization by age, thus very small effects of age support the tool’s utility in this cultural context. Except for child’s sex in correlation of the BOT-2 scores, moderate to large overall eta-squared was not largely due to a single predictor, with the MSEL scores consistently contributing small to moderate effects into the correlation of the KABC-II and BOT-2 scores.
Figure 2.

Scatterplot and least-squares regression fit for relationship between Mullen Scales of Early Learning cognitive ability composite at 1 year of age, and the Kaufman Assessment Battery for Children (2nd edition). Mental Processing Composite standard score at 6 years of age for the present Benin study cohort.
Figure 3.
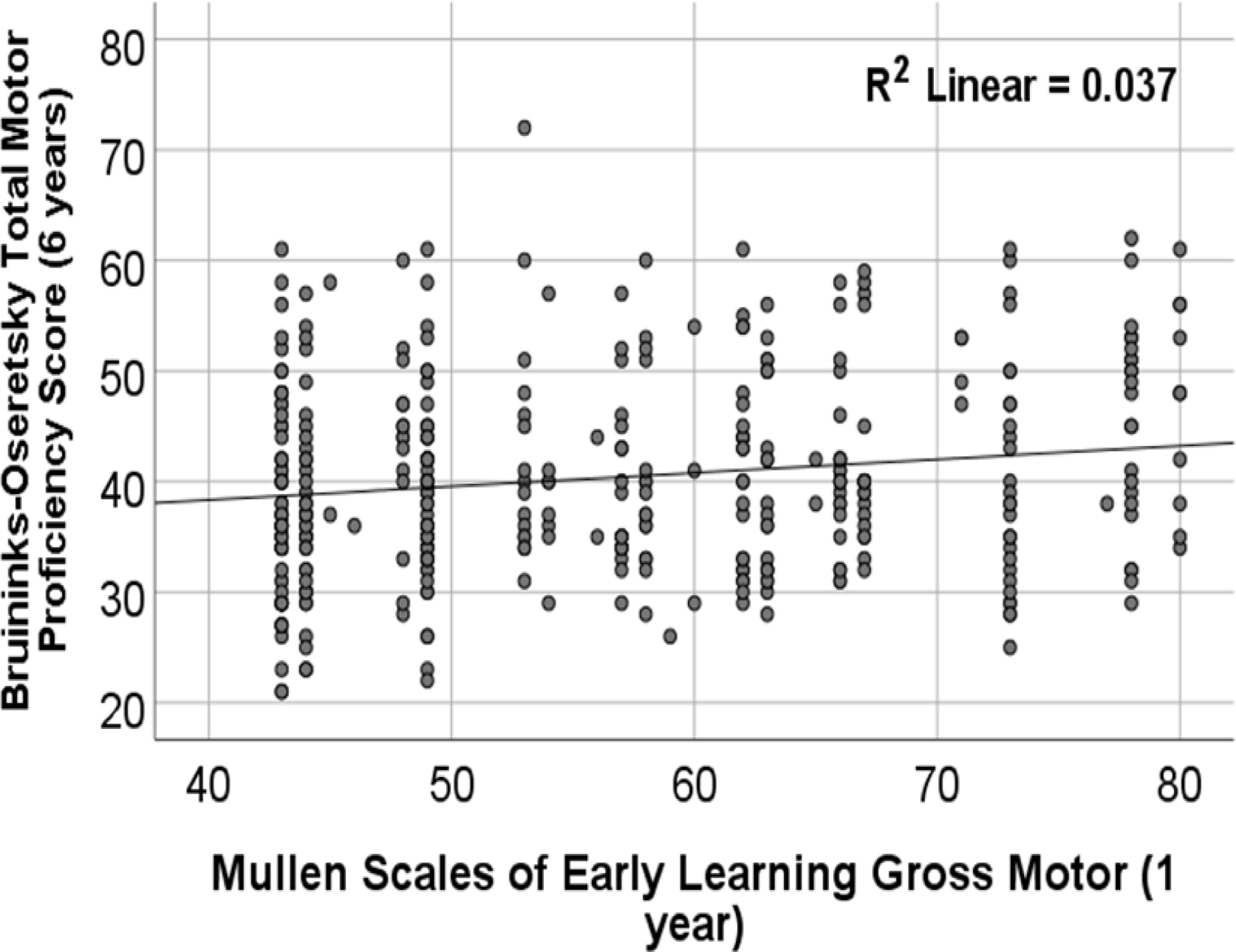
Scatterplot and least-squares regression fit for relationship between Mullen Scales of Early Learning Gross Motor standard score at 1 year of age and the Bruininks-Oseretsky Test (2nd edition). of motor proficiency standard score at 6 years of age for the present Benin study cohort.
Table 3.
Associations of outcomes at 6 years of age with outcomes at 1 year of age. Small eta squared is 0.01, medium eta squared is 0.09, large eta squared is 0.25. In the unadjusted analyses, partial eta squared equals R-squared for the model. In the adjusted models, model eta squared equals R-squared. Statistically significant effects (p<.05) are bolded.
| Cognitive and Motor Tests at Six Years of Age for Study Children | Predictor: Mullen Scales of Early Learning (MSEL) - Cognitive Composite Standardized Score at One Year of Age | Predictor: Mullen Scales of Early Learning (MSEL) - Gross Motor Scaled Score at One Year of Age | ||||
|---|---|---|---|---|---|---|
| Unadjusted partial eta squared (p-value) | Adjusted partial eta squared (p-value) | Multivariable model eta squared | Unadjusted partial eta squared (p-value) | Adjusted partial eta squared (p-value) | Multivariable model eta squared | |
| Kaufman Assessment Battery for Children, 2nd edition (KABC-II) | ||||||
| Mental Processing Index (MPI) | .032 (<.001) | .024 (<.001) | .18 | .019 (.002) | .006 (.088) | .16 |
| Sequential Processing | .036 (<.001) | .025 (<.001) | .19 | .037 (<.001) | .019 (.002) | .18 |
| Simultaneous Processing | .013 (.001) | .008 (.044) | .16 | .017 (.003) | .001 (.035) | .16 |
| Learning | .025 (<.001) | .016 (.004) | .14 | .021 (<.001) | .001 (.040) | .13 |
| Delayed Recall | .020 (.001) | .012 (.016) | .13 | .036 (<.001) | .017 (.003) | .14 |
| Nonverbal Index | .015 (.005) | .017 (.003) | .12 | .019 (.002) | .012 (.016) | .11 |
| Tests of Variables of Attention (TOVA) visual test | ||||||
| ADHD Total Index | .0001 (.802) | <.0001 (.998) | .07 | .007 (.066) | .001 (.437) | .08 |
| D Prime Signal Detection | .0003 (.684) | .0004 (.664) | .14 | .001 (.554) | .001 (.431) | .14 |
| D Prime Signal Detection standardized score | .0003 (.709) | .003 (.262) | .0004 (.676) | .22 | ||
| Percent Omission Errors (inattention) | .0003 (.703) | .0003 (.716) | .07 | .001 (.571) | .003 (.236) | .07 |
| Percent Commission Errors (impulsivity) | .001 (.500) | <.001 (.914) | .07 | .002 (.305) | <.0001 (.972) | .07 |
| Correct Response Time Variability (msec) | .0001 (.805) | <.001 (.930) | .11 | .009 (.033) | .002 (.323) | .11 |
| Correct Response Time Latency (msec) | .001 (.434) | <.001 (.891) | .10 | .002 (.397) | .0002 (.754) | .10 |
| Bruininks-Oseretsky Test, 2nd edition (BOT-2) of motor proficiency | ||||||
| Total Motor Proficiency Standardized Score | .016 (.004) | .021 (.001) | .37 | .037 (<.001) | .012 (.004) | .38 |
Table 4.
The effects of covariates other than the MSEL composite at 1 year of age on the KABC MPI, TOVA D prime signal detection (standard score) and ADHD index, and BOT-2 total score at 6 years of age
| Covariate | KABC MPI | KABC Sequential Processing | KABC Simultaneous Processing | KABC Learning | KABC Delayed Recall | KABC Non-verbal Index | TOVA D’prime | TOVA ADHD | BOT-2 |
|---|---|---|---|---|---|---|---|---|---|
| Partial eta squared (p-value) | Partial eta squared (p-value) | Partial eta squared (p-value) | Partial eta squared (p-value) | Partial eta squared (p-value) | Partial eta squared (p-value) | Partial eta squared (p-value) | Partial eta squared (p-value) | Partial eta squared (p-value) | |
| Maternal education | .019 (<.001) | .025 (.049) | .006 (.372) | .039 (<.001) | .038 (<.001) | .004 (.541) | .004 (.558) | .001 (.910) | .003 (.681) |
| Clinic site | .030 (.023) | .043 (<.001) | .037 (<.001) | .009 (.116) | .004 (.393) | .039 (<.001) | .004 (.407) | .002 (.656) | .050 (<.001) |
| Child’s sex | .011 (.019) | .018 (.003) | .0002 (.739) | .010 (.023) | .014 (.008) | .0005 (.632) | .016 (.007) | .045 (<.001) | .246 (<.001) |
| History of malaria | .0004 (.186) | .005 (.099) | .003 (.220) | .002 (.748) | .001 (.425) | .010 (.023) | .001 (.530) | .007 (.073) | .003 (.195) |
| Time between assessments | .019 (.002) | .001 (.424) | .089 (<.001) | .008 (.046) | .004 (.154) | .026 (<.001) | .098 (<.001) | .009 (.045) | .088 (<.001) |
| Maternal depression | .001 (.443) | .0002 (.774) | .003 (.206) | .004 (.140) | .003 (.259) | .012 (.013) | .001 (.581) | .0004 (.661) | .004 (.181) |
| HOME score | .007 (.062) | .007 (.070) | .004 (.155) | .002 (.375) | .005 (.127) | .005 (.110) | .003 (.267) | .001 (.537) | .012 (.015) |
| SES score | .019 (.002) | .031 (<.001) | .012 (.014) | .012 (.016) | .015 (.007) | .016 (.005) | .005 (.120) | .005 (.133) | .030 (<.001) |
DISCUSSION
In our West African study sample, the MSEL composite cognitive performance at 1 year of age was highly predictive of all the KABC-II cognitive domains (memory, learning, visual-spatial analysis and problem solving, reasoning/planning subtests) and their global performance indices. In contrast, the MSEL cognitive composite was not predictive of TOVA vigilance attention or impulsivity measures or their global performance indicators (ADHD index, D prime signal detection). This divergence between the two types of neuropsychological outcomes (KABC-II cognitive ability versus TOVA attention/impulsivity) attests to the distinction between these two disparate neurocognitive tests as they pertain to neurodevelopmental cognitive development. Finally, the MSEL Gross Motor score at 1-year of age was highly predictive of BOT-2 motor proficiency and KABC-II cognitive ability at 6 years, providing further evidence of the importance of early motor development in establishing the trajectory of neurodevelopment through early and middle childhood (Abubakar, Holding, van Baar, Newton, & van de Vijver, 2008; Abubakar, Van Baar, Van de Vijver, Holding, & Newton, 2008; Abubakar, Van de Vijver, et al., 2008).
We also documented the strong correspondence between these maternal factors and performance on the KABC-II at 6 years, like KABC-II findings with school-age Ugandan children (Bangirana, John, et al., 2009a; Bangirana, Musisi, et al., 2009). We previously demonstrated such construct validity with the KABC-II with a separate cohort sub-Saharan African children (Boivin et al., 2020; Boivin, Maliwichi-Senganimalunje, et al., 2019; Chernoff et al., 2018). In all these studies, poorer overall KABC-II performance measures were significantly associated with known risk factors for poor child development. These included lower HOME caregiving quality and lower SES level.
We also observed significant gender differences favoring boys in the present study for the TOVA attention/impulsivity and BOT-2 motor proficiency overall performance totals. This was not the case for the KABC-II. These gender differences are consistent with what was observed with the KABC-II, TOVA, and BOT-2 in a validation study of HIV positive, HIV-exposed noninfected, and nonexposed/noninfected school-age children at six study sites in four African countries (South Africa, Malawi, Zimbabwe, Uganda) (Chernoff et al., 2018). This gives us more confidence in the viability of applying neurodevelopmental followed by neuropsychological assessments from early to middle childhood in a longitudinal assessment of at-risk children in the sub-Sahara.
HOME caregiving quality and SES were significantly correlated with both the raw and standardized KABC-II MPI global cognitive performance measure of the children in the present study. This finding has been noted with the KABC-II in a previous study of Ugandan school-age children (Bangirana, John, et al., 2009b). It has also been documented in that the quality of the HOME-assessed developmental milieu was significantly related to KABC-II performance at school age for Ugandan children (Bangirana, John, et al., 2009b; Bangirana, Menk, John, Boivin, & Hodges, 2013; Bangirana, Seggane, et al., 2009).
Unexpectedly, maternal depression was not associated with either neurodevelopment at 1 year of neuropsychological performance at 6 years in our Benin children, although it was associated with all the other maternal factors in our present sample (HOME caregiving quality, maternal Raven Progressive Matrices, SES, maternal educational level). Maternal depression of Ugandan mothers with HIV can be associated with quality of caregiving as measured by the HOME (Bass et al., 2016; Boivin, Bangirana, N. Nakasuja, et al., 2013; Boivin, Bangirana, N. Nakasujja, et al., 2013) although socio-economic factors can contribute to maternal depression and anxiety in communities in Uganda for mothers with HIV (Familiar, Murray, et al., 2016; Familiar, Nakasujja, et al., 2016).
One limitation of our study is that the HOME was assessed at TOVI study entry when the present cohort of Benin children were 1 year of age. It might have changed by the time these children were 6 years. However, the predictive correlations for the HOME were just as strong for the KABC-II as for the MSEL in the present cohort. Likewise, maternal education, SES, and maternal nonverbal cognitive ability should not vary much our neurodevelopmental assessment at one year and subsequent neuropsychological assessment at six years. However, it is worth noting that the neurocognition, especially assessed by the MSEL, may be more sensitive to socioeconomic factors in infancy and very early childhood than would be the case for the KABC-II at 6 years (Boivin, Maliwichi-Senganimalunje, et al., 2019).
Another important aspect for our present findings is that the overall MSEL standardized scores at 1 year of age were well within the normal range using American-based norms for adjusting for age. This was not the case for the KABC-II at 6 years of age, like previously observed findings with the Benin children (Bodeau-Livinec et al., 2019). The Bodeau-Livinec et al (2019) study was a cross-sectional (by year of age) study of older siblings of our present TOVI Benin cohort of children. Children 3 to 4 yrs of age were assessed with the MSEL and older siblings (5 to 6 yrs of age) were assessed with the KABC-II. Six-year-olds performed significantly better than five-year-olds on the raw score comparisons on the KABC-II subtests as would be expected, but not so when their scores were standardized using American norms. This was likely because as our normal school-age kids get older, they tend to lose ground on the KABC-II normatively, necessitating the need to control for age beyond the standardization of global test scores (Bergemann et al., 2012). As in the present findings, Caldwell HOME measures were predictive of MSEL cognitive composite and KABC-II MPI overall performance and maternal Raven Progressive Matrices score; while SES was predictive of KABC-II overall performance but not the MSEL.
We have also previously documented in a longitudinal assessment through early childhood with the MSEL, that as children get older, standardized scores tended to decrease for rural Ugandan children (Bass et al., 2017; Boivin, Nakasujja, et al., 2017). This may reflect the differential impact of the environment and culture on such standardized developmental assessments as children age in HICs versus LMICs. Such longitudinal trends through early and middle childhood might reflect the culture fairness of the test as the breadth and depth of such assessment increase with age (Boivin & Giordani, 2009, 2013). Such trends over time for African children might also reflect the modifying impact of the risk factors known to cause or compound developmental delays (e.g., asymptomatic or symptomatic chronic infection such as malaria, helminths, schistosomiasis; anemia and micronutrient deficiencies, toxic environmental exposure factors) (Boivin, Kakooza, Warf, Davidson, & Grigorenko, 2015). The fact that the MSEL predicted KABC-II performance as well as it did, despite these normative trends (using American norms for the MSEL age adjustment and French norms for the KABC-II) is a testament to the accessibility and robust nature of such neurocognitive assessments, even when surmised by Western-based tests that can only be adapted to such radically different cross-cultural contexts (Boivin & Giordani, 2009).
Irrespective, it should not be taken as a given that a Western-based cognitive performance test measures the same constructs across cultural settings, as has been considered by other child development assessment specialists working in the sub-Saharan African setting (Holding et al., 2016). Attempts should first be made to establish the invariance of the constructs across settings, and only after invariance has been established should the test be interpreted as measuring the same cognitive ability construct across those settings. Conducting this kind of analysis often requires larger samples collected across very different LMICs for cross-cultural comparison (Kitsao-Wekulo et al.). Nonetheless, it would be important to see in future studies if the MSEL in very early childhood taps into the same domains in a 6-year old in the aftermath of serious neurodevelopmental risk affecting early brain-behavior development, such as cyanide toxicity in poorly processed cassava for Congolese children for which such “bitter” cassava is the basic food staple (Boivin, Okitundu, et al., 2017; Boivin, D. Okitundu, et al., 2013; Kashala-Abotnes et al., 2019; Kashala-Abotnes et al., 2018). Another example might be in the neurodevelopmental (MSEL). and neuropsychological (KABC-II, TOVA, BOT-2) effects of perinatal HIV infection (Bangirana et al., 2017; Boivin et al., 2010; Ruel et al., 2012), or with early exposure to cerebral malaria (Bangirana et al., 2016; Paul Bangirana et al., 2014; Boivin et al., 2007; John et al., 2008).
Boivin and colleagues have demonstrated in other studies that there is a robust factor structure as well as construct and correspondence validity for the KABC when administered with other neuropsychological tests in sub-Sahara Africa (SSA) (Boivin, Giordani, & Bornefeld, 1995; Chernoff et al., 2018; Giordani et al., 1996). The same has been demonstrated with the KABC and TOVA in Laos (Boivin et al., 1996). As established by Boivin and colleagues in Malawi, other neurodevelopmental tests developed and normed in the African context, such as the MDAT, also have strong predictive validity with the KABC-II and TOVA (Boivin, Mohanty, et al., 2019). Tests such as the MDAT and Kilifi Developmental Inventory have been developed in SSA allowing for more relevant tools and dimensions assessed (Gladstone et al., 2010; Holding et al., 2016; Holding et al., 2004; P. a. A. Holding, A., 2005).
Boivin and colleagues (2019) concluded in their review that there is consensus that valid and relevant early developmental measures are predictive of neuropsychological and cognitive performance in middle childhood and beyond (Pollitt, 1999; Sutcliffe, Soo, & Barnes, 2010). However, up until now these was not much published evidence for the predictive validity of early developmental assessments for school-age cognitive and behavioral outcomes, with African school-age children. This was especially the case in resource-constrained settings for African children at risk from infectious disease, poor nutrition, or other factors such as toxic environmental exposures (Boivin et al., 2015; Suchdev et al., 2017). Our present findings with rural children in Benin at risk in terms of anemia (Mireku et al., 2016; Mireku, Davidson, et al., 2015b), food insecurity (Mireku et al., 2020), helminth exposure (Amanda Garrison et al., 2021; Mireku, Boivin, et al., 2015), lead exposure (A. Garrison et al., 2019), and other risk factors is an important step in establishing the predictive validity of early childhood development measures with neuropsychological measures at school-age in such LMIC settings (Bodeau-Livinec et al., 2019).
The early childhood development and school-age neuropsychological tests that we used in this study that have been well validated and highly contextualized in a variety of African settings (Boivin et al., 2016; Chernoff et al., 2018). Even so, they can still be systematically biased in a different cultural, rural/urban, religious, or linguistic African context (Semrud-Clikeman et al., 2017). Even if the capacity and resources were available to validate a given test for a given context, Western tests and their corresponding norms from HICs still tend to be more readily available and have already undergone a great deal of development and validation for those country settings (Boivin et al., 2013; Boivin & Giordani, 2009). We emphasize again that the purpose of this study is NOT to emphasize on the utility of one test other another. Instead, our purpose in this study was to empirically evaluate an important issue in the adaptation of western-based assessments for children. That is, whether Western-based neurodevelopmental and subsequent neuropsychological tests adapted to the SSA context can have strong predictive correlation with neuropsychological evaluation at school-age when used longitudinally throughout the early lifespan for monitoring neurocognitive integrity in at-risk children. We have done so with a reasonable large study cohort of boys and girls who are representative of a large peri-natal care intervention cohort of rural Benin mothers form several clinics in a rural area of West Africa.
Illingworth in the 1950’s concluded that children who were exceptionally low or high in the developmental curve early on had development measures that were predictive of their cognitive abilities later in childhood. In contrast, younger children well within the “normal” range of early childhood development performance had much less predictive measures of cognitive ability at school age (Illingworth, 1958; Illingworth & Birch, 1959). In fact, early neuropsychological performance indicative of normal brain/behavior development can be predictive of later clock drawing and clock copying abilities in children at school age (Dilworth, Greenberg, & Kusché, 2004). Likewise, at school age academic performance can predict age-related memory decline in later adulthood (Pudas & Rönnlund, 2019), suggesting the potential for the predictive validation of a continuum of brain/behavior neuropsychological assessments throughout the developmental life span.
In terms of the predictive correlation of early childhood to school-age neurocognitive assessments, Torras-Mana and colleagues (2016) documented that Bayley-III scales could significantly predict later cognitive performance (including the KABC) in Spanish children diagnosed with Autism Spectrum Disorder (ASD) (Torras-Mana, Gomez-Morales, Gonzalez-Gimeno, Fornieles-Deu, & Brun-Gasca, 2016). Our present findings are also consistent with those of Boivin et al. (2019). In that Malawian-based such with CM surviors and their non-malaria controls, Boivin and colleagues used the MDAT, which was a development test validated for Malawian children (Gladstone et al., 2010), to significantly predict KABC-II performance when these children reached school age. Our present findings did the same using the MSEL (western-based test) in predicting KABC-II performance in at-risk but non-CM surviving children in Benin.
The above findings along with prior relevant research, taken together, lead us to the conclusion that our longitudinal assessment findings with this cohort of sub-Saharan African children further establishes the following important paradigmatic tenet: that western-based neurodevelopmental and neuropsychological tests used to evaluate brain/behavior performance capture foundational domains for characterizing “risk and resilience” factors for children in the cross-cultural context. The implication of this conclusion is that such evidence helps us better understand how, across the life span, ecological necessity sculpts culturally specific cognitive ability profiles, doing so upon a universal brain/behavior omnibus (Boivin et al., 2013; Boivin & Giordani, 2009). In so doing, our present findings obtained in a longitudinal evaluation of at-risk rural west African children enhances our understanding of a universal brain/behavior omnibus perhaps applicable to the science of child development globally (Sternberg, 2004).
Supplementary Material
Human Subjects Protection.
This study was conducted in accordance with the ethical guidelines of the APA, with IRB approval for the initial evaluation of children at 1 year of age for a study entitled “Anemia in Pregnancy in Benin and Impact on Cognitive Function in Childhood” from New York University School of Medicine (Protocol 09–1253), Michigan State University (BIRB #10–525), and the University of Abomey-Calavi’s Medical School institutional review boards (IRB). For the follow-up assessment at 6 yrs of age, IRB approval was for the protocol entitled “EXposition au PLomb et au manganèse et Risques pour l’Enfant: effet sur le développement neurocognitif et physique de l’enfant à six ans au Bénin” (Projet EXPLORE) from University of Abomey-Calavi Medical School, the Committee of Ethical Research of the Applied Biomedical Sciences Institute (CER-ISBA) and the French Institut de Recherche pour le Développement’s (IRD) Consultative Ethics Committee. The present manuscript is primarily an observational study pertaining to the predictive correlation of early childhood neurodevelopmental assessment with neuropsychological assessment of these same children at school age. The study took place with rural mothers and their children in Benin, West Africa. Written consent was obtained from the parent(s) of each child in this study.
Acknowledgements:
We would like to thank the entire staff of the three health centers (Allada, Attogon, Sékou). just north of Cotonou, Benin. We also thank the study participants at those centers. We gratefully thank our field team who collected the data and provided the medical care. We thank Micheline Garel and Nour Tabbara for translation of Mullen Scales of Early Learning. These findings were originally presented as part of a symposium Neurodevelopmental assessment in low resource areas : implementation and outcomes” at the annual meeting of the International Neuropsychological Society, Denver, Colorado, 8-Feb-2020.
Funding:
The assessment at one-year of age was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development at the National Institutes of Health (grant number R21 HD060524) to MJB, LD, MC, AM, and FB-L. The follow-up assessment study at six years of age was funded by a Fondation de France award to FB-L. The study sponsors had no role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication.
Footnotes
Conflict of Interest: None of the authors have any conflicts of interest or financial disclosures pertaining to this study.
Contributor Information
Michael J. Boivin, Michigan State University Departments of Psychiatry and of Neurology & Ophthalmology, University of Michigan Department of Psychiatry.
Roméo Zoumenou, Institut de Recherche pour le Développement (IRD).
Alla Sikorskii, Michigan State University Department of Psychiatry.
Nadine Fievet, Mère et Enfant Face aux Infections Tropicales, Université Paris Descartes, Paris, France.
Jules Alao, Mère et Enfant Face aux Infections Tropicales, Université Paris Descartes, Paris, France.
Leslie Davidson, Department of Epidemiology, Mailman School of Public Health, Columbia University.
Michel Cot, Université Paris Descartes, Paris, France.
Achille Massougbodji, Centre d’Etude et de Recherche sur le Paludisme Associé à la Grossesse et à l’Enfance (CERPAGE), Université d’Abomey-Calavi, Cotonou, Benin.
Florence Bodeau-Livinec, École des hautes études en santé publique (EHESP), EPOPé team, UMR1153, F-35000 Rennes, France.
REFERENCES
- Bangirana P, John CC, Idro R, Opoka RO, Byarugaba J, Jurek AM, & Boivin MJ (2009a). Socioeconomic predictors of cognition in Ugandan children: Implications for community based interventions. PLoS One, 4(11), e7898. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bangirana P, Menk J, John CC, Boivin MJ, & Hodges JS (2013). The association between cognition and academic performance in Ugandan children surviving malaria with neurological involvement. PLoS One, 8(2), e55653. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bangirana P, Musisi S, Allebeck P, Giordani B, John CC, Opoka RO, … Boivin MJ (2009). A preliminary investigation of the construct validity of the KABC-II in Ugandan children with prior cerebral insult. African Health Sciences, 9(3), 186–192. [PMC free article] [PubMed] [Google Scholar]
- Bangirana P, Opoka RO, Boivin MJ, Idro R, Hodges JS, & John CC (2016). Neurocognitive domains affected by cerebral malaria and severe malarial anemia in children. Learn Individ Differ, 46, 38–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bangirana P, Opoka RO, Boivin MJ, Idro R, Hodges JS, Romero RA, … John CC (2014). Severe malarial anemia is associated with longterm neurocognitive impairment. Clinical Infectious Diseases, 59(3), 336–344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bangirana P, Ruel TD, Boivin MJ, Pillai SK, Giron LB, Sikorskii A, … Achan J (2017). Absence of neurocognitive disadvantage associated with paediatric HIV subtype A infection in children on antiretroviral therapy. J Int AIDS Soc, 20(2). doi: 10.1002/jia2.25015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bangirana P, Seggane M, Allebeck P, Giordani B, John CC, Opoka OR, … Boivin MJ (2009). A preliminary examination of the construct validity of the KABC-II in Ugandan children with a history of cerebral malaria. Afr Health Sci, 9(3), 186–192. [PMC free article] [PubMed] [Google Scholar]
- Bass JK, Nakasujja N, Familiar-Lopez I, Sikorskii A, Murray SM, Opoka R, … Boivin MJ (2016). Association of caregiver quality of care with neurocognitive outcomes in HIV-affected children aged 2–5 years in Uganda. AIDS Care, 28 Suppl 1, 76–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bass JK, Opoka R, Familiar I, Nakasujja N, Sikorskii A, Awadu J, … Boivin M (2017). Randomized controlled trial of caregiver training for HIV-infected child neurodevelopment and caregiver well being. AIDS, 31(13), 1877–1883. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bergemann TL, Bangirana P, Boivin MJ, Connett JE, Giordani BJ, & John CC (2012). Statistical approaches to assess the effects of disease on neurocognitive function over time. J Biomet Biostat(S7:016), 1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bodeau-Livinec F, Cot M, Koura KG, & Boivin MJ (2013). Assessing the effects of maternal anemia on child development in Benin. In Boivin & Giordani B (Eds.), Specialty Topics in Pediatric Neuropsychology (Vol. Neuropsychology of African Children: Risk and Resilience, pp. 203–214). New York, NY: Springer. [Google Scholar]
- Bodeau-Livinec F, Davidson LL, Zoumenou R, Massougbodji A, Cot M, & Boivin MJ (2019). Neurocognitive testing in West African children 3–6 years of age: Challenges and implications for data analyses. Brain Res Bull, 145, 129–135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boivin M, & Sikorskii A (2013). The correspondence between early and middle childhood neurodevelopmental assessments in Malawian and Ugandan children. London, UK, Save the Children Institute of Education; University of London; London School of Hygiene & Tropical Medicine. Workshop Report: page 2. [Google Scholar]
- Boivin MJ, Augustinavicius JL, Familiar-Lopez I, Murray SM, Sikorskii A, Awadu J, … Bass JK (2020). Early Childhood Development Caregiver Training and Neurocognition of HIV-Exposed Ugandan Siblings. J Dev Behav Pediatr, 41(3), 221–229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boivin MJ, Bangirana P, Byarugaba J, Opoka RO, Idro R, Jurek AM, & John CC (2007). Cognitive impairment after cerebral malaria in children: a prospective study. Pediatrics, 119(2), e360–366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boivin MJ, Bangirana P, Nakasuja N, Page CF, Shohet C, Givon D, … Klein PS (2013). A year-long caregiver training program to improve neurocognition in preschool Ugandan HIV-exposed children. J Dev Behav Pediatr, 34(2), 269–278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boivin MJ, Bangirana P, Nakasujja N, Page CF, Shohet C, Givon D, … Klein PS (2013). A year-long caregiver training program improves cognition in preschool Ugandan children with human immunodeficiency virus. J Pediatr, 163, 1409–1416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boivin MJ, Barlow-Mosha L, Chernoff MC, Laughton B, Zimmer B, Joyce C, … Team IPS (2018). Neuropsychological performance in African children with HIV enrolled in a multisite antiretroviral clinical trial. AIDS, 32(2), 189–204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boivin MJ, Chernoff M, Fairlie L, Laughton B, Zimmer B, Joyce C, … Palumbo PE (2019). African Multi-Site 2-Year Neuropsychological Study of School-Age Children Perinatally Infected, Exposed, and Unexposed to Human Immunodeficiency Virus. Clin Infect Dis doi: 10.1093/cid/ciz1088 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boivin MJ, Chounramany C, Giordani B, Xaisida S, & Choulamountry L (1996). Validating a cognitive ability testing protocol with Lao children for community development applications. Neuropsychology, 10(4), 588–599. [Google Scholar]
- Boivin MJ, Dobias K, & Giordani B (2013). Chapter 16 Postscript: Towards a universal brain/behavior omnibus in the neuropsychology of African children. In M. J. B. a. B. G. S. T. i. Neuropsychology P (Ed.), Neuropsychology of Children in Africa: Perspectives on Risk and Resilience, (Vol. Specialty Topics in Pediatric Neuropsychology, pp. 329–333). New York, NY: Springer Science+Business Media. [Google Scholar]
- Boivin MJ, & Giordani B (2009). Neuropsychological assessment of African children: evidence for a universal basis to cognitive ability. In Chiao JY (Ed.), Cultural Neuroscience: Cultural Influences on Brain Function. (Vol. 178, pp. 113–135). New York, NY: Elsevier Publications. [DOI] [PubMed] [Google Scholar]
- Boivin MJ, & Giordani B (Eds.). (2013). Neuropsychology of Children in Africa: Perspectives on Risk and Resilience (Vol. 1). New York, NY: Springer. [Google Scholar]
- Boivin MJ, Giordani B, & Bornefeld B (1995). Use of the Tactual Performance Test for cognitive ability testing with African children. Neuropsychology, 9(3), 409–417. [Google Scholar]
- Boivin MJ, Kakooza AM, Warf BC, Davidson LL, & Grigorenko EL (2015). Reducing neurodevelopmental disorders and disability through research and interventions. Nature, 527(7578), S155–160. doi: 10.1038/nature16029 [DOI] [PubMed] [Google Scholar]
- Boivin MJ, Maliwichi-Senganimalunje L, Ogwang LW, Kawalazira R, Sikorskii A, Familiar-Lopez I, … Fowler MG (2019). Neurodevelopmental effects of ante-partum and post-partum antiretroviral exposure in HIV-exposed and uninfected children versus HIV-unexposed and uninfected children in Uganda and Malawi: a prospective cohort study. Lancet HIV, 6(8), e518–e530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boivin MJ, Mohanty A, Sikorskii A, Vokhiwa M, Magen JG, & Gladstone M (2019). Early and middle childhood developmental, cognitive, and psychiatric outcomes of Malawian children affected by retinopathy positive cerebral malaria. Child Neuropsychol, 25(1), 81–102. [DOI] [PubMed] [Google Scholar]
- Boivin MJ, Nakasujja N, Familiar-Lopez I, Murray SM, Sikorskii A, Awadu J, … Bass JK (2017). Effect of Caregiver Training on the Neurodevelopment of HIV-Exposed Uninfected Children and Caregiver Mental Health: A Ugandan Cluster-Randomized Controlled Trial. J Dev Behav Pediatr, 38(9), 753–764. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boivin MJ, Okitundu D, Makila-Mabe B, Sombo MT, Mumba D, Sikorskii A, … Tshala-Katumbay D (2017). Cognitive and motor performance in Congolese children with konzo during 4 years of follow-up: a longitudinal analysis. Lancet Glob Health, 5(9), e936–e947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boivin MJ, Okitundu D, Makila-Mabe Bumoko G, Sombo MT, Mumba D, Tylleskar T, … Tshala-Katumbay D (2013). Neuropsychological effects of konzo: a neuromotor disease associated with poorly processed cassava. Pediatrics, 131(4), e1231–1239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boivin MJ, Ruel TD, Boal HE, Bangirana P, Cao H, Eller LA, … Wong JK (2010). HIV-subtype A is associated with poorer neuropsychological performance compared with subtype D in antiretroviral therapy-naive Ugandan children. AIDS, 24(8), 1163–1170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boivin MJ, Ruisenor-Escudero H, & Familiar-Lopez I (2016). CNS impact of perinatal HIV infection and early treatment: the need for behavioral rehabilitative interventions along with medical treatment and care. Curr HIV/AIDS Rep, 13(6), 318–327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bruininks RH, & Bruininks BD (2005). BOT2: Bruininks-Oseretsky Test of Motor Proficiency Second Edition. Minneapolis, MN: Pearson Assessments. [Google Scholar]
- Caldwell BM, & Bradley RH (1979). Home Observation for Measurement of the Environment. Little Rock, AR: University of Arkansas Press. [Google Scholar]
- Chernoff MC, Laughton B, Ratswana M, Familiar I, Fairlie L, Vhembo T, … Boivin MJ (2018). Validity of Neuropsychological Testing in Young African Children Affected by HIV. J Pediatr Infect Dis, 13(3), 185–201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cox JL, Holden JM, & Sagovsky R (1987). Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. British Journal of Psychiatry, 150, 782–786. [DOI] [PubMed] [Google Scholar]
- Dilworth JE, Greenberg MT, & Kusché C (2004). Early neuropsychological correlates of later clock drawing and clock copying abilities among school aged children. Child Neuropsychology, 10(1), 24–35. [DOI] [PubMed] [Google Scholar]
- Familiar I, Murray S, Ruisenor-Escudero H, Sikorskii A, Nakasujja N, Boivin MJ, … Bass JK (2016). Socio-demographic correlates of depression and anxiety among female caregivers living with HIV in rural Uganda. AIDS Care, 28(12), 1541–1545. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Familiar I, Nakasujja N, Bass J, Sikorskii A, Murray S, Ruisenor-Escudero H, … Boivin MJ (2016). Caregivers’ depressive symptoms and parent-report of child executive function among young children in Uganda. Learn Individ Differ, 46, 17–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garrison A, Boivin M, Khoshnood B, Courtin D, Alao J, Mireku M, … Bodeau-Livinec F (2021). Soil-transmitted helminth infection in pregnancy and long-term child neurocognitive and behavioral development: a prospective mother-child cohort in Benin. PLoS Negl Trop Dis, in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garrison A, Khoshnood B, Courtin D, Milet J, Garcia A, Massougbodji A, … Bodeau-Livinec F (2019). Blood lead level in infants and subsequent risk of malaria: A prospective cohort study in Benin, Sub-Saharan Africa. PLoS One, 14(7), e0220023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Giordani B, Boivin MJ, Opel B, Dia Nseyila D, Diawaku N, & Lauer RE (1996). Use of the K-ABC with children in Zaire, Africa: An evaluation of the sequential-simultaneous processing distinction within an intercultural context. International Journal of Disability, Development and Education, 43(1), 5–24. [Google Scholar]
- Gladstone M, Jones A, Mtitimila E, Maleta K, Ashorn P, Smyth RL, & Lancaster G (2006). Standardization of a culturally appropriate developmental assessment tool for a rural African setting. Archives of Diseases of Childhood. [Google Scholar]
- Gladstone M, Lancaster G, Jones A, Maleta K, Mtitimila E, Ashorn P, & Smyth R (2008). Can Western developmental screening tools be modified for use in a rural Malawian setting? Archives of Diseases of Childhood, 93, 23–29. [DOI] [PubMed] [Google Scholar]
- Gladstone M, Lancaster GA, Umar E, Nyirenda M, Kayira E, van den Broek NR, & Smyth RL (2010). The Malawi Developmental Assessment Tool (MDAT): the creation, validation, and reliability of a tool to assess child development in rural African settings. PLoS Med, 7(5), e1000273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Greenberg LM (1993). The T.O.V.A (Version 6.X) (Computer Program). Los Alamitos, CA. [Google Scholar]
- Hanlon C, Medhin G, Alem A, Araya M, Abdulahi A, Hughes M, & Prince M (2008). Detecting perinatal common mental disorders in Ethiopia: validation of the self-reporting questionnaire and Edinburgh Postnatal Depression Scale. Journal of Affective Disorders, 108(3), 251–262. [DOI] [PubMed] [Google Scholar]
- Holding P, Anum A, van de Vijver FJ, Vokhiwa M, Bugase N, Hossen T, … Gomes M (2016). Can we measure cognitive constructs consistently within and across cultures? Evidence from a test battery in Bangladesh, Ghana, and Tanzania. Appl Neuropsychol Child, 1–13. doi: 10.1080/21622965.2016.1206823 [DOI] [PubMed] [Google Scholar]
- Holding PA, Taylor HG, Kazungu SD, Mkala T, Gona J, Mwamuye B, … Stevenson J (2004). Assessing cognitive outcomes in a rural African population: development of a neuropsychological battery in Kilifi District, Kenya. J Int Neuropsychol Soc, 10(2), 246–260. [DOI] [PubMed] [Google Scholar]
- Holding P. a. A., A. (2005). Developing a Measure of the Consequences of Prenatal and Peri-Natal Insults in Early Childhood in Kenya: Preliminary Report of the Results for R21(TWOO6805–01/TWO3 007) FIC/NIH RFA, Brain Disorders in the Developing World: Research Across the Lifespan.
- Illingworth RS (1958). Dissociation as a guide to developmental assessment. Arch Dis Child, 33(168), 118–122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Illingworth RS, & Birch LB (1959). The Diagnosis of Mental Retardation in Infancy: A Follow-Up Study. Arch Dis Child, 34(175), 269–273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jennings L, Yebadokpo AS, Affo J, & Agbogbe M (2010). Antenatal counseling in maternal and newborn care: use of job aids to improve health worker performance and maternal understanding in Benin. BMC Pregnancy Childbirth, 10, 75. doi: 10.1186/1471-2393-10-75 [DOI] [PMC free article] [PubMed] [Google Scholar]
- John CC, Bangirana P, Byarugaba J, Opoka RO, Idro R, Jurek AM, … Boivin MJ (2008). Cerebral malaria in children is associated with long-term cognitive impairment. Pediatrics, 122(1), e92–99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kakyo TA, Muliira JK, Mbalinda SN, Kizza IB, & Muliira RS (2012). Factors associated with depressive symptoms among postpartum mothers in a rural district in Uganda. Midwifery, 28(3), 374–379. [DOI] [PubMed] [Google Scholar]
- Kammerer B, Isquith PJ, & Lundy S (2013). Approaches to assessment of very young children in Africa in the context of HIV. In Boivin & Giordani B (Eds.), Neuropsychology of Children in Africa: Perspectives on Risk and Resilience (pp. 17–36). New York: Springer Media & Business. [Google Scholar]
- Kashala-Abotnes E, Okitundu D, Mumba D, Boivin MJ, Tylleskar T, & Tshala-Katumbay D (2019). Konzo: a distinct neurological disease associated with food (cassava) cyanogenic poisoning. Brain Res Bull, 145, 87–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kashala-Abotnes E, Sombo MT, Okitundu DL, Kunyu M, Bumoko Makila-Mabe G, Tylleskar T, … Boivin MJ (2018). Dietary cyanogen exposure and early child neurodevelopment: An observational study from the Democratic Republic of Congo. PLoS One, 13(4), e0193261. doi: 10.1371/journal.pone.0193261 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kitsao-Wekulo P, Holding P, Taylor HG, Abubakar A, Kvalsvig J, & Connolly K Nutrition as an important mediator of the impact of background variables on outcome in middle childhood. Front Hum Neurosci, 7, 713. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koura KG, Boivin MJ, Davidson LL, Ouedraogo S, Zoumenou R, Alao MJ, … Bodeau-Livinec F (2013). Usefulness of child development assessments for low-resource settings in francophone Africa. J Dev Behav Pediatr, 34(7), 486–493. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mireku MO, Boivin MJ, Davidson LL, Ouedraogo S, Koura GK, Alao MJ, … Bodeau-Livinec F (2015). Impact of helminth infection during pregnancy on cognitive and motor functions of one-year-old children. PLoS Negl Trop Dis, 9(3), e0003463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mireku MO, Cot M, Massougbodji A, & Bodeau-Livinec F (2020). Relationship between Stunting, Wasting, Underweight and Geophagy and Cognitive Function of Children. J Trop Pediatr doi: 10.1093/tropej/fmaa009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mireku MO, Davidson LL, Boivin MJ, Zoumenou R, Massougbodji A, Cot M, & Bodeau-Livinec F (2016). Prenatal Iron Deficiency, Neonatal Ferritin, and Infant Cognitive Function. Pediatrics, 138(6). doi: 10.1542/peds.2016-1319 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mireku MO, Davidson LL, Koura GK, Ouedraogo S, Boivin MJ, Xiong X, … Bodeau-Livinec F (2015a). Prenatal Hemoglobin Levels and Early Cognitive and Motor Functions of One-Year-Old Children. Pediatrics, 136(1), e76–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mireku MO, Davidson LL, Koura GK, Ouedraogo S, Boivin MJ, Xiong X, … Bodeau-Livinec F (2015b). Prenatal Hemoglobin Levels and Early Cognitive and Motor Functions of One-Year-Old Children. Pediatrics doi: 10.1542/peds.2015-0491 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mireku MO, Davidson LL, Zoumenou R, Massougbodji A, Cot M, & Bodeau-Livinec F (2018). Consequences of prenatal geophagy for maternal prenatal health, risk of childhood geophagy and child psychomotor development. Trop Med Int Health, 23(8), 841–849. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mullen EM (1995). Mullen Scales of Early Learning:AGS Edition. Minneapolis, MN: American Guidance Services. [Google Scholar]
- Pollitt E (1999). Early iron deficiency anemia and later mental retardation. Am J Clin Nutr, 69(1), 4–5. [DOI] [PubMed] [Google Scholar]
- Pudas S, & Rönnlund M (2019). School performance and educational attainment as early-life predictors of age-related memory decline: protective influences in later-born cohorts. J Gerontol B Psychol Sci Soc Sci, 74(8), 1357–1365. [DOI] [PubMed] [Google Scholar]
- Ruel TD, Boivin MJ, Boal HE, Bangirana P, Charlebois E, Havlir DV, … Wong JK (2012). Neurocognitive and motor deficits in HIV-infected Ugandan children with high CD4 cell counts. Clin Infect Dis, 54(7), 1001–1009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Semrud-Clikeman M, Romero RA, Prado EL, Shapiro EG, Bangirana P, & John CC (2016). Selecting measures for the neurodevelopmental assessment of children in low- and middle-income countries. Child Neuropsychol, 1–42. [DOI] [PMC free article] [PubMed]
- Semrud-Clikeman M, Romero RAA, Prado EL, Shapiro EG, Bangirana P, & John CC (2017). Selecting measures for the neurodevelopmental assessment of children in low- and middle-income countries. Child Neuropsychol, 23(7), 761–802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sternberg RJ (2004). Culture and Intelligence. American Psychologist, 59(5), 325–338. [DOI] [PubMed] [Google Scholar]
- Suchdev PS, Boivin MJ, Forsyth BW, Georgieff MK, Guerrant RL, & Nelson CA 3rd. (2017). Assessment of Neurodevelopment, Nutrition, and Inflammation From Fetal Life to Adolescence in Low-Resource Settings. Pediatrics, 139(Suppl 1), S23–S37. [DOI] [PubMed] [Google Scholar]
- Sutcliffe AG, Soo A, & Barnes J (2010). Predictive value of developmental testing in the second year for cognitive development at five years of age. Pediatr Rep, 2(2), e15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Torras-Mana M, Gomez-Morales A, Gonzalez-Gimeno I, Fornieles-Deu A, & Brun-Gasca C (2016). Assessment of cognition and language in the early diagnosis of autism spectrum disorder: usefulness of the Bayley Scales of infant and toddler development, third edition. J Intellect Disabil Res, 60(5), 502–511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Wyhe KS, van de Water T, Boivin MJ, Cotton MF, & Thomas KG (2017). Cross-cultural assessment of HIV-associated cognitive impairment using the Kaufman assessment battery for children: a systematic review. J Int AIDS Soc, 20(1), 1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.