

Abstract
Cognitive reserve is characterized by a dissociation between cognitive level and brain structure, thereby reducing the impact of deteriorating brain structure on cognitive function. Cognitive reserve is therefore a promising approach to maintaining cognitive function and protecting against symptoms of dementia. The present paper evaluates evidence supporting the claim that bilingualism contributes to cognitive reserve. Four types of evidence are presented: (a) brain and cognitive function in healthy aging, (b) age of onset of symptoms of dementia, (c) relation between clinical level and neuropathology for patients, and (d) rate of cognitive decline in later stages of dementia. In all cases, bilinguals revealed patterns that were consistent with the interpretation of protection from cognitive reserve when compared to monolinguals.
Keywords: bilingualism, cognitive aging, dementia, cognitive reserve
Aging and Dementia in Society
Among the many reasons to be concerned about the increasing aging global population is the rising risk of cognitive decline and dementia. In addition to the obvious personal costs, dementia places substantial stress on public health systems. In 2020, the cost of treating dementia in the U.S., including nursing homes, medication, and physician care, was $305 billion [1]. At present, there are few effective pharmacological interventions and essentially no promising drugs in late-stage clinical trials [2], so postponing the onset of disease symptoms is the most effective defense. For example, a one year delay in symptom onset would reduce worldwide prevalence of Alzheimer’s disease (AD) in 2050 by approximately 9 million cases, and a delay of 2 years would decrease prevalence by 22 million [3]. The behavioral, social and environmental factors that potentially achieve this delay increase cognitive reserve [4, 5] and include physical exercise, formal education, and stimulating employment (Box 1). The urgency of addressing aging, cognitive decline, and dementia has focused new attention on the potential of cognitive reserve to provide relief. Bilingualism is a common experience, with some prevalence estimates including half the world’s population [6]. Recent studies suggest that bilingualism may be another factor that contributes to cognitive reserve. If so, a powerful tool for maintaining brain and cognitive health into older age may be hiding in plain sight.
Box 1: Cognitive Reserve.
The notion of cognitive reserve was created to capture the observation that there was a variable relation between brain health and cognitive outcomes across individuals [4]. Particularly puzzling was the finding that some older adults who had been considered cognitively healthy were discovered in postmortem examinations to have advanced AD pathology [68]. Current investigations of this phenomenon attempt to (a) consolidate the definition and criteria for the related aspects of reserve, including their measurement, (b) describe the factors and activities that contribute to reserve, and (c) identify the mechanisms responsible for the improved cognitive outcomes. Although much progress has been made, questions relating to all three aspects persist.
Two recent reviews, each written by a team of experts, have addressed the problem of definition [69, 70]. Agreeing on a common set of terms and definitions is clearly an essential prerequisite to progress in understanding how these complex systems work. Both teams reviewed theoretical and empirical material to arrive at consensual definitions, although the terms targeted in the two enterprises are not identical. Specifically, one group focused on “neurocognitive reserve”, “neurocognitive maintenance”, and “neurocognitive compensation”, in recognition of the interaction between cognitive and brain processes [69] and the other on “cognitive reserve”, “brain reserve”, and “brain maintenance”, addressing the cognitive and brain manifestations more discretely [70]. Nonetheless, substantial commonality was achieved that helps to clarify the inherently vague notion of “cognitive reserve”. Moreover, both groups recognized the need to include interactions between brain and behavior in any interpretation.
The sources of reserve come from genetic, environmental, and experiential factors, although these categories overlap and do not uniquely specify reserve factors. The main candidates are typically cited as education level, physical activity, social networks, occupational complexity, IQ (including genetic and environmental components), and inherited brain health.
The mechanism by which reserve allows cognitive levels to exceed the presumed limits of brain health is possibly the least understood aspect of reserve and may be different for specific reserve factors. In general, however, the source emanates from the adaptation of brain and cognitive systems through such processes as selection and reorganization to make cognitive activities more automatic and less effortful and therefore more tractable even in the presence of underlying brain physiology.
Cognitive reserve is an essential construct in understanding the inter-individual differences in the trajectories of cognitive aging and the enticing finding that neuropathology does not inevitably lead to cognitive impairment.
The critical feature of experiences that contribute to cognitive reserve is that they are stimulating or effortful. Why would bilingualism belong to this group? A surprising finding from psycholinguistics research is that the bilingual mind is constantly engaged in resolving competition between jointly activated languages; there is no language switch [7]. One would expect, therefore, that bilinguals would make frequent selection errors in which the incorrect language intruded into speech, but this rarely happens [8]. The usual explanation for how bilinguals avoid such intrusions is that bilingual language processing recruits domain-general attentional processes to focus on the target language and avoid interference from the other [9]. This explanation is supported by the overlap of processes involved in bilingual language selection and nonverbal selection more broadly [10]. These domain- general attention processes, which are part of the frontal executive function system, decline with healthy aging. Not surprisingly, therefore, the frequency of bilingual language intrusions increases with aging [11] and dementia [12]. Thus, bilingual experience stimulates crucial attentional processes, fortifying them for other purposes, and potentially creating a foundation for cognitive reserve.
Consequences of Cognitive Reserve for Bilinguals
The signature manifestation of cognitive reserve is a dissociation between brain level and cognitive level, as shown in Figure 1. In typical aging, cognitive level and brain structure decline in parallel (Figure 1a), but with cognitive reserve, cognitive level remains high despite deteriorating brain structure (Figure 1b). Therefore, individuals with high reserve achieve higher cognitive levels than would be expected from brain structure. A related concept, neural reserve, may provide one of the mechanisms for this protection but a full discussion is beyond the scope of the present review [13].
Figure 1. Typical aging versus cognitive reserve.
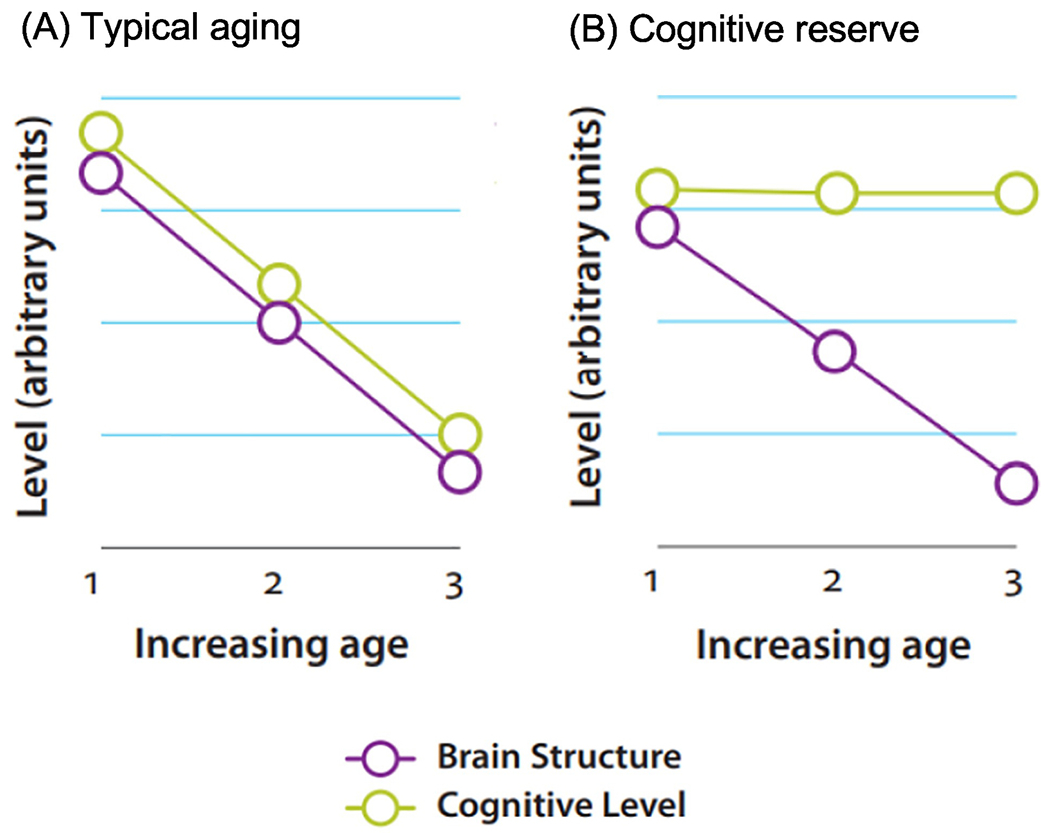
Hypothetical relation between brain structure and cognitive level in typical aging (a.) and with cognitive reserve (b.). The x-axis shows increasing age and the y-axis shows an arbitrary scale for measuring cognitive level and brain structure, with high values indicating better outcomes for each. In cognitive reserve, cognitive level is maintained despite decline in brain structure. Figure adapted from [71].
Stern [14] created a useful illustration showing the relation between cognitive and brain level with cognitive reserve, presented in Figure 2 (Key Figure). Changes in neuropathology (x-axis) are plotted against cognitive level (y-axis) for individuals with high versus low reserve. For both groups, as neuropathology accumulates there is eventually a tipping point beyond which there is rapid cognitive decline, but this point is deferred and occurs at a greater level of pathology for high reserve individuals than for those with low reserve. Therefore, the accumulation of neuropathology affects high and low reserve individuals on a different timetable.
Figure 2 (Key Figure). Relation between neuropathology and cognitive level with cognitive reserve.
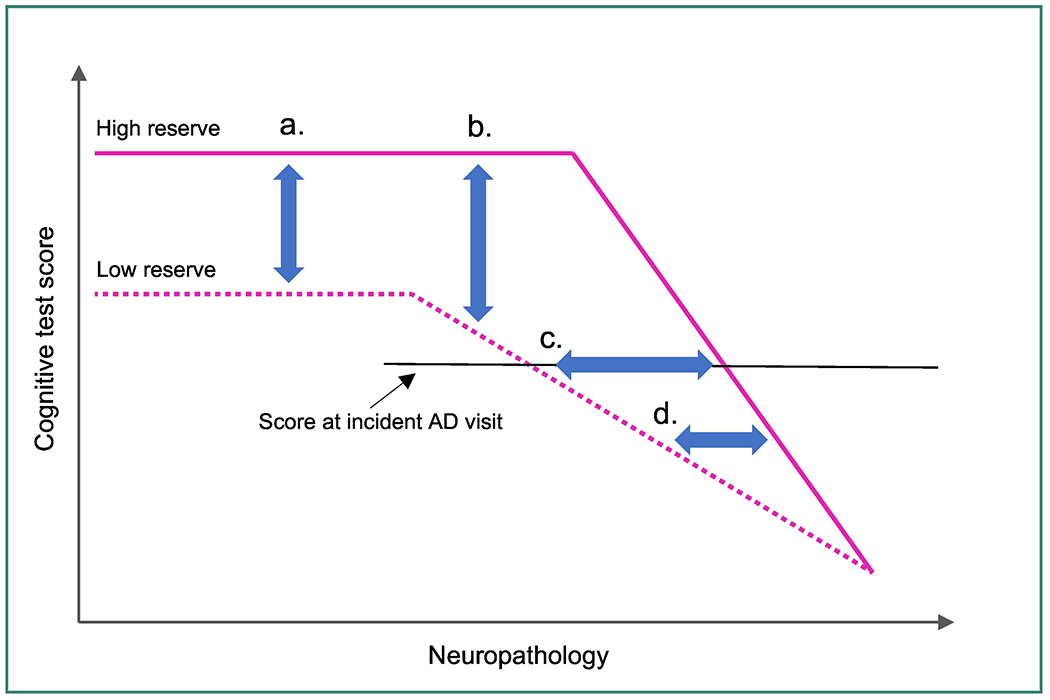
Hypothesized change in cognitive function over time in individuals with high and low cognitive reserve, adapted from [14]. Four predictions for cognitive reserve in bilinguals are indicated: a. Better cognitive level and/or brain structure in older age for bilinguals than monolinguals. b. Earlier diagnosis of dementia for monolinguals than bilinguals. c. More pathology for similar cognitive dementia level for bilinguals than monolinguals. d. More rapid cognitive decline following diagnosis for bilinguals than monolinguals.
The claim that bilingual experience leads to cognitive reserve can be illustrated by considering that the high- and low- reserve lines on Figure 2 represent “bilinguals” and “monolinguals”, respectively. Figure 2 then leads to four predictions regarding outcomes for the two language groups. The first is that for healthy adults, bilinguals will outperform monolinguals on cognitive tasks and possibly have better brain structure (point a); the second is that the cognitive decline associated with dementia will become apparent earlier in monolingual older adults than in bilinguals (point b); the third is that when there is a diagnosis of dementia, bilinguals will have more advanced neuropathology than monolinguals for similar clinical dementia levels (point c); and finally, cognitive decline following the dementia diagnosis will be more rapid for bilinguals than for monolinguals (point d). The predictions at points (a) and (b) entail holding brain level constant and observing the effect on cognition; the predictions at points (c) and (d) entail holding cognitive level constant and observing the corresponding levels of brain structure.
Cognitive and Brain Levels in Health Aging
The research comparing cognitive abilities of monolingual and bilingual healthy adults has become highly contentious [15]. Following an early study showing that bilingual middle-aged and older adults performed the Simon task (a standard executive function task) better than their monolingual counterparts [16], many subsequent studies, primarily with young adults, failed to detect behavioral differences between language groups, leading several researchers to argue that the conclusion was unwarranted [17–19]. Despite this conclusion, evidence continued to accumulate supporting the observation that bilinguals outperformed monolinguals on these tasks, a situation represented by point (a) on Figure 2.
Meta-analyses conducted to resolve the conflicting results have led to conclusions deciding both in favor of positive effects of bilingualism [20–23] and no reliable group difference [24, 25]. Part of the reason for the lack of resolution is that the studies include a heterogenous collection of tasks, linguistic contexts, populations, and inclusion criteria, so combining them in overall analyses potentially obscures the unique features that may be associated with better bilingual performance [26, 27]. The typical effect size in these meta-analyses is about 0.15 to 0.20, a figure that is sometimes rejected as too small to be meaningful (despite being significant) or dismissed after correction for “publication bias” as being unreliable. However, this effect size is similar to that found for the effect of physical exercise on cognitive outcomes, typically between 0.10 and 0.25 [28, 29], an effect that is not considered controversial.
There are also conflicting results when comparing the brain structure of monolingual and bilingual healthy older adults. For example, studies have reported greater grey matter volume in bilinguals than monolinguals [30, 31], no differences between language groups [32, 33], and poorer volume in bilinguals than monolinguals [34]. In all the studies, participants performed similarly on cognitive tasks but showed different outcomes for brain structure. How is that possible?
One possibility pertains to the different ages of the participants. In the studies demonstrating better brain structure by bilinguals than monolinguals, participants were around 60 years old, essentially on the cusp of being “older adults”. In the studies indicating comparable grey matter volume for the language groups, participants were somewhat older, with a mean age of 65 to 70 years, yet in one of those studies [31], the bilinguals had poorer white matter microstructure than monolinguals, suggesting some structural decline in the bilingual brains. Finally, in a study showing poorer grey matter structure for bilinguals, the participants were around 75 years old, and in this case, the bilinguals also had poorer white matter structure than the monolinguals [35]. This interpretation is supported by evidence showing that for young adult bilinguals generally have greater grey matter volume than their monolingual counterparts [36–40]. The pattern, therefore, is that with increasing age, monolingual and bilingual older adults maintain parity on cognitive measures but there is an ongoing deterioration of brain structure for bilinguals, as shown in Figure lb. But why would bilinguals show more brain deterioration than monolinguals in older age? Do bilingual brains simply decline more precipitously than monolingual brains?
To understand this dilemma, it is necessary to consider the cognitive data which, in all cases, remains similar for monolingual and bilingual older adults regardless of brain structure. Put another way, there is a dissociation between brain level and cognitive level for the bilinguals, the signature pattern for cognitive reserve. All participants in these studies were experiencing healthy cognitive aging, with no neurological complaints or memory problems, ensuring consistent and high cognitive level for both groups. However, the brain structure results suggest that despite comparable cognitive levels, the bilinguals had more compromised brain structure. Therefore, sampling procedures that target cognitively healthy individuals may include participants for whom there is neurological decline as long as there is no impact on cognition. But why would such individuals only belong to the bilingual group?
It may be that monolingual older adults with brain structure comparable to the bilinguals would be ineligible for the studies because of the parallel decline in cognitive level, as in Figure la. To investigate that possibility, we used values for white matter structure to match the bilingual participants from a previous study [33] to monolinguals from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) database (adni.loni.usc.edu) [41]. This unusual approach hypothetically asks what would happen if a bilingual brain were put into a monolingual mind. Thus, a group of 32 monolinguals from the database were selected on the basis of matching the bilingual sample for white matter values, age, education, and other background factors, to compare the cognitive status in the two language groups. These data are presented in Table 1. All the bilinguals were experiencing healthy aging, a precondition for having participated in the original study and confirmed by performance on the cognitive tasks administered in that study. In the matched monolingual group, in contrast, 13 of the participants (41%) had received clinical diagnoses of cognitive impairment. These results are consistent with the interpretation that the functional activity involved in bilingual language use is associated with better cognitive function than predicted by the level of brain structure.
Table 1.
Cognitive status of matched groups from Berkes et al. [41].
| Group | N | Age in years | Education in years | MMSE | Fractional Anisotropy | Axial Diffusivity | Radial Diffusivity | PCA scores | Cognitive Profile1 |
|---|---|---|---|---|---|---|---|---|---|
| Bilinguals | 32 | 73.5 | 16.1 | 29.4 | 0.42 | 1.2 x 10−3 | 6.6 x 10−4 | 1.79 (1.1) | CN = 32 (100%) |
| (72% F) | (3.8) | (2.8) | (0.7) | (0.02) | (0.02 x 10−3) | (0.5 x 10−4) | |||
| Monolinguals | 32 | 73.1 | 16.3 | 26.7 | 0.45 | 1.2 x 10−3 | 6.1 x 10−4 | 1.32 (1.2) | CN = 19 (59%) |
| (69% F) | (6.5) | (2.5) | (4.4) | (0.02) | (0.04 x 10−3) | (0.4 x 10−4) | MCI = 8 (25%) | ||
| AD = 5 (16%) |
CN = Clinically normal; MCI = Mild cognitive impairment; AD = Alzheimer’s disease
To summarize, behavioral evidence from healthy older adults provides mixed evidence for cognitive reserve from bilingualism, but evidence from underlying brain structure is more consistent. In some behavioral studies, healthy bilingual older outperform monolinguals on cognitive tasks, but in other studies, performance is equivalent. However, studies using several different approaches demonstrate the central dissociation of cognitive reserve, namely, high cognitive level with declining brain structure.
Clinical Impairment and the Diagnosis of Dementia
As neuropathology accumulates, a deflection point is reached that signals a measurable decline of cognitive function, as shown by point (b) in Figure 2. The deflection point shifts right for high reserve individuals because more neuropathology can be tolerated before these changes become apparent. Therefore, clinical evidence of cognitive decline should be seen at an earlier stage of disease for low reserve than high reserve individuals, and on average low reserve individuals will be younger than their high reserve counterparts when clinical impairment is noticed or diagnosed. For high reserve individuals, early stages of the disease can progress without symptoms. Put another way, the same degree of accumulated neuropathology will be symptomatic in low reserve individuals but asymptomatic in high reserve individuals. Therefore, if bilingualism leads to high reserve, then bilinguals will be older than monolinguals when clinical dementia is diagnosed, all else being equal.
In the first study to investigate this possibility, we examined consecutive records of patients in a memory clinic and classified individuals as monolingual or bilingual on the basis of physician notes from the initial interview, excluding patients for whom the language history was unclear [42]. The final sample consisted of 184 patients (91 monolinguals, 93 bilinguals) matched on relevant background variables. The results showed that bilingual patients were on average 4.1 years older than monolinguals when clinical symptoms of dementia first became apparent. This finding has been subsequently replicated in many countries, with the largest replication being conducted in India with ~650 patients [43]. The Indian study is notable because it was a non-immigrant sample that included a wide range of socioeconomic status and education, all factors that have previously been proposed as confounds with bilingualism. Similar delays have been reported for the onset of symptoms of mild cognitive impairment [44, 45]. Some studies report a role for mediating variables such as education [46] or features of the language and social background [47], but a meta-analysis of these studies investigating age of onset for Alzheimer’s disease or mild cognitive impairment confirmed a significant delay in onset for bilingual patients, with a moderate effect size, d=0.32 [48].
In contrast to retrospective studies that evaluate profiles of patients diagnosed with the disease, prospective studies investigate differential vulnerability to disease before it occurs. Typically, a cohort of healthy older adults is followed over several years, sometimes for decades, and the dependent variable is the rate of disease incidence in specified groups. Therefore, the question is not whether one group acquires the disease on a different timetable but rather if one group is more immune to the disease in that it has lower incidence. Although there is no reason that bilingualism should prevent Alzheimer’s disease, the postponement of symptoms could lower the incidence because it is a disease of aging so individuals may die before symptoms are revealed; presumably these patients die from other causes. Prospective studies show more mixed results than retrospective studies, with some reporting a significantly lower incidence for bilinguals [49] and others showing no significant difference [50]. These results do not contradict those from the retrospective studies because prospective studies rarely report the age of diagnosis of AD, only the proportion of the cohort that has been affected. Nevertheless, despite different outcomes from these studies, the meta-analysis described above [48] also found that the lower incidence for bilinguals with AD was significant, but with a smaller effect size, d = 0.10.
One problem with the prospective studies is that the final sample depends on individuals developing the disease, and that number can be small. For example, in a prospective study conducted in Sweden, [51], a healthy cohort was followed for 10 years, and at the end of that time 112 participants had developed dementia. However, the initial cohort consisted mostly of monolinguals, so those who contracted AD by the end of the study included 102 monolinguals (about 14% of the cohort) and 10 bilinguals (about 12% of the cohort), a difference that was not significant. But with only 10 bilinguals, the statistical analysis is inconclusive; larger samples are required. A creative approach to this problem is to use entire countries as the cohort from which to observe incidence of AD. In one such study, researchers [52] compared the incidence of AD in 93 countries that were classified in terms of the mean number of languages spoken by the population, controlling for wealth, life expectancy, and the like. There was a significant negative relation between the mean number of languages spoken and the incidence of AD; countries with more bilingual populations had a lower incidence of Alzheimer’s disease, all else being equal.
In summary, in both retrospective and prospective studies, bilingualism offered some protection against symptoms of dementia, even if it did not prevent the disease from occurring. Bilingualism has also been cited as a protective factor in other neurological disorders, including cognitive recovery following stroke [53, 54], intensity of aphasia following similar levels of stroke [55, 56], and degree of symptoms of Multiple Sclerosis, Parkinson’s and Huntington’s Disease [57]. Moreover, bilingual AD patients with clinical dementia outperformed comparable monolingual patients on tests of memory and attention [58]. Together these results are consistent with a persistent benefit from bilingualism in the context of neurodegenerative disease.
Cognitive-Brain Relations in Dementia
Instead of examining changes in cognitive level for given values of neuropathology as was the case for points (a) and (b) in Figure 2, one can hold cognitive level constant and examine the consequences on neuropathology, as indicated by point (c) in Figure 2. Here the prediction is that bilinguals will have more neuropathology than monolinguals for similar cognitive levels. The first study to take this approach compared 20 monolingual and 20 bilingual AD patients who were matched on chronological age, clinical dementia levels, and other factors such as education and occupational status [59]. Measurement of brain atrophy was taken from computerized tomography scans that evaluated overall brain atrophy associated with healthy aging. These measures were equivalent for patients in both language groups. However, atrophy in medial-temporal and hippocampal regions is a marker for AD pathology. For all these markers, including temporal horn ratio, third ventricle ratio, and radial width of the temporal horn, there was significantly more atrophy in the bilingual patients than in the monolinguals (all ps < .001). Thus, patients in both language groups presented with similar clinical levels, but bilingual patients had significantly more disease pathology than the monolinguals.
Another approach is to compare levels of metabolic glucose uptake in AD patients. As with medial- temporal atrophy, reduced glucose metabolism is a marker of AD progression. In two studies using this technique, bilingual patients with mild cognitive impairment [60] or AD [61] who were matched with monolingual patients for background measures and clinical impairment level showed poorer metabolic glucose uptake, indicating more advanced disease.
Declining Cognition in Dementia
Regardless of the level of underlying pathology before clinical dementia is manifest, once that landmark has been passed the decline in cognitive function is rapid and inevitable, creating a difficult period for patients and their families. Given that bilingual AD patients are on average older than monolinguals when the disease is detected, and likely have higher levels of neuropathology for similar clinical levels, is there also a difference in the rate of decline following diagnosis? The counterintuitive prediction from cognitive reserve is that the decline will be more rapid for high reserve patients than for their low reserve counterparts. It is as though the built-up resilience can support cognitive function for a period of time but eventually the pathology overwhelms the system and the decline is precipitous. This effect is indicated by the different slopes of the lines at point (d) on Figure 2.
Some early attempts to investigate differences in rate of decline for patients with clinical dementia did not reveal reliable group differences. In two studies in which we examined age of onset of dementia, some patients had multiple Mini Mental Status Exam (MMSE) scores over time recorded in their files, so those data were examined to compare the rate of decline for monolingual and bilingual patients. Neither study indicated any difference between language groups [42, 62], but the data were fragmentary and inconclusive and MMSE is a weak indicator of cognitive level.
A different way of approaching this question is to follow patients who have been diagnosed with mild cognitive impairment longitudinally as the disease progresses. These patients convert to AD at the rate of about 10% to 15% annually [63], so if the diagnosis of mild cognitive impairment comes at a later stage of neuropathology for high reserve than low reserve patients, then the prediction is that the conversion to AD will be more rapid. Unlike a simple evaluation of MMSE scores, the diagnostic decisions that the patient has converted to AD is made by a team of experts evaluating a broad range of data from each patient, conferring reliability and validity onto these judgments. To investigate the possibility that conversion times differ as a function of cognitive reserve, we followed 158 patients (83 monolinguals, 75 bilinguals) who had been diagnosed with mild cognitive impairment until the point that the consensus diagnosis converted to AD [64]. The average conversion times were 2.6 years for monolinguals and 1.9 years for bilinguals, a difference that was significant. Therefore, the ability of cognitive reserve to sustain cognitive level as brain structure declines eventually fails. However, such a negative conclusion takes no account of the time granted to high reserve individuals to function at cognitive levels that exceed the predictions that would be made from the accumulating levels of neuropathology.
Concluding Remarks and Future Directions
The problems associated with aging and dementia affect both individuals and societies by imposing enormous burdens on social, emotional, and financial resources. Any intervention that has the potential to preserve cognitive health with aging, particularly if it can postpone symptoms of dementia, must be carefully evaluated for its efficacy. In the current absence of effective pharmacological therapies, the most promising approach to maintaining cognitive function is through engagement in the activities that contribute to cognitive reserve. The evidence reviewed here supports the conclusion that bilingualism is one such experience.
The activities that are effective in building cognitive reserve may be considered in terms of “passive” and “active” sources. This distinction has been applied to the difference between passive brain reserve and active cognitive reserve [4] but it also captures a distinction within cognitive reserve. Passive activities include details of the individual’s history that accumulated reserve without special attention to that goal, such as formal education; educational decisions were unlikely to have been made with cognitive reserve in mind. Active forms of reserve reflect deliberate choices to engage in various activities for a variety of reasons, one of which may be to build reserve, such as participation in social activities and aerobic exercise. Bilingualism is different from both. Like the passive factors, most bilinguals did not choose to become bilingual but did so because of details of their history, such as immigration or travel. However, like the active factors, at some point using multiple languages can become a choice, as is the decision to pass heritage languages on to the next generation. In that sense, it is a passive factor over which the individual can have active control. This situation is not unique to bilingualism: older adults increasingly engage in formal courses and other educational opportunities for a variety of reasons, and building cognitive reserve is possibly one. However, the complexity and diversity of bilingual experience nonetheless sets this apart from other factors. Just as details of bilingual experience mediate the degree to which cognitive consequences of bilingualism are found [65], so too the details of bilingual experience are likely to impact the extent to which cognitive reserve accumulates [66]. The precise aspects of bilingual experience that influence these outcomes are not yet fully understood, as described in Outstanding Questions, and may combine with other cognitive reserve activities in ways that are not yet known.
There is a final point about the value of bilingualism that is rarely discussed. Despite the ongoing controversy about whether bilingual participants outperform monolinguals on laboratory tasks assessing executive functioning, it remains uncontroversial that bilinguals can communicate in more than one language, an outcome that is not trivial! There is also evidence that bilingualism enhances vocational opportunities that lead to financial advantages [67]. But most important is that bilingualism is the glue that connects people to each other — individuals to strangers across global boundaries and children to their families and ancestors from far away countries. Both types of connection lead to a more integrated world and the possibility for better mutual understanding. Add to that the possibility that bilingualism may also contribute to cognitive reserve and the implications for policy are clear: education systems at all levels should offer and promote foreign language training, community organizations should support and maintain the use of immigrant languages by offering goods and services in those languages, and government policy should acknowledge linguistic diversity and encourage societal multilingualism. There is much to be gained for everyone.
Outstanding Questions Box.
What details of bilingual experience are responsible for the observed effects? Bilingualism is now considered to be a continuum of experiences rather than a categorical event. Research with young adults has identified the importance of factors such as age of acquisition, length of time being bilingual, patterns of language use and switching, intensity of use of each language, and language context, but how these factors influence the accumulation of cognitive reserve in older bilinguals is not known.
Can bilingual training in older age be used as an intervention to maintain cognitive function? There is some evidence that late bilingualism offers some cognitive benefit but does the process of learning a second language later in life also contribute to cognitive reserve?
How does a language experience (left parietal lobe) that enhances executive functioning (frontal lobes) protects memory decline (medial-temporal lobes) in dementia? The original evidence showing later symptom onset of dementia in bilingualism has now been replicated many times, but there is still no adequate explanation for how this protection works. Uncovering the mechanism will have implications for harnessing these processes to boost cognitive reserve broadly.
What is the relation between “cognitive reserve,” in which cognition is protected despite failing brain structure, and “neural reserve,” in which brain structures become more robust and resilient through experience? The two concepts are related, but the nature of that relation will determine how existing data should be interpreted and how future implementations of interventions for cognitive reserve should proceed. Therefore, uncovering the relation between these aspects of reserve is a priority for future research.
Highlights Box.
Cognitive reserve is the most promising avenue to maintaining cognitive health in older age and averting some of the more devastating consequences of cognitive decline and dementia.
Cognitive reserve is characterized by a dissociation between cognitive level and brain structure in that deterioration of brain structure may not impact cognitive function.
Bilingualism appears to contribute to Cognitive reserve in that it is associated with (a) better cognitive performance than would be predicted by brain structure in older adults, (b) later evidence of symptoms of dementia compared to monolinguals, (c) greater pathology for comparable levels of dementia as found for monolinguals, and (d) more rapid decline of cognitive function in more advanced stages of dementia.
More support should be given to societal attitudes to foreign language learning and bilingualism.
Acknowledgments
Acknowledgements
The research described in this paper was supported by grant R21AG048431 from the NIH National Institute on Aging and grant A2559 from the Natural Sciences and Engineering Research Council, Canada.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Alzheimer’s Association, 2020 Alzheimer’s disease facts and figures. Alzheimers & Dementia, 2020. 16; p. 391–460. [Google Scholar]
- 2.Cummings J, et al. , Alzheimer’s disease drug development pipeline: 2017. Alzheimer’s & Dementia: Translational Research & Clinical Interventions, 2017. 3(3): p. 367–384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Brookmeyer R, et al. , National estimates of the prevalence of Alzheimer’s disease in the United States. Alzheimers & Dementia, 2011. 7(1): p. 61–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Stern Y, What is cognitive reserve? Theory and research application of the reserve concept. Journal of the International Neuropsychological Society, 2002. 8: p. 448–460. [PubMed] [Google Scholar]
- 5.Barulli D and Stern Y, Efficiency, capacity, compensation, maintenance, plasticity: emerging concepts in cognitive reserve. Trends in Cognitive Sciences, 2013. 17(10): p. 502–509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wei L, Dimensions of bilingualism, in The bilingualism reader, Wei L, Editor. 2000, Routledge: London. p. 3–25. [Google Scholar]
- 7.Kroll JF, Bobb SC, and Hoshino N, Two languages in mind: Bilingualism as a tool to investigate language, cognition, and the brain. Current Directions in Psychological Science, 2014. 23: p. 159–163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gollan TH and Goldrick M, A switch is not a switch: Syntactically-driven bilingual language control. Journal of Experimental Psychology: Learning Memory and Cognition, 2018. 44(1): p. 143–156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bialystok E, The bilingual adaptation: How minds accommodate experience. Psychological Bulletin, 2017. 143(3): p. 233–262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Luk G, et al. , Cognitive control for language switching in bilinguals: A quantitative meta analysis of functional neuroimaging studies. Language and Cognitive Processes, 2012. 27: p. 1479–1488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Gollan TH, Sandoval T, and Salmon DP, Cross-language intrusion errors in aging bilinguals reveal the link between executive control and language selection. Psychological Science 2011. 22(9): p. 1155–1164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gollan TH, et al. , Bilingual language intrusions and other speech errors in Alzheimer’s disease. Brain & Cognition, 2017. 118: p. 27–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Perani D and Abutalebi J, Bilingualism, dementia, cognitive and neural reserve. Current Opinion in Neurology, 2015. 28: p. 618–625. [DOI] [PubMed] [Google Scholar]
- 14.Stern Y, Cognitive reserve in ageing and Alzheimer’s disease. The Lancet Neurology, 2012. 11(11): p. 1006–1012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Antoniou M, The advantages of bilingualism debate. Annual Review of Linguistics, 2019. 5: p. 1–21. [Google Scholar]
- 16.Bialystok E, et al. , Bilingualism, aging, and cognitive control: Evidence from the Simon task. Psychology and Aging, 2004. 19(2): p. 290–303. [DOI] [PubMed] [Google Scholar]
- 17.Paap KR and Greenberg ZI, There is no coherent evidence for a bilingual advantage in executive processing. Cognitive Psychology, 2013. 66(2): p. 232–58. [DOI] [PubMed] [Google Scholar]
- 18.Anton E, Carreiras M, and Dunabeitia JA, The impact of bilingualism on executive functions and working memory in young adults. PLoS One, 2019.14(2): p. e0206770. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.von Bastian CC, Souza AS, and Gade M, No evidence for bilingual cognitive advantages: A test of four hypotheses. Journal of Experimental Psychology: General, 2016.145: p. 246–258. [DOI] [PubMed] [Google Scholar]
- 20.Armstrong BA, et al. , The effect of bilingualism on older adults’ Inhibitory Control: A meta-analysis. Gerontologist, 2019. 10.1093/geront/gnz086 [DOI] [PubMed] [Google Scholar]
- 21.Grundy JG, The effects of bilingualism on executive functions: an updated quantitative analysis. Journal of Cultural Cognitive Science, 2020. 10.1007/S41809-020-00062-5 [DOI] [Google Scholar]
- 22.Ware AT, Kirkovski M, and Lum JAG, Meta-analysis reveals a bilingual advantage that is dependent on task and age. Frontiers in Psychology, 2020.11: p. 1458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.van den Noort M, et al. , Does the bilingual advantage in cognitive control exist and if so, what are its modulating factors? A systematic review. Behavioral Sciences, 2019. 9(3). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Donnelly S, Brooks PJ, and Homer BD, Is there a bilingual advantage on interference-control tasks? A multiverse meta-analysis of global reaction time and interference cost. Psychonomic Bulletin and Review, 2019. 26: p. 1122–1147. [DOI] [PubMed] [Google Scholar]
- 25.Lehtonen M, et al. , Is bilingualism associated with enhanced executive functioning in adults? A meta-analytic review. Psychological Bulletin, 2018.144: p. 394–425. [DOI] [PubMed] [Google Scholar]
- 26.de Bruin A, Not all bilinguals are the same: A call for more detailed assessments and descriptions of bilingual experiences. Behavioral Sciences, 2019. 9(3) p.33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Surrain S and Luk G, Describing bilinguals: A systematic review of labels and descriptions used in the literature between 2005–2015. Bilingualism: Language and Cognition, 2019. 22: p. 401–415. [Google Scholar]
- 28.Chang YK, et al. , The effects of acute exercise on cognitive performance: a meta-analysis. Brain Research 2012.1453: p. 87–101. [DOI] [PubMed] [Google Scholar]
- 29.Etnier JL, et al. , The influence of physical fitness and exercise upon cognitive functioning: A meta-analysis. Journal of Sport and Exercise Psychology, 1997. 19: p. 249–277. [Google Scholar]
- 30.Abutalebi J, et al. , Bilingualism protects anterior temporal lobe integrity in aging. Neurobiology of Aging, 2014. 35(9): p. 2126–33. [DOI] [PubMed] [Google Scholar]
- 31.Abutalebi J, et al. , The neuroprotective effects of bilingualism upon the inferior parietal lobule: A structural neuroimaging study in aging Chinese bilinguals. Journal of Neurolinguistics, 2015.33: p. 3–13· [Google Scholar]
- 32.Olsen RK, et al. , The effect of lifelong bilingualism on regional grey and white matter volume. Brain Research, 2015.1612: p. 128–39. [DOI] [PubMed] [Google Scholar]
- 33.Gold BT, Johnson NF, and Powell DK, Lifelong bilingualism contributes to cognitive reserve against white matter integrity declines in aging. Neuropsychologia, 2013. 51(13): p. 2841–2846. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Anderson JAE, Grundy JG, and Bialystok E, Lifelong bilingualism leads to cognitive reserve in older adults, in Annual Meeting of the Psychonomic Society. 2019: Montreal, Canada. [Google Scholar]
- 35.Anderson JAE, et al. , Effects of bilingualism on white matter integrity in older adults. Neuroimage 2018.167: p. 143–150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Heim S, et al. , Bilingualism and “Brain Reserve”: A matter of age. Neurobiology of Aging, 2019. 81: p. 157–165. [DOI] [PubMed] [Google Scholar]
- 37.Del Maschio N, et al. , Neuroplasticity across the lifespan and aging effects in bilinguals and monolinguals. Brain and Cognition, 2018.125: p. 118–126. [DOI] [PubMed] [Google Scholar]
- 38.Li P, Legault J, and Litcofsky KA, Neuroplasticity as a function of second language learning: Anatomical changes in the human brain. Cortex, 2014. 58C: p. 301–324. [DOI] [PubMed] [Google Scholar]
- 39.Olulade OA, et al. , Neuroanatomical evidence in support of the bilingual advantage theory. Cerebral Cortex, 2016. 26: p. 3196–3204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Pliatsikas C, et al. , The effect of bilingualism on brain development from early childhood to young adulthood. Brain Structure and Function, 2020. 225(7): p. 2131–2152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Berkes M, et al. , Poorer clinical outcomes for older adult monolinguals when matched to bilinguals on brain health. Brain Structure and Function, 2021, DOI 10.1007/S00429-020-02185-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Bialystok E, Craik FIM, and Freedman M, Bilingualism as a protection against the onset of symptoms of dementia. Neuropsychologia, 2007. 45(2): p. 459–464. [DOI] [PubMed] [Google Scholar]
- 43.Alladi S, et al. , Bilingualism delays age at onset of dementia, independent of education and immigration status. Neurology, 2013. 81: p. 1938–1944. [DOI] [PubMed] [Google Scholar]
- 44.Calabria M, et al. , Active bilingualism delays the onset of mild cognitive impairment. Neuropsychologia, 2020: p. 107528. [DOI] [PubMed] [Google Scholar]
- 45.Ramakrishnan S, et al. , Comparative effects of education and bilingualism on the onset of Mild Cognitive Impairment. Dementia and Geriatric Cognitive Disorders, 2017. 44(3-4): p. 222–231. [DOI] [PubMed] [Google Scholar]
- 46.Gollan TH, et al. , Degree of bilingualism predicts age of diagnosis of Alzheimer’s disease in low-education but not in highly educated Hispanics. Neuropsychologia, 2011. 49(14): p. 3826– 30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Chertkow H, et al. , Multilingualism (But Not Always Bilingualism) Delays the Onset of Alzheimer Disease: Evidence From a Bilingual Community. Alzheimer Disease and Associated Disorders, 2010. 24(2): p. 118–125. [DOI] [PubMed] [Google Scholar]
- 48.Anderson JAE, Hawrylewicz K, and Grundy JG, Does bilingualism protect against dementia? A meta-analysis. Psychonomic Bulletin & Review, 2020. 27(5): p. 952–965. [DOI] [PubMed] [Google Scholar]
- 49.Wilson RS, et al. , Early life instruction in foreign language and music and incidence of mild cognitive impairment. Neuropsychology, 2015. 29: p. 292–302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Zahodne LB, et al. , Bilingualism does not alter cognitive decline or dementia risk among Spanish-speaking immigrants. Neuropsychology, 2014. 28(2): p. 238–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Ljungberg JK, et al. , The effect of language skills on dementia in a Swedish longitudinal cohort. Linguistic Approaches to Bilingualism, 2016. 6: p. 190–204. [Google Scholar]
- 52.Klein RM, Christie J, and Parkvall M, Does multilingualism affect the incidence of Alzheimer’s disease?: A worldwide analysis by country. SSM - Population Health, 2016. 2: p. 463–467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Lahiri D, et al. , Effect of bilingualism on aphasia recovery. Aphasiology, 2020: p. 1–22. [Google Scholar]
- 54.Alladi S, et al. , Impact of bilingualism on cognitive outcome after stroke. Stroke, 2016. 47: p. 258–261. [DOI] [PubMed] [Google Scholar]
- 55.Paplikar A, et al. , Bilingualism and the severity of poststroke aphasia. Aphasiology, 2019. 33(1): p. 58–72. [Google Scholar]
- 56.Dekhtyar M, Kiran S, and Gray T, Is bilingualism protective for adults with aphasia? Neuropsychologia, 2020.139: p. 107355. [DOI] [PubMed] [Google Scholar]
- 57.Voits T, et al. , Beyond Alzheimer’s disease: Can bilingualism be a more generalized protective factor in neurodegeneration? Neuropsychologia, 2020.147: p. 107593. [DOI] [PubMed] [Google Scholar]
- 58.Weissberger GH, et al. , Neuropsychological deficit profiles, vascular risk factors, and neuropathological findings in Hispanic older adults with autopsy-confirmed Alzheimer’s Disease. Journal of Alzheimers Disease, 2019. 67(1): p. 291–302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Schweizer TA, et al. , Bilingualism as a contributor to cognitive reserve: Evidence from brain atrophy in Alzheimer’s disease. Cortex, 2012. 48(8): p. 991–996. [DOI] [PubMed] [Google Scholar]
- 60.Kowoll ME, et al. , Bilingualism as a contributor to cognitive reserve? Evidence from cerebral glucose metabolism in Mild Cognitive Impairment and Alzheimer’s Disease. Frontiers in Psychiatry, 2016. 7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Perani D, et al. , The impact of bilingualism on brain reserve and metabolic connectivity in Alzheimer’s dementia. Proceedings of the National Academy of Sciences, 2017: p. 201610909. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Bialystok E, et al. , Effects of bilingualism on the age of onset and progression of MCI and AD: evidence from executive function tests. Neuropsychology, 2014. 28(2): p. 290–304. [DOI] [PubMed] [Google Scholar]
- 63.Petersen RC, et al. , Current concepts in Mild Cognitive Impairment. Archives of Neurology, 2001. 58: p. 1985–1992. [DOI] [PubMed] [Google Scholar]
- 64.Berkes M, et al. , Conversion of Mild Cognitive Impairment to Alzheimer Disease in Monolingual and Bilingual Patients. Alzheimer’s Disease and Associated Disorders, 2020. 34: p.225–230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.DeLuca V, et al. , Redefining bilingualism as a spectrum of experiences that differentially affects brain structure and function. Proceedings of the National Academy of Sciences, 2019. 116(15): p. 7565–7574· [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Zhang H, Wu YJ, and Thierry G, Bilingualism and aging: A focused neuroscientific review. Journal of Neurolinguistics, 2020. 54: p. 100890. [Google Scholar]
- 67.Callahan RM and Gandara PC, The bilingual advantage: Language, literacy, and the US labor market. 2014: Multilingual Matters, Callahan, Rebecca M, Ed.; Gándara Patricia C., Ed. [Google Scholar]
- 68.Katzman R, et al. , Development of dementing illnesses in an 80-year-old volunteer cohort. Annals of Neurology, 1989. 25: p. 317–324. [DOI] [PubMed] [Google Scholar]
- 69.Cabeza R, et al. , Maintenance, reserve and compensation: the cognitive neuroscience of healthy ageing. Nature Reviews Neuroscience, 2018.19(11): p. 701–710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Stern Y, et al. , Whitepaper: Defining and investigating cognitive reserve, brain reserve, and brain maintenance. Alzheimers & Dementia, 2020.16: p. 1305–1311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Bialystok E, Anderson JAE, and Grundy JG, Interpreting cognitive decline in the face of cognitive reserve: Does bilingualism affect cognitive aging? Linguistic Approaches to Bilingualism, 2018. 10.1075/lab.18040.bia [DOI] [Google Scholar]