

Abstract
Objectives
This study characterized the clinical phenotypes of individuals with vocal tremor (VT) using tremor classification criteria published by the International Parkinson and Movement Disorder Society (IPMDS) including laryngeal features from the American Academy of Otolaryngology—Head and Neck Surgery (AAO‐HNS).
Methods
VT phenotypic descriptors were extracted from participant medical records from 2017 to 2019. Clinical phenotype descriptors included the: (a) chief complaint and discipline for the first appointment, (b) demographics, (c) tremor body distribution, condition, frequency, and progression, (d) exacerbating/alleviating factors, (e) treatment approaches, and (g) neurologic comorbidities. Descriptive statistics were conducted.
Results
Of 179 meeting inclusion criteria, 2/3 were female; tremor onset affected voice (43%) or extremity (32%) and 2/3 were documented with tremor duration of 3 years or more. Those with primary VT first saw otolaryngology or speech language pathology (59%), whereas those with primary extremity/head tremor first saw neurology (36%). Documentation commonly omitted tremor clinical features such as (a) observed conditions of tremor (64%), (b) laryngeal features (64%), and (c) tremor frequency (92%). Thus, VT classification was based on comorbidity in 49% of patients (ie, essential tremor (48%), dystonia (72%), and Parkinson's disease (100%)) and 32% had inadequate documentation to classify.
Conclusion
The majority of individuals with VT were unable to be classified based on documented clinical features highlighting the need for consistent multidisciplinary assessment of tremor affecting speech structures. The primary site of tremor determined the first discipline seen. Most commonly classified VT categories included essential tremor (47%), dystonia (28%), Parkinsonism (7%), and isolated VT (19%).
Level of Evidence
4.
Keywords: essential tremor, laryngeal dystonia, Parkinson's disease, vocal tremor, voice tremor
This study characterized electronic medical record documentation of clinical phenotypes of individuals with vocal tremor (VT) using tremor classification criteria published by the International Parkinson and Movement Disorder Society (IPMDS) including laryngeal features from the American Academy of Otolaryngology – Head and Neck Surgery (AAO‐HNS). The majority of individuals with VT were unable to be classified, highlighting the need for consistent multi‐disciplinary assessment and documentation of tremor affecting speech structures. Of 105 individuals able to be classified, 47% were classified as essential tremor, 28% as dystonia, 19% as isolated VT and 7% as Parkinsonism; 2/3 were female for all but the essential tremor group (47%), isolated vocal tremor had later onset of tremor (67 years) compared to other groups (53‐58 years), and those with primary VT first saw otolaryngology/speech‐language pathology (59%) whereas those with primary extremity tremor first saw neurology (36%).

1. INTRODUCTION
The voice is intrinsically tied to personal identity such that impaired quality and function of the voice is associated with lower self‐esteem, impaired communication, and decreased quality of life. 1 , 2 , 3 Vocal tremor (VT) is a common, but poorly studied neurogenic voice problem that can interfere with communication and is typically associated with other movement disorders such as essential tremor (ET), dystonia, and Parkinson's disease (PD). 4 Distinguishing clinical features of VT in isolation or associated with other movement disorders have not been elucidated from prior research. Further, prior investigation of VT has not systematically compared clinical tremor features using tremor classification criteria.
Updated consensus‐based classification criteria for tremor were recently published by the International Parkinson and Movement Disorder Society (IPMDS) that broadly defined tremor as an involuntary, rhythmic oscillatory movement of a body part further classified into tremor syndromes across two clinical axes—clinical features (axis 1) and etiology (axis 2). 5 The IPMDS task force defined several tremor‐specific clinical features (ie, axis 1) (see Figure 1) used to classify clinical syndromes of tremor such as essential tremor (ET), dystonia (DT), or Parkinsonism (see Figure 2). 5 This updated framework classifies individuals with ET having clinical features for less than the minimum duration of 3 years as “indeterminate tremor.” Isolated vocal tremor (IVT) is classified separately, among other isolated tremors affecting individual body structures such as the palate, jaw, and head. This new classification of IVT appeared based on the rationale that the “voice” represents tremor affecting only the larynx. Unfortunately, this reclassification of isolated VT overlooks that VT could originate from any singular or combined respiratory or upper airway speech structure(s) affected by tremor. That is, isolated VT may not meet the classification requirement of an isolated tremor affecting a singular structure. Unfortunately, few publications adequately describe clinical features of VT to elucidate the characteristics necessary for tremor classification. For example, a recent literature review investigated isolated VT as a clinical variant of ET and identified only three publications that adequately characterized individuals with IVT for comparison to classification features of ET. 6
FIGURE 1.

Axis 1 clinical features recommended for classification of tremor by the IPMDS
FIGURE 2.

Axis 1 classification criteria for ET, Essential Tremor Plus, Dystonia, and Parkinsonian tremors
Guidance regarding classification of tremor affecting upper airway structures was published in 2005 by the AAO‐HNS Neurolaryngology Committee. This consensus document offers clinical features of “laryngeal tremor” obtained during nasoendoscopy to distinguish individuals with VT associated with ET, dystonia, or Parkinsonism (see Figure 3). 7 AAO‐HNS characteristics of VT classified as ET included individuals with IVT and the observation of tremor affecting one or multiple upper airway structures regardless of task (ie, during both respiration and speech tasks). In contrast, dystonic VT (DT) (eg, spasmodic dysphonia, or laryngeal dystonia) was characterized by tremor affecting the larynx during speech production (ie, task specificity). 7 Also, DT symptoms may be reduced or eliminated during a “sensory trick” such as placement of the nasoendoscope with or without use of topical anesthesia. 7 Parkinsonism VT was defined by a comorbidity of idiopathic PD and associated with vertical laryngeal oscillation. 7
FIGURE 3.
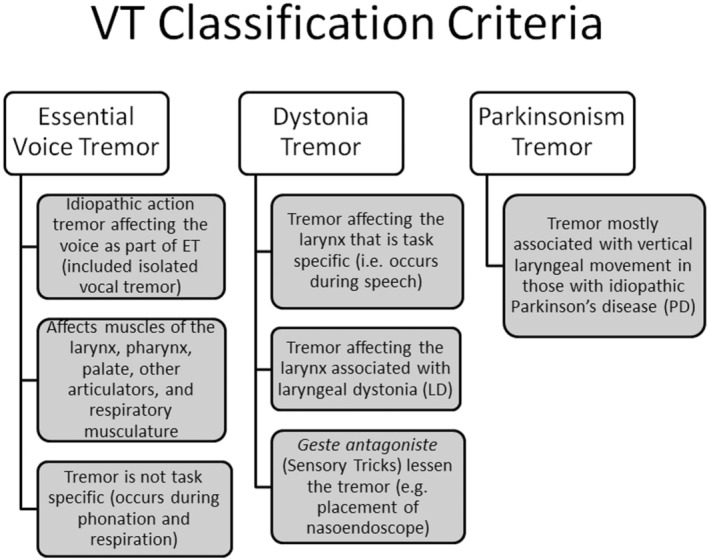
AAO‐HNS Neurolaryngology Committee 7 classification criteria for VT associated with ET, dystonia, and Parkinsonism
Although these two consensus documents offer guidance regarding critical clinical features to assess in those exhibiting VT, no prior studies have systematically utilized these criteria to distinguish VT characteristics by tremor category. 6 , 8 , 9 , 10 The purpose of this study was to characterize the documented clinical phenotypes of individuals with VT using combined IPMDS and AAO‐HNS tremor classification criteria. Typical medical discipline entry points, patterns of assessment, treatment and clinical phenotypic descriptors were also evaluated.
2. MATERIALS AND METHODS
This study was approved by the University of Utah IRB (Protocol#00127836).
2.1. Participants
Participants for this study were identified using the University of Utah (UofU) Data Warehouse and met these inclusion/exclusion criteria: (a) 18 years of age or older, (b) electronic medical record (EMR) documentation containing the phrase, “vocal tremor” or “voice tremor,” (c) completed appointments within UofU outpatient clinics from 2017 to 2019, and (d) a diagnosis containing one or more of the ICD‐10 CPT codes listed in Table 1. The first 300 participants meeting inclusion criteria were identified for manual inspection and EMR data extraction.
TABLE 1.
ICD‐10 codes used to identify participants for consideration for inclusion in the study
| ICD‐10 codes | ICD‐10 associated descriptors |
|---|---|
| R49.0 | Dysphonia |
| Vocal tremor (VT) | |
| Spasmodic dysphonia (SD) | |
| Spasmodic dysphonia + vocal tremor (SD + VT) | |
| Adductor spasmodic dysphonia with vocal tremor (ADSD + VT) | |
| Adductor spasmodic dysphonia with vocal tremor (ADSD + VT) | |
| Adductor spasmodic dysphonia (ADSD) | |
| Abductor spasmodic dysphonia (ABSD) | |
| Mixed spasmodic dysphonia | |
| Essential tremor of spasmodic dysphonia | |
| Dystonic tremor | |
| G25.0 | Essential tremor (ET) |
| G20 | Idiopathic Parkinson's disease (PD) |
| G21.9 | Secondary to Parkinson's disease |
| G24.9 | Dystonia |
2.2. VT clinical feature and classification procedures
The research team (VT, KD, and JBK) developed and reached consensus on operationally defined methods of data extraction. Simultaneous evaluation of EMR documentation was completed on the first five participants to reach consensus. Data extraction and classification criteria are described in Tables 2, 3, 4. Inter‐rater reliability checks were randomly conducted on 15% of participants throughout data collection demonstrating ≥80% reliability across all extracted items and time points.
TABLE 2.
Criteria applied to clinical features and characteristics for EMR data extraction
| Demographics (age, sex, duration of disease) | Age:
|
| Initial evaluation | Date of service: The initial appointment date for tremor despite presence/absence of accompanying notes |
Service/specialty: The service associated with the initial evaluation date above
| |
| Presenting complaint | Primary complaint associated with the initial evaluation date above
|
| Onset of symptoms | Years from the initial evaluation (ie, initial consult year – year documented in the clinical encounter)
|
| Progression | Relating to tremor severity or spread to other body parts over time
|
| Voice percent normal | The patient report of the proportion of normal their current voice is during the clinic visit (eg, 60% of their normal voice)
|
|
Condition of Tremor (rest, postural, and kinetic) |
Determined using the history and physical examination from the first notes available from each specialty and record for any body distribution. Information regarding condition(s) under which tremor was observed could be recorded based on medical record information across the entirety of time span of tremor documentation and before or after treatment approaches if the tremor(s) evolved. |
Condition of VT:
| |
| VT frequency (Hz) | This was only recorded with VT using acoustic measures rather than kinematic measures of tremor rate affecting individual structures. |
| Laryngeal tremor excursion | Vertical:
|
Lengthwise:
| |
AB/ADD:
| |
| Exacerbated by stress | Documented as per HPI and can be reported as anxiety, nervousness, etc. |
| Alcohol responsive | Documentation of benefit of alcohol to tremor
|
| Primary body site | Body site where the tremor was first observed
|
| Body site distribution |
Only documented is a body site is positive for tremor through direct observation of tremor.
For VT, do not assume there is a tremor in the larynx, pharynx, etc. unless there was direct observation of tremor using nasoendoscopy.
|
| Family history | Documented anywhere in the medical chart
|
| Parkinsonism symptoms | See Table 4 for criteria |
| Medication trial | Trialed (yes/no):
|
Type trialed:
| |
Benefit:
| |
| Behavioral (SLP) trial | Trialed (yes/no):
|
Benefit:
| |
| Procedure/surgery trial | Trialed (yes/no) |
Type trialed:
| |
Benefit:
| |
| Disciplines seen | Neurology, ENT, SLP, and psychiatry (ie, psychiatry, neuropsychiatry or neurobehavioral specialists) |
| Diagnoses (primary, secondary, and other) | Diagnosis(es) given at the time of the initial evaluation and recorded in the medical record
|
| Evolving diagnosis | Any diagnosis that changed over subsequent clinical evaluations
|
TABLE 3.
Classification of medications extracted from the EMR
| Medication class | Common medications |
|---|---|
| Beta blocker | Metroprolol |
| Propanolol | |
| Muscle relaxant/antispasmodic | Baclofen |
| Cyclobenzaprine | |
| Benzodiazepine | Alprazolam |
| Clonazepam | |
| Diazepam | |
| Lorazepam | |
| Anticonvulsant | Carbemazepine |
| Gabapentin | |
| Lamotrigine | |
| Levetiracetam | |
| Oxcarbazepine | |
| Phenytoin | |
| Primidone | |
| Topirimate | |
| Valproic acid | |
| Parkinson medications | Amantadine |
| Carbidopa‐Levodopa | |
| Entacapone | |
| Pramipexole | |
| Ropinirole | |
| Selegiline | |
| Other neuropsychiatric medication | Amitryptiline |
| Buproprion | |
| Citalopram | |
| Duloxetine | |
| Fluoxetine | |
| Lithium | |
| Mirtazapine | |
| Paroxetine | |
| Quetiapine |
TABLE 4.
Criteria for medical record classification of vocal tremor (VT)
| VT classification | Clinical features |
|---|---|
| Essential tremor |
1. Bilateral upper limb action tremor (postural or kinetic) 2. At least 3 years' duration 3. With or without tremor in other locations 4. Speech structures exhibited oscillation during respiration and speech tasks 5. Absence of other neurological signs such as dystonia, ataxia, or parkinsonism |
| Inadequate information to classify | Conflicting or missing tremor features that preclude classification |
| Vocal tremor classified by comorbidity | Tremor observed in upper airway structures associated with a single co‐existing neurologic disorder (e.g., essential tremor, dystonia, Parkinson's disease) in the absence of confirmatory nasoendoscopic examination |
| Dystonic tremor |
1. Tremor in a body part affected by dystonia 2. May be focal or segmental 3. Tremor affecting speech structures showing task specificity 4. Sensory trick(s) are reportedly helpful in reducing symptoms 5. Clinical feature of clear phoneme specificity during speech |
| Isolated vocal tremor |
1. Vocal tremor in the absence of tremor affecting the limbs or head 2. No known co‐occurring neurologic comorbidities 3. Tremor observed in speech structures (larynx, tongue, pharynx, palate, face, jaw) |
| Essential plus |
1. Tremor with the characteristics of ET 2. Additional neurological signs of uncertain significance such as impaired tandem gait, questionable dystonic posturing, memory impairment, or other mild neurologic signs. |
| Indeterminate tremor | Does not fit into an established syndrome of ET and has a duration for less than 3 years requiring further observation to clarify the tremor syndrome. |
| Parkinsonism |
1. Tremor observed in someone with bradykinesia and rigidity 2. Documented 4‐7 Hz rest tremor (pill rolling) of the hand 3. Resting tremor of the lower limb, jaw, tongue, or foot 4. Tremor may be asymmetrical and may diminish upon initiation of movement5. May be associated with a diagnosis of Parkinson's disease |
| Other | Tremor etiology from a neurologic condition not defined above |
Final VT classification was rendered upon completion of EMR data extraction using combined tremor classification criteria from the IPMDS and AAO‐HNS (see Table 4). Individuals with VT and a single related neurological diagnosis without nasoendoscopy were “classified by comorbidity.” Those with conflicting or inadequate clinical descriptors were marked as “inadequate information to classify.”
2.3. Statistical analysis
Descriptive statistics were used to analyze and characterize data across all participants as well as by tremor classifications.
3. RESULTS
3.1. Classification rate using medical record documentation
A total of 179 individuals met initial inclusion criteria (see Figure 4); however, a total of 119 (66%) individuals demonstrated adequate EMR documentation to classify and characterize their tremor. Of these individuals, 99 (83%) completed a nasoendoscopy. That is, 55% of the total VT population meeting inclusion criteria completed nasoendoscopic evaluation. Of those classified (N = 119), eight were assigned to tremor categories with fewer than five individuals and an additional six were classified as indeterminate tremor (Figure 4). Thus, outcomes are reported on 105 individuals with VT classified as dystonia (DT), Parkinsonism (PD), essential tremor (ET), and isolated VT (IVT).
FIGURE 4.

Flowchart of participant screening and inclusion evaluation for this study. Only classification categories with ≥5 individuals were included in study analyses and results. Those with indeterminate tremor were also excluded
3.2. Demographic characteristics
Detailed demographic characteristics of the total group and VT classification categories are shown in Table 5.
TABLE 5.
Demographic characteristics overall and by VT classification
| Tremor classification | |||||
|---|---|---|---|---|---|
| Dystonia | Parkinson's disease | Essential tremor | Isolated vocal tremor | Total | |
| Clinical characteristics | N = 29 | N = 7 | N = 49 | N = 20 | N = 105 |
| Classified by comorbidity (%) | 21 (72%) | 7 (100%) | 23 (48%) | 0 (0%) | 51 (49%) |
| Gender | |||||
| Female | 22 (76%) | 6 (86%) | 23 (47%) | 14 (71%) | 65 (62%) |
| Male | 7 (24%) | 1 (14%) | 26 (53%) | 6 (29%) | 40 (38%) |
| Mean age at first evaluation in years (SD, range) | 67 (8.3, 50‐83) | 71 (8.8, 63‐86) | 62 (12.2, 30‐87) | 70 (7.9, 51‐80) | 67 (10.6, 30‐87) |
| Mean age at onset of tremor in years (SD, range) | 53 (12.3, 27‐73) | 58 (10.2, 51‐72) | 56 (11.9, 31‐78) | 67 (12.6, 40‐85) | 52 (12.8, 27‐85) |
| Mean duration of tremor symptoms in years (SD, range) | 10 (7.3, <1‐20+) | 5 (3.5, 1‐11) | 12 (7.2, <1‐20+) | 4 (4.6, <1‐20+) | 10 (7.3, <1‐20+) |
| Family history | |||||
| Tremor | 10 (34%) | 2 (29%) | 29 (59%) | 3 (15%) | 44 (42%) |
| Dystonia | 2 (7%) | 0% | 0 (0%) | 1 (5%) | 3 (3%) |
| Parkinson's disease | 1 (3%) | 2 (29%) | 5 (10%) | 0 (0%) | 8 (8%) |
| Unknown/undocumented | 11 (38%) | 0% | 10 (20%) | 7 (35%) | 28 (27%) |
| Exacerbated by stress (%) | |||||
| Yes | 4 (14%) | 3 (43%) | 14 (29%) | 1 (5%) | 22 (21%) |
| Unknown/undocumented | 25 (86%) | 4 (57%) | 33 (67%) | 19 (95%) | 81 (77%) |
| Responsive to alcohol (%) | |||||
| Yes | 3 (10%) | 0 (0%) | 5 (10%) | 1 (5%) | 9 (9%) |
| Not applicable | 13 (45%) | 5 (71%) | 26 (53%) | 11 (55%) | 55 (52%) |
| Unknown/undocumented | 12 (41%) | 2 (29%) | 16 (33%) | 8 (40%) | 38 (36%) |
| First site of tremor (%) | |||||
| Voice | 18 (28%) | 1 (14%) | 6 (12%) | 20 (100%) | 45 (43%) |
| Head | 0 (0%) | 1 (14%) | 3 (6%) | 0 (0%) | 4 (4%) |
| Extremity | 4 (14%) | 4 (57%) | 26 (53%) | 0 (0%) | 34 (32%) |
| Multiple | 2 (7%) | 0 (0%) | 6 (12%) | 0 (0%) | 8 (8%) |
| Unknown/undocumented | 5 (17%) | 1 (14%) | 8 (16%) | 0 (0%) | 14 (13%) |
| Progression (%) | 16 (55%) | 7 (100%) | 42 (86%) | 6 (30%) | 71 (68%) |
| Comorbidities (%) | |||||
| GERD | 7 (24%) | 3 (43%) | 15 (31%) | 10 (50%) | 35 (33%) |
| Dysphagia | 5 (17%) | 4 (57%) | 15 (31%) | 12 (60%) | 36 (34%) |
| Dyspnea | 2 (7%) | 1 (14%) | 5 (10%) | 5 (25%) | 13 (12%) |
| Anxiety | 5 (17%) | 4 (57%) | 16 (33%) | 5 (25%) | 30 (29%) |
| Depression | 4 (14%) | 4 (57%) | 15 (31%) | 4 (20%) | 27 (26%) |
| Other psychiatric illness | 3 (10%) | 0 (0%) | 1 (2%) | 0 (0%) | 4 (4%) |
3.2.1. VT classification
Of those with VT that were classified, 29 individuals (28%) were classified as DT, 7 as PD (7%), 49 as ET (47%), and 20 as IVT (19%). Within groups, the majority of those classified as DT, ET and PD were based on comorbidities rather than clinical features.
3.2.2. Sex
The majority of participants were female (62%); similar findings occurred for all tremor categories except for ET in which nearly equal representation between males (53%) and females (47%) occurred.
3.2.3. Age
The mean age at first evaluation was 67 years (SD = 10.6; 30‐87 years). The average age at tremor onset was 52 years (SD = 12.8; 27‐85 years). Those diagnosed with IVT exhibited a later average onset of tremor (67; 40‐85 years) compared to other VT categories averaging 53‐58 years (range = 27‐78 years). The time from onset of tremor and the initial evaluation averaged 12 and 13 years in those with DT and PD, respectively, whereas IVT and ET averaged 4 and 6 years, respectively.
3.2.4. Duration of symptoms
The average duration of tremor symptoms was 10 years (SD = 7.3; <1 to 20+ years). The longest duration of symptoms occurred in those with DT (10 ± 7.3 years; <1 to 20+ years) and ET (12 ± 7.2 years; <1 = 20+ years). Those with PD and IVT showed the shortest average duration of symptoms (5 and 4 years, respectively).
3.2.5. Family history
On average, 42% of those with VT reported a family history of tremor. The majority belonged to the ET group (59%) with ~1/3 each from the DT and PD groups. Approximately 30% of those with PD also reported a family history of PD. Family history features were unknown in 38% of those with DT and 35% of those with IVT.
3.2.6. Exacerbated by stress
This feature was not documented or assessed in 77% of participants.
3.2.7. Responsive to alcohol
The study location potentially influenced outcomes for this clinical feature. The majority of respondents did not consume alcohol (52%); this feature was undocumented in ~1/3 of participants and only 9% confirmed that alcohol reduced tremor symptoms.
3.2.8. First site of tremor
The first site of tremor was reported as the voice in 100% of those with IVT and ~60% of those with DT. Those reporting tremor first in the extremities (eg, hands) were primarily classified as ET (54%) and PD (57%).
3.2.9. Progression of tremor
On average, the majority of participants (68%) reported progression of their symptoms. However, only 1/3 of the IVT group reported progression of their tremor symptoms.
3.2.10. Comorbidities
On average, 29% of participants were documented with anxiety and depression; approximately 33% were documented with GERD and dysphagia. Over 50% of those classified as PD were documented with anxiety, depression, and dysphagia, and 43% had GERD. Over 50% of the IVT group was documented with GERD and dysphagia; DT had the fewest comorbidities.
3.3. VT clinical features
The clinical features of body distribution, symmetry, and condition of tremor by classification category are shown in Table 6.
TABLE 6.
VT nasoendoscopy clinical features of body distribution, symmetry, and condition by tremor category
| Dystonia (DT) (N = 22) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Condition | ||||||||||||
| Body distribution | Symmetry | Respiration | Speech | |||||||||
| Speech structure | Present | Absent | Unknown | Unilateral | Bilateral | Unknown | Present | Absent | Unknown | Present | Absent | Unknown |
| Larynx | 21 (95%) | 0 (0%) | 1 (5%) | 0 (0%) | 7 (32%) | 15 (68%) | 4 (18%) | 4 (18%) | 14 (64%) | 19 (86%) | 0 (0%) | 3 (14%) |
| Pharynx | 11 (50%) | 4 (18%) | 7 (32%) | 0 (0%) | 6 (27%) | 16 (73%) | 0 (0%) | 0 (0%) | 22 (100%) | 9 (41%) | 0 (0%) | 13 (59%) |
| Palate | 16 (73%) | 0 (0%) | 6 (27%) | 0 (0%) | 6 (27%) | 16 (73%) | 2 (9%) | 1 (5%) | 19 (86%) | 12 (55%) | 0 (0%) | 10 (45%) |
| Tongue | 7 (32%) | 6 (27%) | 9 (41%) | 0 (0%) | 2 (9%) | 20 (91%) | 0 (0%) | 1 (5%) | 21 (95%) | 4 (18%) | 0 (0%) | 18 (82%) |
| Face | 1 (5%) | 9 (41%) | 12 (55%) | 0 (0%) | 9 (41%) | 13 (59%) | 0 (0%) | 0 (0%) | 22 (100%) | 0 (0%) | 0 (0%) | 22 (100%) |
| Jaw | 2 (9%) | 2 (9%) | 18 (82%) | 0 (0%) | 0 (0%) | 22 (100%) | 0 (0%) | 0 (0%) | 22 (100%) | 0 (0%) | 0 (0%) | 22 (100%) |
| Parkinson's disease (PD) (N = 5) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Condition | ||||||||||||
| Body distribution | Symmetry | Respiration | Speech | |||||||||
| Speech structure | Present | Absent | Unknown | Unilateral | Bilateral | Unknown | Present | Absent | Unknown | Present | Absent | Unknown |
| Larynx | 5 (100%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 5 (100%) | 1 (20%) | 0 (0%) | 4 (80%) | 2 (40%) | 0 (0%) | 3 (60%) |
| Pharynx | 1 (20%) | 0 (0%) | 4 (80%) | 0 (0%) | 1 (20%) | 4 (80%) | 0 (0%) | 0 (0%) | 5 (100%) | 1 (20%) | 0 (0%) | 4 (80%) |
| Palate | 2 (40%) | 0 (0%) | 3 (60%) | 0 (0%) | 1 (20%) | 4 (80%) | 1 (20%) | 0 (0%) | 4 (80%) | 2 (40%) | 0 (0%) | 3 (60%) |
| Tongue | 1 (20%) | 2 (40%) | 2 (40%) | 0 (0%) | 0 (0%) | 5 (100%) | 0 (0%) | 0 (0%) | 5 (100%) | 0 (0%) | 0 (0%) | 5 (100%) |
| Face | 0 (0%) | 2 (40%) | 3 (60%) | 0 (0%) | 0 (0%) | 3 (60%) | 0 (0%) | 0 (0%) | 3 (60%) | 0 (0%) | 0 (0%) | 5 (100%) |
| Jaw | 0 (0%) | 0 (0%) | 5 (100%) | 0 (0%) | 0 (0%) | 5 (100%) | 0 (0%) | 0 (0%) | 5 (100%) | 0 (0%) | 0 (0%) | 5 (100%) |
| Essential tremor (ET) (N = 25) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Condition | ||||||||||||
| Body distribution | Symmetry | Respiration | Speech | |||||||||
| Speech structure | Present | Absent | Unknown | Unilateral | Bilateral | Unknown | Present | Absent | Unknown | Present | Absent | Unknown |
| Larynx | 25 (100%) | 0 (0%) | 0 (0%) | 0 (0%) | 11 (44%) | 14 (56%) | 7 (28%) | 3 (12%) | 15 (60%) | 23 (92%) | 0 (0%) | 2 (8%) |
| Pharynx | 18 (72%) | 4 (16%) | 3 (12%) | 0 (0%) | 11 (44%) | 14 (56%) | 3 (12%) | 1 (4%) | 21 (84%) | 14 (56%) | 0 (0%) | 11 (44%) |
| Palate | 18 (72%) | 4 (16%) | 3 (12%) | 0 (0%) | 7 (28%) | 18 (72%) | 5 (20%) | 2 (8%) | 18 (72%) | 15 (60%) | 0 (0%) | 10 (40%) |
| Tongue | 4 (16%) | 16 (64%) | 5 (20%) | 0 (0%) | 2 (8%) | 23 (92%) | 2 (8%) | 0 (0%) | 23 (92%) | 1 (4%) | 0 (0%) | 24 (96%) |
| Face | 4 (16%) | 15 (60%) | 6 (24%) | 0 (0%) | 11 (44%) | 14 (56%) | 2 (8%) | 0 (0%) | 23 (92%) | 1 (4%) | 0 (0%) | 24 (96%) |
| Jaw | 9 (36%) | 2 (8%) | 14 (56%) | 0 (0%) | 2 (8%) | 23 (92%) | 2 (8%) | 0 (0%) | 23 (92%) | 2 (8%) | 0 (0%) | 23 (92%) |
| Isolated vocal tremor (IVT) (N = 20) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Speech structure | Condition | |||||||||||
| Body distribution | Symmetry | Respiration | Speech | |||||||||
| Present | Absent | Unknown | Unilateral | Bilateral | Unknown | Present | Absent | Unknown | Present | Absent | Unknown | |
| Larynx | 19 (95%) | 0 (0%) | 1 (5%) | 1 (5%) | 5 (25%) | 14 (70%) | 10 (50%) | 1 (5%) | 9 (45%) | 16 (80%) | 0 (0%) | 4 (20%) |
| Pharynx | 9 (45%) | 7 (35%) | 4 (20%) | 0 (0%) | 6 (30%) | 14 (70%) | 2 (10%) | 0 (0%) | 18 (90%) | 6 (30%) | 0 (0%) | 14 (70%) |
| Palate | 10 (50%) | 5 (25%) | 5 (25%) | 0 (0%) | 7 (35%) | 13 (65%) | 2 (10%) | 0 (0%) | 18 (90%) | 10 (50%) | 0 (0%) | 10 (50%) |
| Tongue | 3 (15%) | 8 (40%) | 9 (45%) | 0 (0%) | 2 (10%) | 18 (90%) | 2 (10%) | 0 (0%) | 18 (90%) | 1 (5%) | 0 (0%) | 19 (95%) |
| Face | 1 (5%) | 9 (45%) | 10 (50%) | 0 (0%) | 9 (45%) | 11 (55%) | 1 (5%) | 0 (0%) | 19 (95%) | 0 (0%) | 0 (0%) | 20 (100%) |
| Jaw | 1 (5%) | 3 (15%) | 16 (80%) | 0 (0%) | 0 (0%) | 20 (100%) | 0 (0%) | 0 (0%) | 20 (100%) | 1 (5%) | 0 (0%) | 19 (95%) |
3.3.1. Body distribution
As shown in Table 6 and Figure 5, the anatomical distribution of tremor affecting speech structures showed tremor of the larynx for all categories of VT. The pharynx and palate were also frequently affected in those with DT, ET and IVT. The tongue, face, and jaw were less frequently documented.
FIGURE 5.

Body distribution of tremor across speech structures by classification
3.3.2. Tremor symmetry
Tremor symmetry across affected structures was undocumented for 56% to 100% of structures; however, those in which symmetry was documented showed bilateral tremor. Unilateral laryngeal tremor was documented in one individual classified with IVT.
Additional features of laryngeal tremor were infrequently documented. When documented, 40% to 52% of all tremor categories exhibited horizontal oscillation of the larynx (ie, abduction/adduction) (see Figure 6). Vertical oscillation of the larynx was documented in 50% of those with DT and 48% of those with ET compared to 20% and 26% of those with PD and IVT, respectively. Lengthwise oscillation (ie, anterior/posterior) oscillation was undocumented in 72% to 100% of individuals.
FIGURE 6.

Laryngeal tremor features by VT classification
3.3.3. Condition of tremor
Tremor affecting speech structures was typically judged during speech production. Across VT categories, specification of tremor assessment during respiration was not typically documented at comparable rates for the larynx (48%‐80%), pharynx (84%‐100%), palate (72%‐89%), tongue (89%‐100%), face (60%‐100%), and jaw (92%‐100%). The most frequent occurrence of laryngeal tremor across conditions occurred for those classified as IVT (48%) and ET (28%).
3.3.4. Tremor frequency
Of 105 individuals, 5 individuals had measures of VT frequency; acoustic measures were documented for 1 individual each with ET (2‐4 Hz) and DT (4‐5 Hz), and 3 individuals with IVT (4‐10 Hz) (N = 7).
3.4. VT clinical assessment patterns by discipline
The clinical patterns of VT care based on symptoms and discipline‐specific encounters are summarized in Table 7.
TABLE 7.
Vocal tremor classifications and discipline‐specific assessment and treatment patterns
| Tremor classification | |||||
|---|---|---|---|---|---|
| Dystonia | Parkinson's disease | Essential tremor | Isolated vocal tremor | Total | |
| Characteristic | N = 29 | N = 7 | N = 49 | N = 20 | N = 105 |
| Primary complaint at first visit | |||||
| Voice | 24 (83%) | 1 (14%) | 20 (41%) | 16 (80%) | 61 (58%) |
| Extremity tremor | 6 (14%) | 4 (57%) | 28 (57%) | 0 (0%) | 38 (36%) |
| Other | 1 (3%) | 2 (29%) | 1 (2%) | 4 (20%) | 8 (8%) |
| First specialty to assess tremor (%) | |||||
| OTO ± SLP | 26 (90%) | 1 (14%) | 22 (45%) | 20 (100%) | 69 (66%) |
| Neurology | 3 (10%) | 6 (86%) | 24 (49%) | 0 (0%) | 33 (31%) |
| Other | 0 (0%) | 0 (0%) | 3 (6%) | 0 (0%) | 3 (3%) |
| All disciplines seen (%) | |||||
| OTO | 26 (90%) | 4 (57%) | 28 (57%) | 19 (95%) | 77 (73%) |
| SLP | 23 (79%) | 5 (71%) | 26 (53%) | 19 (95%) | 73 (70%) |
| Neurology | 14 (48%) | 7 (100%) | 42 (86%) | 3 (15%) | 66 (63%) |
| Psych | 2 (7%) | 3 (43%) | 15 (31%) | 2 (10%) | 22 (21%) |
| Medication trial (%) | |||||
| Yes | 11 (38%) | 7 (100%) | 42 (86%) | 2 (10%) | 62 (59%) |
| No | 15 (52%) | 0 (0%) | 7 (14%) | 18 (90%) | 40 (38%) |
| Speech therapy trial (%) | |||||
| Yes | 10 (34%) | 2 (29%) | 11 (22%) | 13 (65%) | 36 (34%) |
| No | 17 (59%) | 5 (71%) | 37 (76%) | 7 (35%) | 66 (63%) |
| Procedure/surgery trial (%) | |||||
| Yes | 24 (83%) | 2 (29%) | 29 (59%) | 6 (30%) | 61 (58%) |
| No | 5 (17%) | 5 (71%) | 19 (39%) | 14 (70%) | 43 (41%) |
3.4.1. Primary complaint at initial encounter
Voice was the primary complaint during the first clinic visit in 61 patients (58%); extremity tremor was the primary complaint in 38 patients (36%). The majority of individuals classified as IVT (80%) and DT (83%) reported their voice as a primary concern compared to 41% of those with ET and 14% of those with PD. In addition, VT was documented in eight patients (8%) listing primary complaints other than tremor such as cough, dysphagia, weakness, or various gait or movement disorders. Those classified with PD primarily expressed concern about symptoms affecting their extremities (57%) as did those with ET (57%).
3.4.2. Initial evaluation by discipline
The initial evaluation was documented by otolaryngology (OTO) and/or speech‐language pathology (SLP) for 69 patients (66%), neurology in 33 patients (31%), or another specialty in 3 patients (3%). Those classified with DT and IVT most commonly saw OTO or SLP first (90% and 100%), respectively. Those classified with PD presented first to neurology (86%) whereas those classified with ET presented either to OTO/SLP (45%) or neurology (49%) at nearly equal rates and corresponding with their primary complaint of voice (OTO/SLP) versus extremity tremor, or other movement disorder (neurology).
3.4.3. Disciplines involved in care over time
The majority of individuals with VT were evaluated/treated by OTO (73%), SLP (70%), and neurology (63%). A smaller proportion was seen by psychiatry/neuropsychiatry (21%) and neuro‐ophthalmology (4%). Nearly 100% of those classified as IVT and ~80% of those with DT were seen by OTO/SLP whereas the majority of those with ET (86%) and PD (100%) saw neurology compared to OTO (~50%). Those with PD were seen by SLPs 71% of the time compared to ~50% of those with ET.
3.5. Treatment patterns
3.5.1. Pharmaceutical
Medications were trialed in 59% of all participants (see Table 7). As shown in Figure 7, all individuals classified as PD were prescribed Parkinsonism medications. A small proportion of those with ET (22%) also trialed these medications. Beta blockers and anticonvulsants were the next most common class of medication prescribed to those in the ET (71% and 69%, respectively) and DT (24% for both) groups. A small proportion of each VT group was prescribed a benzodiazepine (5%‐22%) or medications for depression, anxiety, etc. (5%‐29%).
FIGURE 7.

Medications prescribed by VT classification
3.5.2. Procedural/surgical treatment
Procedural or surgical intervention was trialed in 61 (58%) of participants (see Table 7). As shown in Figure 8, botulinum toxin (Botox) was used to treat 83% of those classified as DT, 35% with ET (35%), and 30% with IVT. Other surgical treatments included unilateral or bilateral deep brain stimulation (DBS) in the DT, PD, and ET groups (3%‐14%) and focused ultrasound (FUS) treatment for those in the ET group (16%). Outcomes specific to VT were not documented for these therapies.
FIGURE 8.

Procedure and surgical treatments trialed by VT classification
3.5.3. Behavioral treatment
Behavioral treatment was completed in 34% of participants. The majority receiving behavioral treatment were classified as IVT (65%) whereas 1/3 or less of the other groups received behavioral treatment.
4. DISCUSSION
This is the first study to systematically evaluate VT clinical features using combined IPMDS and AAO‐HNS tremor classification criteria. The findings of this study offer important insights regarding VT clinical features for classification in addition to clinician assessment, documentation, and treatment patterns to inform future clinical practice and research patterns.
4.1. VT documentation challenges
Notable limitations in the systematic data extraction from this regional medical center's EMR documentation elucidate inconsistencies in clinical practice and documentation patterns across disciplines that likely can be generalized to other clinic sites/regions. One third of the total number of participants could not be classified due to inadequate documentation of VT clinical features. This is likely due to less than half of all participants undergoing VT evaluation using nasoendoscopy. In addition, interpretation of nasoendoscopy exams was limited by the absence of both positive and negative findings from OTO and SLP disciplines regarding body distribution, condition of tremor, and symmetry. Consequently, half of all patients in the DT, ET, and PD groups were classified based on comorbidities rather than VT clinical features.
The likelihood that these documentation patterns generalize to other OTO and SLP clinicians is probable given that there is no accepted standard practice of VT assessment and the current VT literature identifies few clinical features necessary for VT classification. 6 , 9 , 11 , 12 The only published vocal tremor scoring system evaluates tremor presence/absence and severity for each of the visible pharyngeal structures during nasoendoscopy. 11 In contrast, neurology clinicians evidenced consistent clinical assessment and documentation patterns of tremor. Unfortunately, participants evaluated solely by neurology did not complete imaging of upper airway structures critical to document speech structure contributions to VT. These findings underline the importance of multi‐disciplinary assessment of VT by OTO, SLP, and neurology to assure that all relevant features, including the extremities, are assessed and documented for VT classification.
4.2. VT clinical features
On average, females comprised the majority of those with VT. The only category where this was not the case was for those classified as ET in which nearly equal representation of males and females occurred. This was contrary to previously published findings for essential VT (EVT). 9 , 10 However, prior findings for EVT included those separately classified in this study as IVT. Those with IVT in this study exhibited a higher proportion of females similar to the DT and PD groups. The ET group showed similar male‐to‐female ratios as reported in the literature for ET, in general. 13 , 14 , 15 , 16 , 17 , 18 The IVT group was also older at onset of their tremor than the ET group by ~10 years, on average. Currently, the OTO and SLP disciplines consider IVT to be a clinical variant of ET 6 , 7 , 8 , 9 , 19 whereas the IPDMS did not find adequate evidence in the literature to combine these two groups. 5 Our findings suggest that separate classification of those with VT into IVT and ET groups is warranted until adequate evidence accumulates to support IVT as a clinical variant of ET.
Not surprisingly, the first site of tremor was commonly reported to affect extremities in those classified as ET and PD. In contrast, those classified as DT and IVT reported voice as the first site of tremor. Nearly all of those in the ET and PD groups reported progression of their tremor symptoms over time as did half of the DT group and 1/3 of those in the IVT. This finding suggests that tremor affecting extremities is more likely to progress than tremor predominantly affecting speech structures.
Laryngeal tremor was identified for all VT categories. Body distribution was best documented for the larynx, pharynx, and palate, although symmetry and condition of VT was poorly documented. Tremors of the pharynx and palate were most frequently documented in those with DT, ET, and IVT. PD also showed tremor of the palate, but the pharynx was not commonly documented. Tremor affecting the tongue, face, and jaw tremor was less frequently documented; however, it was unclear whether tremor was absent, or untested in these structures. The lack of documentation for body distribution points to the need for a systematic, multidisciplinary assessment.
On average, laryngeal tremor features were absent in over 68% of participants. When documented, unique laryngeal tremor features included consistent documentation of horizontal oscillation of the arytenoids across all VT groups with vertical oscillation mostly in those with DT and ET. IVT and PD also showed vertical oscillation in some participants; however, the AAO‐HNS described vertical laryngeal tremor as a prominent feature of PD in contrast to our findings. 7 Lengthwise laryngeal tremor was less commonly documented across all VT groups.
Documentation of laryngeal tremor features may indicate optimal musculature for Botox treatment; horizontal oscillation supports treatment targeting interarytenoid musculature 20 whereas lengthwise oscillation supports injection of the thyroarytenoid (TA) musculature. 21 Vertical oscillation suggests benefit from treatment of extrinsic neck musculature. 22 , 23 Thus, documentation of this clinical feature is important for VT classification as well as Botox treatment planning.
Condition of tremor (ie, respiration vs speech observation) was infrequently reported resulting in difficulty judging task specificity. Task specificity is a critical clinical feature of DT in addition to documentation of benefit from sensory tricks. The absence of documentation of these features required classification based on clinical findings of phoneme specificity with comorbid dystonia. 7 Reliance on auditory‐perception of phoneme specificity of symptoms to classify DT is problematic given that VT can only be heard during voicing. Thus, VT is also best perceived during production of voiced phonemes. As such, classification of DT vs ET requires direct observation of upper airway structures during respiration and speech tasks and assessment of sensory tricks to distinguish these groups.
To classify those with VT, consistent clinical assessment of tremor affecting speech structures is needed to document positive and negative findings regarding body distribution, frequency, and condition. An example of such a speech structure tremor assessment tool is shared in the Appendix materials.
4.3. VT and discipline‐specific patterns
On average, the initial evaluation of VT was by OTO/SLP. Those classified as DT and IVT most commonly saw OTO/SLP disciplines first whereas those in the PD group saw the neurologist first. Those in the ET group were split between disciplines at the first visit corresponding to their primary complaint for voice or extremities. These findings suggest that PD and ET groups more commonly experience tremor first in their extremities. 5 , 18 , 24 , 25 , 26 Interestingly, voice was a primary issue for nearly half of the ET group; this may reflect that half experienced onset of tremor first in the voice, or were bothered by VT more than extremity tremor. Future investigation is needed to clarify this pattern.
4.4. Treatment patterns
Treatment patterns differed by VT group. Overall, medication and procedure/surgery approaches were documented in approximately half of participants. Pharmaceutical treatment was most common in the PD and ET groups and in 40% of those in the DT group. The most common classes of medication prescribed for those with ET and DT included beta blockers and anticonvulsants whereas those with PD trialed Parkinsonism medications. DT and ET were most commonly recommended for procedure/surgical treatment with the most frequently used treatment being Botox injections. Speech treatment was documented in approximately 1/3 of the DT, ET, and PD groups in contrast to the majority of the IVT groups. Treatment outcomes specific to VT were not adequately documented for reporting and would be an important aspect for future investigation relative to VT groups and associated clinical features.
4.5. Study limitations
The outcomes of this study relied on the accuracy of electronic medical record documentation to extract and characterize clinical features of those identified with vocal tremor for classification. None of the participants underwent additional clinical testing to substantiate the accuracy of documented features. Future clinical research is necessary to address missing medical record documentation of vocal tremor clinical features as well as to evaluate replicability of this study's findings.
5. CONCLUSION
Clinical features of VT critical for classification were often absent from EMR documentation resulting in frequent classification by comorbidity, or inability to classify participants. Body distribution was commonly documented demonstrating VT most commonly affected the larynx for all groups; however, the pharynx and palate were also frequently affected whereas tongue, jaw, and face were less commonly documented. Several novel demographic findings between VT groups were found. To classify VT groups, multidisciplinary evaluation by OTO, SLP, and neurology is recommended, including consistent assessment of positive and negative findings for body distribution, frequency, and condition of tremor patterns affecting speech structures.
CONFLICT OF INTEREST
V. T. has no conflicts of interest to disclose. K. D. is currently employed as a University of Utah pre‐doctoral student on R01DC016838. J. B.‐K. is the PI of R01DC016838 that partially supported this project; she also receives royalties from MedBridge for online courses on the topic of vocal tremor assessment and treatment. Nonfinancial conflicts include service as a scientific advisory member for the NSDA and membership in ASHA and ASHA's Special Interest Group on voice and upper airway disorders.
Supporting information
Appendix S1 Clinical protocol for assessment of tremor features affecting speech structures.
ACKNOWLEDGMENTS
This project was partially funded by R01DC016838 (PI: Barkmeier‐Kraemer), “Physiologic correlates of vocal tremor affecting those with essential tremor.”
Torrecillas V, Dwenger K, Barkmeier‐Kraemer JM. Classification of vocal tremor using updated consensus‐based tremor classification criteria. Laryngoscope Investigative Otolaryngology. 2021;6:261–276. 10.1002/lio2.544
Funding information National Institute on Deafness and Other Communication Disorders, Grant/Award Number: R01DC016838
BIBLIOGRAPHY
- 1. Hogikyan ND, Sethuraman G. Validation of an instrument to measure voice‐related quality of life (V‐RQOL). J Voice. 1999;13(4):557‐569. [DOI] [PubMed] [Google Scholar]
- 2. Cohen SM. Self‐reported impact of dysphonia in a primary care population: an epidemiological study. Laryngoscope. 2010;120(10):2022‐2032. [DOI] [PubMed] [Google Scholar]
- 3. Verdonck‐de Leeuw IM, Mahieu HF. Vocal aging and the impact on daily life: a longitudinal study. J Voice. 2004;18(2):193‐202. [DOI] [PubMed] [Google Scholar]
- 4. Woodson G. Management of neurologic disorders of the larynx. Ann Otol Rhinol Laryngol. 2008;117(5):317‐326. [DOI] [PubMed] [Google Scholar]
- 5. Bhatia KP, Bain P, Bajaj N, et al. Consensus statement on the classification of tremors. From the task force on tremor of the International Parkinson and Movement Disorder Society. Mov Disord. 2018;33(1):75‐87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Barkmeier‐Kraemer JM. Isolated voice tremor: a clinical variant of essential tremor or a distinct clinical phenotype? Tremor Other Hyperkinet Mov (N Y). 2020;10. 10.7916/tohm.v0.738. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Merati AL, Heman‐Ackah YD, Abaza M, Altman KW, Sulica L, Belamowicz S. Common movement disorders affecting the larynx: a report from the neurolaryngology committee of the AAO‐HNS. Otolaryngol Head Neck Surg. 2005;133(5):654‐665. [DOI] [PubMed] [Google Scholar]
- 8. Patel A, Frucht SJ. Isolated vocal tremor as a focal phenotype of essential tremor: a retrospective case review. J Clin Mov Disord. 2015;2:1‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Sulica L, Louis ED. Clinical characteristics of essential voice tremor: a study of 34 cases. Laryngoscope. 2010;120(3):516‐528. [DOI] [PubMed] [Google Scholar]
- 10. Massey EW, Paulson GW. Essential vocal tremor: clinical characteristics and response to therapy. South Med J. 1985;78(3):316‐317. [PubMed] [Google Scholar]
- 11. Bove M, Daamen N, Rosen C, Wang CC, Sulica L, Gartner‐Schmidt J. Development and validation of the vocal tremor scoring system. Laryngoscope. 2006;116(9):1662‐1667. [DOI] [PubMed] [Google Scholar]
- 12. Ludlow CL, Domangue R, Sharma D, et al. Consensus‐based attributes for identifying patients with spasmodic dysphonia and other voice disorders. JAMA Otolaryngol Head Neck Surg. 2018;144(8):657‐665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Elble RJ. The essential tremor syndromes. Curr Opin Neurol. 2016;29(4):507‐512. [DOI] [PubMed] [Google Scholar]
- 14. Govert F, Deuschl G. Tremor entities and their classification: an update. Curr Opin Neurol. 2015;28(4):393‐399. [DOI] [PubMed] [Google Scholar]
- 15. Louis ED. Diagnosis and management of tremor. Continuum (Minneap Minn). 2016;22(4):1143‐1158. [DOI] [PubMed] [Google Scholar]
- 16. Louis ED. Essential tremor: a nuanced approach to the clinical features. Pract Neurol. 2019;19(5):389‐398. [DOI] [PubMed] [Google Scholar]
- 17. Louis ED, Ottman R. How many people in the USA have essential tremor? Deriving a population estimate based on epidemiological data. Tremor Other Hyperkinet Mov (N Y). 2014;4:259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Romero JP, Benito‐León J, Bermejo‐Pareja F. The NEDICES study: recent advances in the understanding of the epidemiology of essential tremor. Tremor Other Hyperkinet Mov (N Y). 2012;2. 10.7916/D8N58K4H. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Orbelo DM, Duffy JR, Hughes Borst BJ, Ekbom D, Maragos NE. Differences in botulinum toxin dosing between patients with adductor spasmodic dysphonia and essential voice tremor. J Voice. 2014;28(1):123‐127. [DOI] [PubMed] [Google Scholar]
- 20. Kendall KA, Leonard RJ. Interarytenoid muscle botox injection for treatment of adductor spasmodic dysphonia with vocal tremor. J Voice. 2011;25(1):114‐119. [DOI] [PubMed] [Google Scholar]
- 21. Blitzer A, Brin MF, Stewart CF. Botulinum toxin management of spasmodic dysphonia (laryngeal dystonia): a 12‐year experience in more than 900 patients. Laryngoscope. 2015;125(8):1751‐1757. [DOI] [PubMed] [Google Scholar]
- 22. Nelson RC, Silva Merea V, Tierney WS, Milstein C, Benninger MS, Bryson PC. Laryngeal botulinum toxin injection for vocal tremor: utility of concurrent strap muscle injection. Laryngoscope. 2019;129(6):1433‐1437. [DOI] [PubMed] [Google Scholar]
- 23. Gurey LE, Sinclair CF, Blitzer A. A new paradigm for the management of essential vocal tremor with botulinum toxin. Laryngoscope. 2013;123(10):2497‐2501. [DOI] [PubMed] [Google Scholar]
- 24. Armstrong MJ, Okun MS. Diagnosis and treatment of Parkinson disease: a review. JAMA. 2020;323(6):548‐560. [DOI] [PubMed] [Google Scholar]
- 25. Gigante AF, Pellicciari R, Iliceto G, et al. Rest tremor in Parkinson's disease: body distribution and time of appearance. J Neurol Sci. 2017;375:215‐219. [DOI] [PubMed] [Google Scholar]
- 26. Pasquini J, Ceravolo R, Qamhawi Z, et al. Progression of tremor in early stages of Parkinson's disease: a clinical and neuroimaging study. Brain. 2018;141(3):811‐821. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix S1 Clinical protocol for assessment of tremor features affecting speech structures.