

Abstract
Coronavirus disease 2019 vaccinations for healthcare workers (HCWs) have begun in South Korea. To investigate adverse events (AEs) of the first dose of each vaccine, any symptom was collected daily for seven days after vaccination in a tertiary hospital. We found that 1,301 of 1,403 ChAdOx1 nCoV-19 recipients and 38 of 80 BNT162b2 recipients reported AEs respectively (90.9% vs. 52.5%): injection-site pain (77.7% vs. 51.2%), myalgia (60.5% vs. 11.2%), fatigue (50.7% vs. 7.5%), headache (47.4% vs. 7.5%), and fever (36.1% vs. 5%; P < 0.001 for all). Young HCWs reported more AEs with ChAdOx1 nCoV-19 than with BNT162b2. No incidences of anaphylaxis were observed. Only one serious AE required hospitalization for serious vomiting, and completely recovered. In conclusion, reported AEs were more common in recipients with ChAdOx1 nCoV-19 than in those with BNT162b2. However, most of the reported AEs were mild to moderate in severity. Sufficient explanation and preparation for expected AEs required to promote widespread vaccination.
Keywords: Coronavirus Disease 2019, Vaccine, Adverse Event, ChAdOx1 nCoV-19 Vaccine, BNT162b2 mRNA COVID-19 Vaccine
Graphical Abstract
Coronavirus disease 2019 (COVID-19) has rapidly spread worldwide to more than 121 million confirmed cases and 2.6 million death as of March 21, 2021.1 To overcome the global-pandemic of COVID-19, several vaccines have been developed and proven effective for preventing virus infection and disease progression in a real-world setting.2,3,4,5,6,7,8,9 As of March 15, 2021, the Korea Ministry of Food and Drug Safety has approved two COVID-19 vaccines: the ChAdOx1 nCoV-19 vaccine from Oxford/AstraZeneca (ChAdOx1 nCoV-19) and the BNT162b2 mRNA COVID-19 vaccine from BioNTech and Pfizer (BNT162b2). Because of the characteristics of each vaccine platform, different degrees of reactogenicity and adverse events (AEs) are anticipated in recipients.2 Although the incidence rates of AEs of ChAdOx1 nCoV-19 and BNT162b2 varied in clinical trials, the differences might have resulted from the method of monitoring AEs.3,4,6,7,8,10 In this study, we evaluated and compared the AEs of ChAdOx1 nCoV-19 and BNT162b2 mRNA vaccines in the prospective cohort of healthcare workers (HCWs) using a self-report form.
Samsung Changwon Hospital is a 750-bed tertiary care academic hospital with an 8-bed intensive care unit for severe COVID-19 patients. A BNT162b2 vaccination program was initiated for HCWs who encounter COVID-19 patients on March 3, 2021, while ChAdOx1 nCoV-19 vaccination program began on March 5, 2021. After obtaining consent, all willing HCWs were vaccinated. To investigate for and manage AEs, the center for infection prevention and control of our hospital requested vaccine recipients to report their symptoms daily for seven days after vaccination. Symptoms were recorded using a self-report form. The reported AEs were classified as local events (pain at the injection site, redness/swelling at the injection site, and regional lymphadenopathy associated with the injection) and systemic events (fever, chill, fatigue, nausea, vomiting, headache, myalgia, arthralgia, urticaria, and others). Our hospital guidelines for vaccine AEs were based on the national guidelines (Supplementary Table 1)11; HCWs with AE were referred for the medical care or observation depending on type and severity of AEs. We also compared the frequencies and characteristics of AEs between vaccines. All statistical analyses were performed using SPSS version 23.0 for Windows (IBM Corp., 2015, Chicago, IL, USA). Student's t-test or Mann-Whitney test was used to compare the continuous variables of the two groups, and one-way ANOVA or Kruskal–Wallis test was used to compare the continuous variables of the groups. Categorical variables were compared using the χ2 test or Fisher's exact test. All P values were two-tailed, and P values < 0.05 were considered statistically significant.
During the vaccination program, 1,440 and 80 HCWs received the ChAdOx1 nCoV-19 and BNT162b2 vaccines, respectively. There was no significant difference in age and occupation type between the groups; however, there was much more male HCWs in the BNT162b2 group than in the ChAdOx1 nCoV-19 group (Supplementary Table 2).
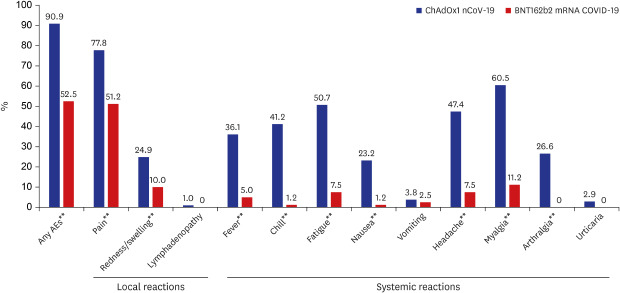
Among these recipients, 1,431 and 80 HCWs in the respective vaccine groups reported symptoms at least once during the seven days following vaccination (Supplementary Table 3). Table 1 and Fig. 1 display the AEs reported after vaccination. Reported AEs were more common in recipients of the ChAdOx1 nCoV-19 vaccine than in those given the BNT162b2 vaccine (90.9% vs. 52.5%, P < 0.001). In addition, ChAdOx1 nCoV-19 recipients were 9.5 times more likely to require medication to relieve their AEs compared to BNT162b2 recipients (70.9% vs. 7.5%, P < 0.001). In general, AEs occurred on the day following vaccination and continued for one or two days. Injection-site pain was the most common local adverse reaction (AR) in both vaccination groups (77.7% vs. 51.2%, P < 0.001) and persisted for an average of 3 days (range: 2–4) and 2 days (range: 1–3), respectively. After each vaccination, 36.1% (517/1,431) and 5.0% (4/80) of respective patients reported fever. Fever ≥ 39.0°C was relatively common in the ChAdOx1 nCoV-19 group (12.8% of ChAdOx1 nCoV-19 recipients). No neurologic AEs or anaphylaxis events were observed in either group of vaccine recipients.
Table 1. Local and systemic adverse events following vaccination.
| Variables | ChAdOx1 nCoV-19 vaccine (n = 1,431) | BNT162b2 vaccine (n = 80) | P value | |||
|---|---|---|---|---|---|---|
| All adverse events | 1,301 (90.9) | 42 (52.5) | < 0.001 | |||
| Adverse events requiring medication | 1,015 (70.9) | 6 (7.5) | < 0.001 | |||
| Adverse events requiring hospitalization | 1 (0.1) | 0 (0.0) | > 0.999 | |||
| Local reaction | ||||||
| Pain at the injection site | 1,114 (77.8) | 41 (51.2) | < 0.001 | |||
| Peak grade of recorded symptom | 0.284 | |||||
| Grade 1 | 861 (77.4) | 34 (87.8) | ||||
| Grade 2 | 211 (19.0) | 4 (9.8) | ||||
| Grade 3 | 41 (3.7) | 1 (2.4) | ||||
| Symptom onset | 1 (1–1) | 1 (1–1) | 0.016 | |||
| Duration | 3 (2–4) | 2 (1–3) | 0.014 | |||
| Redness/swelling at the injection site | 352/1,415b (24.9) | 8 (10.0) | 0.002 | |||
| Peak grade of recorded symptoms | 0.553 | |||||
| Grade 1 | 266 (75.6) | 8 (100.0) | ||||
| Grade 2 | 71 (20.2) | 0 (0.0) | ||||
| Grade 3 | 14 (4.0) | 0 (0.0) | ||||
| Grade 4 | 1 (0.3) | 0 (0.0) | ||||
| Symptom onset | 2 (1–3) | 1 (1–1) | 0.019 | |||
| Duration | 2 (1–3) | 2 (2–2.75) | 0.272 | |||
| Lymphadenopathy | 14 (1.0) | 0 (0.0) | > 0.999 | |||
| Symptom onset | 2 (1–3.5) | NA | ||||
| Duration | 1 (1–1) | NA | ||||
| Systemic events | ||||||
| Fever | 517 (36.1) | 4 (5.0) | < 0.001 | |||
| Peak grade of recorded symptom (°C) (mean ± SD) | 38.3 ± 0.6 | 37.6a | 0.754 | |||
| Grade 1 (37.5–38.4) | 334 (64.6) | 4 (100.0) | ||||
| Grade 2 (38.5–38.9) | 117 (22.6) | 0 (0.0) | ||||
| Grade 3 (39.0–40.0) | 65 (12.6) | 0 (0.0) | ||||
| Grade 4 (> 40.0) | 1 (0.2) | 0 (0.0) | ||||
| Symptom onset | 1 (1–2) | 1 (1–1) | 0.232 | |||
| Duration | 1 (1–2) | 1 (1–1.75) | 0.731 | |||
| Chills | 589 (41.2) | 1 (1.2) | < 0.001 | |||
| Symptom onset | 1 (1–1) | 1 | 0.581 | |||
| Duration | 1 (1–2) | 1 | 0.460 | |||
| Fatigue | 726 (50.7) | 6 (7.5) | < 0.001 | |||
| Symptom onset | 1 (1–2) | 1 (1–1.25) | 0.411 | |||
| Duration | 2 (1–2) | 2 (1.74–2.5) | 0.279 | |||
| Nausea | 327/1,411b (23.2) | 1 (1.2) | < 0.001 | |||
| Vomiting | 53/1,411b (3.8) | 2 (2.5) | 0.765 | |||
| Peak grade of recorded symptom | 0.617 | |||||
| Grade 0 | 209 (62.0) | 1 (50.0) | ||||
| Grade 1 | 95 (28.2) | 1 (50.0) | ||||
| Grade 2 | 28 (8.4) | 0 (0.0) | ||||
| Grade 3 | 4 (1.2) | 0 (0.0) | ||||
| Grade 4 | 1 (0.3) | 0 (0.0) | ||||
| Symptom onset | 1 (1–2) | 1,1 | 0.332 | |||
| Duration | 1 (1–2) | 2,3 | 0.043 | |||
| Headache | 678 (47.4) | 6 (7.5) | < 0.001 | |||
| Symptom onset | 1 (1–2) | 1 (1–2.5) | 0.631 | |||
| Duration | 2 (1–2) | 2 (1–2.25) | 0.515 | |||
| Myalgia | 866 (60.5) | 9 (11.2) | < 0.001 | |||
| Symptom onset | 1 (1–1) | 1 (1–2) | 0.233 | |||
| Duration | 1 (1–2) | 2 (1–2) | 0.909 | |||
| Arthralgia | 381 (26.6) | 0 (0.0) | < 0.001 | |||
| Symptom onset | 1 (1–2) | |||||
| Duration | 1 (1–2) | |||||
| Urticaria | 42 (2.9) | 0 (0.0) | 0.166 | |||
| Symptom onset | 1 (1–2) | |||||
| Duration | 1 (1–1) | |||||
Data represent the number (%) of patients or the median value of days (interquartile range) unless otherwise specified.
aRecorded fever in all four recipients was ≥ 37.6°C; bThere were 16 and 20 missing data or non-response instances for redness/swelling at the injection site and nausea/vomiting, respectively.
Fig. 1. Incidence of reported adverse events in each vaccine group.

AEs = adverse events.
**P < 0.005.
In the ChAdOx1 nCoV-19 group, age and sex relationship were observed between patients with AEs (mean age: 35.2 years; 85.3% of male and 93.0% of female) and without AEs (mean age: 42.3 years; 14.7% of male and 7.0% of female) (both P < 0.001) (Supplementary Table 4). Local and systemic AEs tended to be more frequently reported by young HCWs who received the ChAdOx1 nCoV-19 vaccine (Fig. 2A and Supplementary Table 5). Fever was more frequently reported in young HCWs, which showed a four-fold higher incidence in those aged 20–29 compared to those aged ≥ 50 (48.4% vs. 12.2%; Fig. 2A and Supplementary Table 5). However, the AE of fever showed early onset and rapid resolution; no HCWs reported fever six days after vaccination (Fig. 2B and Supplementary Table 6). Among recipients of the ChAdOx1 nCoV-19 vaccine, there was only one case of hospitalization due to AEs, which was defined as a serious AE by the Uppsala Monitoring Center. A 23-year-old female had fever, general myalgia, and nausea/vomiting on the first day following vaccination. Because of dehydration due to vomiting, she admitted to our hospital five days after the vaccination. She recovered completely after receiving hydration and supportive care.
Fig. 2. Proportions of reported adverse events in ChAdOx1 nCoV-19 vaccine recipients stratified by age (A). Positive responses rates of each adverse events in ChAdOx1 nCoV-19 vaccine recipients on post-vaccination days 0–7 (B).

*P < 0.05; **P < 0.005.
Different vaccine platforms including mRNA, adenoviral vector, inactivated virus vector, and adjuvant have been anticipated to produce different reactogenicities according to platform.2 ChAdOx1 nCoV-19 is a replication-deficient simian adenovirus-vectored vaccine, while BNT162b2 is a lipid nanoparticle–formulated, nucleoside-modified RNA (modRNA) vaccine.2 Our study showed that there was a much higher incidence of mild-to-moderate AEs in recipients of the ChAdOx1 than in those with BNT162b2, and ChAdOx1 nCoV-19 recipients were 9.5 times as likely to require medication to relieve their AEs compared to BNT162b2 recipients. This finding is in line with the report that there were numerically more incidences of AEs in recipients of the ChAdOx1 nCoV-19 vaccine compared with those who received the BNT162b2 vaccine.3,4,6,7,8,10 A phase 2/3 trial of ChAdOx1 nCoV-19 showed that ARs were more common in participants given the ChAdOx1 nCoV-19 vaccine than in the MenACWY vaccine group; at least one local symptom was reported by 88.0% of vaccine recipients from 18–55 years of age, and at least one systemic symptom was present in 86.0% of recipients from 18–55 years after the first ChAdOx1 nCoV-19 vaccination.7 Within 7 days after the first vaccination with ChAdOx1 nCoV-19, the incidence of objectively measured fever was 24% of vaccine recipients from 18-55 years of age.7 In contrast, the result from the safety monitoring system in U.S (V-safe) showed that injection site pain (72.9%), fatigue (21.9%), headache (17.5%), and myalgia (14.7%) were most frequently reported in the BNT162b2 recipients.10 Only 5.8% of BNT162b2 recipients showed fever.10 ARs were less common in older than in younger adults in both ChAdOx1 nCoV-19 and BNT162b2 recipients.4,7
Consistent with prior data, our study indicated that there was similar incidence of mild-to-moderate AEs of the ChAdOx1 vaccine, and young HCWs reported more than their older counterparts. Although it seemed that more ChAdOx1 recipients in our study reported fever, the incidence decreased from 36.1% to 23.9% when fever was defined as temperature ≥ 38.0°C instead of ≥ 37.5°C. Although more ChAdOx1 nCoV-19 recipients required medications to relieve their AEs compared to BNT162b2 recipients in our study, most of the reported local and systemic AEs were mild to moderate in severity and continued for only one or two days. Recently, there has been concern about an association between the ChAdOx1 vaccine and occurrence of blood clots. The Committee of the European Medicines Agency has confirmed that the ChAdOx1 vaccine is not associated with an increase in thromboembolic events, however, they concluded that the ChAdOx1 vaccine may be associated with disseminated intravascular coagulation or cerebral venous sinus thrombosis.12 Prior to vaccination, sufficient explanations of the expected AEs of the vaccine as well as the overall vaccine safety should be given. Preparing hospital guidelines and medications for symptom relief using data from a real clinical setting might decrease fear and confusion both before and after vaccination and serve to promote wider vaccination. A phase 1/2 clinical trial of ChAdOx1 showed that prophylactic use of acetaminophen with vaccination could increase tolerability to AEs.6 Intriguingly, fewer AEs were reported after the second vaccination than after the first in the phase 2/3 trial of ChAdOx1 nCoV-19.7 In contrast, reactogenicity was more common and severe after the second dose than after the first dose in the phase 2/3 trial of BNT162b2, although local reactogenicity was similar after the two doses.4 Additional evidence is required to determine whether the frequency or severity of AEs differs between vaccinations.
Our study had several limitations. First, a small number of HCWs received the BNT162b2 vaccination, so AEs for BNT162b2 could not be sufficiently described. Second, self-report symptoms are subjective rather than objective. However, this study participants were largely health care workers, and therefore self-report data reliability may be high. Third, we did not collect information on AEs that occurred more than seven days after the vaccination and could have missed important events. Finally, there were unresponded data to be able to cause bias; however, our overall response rate exceeded 90%. Our study response rate was higher than those reported by prior clinical studies. Despite these limitations, this study was significant in evaluating and comparing the AEs of HCWs who received ChAdOx1 nCoV-19 or BNT162b2 vaccination in a real clinical setting.
In conclusion, the incidence of AEs was a much higher in recipients with the ChAdOx1 nCoV-19 vaccine than in those with the BNT162b2 vaccine. However, most of the reported AEs were mild to moderate in severity and continued for only one or two days. Because of the speed of COVID-19 vaccine development and deployment, there have been concerns among the public about the safety of COVID-19 vaccines. Sufficient explanation and preparation for expected AEs before and after vaccination remain vital to relieve unnecessary fear and promote vaccination.
Footnotes
Disclosure: The authors have no potential conflicts of interest to declare.
- Conceptualization: Peck KR.
- Data curation: Yun SY, Ryu JS.
- Formal analysis: Kim SH.
- Investigation: Lee EH, Seo KH, Lee SH.
- Methodology: Kim SH, Wi YM.
- Software: Kim SH.
- Validation: Kim SH, Wi YM.
- Writing - original draft: Kim SH, Wi YM, Peck KR.
- Writing - review & editing: Kim SH, Wi YM, Yun SY, Ryu JS, Shin JM, Lee EH, Seo KH, Lee SH, Peck KR.
SUPPLEMENTARY MATERIALS
Hospital guidelines for managing adverse events after vaccination
Clinical characteristics of vaccine recipients
The response rate on each postvaccination day
Clinical characteristics of vaccine recipients with adverse events
Proportions of reported adverse events of ChAdOx1 nCoV-19 vaccine recipients stratified by age
Positive responses rate of each adverse events of ChAdOx1 nCoV-19 vaccine recipients on post-vaccination day 0–7
References
- 1.World Health Organization. WHO coronavirus (COVID-19) dashboard. [Updated 2021]. [Accessed March 21, 2021]. https://covid19.who.int.
- 2.Krammer F. SARS-CoV-2 vaccines in development. Nature. 2020;586(7830):516–527. doi: 10.1038/s41586-020-2798-3. [DOI] [PubMed] [Google Scholar]
- 3.Walsh EE, Frenck RW, Jr, Falsey AR, Kitchin N, Absalon J, Gurtman A, et al. Safety and immunogenicity of two RNA-based Covid-19 vaccine candidates. N Engl J Med. 2020;383(25):2439–2450. doi: 10.1056/NEJMoa2027906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Polack FP, Thomas SJ, Kitchin N, Absalon J, Gurtman A, Lockhart S, et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N Engl J Med. 2020;383(27):2603–2615. doi: 10.1056/NEJMoa2034577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Dagan N, Barda N, Kepten E, Miron O, Perchik S, Katz MA, et al. BNT162b2 mRNA Covid-19 vaccine in a nationwide mass vaccination setting. N Engl J Med. 2021:NEJMoa2101765. doi: 10.1056/NEJMoa2101765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Folegatti PM, Ewer KJ, Aley PK, Angus B, Becker S, Belij-Rammerstorfer S, et al. Safety and immunogenicity of the ChAdOx1 nCoV-19 vaccine against SARS-CoV-2: a preliminary report of a phase 1/2, single-blind, randomised controlled trial. Lancet. 2020;396(10249):467–478. doi: 10.1016/S0140-6736(20)31604-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ramasamy MN, Minassian AM, Ewer KJ, Flaxman AL, Folegatti PM, Owens DR, et al. Safety and immunogenicity of ChAdOx1 nCoV-19 vaccine administered in a prime-boost regimen in young and old adults (COV002): a single-blind, randomised, controlled, phase 2/3 trial. Lancet. 2021;396(10267):1979–1993. doi: 10.1016/S0140-6736(20)32466-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Voysey M, Clemens SA, Madhi SA, Weckx LY, Folegatti PM, Aley PK, et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: an interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet. 2021;397(10269):99–111. doi: 10.1016/S0140-6736(20)32661-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Voysey M, Costa Clemens SA, Madhi SA, Weckx LY, Folegatti PM, Aley PK, et al. Single-dose administration and the influence of the timing of the booster dose on immunogenicity and efficacy of ChAdOx1 nCoV-19 (AZD1222) vaccine: a pooled analysis of four randomised trials. Lancet. 2021;397(10277):881–891. doi: 10.1016/S0140-6736(21)00432-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Gee J, Marquez P, Su J, Calvert GM, Liu R, Myers T, et al. First month of COVID-19 vaccine safety monitoring - United States, December 14, 2020-January 13, 2021. MMWR Morb Mortal Wkly Rep. 2021;70(8):283–288. doi: 10.15585/mmwr.mm7008e3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.The COVID-19 Vaccination Response Promotion Team. Adverse Event Management Guidelines after Coronavirus Disease 19 Vaccination. Cheongju: Korea Centers for Disease Control and Prevention; 2021. p. 90. [Google Scholar]
- 12.European Medicines Agency. [Updated 2021]. [Accessed April 18, 2021]. https://www.ema.europa.eu.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Hospital guidelines for managing adverse events after vaccination
Clinical characteristics of vaccine recipients
The response rate on each postvaccination day
Clinical characteristics of vaccine recipients with adverse events
Proportions of reported adverse events of ChAdOx1 nCoV-19 vaccine recipients stratified by age
Positive responses rate of each adverse events of ChAdOx1 nCoV-19 vaccine recipients on post-vaccination day 0–7