

Abstract
Background:
Although randomized controlled trials (RCTs) have demonstrated that high fluoride increases bone mineral density (BMD) and skeletal fragility, observational studies of low-dose chronic exposure through drinking water (, the maximum recommended by the World Health Organization) have been inconclusive.
Objective:
We assessed associations of fluoride in urine, and intake via diet and drinking water, with BMD and fracture incidence in postmenopausal women exposed to drinking water fluoride .
Methods:
Data were from participants in the Swedish Mammography Cohort–Clinical, a population-based prospective cohort study. At baseline (2004–2009), fluoride exposure was assessed based on urine concentrations () and estimated dietary intake (including drinking water) (), and BMD was measured using dual energy X-ray absorptiometry. Incident fractures were ascertained via register-linkage through 2017. Residential history was collected to identify women with long-term consistent drinking water exposures prior to baseline.
Results:
At baseline, mean urine fluoride was creatinine () and mean dietary intake was (), respectively. During follow-up, 850, 529, and 187 cases of any fractures, osteoporotic fractures, and hip fractures, respectively, were ascertained. Baseline BMD was slightly higher among women in the highest vs. lowest tertiles of exposure. Fluoride exposures were positively associated with incident hip fractures, with multivariable-adjusted hazard ratios of 1.50 (95% CI: 1.04, 2.17) and 1.59 (95% CI: 1.10, 2.30), for the highest vs. lowest tertiles of urine fluoride and dietary fluoride, respectively. Associations with other fractures were less pronounced for urine fluoride, and null for dietary fluoride. Restricting the analyses to women with consistent long-term drinking water exposures prior to baseline strengthened associations between fractures and urinary fluoride.
Discussion:
In this cohort of postmenopausal women, the risk of fractures was increased in association with two separate indicators of fluoride exposure. Our findings are consistent with RCTs and suggest that high consumption of drinking water with a fluoride concentration of may increase both BMD and skeletal fragility in older women. https://doi.org/10.1289/EHP7404
Introduction
Exposure to fluoride occurs mainly through drinking water, which may include fluoride from natural sources and fluoride added to prevent tooth decay. Naturally occurring fluoride concentrations can vary substantially, from insignificant to well above the World Health Organization (WHO)-recommended limit of (WHO 2006), whereas the concentration in artificially fluoridated water is typically around (U.S. Department of Health and Human Services Federal Panel on Community Water Fluoridation 2015). Although low levels of fluoride are beneficial for oral health, the therapeutic range is narrow, and it is well established that individuals living in areas with high naturally occurring fluoride have an increased risk of dental and skeletal fluorosis (the former a result of early life exposure) (NRC 2006). Because of its ability to induce bone formation (Farley et al. 1983), the antifracture effect of fluoride was extensively studied in randomized controlled trials (RCTs) in the early 1990s. However, although high-dose fluoride therapy increased bone mineral density (BMD), it had no effect on the overall vertebral fracture rate, and it increased the risk of nonvertebral fractures (Haguenauer et al. 2000; Riggs et al. 1990).
A number of observational studies have assessed the association of chronic low-to-moderate exposure to fluoride, mainly via drinking water, with bone health. Although some reports suggest that fluoride may increase susceptibility to fractures (Danielson et al. 1992; Jacobsen et al. 1992; Kurttio et al. 1999; Li et al. 2001; Sowers et al. 1991), others have reported no association (Cauley et al. 1995; Feskanich et al. 1998; Hillier et al. 2000; Karagas et al. 1996; Näsman et al. 2013; Sowers et al. 2005) or evidence of a protective association (Lehmann et al. 1998; Phipps et al. 2000; Simonen and Laitinen 1985). Authors of a systematic review and meta-analysis published in 2015 concluded that chronic exposure to fluoride in drinking water was not associated with a significant increase in hip fracture risk (Yin et al. 2015). However, most of the data included in the analysis were from ecological studies with potential biases due to exposure misclassification and insufficient control of confounding.
The aim of the present study was to examine associations of urinary fluoride, and individual-level estimates of fluoride intake through drinking water and diet, with baseline BMD and fracture incidence in a population-based prospective cohort of postmenopausal women living in an area where municipal drinking water natural fluoride concentrations ranged from 0 to .
Materials and Methods
Study Population
The Swedish Mammography Cohort (SMC) is a population-based prospective cohort, part of the Swedish Infrastructure for Medical Population-based Life-course and Environmental Research (SIMPLER; www.simpler4health.se). The cohort was established in 1987–1990 when all female residents of two counties who were born in 1914–1948 were sent a diet and lifestyle questionnaire and invited to participate in the study (, response rate 74%). An additional questionnaire was sent out in 1997 to update information on diet and lifestyle (response rate 70%). A detailed description of the SMC is provided elsewhere (Harris et al. 2013).
The present study is based in a clinical subcohort [SMC–Clinical (SMC-C)] that was established in 2003–2009 when all SMC participants who were of age and residing in the city of Uppsala or nearby surrounding areas were invited to a health examination. The women provided blood and urine samples, underwent a bone density scan, and answered a questionnaire on diet, drinking water consumption, and lifestyle factors. Of 8,311 eligible women, 65% completed the questionnaire, 61% participated in the health examination, 5,022 had bone scans, and 4,480 provided urine samples for element analysis. The present analysis includes data from 4,306 women with urine fluoride and creatinine measurements and bone scans of all skeletal sites investigated and who were enrolled from 2004 and onward (Figure 1). Written informed consent was obtained from all study participants, and the study was approved by the Regional Ethical Review Board in Stockholm, Sweden.
Figure 1.
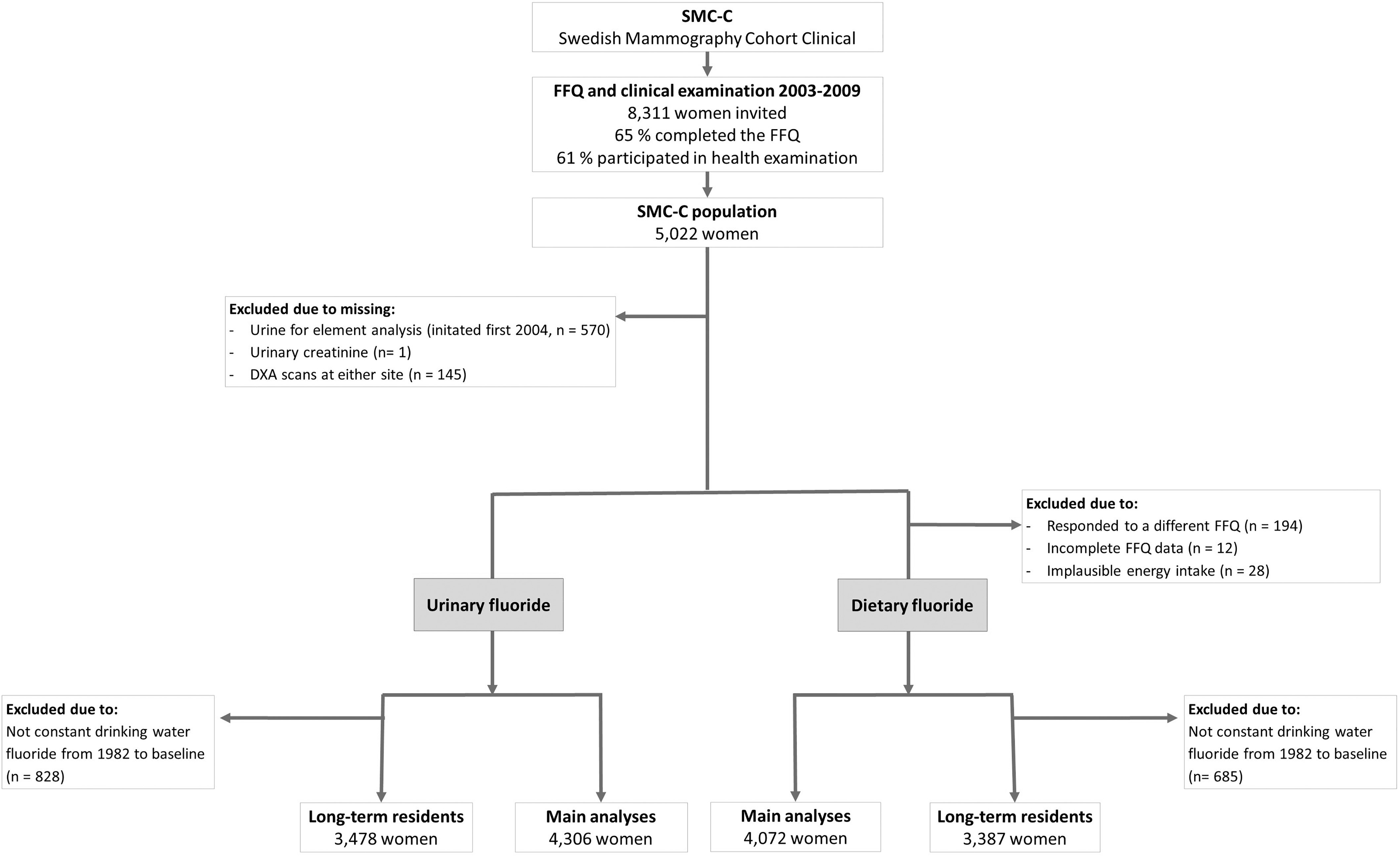
Flow chart of eligible participants in the study. Note: DXA, dual energy X-ray absorptiometry; FFQ, food frequency questionnaire; SMC-C, Swedish Mammography Cohort–Clinical.
Fluoride Exposure Assessment and Covariates
Assessment of fluoride biomarker.
Fluoride anions were measured in the first voided urine using an ion-selective electrode (Combined ISE F 800 DIN; WTW; Xylem Analytics Germany GmbH). Prior to analysis, a total ionic strength adjustment buffer was added 1:1 (WTW, Xylem Analytics Germany GmbH) to all samples, including standard solutions. The instrument was calibrated using a set of standard solutions (0.01, 0.1, 1.0, and ) that was prepared fresh each day from a sodium fluoride stock solution (; WTW; Xylem Analytics Germany GmbH). The fluoride concentration of a commercial reference material (Seronorm Trace Elements Urine, Ref. 201205, Lot: NO2525; Sero AS) was measured for quality control, and the agreement between the reference value ( fluoride/L) and the obtained value ( fluoride/L) was good. The coefficient of variation (CV) was 7% based on two samples, each measured 50 times during the analytical period. Urine fluoride concentrations were adjusted to the creatinine concentration in each sample to account for variation in urine dilution (in milligrams fluoride per gram creatinine).
Assessment of dietary fluoride.
We used the Swedish National Food Agency’s database (https://www.livsmedelsverket.se/en) and, in cases of missing information, the U.S. Department of Agriculture’s National Fluoride Database of Selected Beverages and Foods (USDA 2005) to estimate the fluoride content of individual foods and beverages. For fluoride levels in tea (assumed to be a major source), additional data were extracted from scientific articles (Malinowska et al. 2008). Tap water fluoride concentrations (stable over decades) were obtained from Vattentäktsarkivet, Geological Survey of Sweden, and the Swedish Water and Wastewater Association and were used to categorize each residence into one of four groups based on average tap water fluoride concentrations of 0, 0.3, 0.5, or fluoride/L, respectively. The average for each participant’s group was used to estimate the contribution of fluoride in tap water to the fluoride content of meals and beverages prepared with tap water. Intake frequencies of individual foods (classified into eight predefined consumption categories) and beverages (according to the exact number of glasses or cups consumed daily or weekly) were derived from a semi-quantitative 124-item food frequency questionnaire (FFQ) concerning habitual food and beverage consumption during the past year. A description of the FFQ and validation is described elsewhere (Harris et al. 2013). Total fluoride intake from diet and drinking water at baseline was estimated for each participant by multiplying the intake of each food and beverage item consumed by its estimated fluoride content. Finally, estimated intakes were adjusted for total energy intake using the residual method (Willett and Stampfer 1986). A total of 234 women were excluded from analyses of dietary fluoride, including 194 who completed a short version of the FFQ, 12 with incomplete FFQ data, and 28 with implausible energy intakes ( above or below the log-transformed mean) (Figure 1).
To identify women with approximately consistent long-term drinking water fluoride exposures prior to baseline, we obtained data on annual residential history for each participant. We considered exposure to be constant if the participants remained within the same area or an area with the same drinking water fluoride concentration from 1982 (the first year data was available from) to baseline (2004–2009).
Assessment of covariates.
Self-reported information on use of postmenopausal hormones, physical activity, smoking status, alcohol consumption, use of vitamin D and calcium supplements, and dietary intake of calcium was obtained from the SMC-C questionnaire completed at baseline (2004–2009), and information about educational level, parity, and ever use of corticosteroids was obtained from the previous SMC questionnaire (in 1997). Information about lean body mass and fat mass was derived from the bone scan (see the section “Outcome Assessment”) at the SMC-C clinical examination and attained height was measured at the same visit. Urinary calcium excretion was assessed using inductively coupled plasma mass spectrometry (ICP-MS 7700ce; Agilent Technologies) and expressed as milligrams per gram creatinine. The estimated glomerular filtration rate (eGFR) was derived from plasma creatinine and cystatin C using the combined creatinine-cystatin C Chronic Kidney Disease Epidemiology Collaboration equation (Inker et al. 2012). Beta-CrossLaps, a marker of bone resorption, was measured in plasma using routine methods (Roche Cobas 8000) at the Department of Clinical Chemistry and Pharmacology (Uppsala University Hospital). The CV for Beta-CrossLaps was 1.8% at and 1.4% at . Information on prevalent diabetes (both type I and type II) was based on self-report (through answer to the question “have you been diagnosed with diabetes?” in the 1997 and 2004–2009 questionnaires) and on linkage to the Swedish National Board of Health and Welfare’s National Patient Register (NPR) and the Swedish National Diabetes Register.
Outcome Assessment
At the clinical examination at baseline, BMD (in grams per centimeter squared) was measured at the lumbar spine and femoral neck using dual energy X-ray absorptiometry (DXA; Lunar Prodigy; Lunar Corp.) with a 0.8–1.5% based on triple measurements in 15 participants. Left and right femoral neck measurements were averaged unless a measurement was available for only one side (2%; ).
Incident fractures that occurred after the baseline clinical examination and before the end of follow-up (31 December 2017) were ascertained via linkage to the NPR, which also includes information on fractures that did not result in hospitalization. An evaluation of the NPR showed positive predictive values of 95–98% for hip fractures (Ludvigsson et al. 2011). We evaluated according to the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10; WHO 2016), three outcomes (main diagnosis) related to incident fractures during the follow-up period: a) the first incidence of any fracture (ICD-10 codes S12, S22, S32, S42, S52, S62, S72, S82, and S92); b) the first major osteoporotic fracture [lumbar spine, proximal humerus, distal forearm, and hip (ICD-10 codes S32.0, S42.2, S52.5–S52.6, and S72.0–S72.2)]; and c) the first hip fracture (ICD-10 codes S72.0–S72.2.)
Statistical Analysis
We categorized participants into tertiles of urinary and dietary fluoride exposure at baseline. The correlation between urinary and dietary fluoride was assessed by Spearman’s rank correlation (rho). Cross-sectional associations of fluoride exposure with BMD were investigated by multivariable linear regression. Fracture incidence was assessed by Cox proportional hazard regression analysis with attained age as the underlying time scale. For each fracture-specific analysis, participants contributed to the person-time from the date of the clinical examination until the date of first incident fracture, the date of death, or the end of follow-up (31 December 2017), whichever occurred first. The proportional hazard assumption was tested using Schoenfelds residuals, and no departure from the assumption was observed. Tests for linear trend () across tertiles of exposure were conducted by assigning the median value for each tertile and modeling it as a continuous variable.
Multivariable regression models were adjusted for potential confounders that were selected a priori based on potential associations with fluoride exposure and because they were established or potential risk factors for the outcomes, including the following: age (Kanis et al. 2019) (continuous), education (Crandall et al. 2014) (, 9–12, and ), height (Hemenway et al. 1995) (continuous, in centimeters), total fat mass (Kanis et al. 2019) (continuous, in kilograms), lean body mass (Kanis et al. 2019) (continuous, in kilograms), parity (Wang et al. 2016) (number of children), smoking status (Kanis et al. 2019) (never, former, current , current ), physical activity (Stattin et al. 2017) (walk or bike : yes/no; exercise : yes/no), alcohol intake (Kanis et al. 2019) (, 0.5–15, ), prevalent diabetes at baseline (Kanis et al. 2019) (yes/no), eGFR (Kim et al. 2016) (, , ), urinary calcium (for models of associations with urinary fluoride, in tertiles) or dietary calcium intake (Warensjö et al. 2011) (for associations with dietary fluoride, in tertiles), use of calcium supplements (Weaver et al. 2016) (yes/no), use of vitamin D supplements (Weaver et al. 2016) (yes/no), ever use of postmenopausal hormones (Kanis et al. 2019) (yes/no), and ever use of corticosteroids (Kanis et al. 2019) (yes/no). Means presented in Table 1 were age-standardized, according to seven quantiles of age at baseline, to visualize nonage related differences in covariates across exposure categories.
Table 1.
Baseline age-standardized main characteristics of 4,306 women from the Swedish mammography cohort by tertiles of urinary fluoride (; mg/g creatinine) and by dietary fluoride ( mg/d).
| Characteristics [continuous: mean (), categorical: proportions ()] | Tertiles of urinary fluoride | Tertiles of dietary fluoride | ||||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 1 | 2 | 3 | |
| Fluoride exposure (mg/g creatinine or mg/d) | 0.7 () | 1.1 () | 1.9 () | 1.3 () | 2.1 () | 3.2 () |
| 1,436 | 1,435 | 1,435 | 1,358 | 1,357 | 1,357 | |
| Proportion of women receiving drinking water with fluoride concentration of | 76 | 93 | 94 | 73 | 96 | 98 |
| Drinking water (glasses/d)a | 3.1 () | 3.8 () | 4.2 () | 2.6 () | 3.8 () | 5.3 () |
| Tea (cups/d)a | 0.7 () | 0.9 () | 1.4 () | 0.4 () | 0.8 () | 2.0 () |
| Coffee (cups/d)a | 2.6 () | 2.6 () | 2.5 () | 2.5 () | 2.8 () | 2.8 () |
| Age (y) | 68 () | 67 () | 68 () | 69 () | 67 () | 66 () |
| Education {y [% ()]} | ||||||
| 25 (366) | 24 (338) | 21 (312) | 25 (360) | 24 (322) | 21 (275) | |
| 10–11 | 38 (546) | 38 (539) | 40 (579) | 40 (538) | 39 (525) | 37 (507) |
| 36 (520) | 38 (553) | 38 (542) | 35 (459) | 37 (506) | 41 (570) | |
| Missing | (4) | (5) | (2) | (1) | (4) | (5) |
| Height (cm) | 164 () | 164 () | 163 () | 164 () | 164 () | 164 () |
| Total fat mass (kg) | 28 () | 26 () | 25 () | 27 () | 26 () | 27 () |
| Missing [% ()] | 1 (14) | (7) | 1 (14) | 1 (9) | 1 (11) | 1 (11) |
| Lean body mass (kg) | 40 () | 39 () | 39 () | 39 () | 39 () | 40 () |
| Missing [% ()] | 1 (14) | (7) | 1 (14) | 1 (9) | 1 (11) | 1 (11) |
| Parity ( children) | 2 () | 2 () | 2 () | 2 () | 2 () | 2 () |
| Smoking status [% ()] | ||||||
| Never | 51 (739) | 51 (726) | 51 (728) | 54 (751) | 49 (661) | 51 (675) |
| Former | 35 (498) | 36 (512) | 35 (498) | 33 (428) | 37 (502) | 36 (497) |
| Current | 8 (117) | 8 (116) | 10 (143) | 7 (102) | 8 (118) | 10 (132) |
| Missing | 6 (82) | 6 (81) | 5 (66) | 6 (77) | 6 (76) | 4 (53) |
| Physical activity [% ()] | ||||||
| Walk/bike | 34 (484) | 39 (560) | 42 (602) | 36 (480) | 37 (508) | 42 (579) |
| Walk/bike | 62 (889) | 56 (807) | 54 (773) | 60 (812) | 59 (805) | 53 (723) |
| Walk/bike missing | 4 (63) | 5 (68) | 4 (60) | 5 (66) | 4 (44) | 4 (55) |
| Exercise | 74 (1,065) | 78 (1,120) | 78 (1,119) | 78 (1,058) | 80 (1,081) | 79 (1,079) |
| Exercise | 21 (297) | 17 (245) | 16 (238) | 17 (226) | 16 (218) | 16 (217) |
| Exercise missing | 5 (74) | 5 (70) | 5 (78) | 5 (74) | 3 (58) | 5 (61) |
| Alcohol {g/d [% ()]} | ||||||
| 12 (173) | 13 (183) | 14 (209) | 14 (197) | 13 (181) | 14 (172) | |
| 0.5–15 | 72 (1,028) | 73 (1,055) | 73 (1,043) | 76 (1,027) | 76 (1,037) | 77 (1,048) |
| 9 (132) | 10 (143) | 9 (135) | 10 (134) | 10 (139) | 10 (137) | |
| Missing | 7 (103) | 4 (54) | 3 (49) | 0 (0) | 0 (0) | 0 (0) |
| Prevalent diabetes [% ()] | ||||||
| Yes | 7 (95) | 4 (60) | 6 (92) | 5 (1,286) | 7 (1,268) | 5 (1,289) |
| No | 93 (1,341) | 96 (1,375) | 94 (1,343) | 95 (72) | 93 (89) | 95 (68) |
| eGFR { [% ()]}b | ||||||
| 87 (1,259) | 90 (1,305) | 90 (1,291) | 89 (1,187) | 90 (1,214) | 89 (1,227) | |
| 59–30 | 12 (166) | 9 (127) | 9 (141) | 10 (151) | 10 (130) | 10 (119) |
| 1 (11) | (3) | (3) | 1 (10) | 1 (2) | 1 (4) | |
| Missing | 1 (9) | 1 (9) | 1 (10) | 1 (10) | 1 (11) | 1 (7) |
| Urinary calcium (mg/g creatinine) | 148 () | 160 () | 193 () | 160 () | 165 () | 165 () |
| Dietary calcium (mg/d) | 1,085 () | 1,088 () | 1,099 () | 1,065 () | 1,095 () | 1,113 () |
| Missing [% ()] | 8 (115) | 4 (62) | 4 (58) | (1) | 0 (0) | 0 (0) |
| Calcium supplement use [% ()] | ||||||
| Yes | 12 (175) | 14 (203) | 18 (251) | 14 (200) | 14 (191) | 18 (238) |
| No | 60 (861) | 60 (871) | 57 (812) | 62 (829) | 63 (863) | 61 (837) |
| Missingc | 28 (400) | 25 (361) | 26 (372) | 23 (329) | 22 (303) | 21 (282) |
| Vitamin D supplement use [% ()] | ||||||
| Yes | 7 (100) | 8 (113) | 11 (152) | 9 (123) | 8 (111) | 10 (131) |
| No | 67 (958) | 67 (958) | 65 (931) | 68 (917) | 70 (957) | 69 (958) |
| Missingc | 26 (378) | 25 (364) | 24 (352) | 23 (318) | 21 (289) | 21 (268) |
| Ever use of postmenopausal oral estrogen [% ()] | ||||||
| Yes | 58 (838) | 63 (906) | 64 (914) | 59 (792) | 64 (866) | 63 (868) |
| No | 39 (565) | 35 (497) | 34 (487) | 38 (528) | 34 (462) | 35 (463) |
| Missingc | 2 (33) | 2 (32) | 2 (34) | 3 (38) | 3 (29) | 2 (26) |
| Ever use of corticosteroids [% ()] | ||||||
| Yes | 11 (160) | 12 (178) | 16 (227) | 12 (160) | 13 (173) | 14 (192) |
| No | 77 (1,109) | 74 (1,066) | 72 (1,031) | 75 (1,019) | 76 (1,026) | 73 (998) |
| Missingc | 12 (167) | 13 (191) | 12 (177) | 13 (179) | 12 (158) | 12 (167) |
| Serum Beta-CrossLaps (ng/L) | 441 () | 467 () | 492 () | 461 () | 466 () | 465 () |
| Missing [% ()] | (6) | (8) | (7) | 1 (7) | 1 (8) | (6) |
| BMD () | ||||||
| Spine | 1.13 () | 1.12 () | 1.11 () | 1.11 () | 1.12 () | 1.13 () |
| Femoral neck | 0.87 () | 0.87 () | 0.86 () | 0.86 () | 0.87 () | 0.87 () |
Note: Continuous variables are presented as means () and categorical as proportions (). Means and proportions were age-standardized, according to seven quantiles of age at baseline. Data were complete for all observations unless otherwise indicated. BMD, bone mineral density; eGFR, estimated glomerular filtration rate; SD, standard deviation.
The predefined volumes indicated in the questionnaire were for water and for coffee and tea.
eGFR was assessed using the combined creatinine-cystatin C Chronic Kidney Disease Epidemiology Collaboration equation.
Nonresponse was interpreted as no use in the analyses because of how the questionnaire was structured.
Because fluoride is stored primarily in bone and is released when bone is resorbed, bone resorption is a potential cause of both increased urinary fluoride and bone degradation. Therefore, we additionally adjusted for Beta-CrossLaps, a biochemical marker of bone resorption (Vasikaran et al. 2011), when estimating associations with urine fluoride concentrations. Fluoride is not known to impact osteoclasts [existing evidence is inconclusive; NRC (2006)]; therefore, bone resorption is unlikely to mediate associations between urine fluoride and BMD or incident fractures. Because of the structure of the study questionnaire, nonresponse was interpreted as no use. Accordingly, participants with missing data for use of vitamin D and calcium supplements (25% and 26%, respectively) were classified as nonusers in the analyses. Similarly, participants with missing data for corticosteroids (12%) and postmenopausal hormone use () were also classified as nonusers. For all other covariates, missing data ( of values across the cohort) was handled by multiple imputation using a chained equation technique with 9 predictors and 20 imputations.
In addition to the main analyses, we performed several sensitivity analyses. We repeated analyses after restricting the population to women who had consistent long-term drinking water fluoride exposures from 1982 to baseline to assess the potential influence of long-term exposures. Given RCT evidence that fluoride may not influence vertebral fractures (Riggs et al. 1990), we repeated the analyses of major osteoporotic fractures after excluding them from the outcome. To assess the hypothesis that deleterious skeletal effects of fluoride are primarily related to bone quality and not bone quantity, we adjusted prospective multivariable models for baseline BMD. In addition, we repeated the analyses of BMD and incident fractures that included women with missing hip or spine BMD data and the analyses of urinary fluoride that were restricted to women with complete dietary fluoride data () and that excluded women with unrealistic urinary creatinine values (creatinine and , ). The software used for statistical analysis was STATA/SE (version 14.0; Stata Corporation, Inc.). All tests were two sided with the level of significance set at 0.05.
Results
Mean urinary fluoride at baseline was creatinine (5th–95th percentiles: creatinine) and mean estimated dietary fluoride intake was (5th–95th percentiles: ). Tap water consumption (as drinking water) accounted for the largest proportion of estimated exposure, followed by coffee and tea (brewed with tap water). Together, these sources accounted for 78% of the total estimated dietary fluoride intake for the cohort (Figure 2). The average number of servings of drinking water, tea, and coffee consumed by women in the highest tertile of dietary fluoride were 5.3 (), 2.0 (), and 2.8 (), respectively (Table 1). Urinary and dietary fluoride were moderately correlated (). There were no major differences in the baseline age-standardized distributions of covariates across tertiles of urinary and dietary fluoride apart from a higher proportion of ever users of calcium and vitamin D supplements as well as corticosteroids among the women in the highest tertile of urinary fluoride compared with lowest tertile (Table 1).
Figure 2.

Major sources of dietary fluoride intake estimated for 4,072 women of the Swedish Mammography Cohort–Clinical. Tap water refers to tap water consumed as drinking water and coffee and tea brewed with tap water.
In the cross-sectional assessment, we estimated exposure-dependent associations of urinary and dietary fluoride with increased BMD at both the lumbar spine and femoral neck, with the most pronounced association with BMD being at the spine ( ; Table 2). The estimated multivariable mean difference in BMD, comparing the highest with the lowest tertiles of urinary fluoride, was [95% confidence interval (CI): 0.000, ], and (95% CI: 0.001, ) at the lumbar spine and femoral neck, respectively. The corresponding associations for dietary fluoride were (95% CI: 0.004, ) and (95% CI: 0.000, ), respectively (Table 2). Restricting the analysis to women with approximately constant long-term drinking water fluoride prior to baseline ( and 3,387 for models of urine and dietary fluoride, respectively) yielded almost identical results (Table S1).
Table 2.
Cross-sectional mean differences in BMD [ coefficients (95% CI), ] across tertiles of urinary fluoride (mg/g creatinine) () and dietary fluoride (mg/d) () with BMD at the lumbar spine and femoral neck.
| Categories | Tertiles of urinary fluoride | Tertiles of dietary fluoride | ||||||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 1 | 2 | 3 | |||
| 1,436 | 1,435 | 1,435 | 1,358 | 1,357 | 1,357 | |||
| Fluoride exposure {mg/g creatinine or mg/d [median (range)]} | 0.68 (0.14–0.88) | 1.08 (0.88–1.30) | 1.64 (1.30–116.51) | 1.38 (0.26–1.74) | 2.04 (1.74–2.41) | 2.94 (2.41–11.16) | ||
| Lumbar spine | ||||||||
| Age-adjusted (95% CI) | Ref | (, 0.001) | (, ) | Ref | 0.003 (, 0.018) | 0.019 (0.004, 0.033) | ||
| Multivariable-adjusted (95% CI)a | Ref | 0.007 (, 0.020) | 0.013 (0.000, 0.027) | 0.05 | Ref | 0.005 (, 0.019) | 0.017 (0.004, 0.031) | 0.01 |
| Femoral neck | ||||||||
| Age-adjusted (95% CI) | Ref | (, 0.005) | (, ) | Ref | 0.006 (, 0.014) | 0.010 (0.001, 0.018) | ||
| Multivariable-adjusted (95% CI)a | Ref | 0.007 (, 0.015) | 0.009 (0.001, 0.016) | 0.04 | Ref | 0.007 (, 0.015) | 0.008 (0.000, 0.017) | 0.05 |
Note: The total number of participants in the urinary fluoride and dietary fluoride analyses were 4,306 and 4,072, respectively. Two hundred thirty-four women were excluded from the dietary fluoride analyses because of missing dietary fluoride information due either to responding to a shorter version of the FFQ or having missing/inadequate reported dietary intake (energy intake outside 3 SD of the log-transformed mean). BMD, bone mineral density (); CI, confidence interval; eGFR, estimated glomerular filtration rate; FFQ, food frequency questionnaire; Ref, reference; SD, standard deviation.
Multivariable-adjusted models were adjusted for age, education, height, total fat mass, lean body mass, parity, smoking status, physical activity, alcohol intake, diabetes, eGFR, tertiles of urinary excretion of calcium (for urinary fluoride) or tertiles of dietary intake of calcium (for dietary fluoride), use of calcium supplements, use of vitamin D supplements, ever use of estrogen, and ever use of corticosteroids. Urinary fluoride models were additionally adjusted for serum Beta-CrossLaps (ng/L).
During an average of 9.3 y of follow-up (40,200 person-years), 850 incident cases of any first fracture, 529 incident cases of the first major osteoporotic fracture, and 187 incident cases of first hip fractures were ascertained. The corresponding number of fractures in the analyses of dietary fluoride were 799, 498, and 174, respectively. The risk of any fracture was not associated with dietary fluoride intake, whereas urinary fluoride was associated with a nonsignificant increase in risk for the highest tertile relative to the lowest [adjusted (95% CI: 0.95, 1.34), 0.11] (Table 3). Both urinary and dietary fluoride were associated with hip fractures, with multivariable-adjusted HRs for the highest vs. lowest tertiles of 1.50 [(95% CI: 1.04, 2.17), 0.02] and 1.59 [(95% CI: 1.10, 2.30), 0.01], respectively. Corresponding estimates for major osteoporotic fractures were (95% CI: 0.98, 1.50) and 1.11 (95% CI: 0.89, 1.38) for urinary and dietary fluoride, respectively. When restricted to women with approximately constant long-term drinking water fluoride from 1982 to baseline, HRs for urinary fluoride increased slightly for all outcomes (Table 4). Associations with dietary fluoride remained null for all fractures and for major osteoporotic fractures, whereas the positive association with hip fractures was attenuated [adjusted HR for the third vs. first 1.40 (95% CI: 0.94, 2.09), ]. (Table 4).
Table 3.
Hazard ratios of total, osteoporotic, and hip fractures and corresponding 95% CIs by tertiles of urinary fluoride (mg/g creatinine) () and dietary fluoride (mg/d) (), respectively.
| Categories | Tertiles of urinary fluoride | Tertiles of dietary fluoride | ||||||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 1 | 2 | 3 | |||
| 1,436 | 1,435 | 1,435 | 1,358 | 1,357 | 1,357 | |||
| Fluoride exposure {mg/g creatinine or mg/d [median (range)]} | 0.68 (0.14–0.88) | 1.08 (0.88–1.30) | 1.64 (1.30–116.51) | 1.38 (0.26–1.74) | 2.04 (1.74–2.41) | 2.94 (2.41–11.16) | ||
| All fractures | ||||||||
| Cases | 261 | 267 | 322 | 268 | 272 | 259 | ||
| Person-years | 12,825 | 13,232 | 12,974 | 12,172 | 12,505 | 12,572 | ||
| Incidence ratea | 211 (185–237) | 210 (184–235) | 254 (227–282) | 215 (189–241) | 224 (197–251) | 228 (199–257) | ||
| Age-adjusted HR (95% CI) | 1 (Ref) | 0.99 (0.83, 1.17) | 1.18 (1.01, 1.40) | 1 (Ref) | 1.03 (0.87, 1.22) | 1.03 (0.86, 1.22) | ||
| Multivariable-adjusted HR (95% CI)b | 1 (Ref) | 0.98 (0.82, 1.16) | 1.13 (0.95, 1.34) | 0.11 | 1 (Ref) | 1.02 (0.86, 1.21) | 1.01 (0.85, 1.20) | 0.96 |
| Major osteoporotic fractures | ||||||||
| Cases | 157 | 161 | 211 | 162 | 169 | 167 | ||
| Person-years | 13,465 | 13,817 | 13,638 | 12,794 | 13,124 | 13,136 | ||
| Incidence ratea | 128 (108–148) | 129 (109–149) | 167 (145–190) | 130 (110–150) | 140 (118–161) | 153 (129–177) | ||
| Age-adjusted HR (95% CI) | 1 (Ref) | 1.01 (0.81, 1.25) | 1.29 (1.05, 1.59) | 1 (Ref) | 1.06 (0.86, 1.32) | 1.12 (0.90, 1.39) | ||
| Multivariable-adjusted HR (95% CI)b | 1 (Ref) | 0.99 (0.79, 1.24) | 1.21 (0.98, 1.50) | 0.05 | 1 (Ref) | 1.07 (0.86, 1.33) | 1.11 (0.89, 1.38) | 0.38 |
| Hip fractures | ||||||||
| Cases | 50 | 54 | 83 | 54 | 55 | 65 | ||
| Person-years | 14,127 | 14,477 | 14,416 | 13,464 | 13,801 | 13,804 | ||
| a | 43 (31–54) | 46 (34–59) | 67 (52–81) | 42 (31–54) | 47 (35–60) | 66 (49–82) | ||
| Age-adjusted HR (95% CI) | 1 (Ref) | 1.07 (0.73, 1.58) | 1.50 (1.06, 2.13) | 1 (Ref) | 1.11 (0.76, 1.62) | 1.58 (1.10, 2.28) | ||
| Multivariable-adjusted (95% CI)b | 1 (Ref) | 1.12 (0.75, 1.65) | 1.50 (1.04, 2.17) | 0.02 | 1 (Ref) | 1.12 (0.76, 1.63) | 1.59 (1.10, 2.30) | 0.01 |
Note: The total number of participants in the urinary fluoride and dietary fluoride analyses were 4,306 and 4,072, respectively. Two hundred thirty-four women were excluded from the dietary fluoride analyses because of missing dietary fluoride information due either to responding to a shorter version of the FFQ or having missing/inadequate reported dietary intake (energy intake outside 3 SD of the log-transformed mean). For each outcome, women contributed with person-time from the date of clinical examination until the of date of the specific event studied, death, or end of follow-up at 31 December 2017. CI, confidence interval; eGFR, estimated glomerular filtration rate; FFQ, food frequency questionnaire; HR, hazard ratio; Ref, reference; SD, standard deviation.
Age-standardized incidence rates per 10,000 person-years.
Multivariable-adjusted models were adjusted for age, education, height, total fat mass, lean body mass, parity, smoking status, physical activity, alcohol intake, diabetes, eGFR, tertiles of urinary excretion of calcium (for urinary fluoride) or tertiles of dietary intake of calcium (for dietary fluoride), use of calcium supplements, use of vitamin D supplements, ever use of estrogen, and ever use of corticosteroids. Urinary fluoride models were additionally adjusted for serum Beta-CrossLaps (ng/L).
Table 4.
Hazard ratios of total, osteoporotic, and hip fractures and corresponding 95% CIs by tertiles urinary fluoride (mg/g creatinine) () and dietary fluoride (mg/d) (), respectively, among women with approximately constant drinking water fluoride concentrations from 1982 to baseline.
| Categories | Tertiles of urinary fluoride | Tertiles of dietary fluoride | ||||||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 1 | 2 | 3 | |||
| 1,092 | 1,191 | 1,195 | 1,115 | 1,145 | 1,127 | |||
| Fluoride exposure {mg/g creatinine or mg/d [median (range)]} | 0.68 (0.15–0.88) | 1.08 (0.88–1.30) | 1.64 (1.30–116.51) | 1.40 (0.26–1.74) | 2.04 (1.74–2.41) | 2.92 (2.41–11.16) | ||
| All fractures | ||||||||
| Cases | 192 | 219 | 280 | 221 | 232 | 221 | ||
| Person-years | 9,861 | 11,036 | 10,819 | 10,087 | 10,536 | 10,383 | ||
| Age-adjusted HR (95% CI) | 1 Ref | 1.02 (0.84, 1.24) | 1.29 (1.08, 1.55) | 1 Ref | 1.05 (0.87, 1.26) | 1.06 (0.88, 1.28) | ||
| Multivariable-adjusted HR (95% CI)a | 1 Ref | 1.02 (0.84, 1.24) | 1.25 (1.03, 1.51) | 0.01 | 1 Ref | 1.05 (0.87, 1.26) | 1.04 (0.86, 1.25) | 0.72 |
| Major osteoporotic fractures | ||||||||
| Cases | 117 | 131 | 188 | 138 | 146 | 141 | ||
| Person-years | 10,307 | 11,509 | 11,394 | 10,533 | 11,052 | 10,881 | ||
| Age-adjusted HR (95% CI) | 1 Ref | 1.01 (0.79, 1.30) | 1.41 (1.12, 1.77) | 1 Ref | 1.06 (0.84, 1.34) | 1.10 (0.87, 1.39) | ||
| Multivariable-adjusted HR (95% CI)a | 1 Ref | 1.00 (0.78, 1.29) | 1.33 (1.05, 1.69) | 1 Ref | 1.06 (0.84, 1.34) | 1.07 (0.85, 1.36) | 0.57 | |
| Hip fractures | ||||||||
| Cases | 38 | 42 | 73 | 48 | 45 | 53 | ||
| Person-years | 10,809 | 12,069 | 12,106 | 11,090 | 11,658 | 11,464 | ||
| Age-adjusted HR (95% CI) | 1 Ref | 1.01 (0.65, 1.57) | 1.56 (1.06, 2.32) | 1 Ref | 1.03 (0.68, 1.55) | 1.41 (0.95, 2.09) | ||
| Multivariable-adjusted HR (95% CI)a | 1 Ref | 1.07 (0.68, 1.67) | 1.58 (1.05, 2.37) | 0.02 | 1 Ref | 1.02 (0.68, 1.54) | 1.40 (0.94, 2.09) | 0.09 |
Note: For each outcome, women contributed with person-time from the date of clinical examination until the of date of the specific event studied, death, or end of follow-up at 31 December 2017. The total number of participants in the urinary fluoride and dietary fluoride analyses were 3,478 and 3,387, respectively. Ninety-one women were excluded from the dietary fluoride analyses because of missing dietary fluoride information due either to responding to a shorter version of the FFQ or having missing/inadequate reported dietary intake (energy intake outside 3 SD of the log-transformed mean). CI, confidence interval; eGFR, estimated glomerular filtration rate; FFQ, food frequency questionnaire; HR, hazard ratio; Ref, reference; SD, standard deviation.
Multivariable-adjusted models were adjusted for age, education, height, total fat mass, lean body mass, parity, smoking status, physical activity, alcohol intake, diabetes, eGFR, tertiles of urinary excretion of calcium (for urinary fluoride) or tertiles of dietary intake of calcium (for dietary fluoride), use of calcium supplements, use of vitamin D supplements, ever use of estrogen, and ever use of corticosteroids. Urinary fluoride models were additionally adjusted for serum Beta-CrossLaps (ng/L).
Results for incident fractures were robust to additional sensitivity analyses, including results for major osteoporotic fractures after excluding vertebral fractures (Table S2), models of incident fractures with additional adjustment for baseline BMD (Table S3), models that included women with missing hip or spine BMD data (additional observations: 131–139 for lumbar spine BMD; 1 for femoral neck BMD; 137–145 for incident fractures; Tables S4 and S5), and associations with urinary fluoride after excluding 234 women without dietary fluoride data (Tables S6 and S7) and 142 women with urine creatinine concentrations or (Tables S8 and S9).
Discussion
In this comprehensive prospective population-based study of postmenopausal women, we explored indicators of bone health in relation to fluoride exposure in an area with natural public drinking water concentrations ranging from 0 to , well below the maximum level recommended by the WHO (WHO 2006). We estimated 50% (95% CI: 4, 217%) and 59% (95% CI: 11%, 230%) higher rates of hip fractures for the highest compared with the lowest tertiles of creatinine-adjusted urinary fluoride concentrations and estimated intake via drinking water and diet, respectively. Associations with all fractures and major osteoporotic fractures were positive but nonsignificant for urine fluoride, and null for dietary fluoride. Restricting analyses to women whose drinking water fluoride concentrations were likely to be constant from 1982 to baseline (2004–2009) strengthened the associations between urinary fluoride and the risk of fractures during follow-up. In addition, the adjusted mean BMD was slightly higher among women with higher urine and dietary fluoride levels at baseline. Altogether, these findings suggest that daily high consumption of tap water and beverages based on tap water [i.e., approximately 10 () servings of ] with fluoride content of may increase both BMD and bone fragility.
Fluoride has a potent effect on bone cell function, bone structure, and bone strength. Hydroxyapatite, the most abundant inorganic component of bone and the source of its rigidity, is converted to fluorapatite when fluoride ions replace hydroxyl ions. Fluorapatite is harder and more resistant to acidic mineral dissolution than hydroxyapatite (NRC 2006). Fluoride can also induce bone growth through stimulation of osteoblasts, an effect especially evident at the lumbar spine (Farley et al. 1983; Haguenauer et al. 2000). In the 1990s, the potential antifracture effect of fluoride on bone was extensively explored in RCTs (Haguenauer et al. 2000). However, the results were disappointing because fluoride failed to reduce vertebral fracture rates and, instead, increased the risk of nonvertebral fractures at high doses () (Haguenauer et al. 2000; Riggs et al. 1990). The increased risk was suggested to be attributed reduced elasticity and strength of the newly formed bone (Fratzl et al. 1994; Riggs et al. 1990).
In the present study, urinary fluoride excretion and estimated dietary fluoride intake were associated with increased BMD, with a stronger association for lumbar spine BMD than femoral neck BMD. The highest tertiles of urine and dietary fluoride were also associated with an increased risk of hip fractures. Although our estimates suggest a very small effect on BMD, they are in line with effects reported for therapeutic doses of fluoride in RCTs (Haguenauer et al. 2000; Riggs et al. 1990). The stronger positive association for lumbar spine than femoral neck density has been suggested to reflect differences in the effects of fluoride on trabecular vs. cortical bone (Riggs et al. 1990). It can be argued that the results of RCTs, based on very high fluoride doses during a limited period (), may not be translatable to long-term low-to-moderate exposure in real-life settings. However, because fluoride accumulates in bone (NRC 2006), low-dose exposures over extended periods also may be sufficient to produce adverse effects. Our finding of stronger associations with urine fluoride when restricted to women likely to have consistent drinking water fluoride levels for at least 20 y before baseline further supports the possibility that long-term exposures may have adverse effects, even when drinking water fluoride concentrations are below recommended limits.
Most observational evidence regarding the effects of fluoride on bone has been based on fracture rates or BMD in relation to ecological assessments of fluoride concentrations in drinking water, and results have been discordant, with some studies reporting no association between drinking water fluoride and bone parameters (Cauley et al. 1995; Feskanich et al. 1998; Hillier et al. 2000; Karagas et al. 1996; Näsman et al. 2013; Sowers et al. 2005) and others suggesting increased fracture risk or changes in BMD (Danielson et al. 1992; Jacobsen et al. 1992; Kurttio et al. 1999; Li et al. 2001; Sowers et al. 1991). We are aware of only two previous studies that used individual-level biomarkers to assess fluoride exposure (Feskanich et al. 1998; Sowers et al. 2005). A nested case–control study within the Nurses’ Health Study cohort (Feskanich et al. 1998) found no association between toenail fluoride concentrations and self-reported forearm or hip fractures in 241 matched case–control pairs. Similarly, a prospective study of 1,300 women residing in three U.S. communities with contrasting fluoride levels in drinking water () found no association between serum fluoride concentrations and baseline BMD or the risk of self-reported fractures over 4-y of follow-up (Sowers et al. 2005). Discrepant findings may be related to the use of different biomarkers, with urine and serum reflecting short-term exposures, whereas toenail clippings reflect exposure over several months. Urine is the most frequently used biomarker and, excluding fluoride concentrations in dentin and bone, is considered the most valid (EFSA Panel on Dietetic Products, Nutrition, and Allergies 2013). Discrepancies may also be related to differences in study design, fracture ascertainment, sample sizes, and study population characteristics.
Strengths of the present study include its population-based prospective design, range of fluoride exposures, and use of two different measures of fluoride exposure. The almost complete ascertainment of cases via register-linkage, and the use of DXA measurements to assess BMD are other strengths. Moreover, bottled water consumption is very low in Sweden, which had the lowest estimated bottled water consumption per capita of 25 EU countries in 2019 (, compared with for the EU as a whole) (Conway 2020). In addition, an online survey of Swedish adults indicated that tap water accounted for 78% of nonalcoholic beverage consumption in 2013 (Säve-Söderbergh et al. 2018). Thus, although some degree of exposure misclassification is inevitable, bottled water consumption is unlikely to have a substantial effect on the accuracy of estimated intakes based on municipal drinking water fluoride concentrations. Finally, although we cannot rule out the possibility of residual confounding, we had detailed information on a number of factors relevant to bone health and fluoride exposures and adjusted for them as potential confounders.
Self-reported information on dietary habits is inevitably associated with some degree of measurement error. Nevertheless, tap water, coffee, and tea, which are likely reported with higher precision than other dietary items (Wolk et al. 1997), accounted for 78% of estimated dietary fluoride intake in our study. In addition to estimating dietary intakes, we used urine fluoride excretion to classify exposure. Using a single urine sample is a limitation, given that the circulating half-life of fluoride is short (Buzalaf and Whitford 2011). Fluoride release due to bone degradation also may have increased urinary fluoride excretion in some women. However, we adjusted for plasma Beta-CrossLaps, a biochemical marker of bone resorption, to limit this potential source of confounding. The correlation between urinary and dietary fluoride was moderate (). There may be several reasons underlying this observation, including that urinary fluoride is a biomarker of short-term exposure, whereas the FFQ reflected average consumption during the past year. Finally, our study population consisted solely of middle-aged to elderly women in Sweden, and thus, our findings may not apply to other population subgroups or to women in other countries. Notwithstanding this potential limitation, our results provide insights into the association of fluoride exposure with bone health in postmenopausal women—the group where the burden of hip fractures is the largest.
Conclusion
The risk of hip fractures was increased among Swedish women who had the highest levels of urine fluoride excretion and the highest estimated fluoride intake from beverages and food relative to women with the lowest levels of each exposure. Our findings, which are consistent with the effects of high fluoride exposures observed in RCTs (resulting in a denser but more fragile skeleton), suggest that long-term consumption of tap water with a fluoride concentration of , which is below the maximum concentration recommended by the WHO, may adversely affect bone health in postmenopausal women.
Supplementary Material
Acknowledgments
initiated the study and obtained the funding and A.W., K.M., and designed it and collected the data. and M.K. supervised the urinary measurements. E.H., supervised by , complied the database on fluoride and performed the statistical analyses as well as interpreted the data together with C.D.V. and . All authors contributed to the interpretation of the data. E.H. wrote the first draft of the manuscript, and C.D.V., M.K., A.W., K.M., and revised it, provided comments, and approved the latest version.
This work was supported by grants from Formas, the Swedish Research Council for Environment, Agricultural Sciences and Spatial Planning (2020-01630), and from the Swedish Research Council (2017-00822). The study sponsors had no role in the initiation of the study or interpretation of the results.
References
- Buzalaf MAR, Whitford GM. 2011. Fluoride metabolism. Monogr Oral Sci 22:20–36, PMID: 21701189, 10.1159/000325107. [DOI] [PubMed] [Google Scholar]
- Cauley JA, Murphy PA, Riley TJ, Buhari AM. 1995. Effects of fluoridated drinking water on bone mass and fractures: the study of osteoporotic fractures. J Bone Miner Res 10(7):1076–1086, PMID: 7484283, 10.1002/jbmr.5650100712. [DOI] [PubMed] [Google Scholar]
- Conway J. 2020. Per capita consumption of bottled water in Europe in 2019, by country. https://www.statista.com/statistics/455422/bottled-water-consumption-in-europe-per-capita/ [accessed 4 March 2021].
- Crandall CJ, Han W, Greendale GA, Seeman T, Tepper P, Thurston R, et al. 2014. Socioeconomic status in relation to incident fracture risk in the Study of Women’s Health Across the Nation. Osteoporos Int 25(4):1379–1388, PMID: 24504101, 10.1007/s00198-013-2616-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Danielson C, Lyon JL, Egger M, Goodenough GK. 1992. Hip fractures and fluoridation in Utah’s elderly population. JAMA 268(6):746–748, PMID: 1640574, 10.1001/jama.1992.03490060078027. [DOI] [PubMed] [Google Scholar]
- EFSA Panel on Dietetic Products, Nutrition, and Allergies. 2013. Scientific opinion on dietary reference values for fluoride. EFSA J 11(8):3332, 10.2903/j.efsa.2013.3332. [DOI] [Google Scholar]
- Farley JR, Wergedal JE, Baylink DJ. 1983. Fluoride directly stimulates proliferation and alkaline phosphatase activity of bone-forming cells. Science 222(4621):330–332, PMID: 6623079, 10.1126/science.6623079. [DOI] [PubMed] [Google Scholar]
- Feskanich D, Owusu W, Hunter DJ, Willett W, Ascherio A, Spiegelman D, et al. 1998. Use of toenail fluoride levels as an indicator for the risk of hip and forearm fractures in women. Epidemiology 9(4):412–416, PMID: 9647905, 10.1097/00001648-199807000-00011. [DOI] [PubMed] [Google Scholar]
- Fratzl P, Roschger P, Eschberger J, Abendroth B, Klaushofer K. 1994. Abnormal bone mineralization after fluoride treatment in osteoporosis: a small-angle X-ray-scattering study. J Bone Miner Res 9(10):1541–1549, PMID: 7817799, 10.1002/jbmr.5650091006. [DOI] [PubMed] [Google Scholar]
- Haguenauer D, Welch V, Shea B, Tugwell P, Adachi JD, Wells G. 2000. Fluoride for the treatment of postmenopausal osteoporotic fractures: a meta-analysis. Osteoporos Int 11(9):727–738, PMID: 11148800, 10.1007/s001980070051. [DOI] [PubMed] [Google Scholar]
- Harris H, Håkansson N, Olofsson C, Stackelberg O, Julin B, Åkesson A, et al. 2013. The Swedish mammography cohort and the cohort of Swedish men: study design and characteristics of two population-based longitudinal cohorts. OA Epidemiology 1(2):16, 10.13172/2053-079X-1-2-943. [DOI] [Google Scholar]
- Hemenway D, Feskanich D, Colditz GA. 1995. Body height and hip fracture: a cohort study of 90,000 women. Int J Epidemiol 24(4):783–786, PMID: 8550276, 10.1093/ije/24.4.783. [DOI] [PubMed] [Google Scholar]
- Hillier S, Cooper C, Kellingray S, Russell G, Hughes H, Coggon D. 2000. Fluoride in drinking water and risk of hip fracture in the UK: a case-control study. Lancet 355(9200):265–269, PMID: 10675073, 10.1016/S0140-6736(99)07161-5. [DOI] [PubMed] [Google Scholar]
- Inker LA, Schmid CH, Tighiouart H, Eckfeldt JH, Feldman HI, Greene T, et al. 2012. Estimating glomerular filtration rate from serum creatinine and cystatin C. N Engl J Med 367(1):20–29, PMID: 22762315, 10.1056/NEJMoa1114248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jacobsen SJ, Goldberg J, Cooper C, Lockwood SA. 1992. The association between water fluoridation and hip fracture among white women and men aged 65 years and older. A national ecologic study. Ann Epidemiol 2(5):617–626, PMID: 1342313, 10.1016/1047-2797(92)90006-C. [DOI] [PubMed] [Google Scholar]
- Kanis JA, Cooper C, Rizzoli R, Reginster JY, Scientific Advisory Board of the European Society for Clinical and Economic Aspects of Osteoporosis, Committees of Scientific Advisors and National Societies of the International Osteoporosis Foundation. 2019. European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int 30(1):3–44, PMID: 30324412, 10.1007/s00198-018-4704-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karagas MR, Baron JA, Barrett JA, Jacobsen SJ. 1996. Patterns of fracture among the United States elderly: geographic and fluoride effects. Ann Epidemiol 6(3):209–216, PMID: 8827156, 10.1016/1047-2797(96)00006-3. [DOI] [PubMed] [Google Scholar]
- Kim SM, Long J, Montez-Rath M, Leonard M, Chertow GM. 2016. Hip fracture in patients with non-dialysis-requiring chronic kidney disease. J Bone Miner Res 31(10):1803–1809, PMID: 27145189, 10.1002/jbmr.2862. [DOI] [PubMed] [Google Scholar]
- Kurttio P, Gustavsson N, Vartiainen T, Pekkanen J. 1999. Exposure to natural fluoride in well water and hip fracture: a cohort analysis in Finland. Am J Epidemiol 150(8):817–824, PMID: 10522652, 10.1093/oxfordjournals.aje.a010086. [DOI] [PubMed] [Google Scholar]
- Lehmann R, Wapniarz M, Hofmann B, Pieper B, Haubitz I, Allolio B. 1998. Drinking water fluoridation: bone mineral density and hip fracture incidence. Bone 22(3):273–278, PMID: 9514220, 10.1016/s8756-3282(97)00273-1. [DOI] [PubMed] [Google Scholar]
- Li Y, Liang C, Slemenda CW, Ji R, Sun S, Cao J, et al. 2001. Effect of long-term exposure to fluoride in drinking water on risks of bone fractures. J Bone Miner Res 16(5):932–939, PMID: 11341339, 10.1359/jbmr.2001.16.5.932. [DOI] [PubMed] [Google Scholar]
- Ludvigsson JF, Andersson E, Ekbom A, Feychting M, Kim JL, Reuterwall C, et al. 2011. External review and validation of the Swedish National Inpatient Register. BMC Public Health 11:450, PMID: 21658213, 10.1186/1471-2458-11-450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Malinowska E, Inkielewicz I, Czarnowski W, Szefer P. 2008. Assessment of fluoride concentration and daily intake by human from tea and herbal infusions. Food Chem Toxicol 46(3):1055–1061, PMID: 18078704, 10.1016/j.fct.2007.10.039. [DOI] [PubMed] [Google Scholar]
- Näsman P, Ekstrand J, Granath F, Ekbom A, Fored CM. 2013. Estimated drinking water fluoride exposure and risk of hip fracture: a cohort study. J Dent Res 92(11):1029–1034, PMID: 24084670, 10.1177/0022034513506443. [DOI] [PubMed] [Google Scholar]
- NRC (National Research Council). 2006. Fluoride in Drinking Water: A Scientific Review of EPA’s Standards. Washington, DC: National Academies Press. [Google Scholar]
- Phipps KR, Orwoll ES, Mason JD, Cauley JA. 2000. Community water fluoridation, bone mineral density, and fractures: prospective study of effects in older women. BMJ 321(7265):860–864, PMID: 11021862, 10.1136/bmj.321.7265.860. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Riggs BL, Hodgson SF, O’Fallon WM, Chao EY, Wahner HW, Muhs JM, et al. 1990. Effect of fluoride treatment on the fracture rate in postmenopausal women with osteoporosis. N Engl J Med 322(12):802–809, PMID: 2407957, 10.1056/NEJM199003223221203. [DOI] [PubMed] [Google Scholar]
- Säve-Söderbergh M, Toljander J, Mattisson I, Åkesson A, Simonsson M. 2018. Drinking water consumption patterns among adults—SMS as a novel tool for collection of repeated self-reported water consumption. J Expo Sci Environ Epidemiol 28(2):131–139, PMID: 28612838, 10.1038/jes.2017.8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simonen O, Laitinen O. 1985. Does fluoridation of drinking-water prevent bone fragility and osteoporosis? Lancet 2(8452):432–434, PMID: 2863455, 10.1016/s0140-6736(85)92748-5. [DOI] [PubMed] [Google Scholar]
- Sowers MF, Clark MK, Jannausch ML, Wallace RB. 1991. A prospective study of bone mineral content and fracture in communities with differential fluoride exposure. Am J Epidemiol 133(7):649–660, PMID: 2018020, 10.1093/oxfordjournals.aje.a115940. [DOI] [PubMed] [Google Scholar]
- Sowers M, Whitford GM, Clark MK, Jannausch ML. 2005. Elevated serum fluoride concentrations in women are not related to fractures and bone mineral density. J Nutr 135(9):2247–2252, PMID: 16140906, 10.1093/jn/135.9.2247. [DOI] [PubMed] [Google Scholar]
- Stattin K, Michaëlsson K, Larsson SC, Wolk A, Byberg L. 2017. Leisure-time physical activity and risk of fracture: a cohort study of 66,940 men and women. J Bone Miner Res 32(8):1599–1606, PMID: 28460152, 10.1002/jbmr.3161. [DOI] [PubMed] [Google Scholar]
- U.S. Department of Health and Human Services Federal Panel on Community Water Fluoridation. 2015. U.S. Public Health Service recommendation for fluoride concentration in drinking water for the prevention of dental caries. Public Health Rep 130(4):318–331, PMID: 26346489, 10.1177/003335491513000408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- USDA (U.S. Department of Agriculture). 2005. USDA National Fluoride Database of Selected Beverages and Foods. Release 2. Washington, DC: U.S. Department of Agriculture. https://data.nal.usda.gov/dataset/usda-national-fluoride-database-selected-beverages-and-foods-release-2-2005 [accessed 21 March 2021]. [Google Scholar]
- Vasikaran S, Eastell R, Bruyère O, Foldes AJ, Garnero P, Griesmacher A, et al. 2011. Markers of bone turnover for the prediction of fracture risk and monitoring of osteoporosis treatment: a need for international reference standards. Osteoporos Int 22(2):391–420, PMID: 21184054, 10.1007/s00198-010-1501-1. [DOI] [PubMed] [Google Scholar]
- Wang Q, Huang Q, Zeng Y, Liang JJ, Liu SY, Gu X, et al. 2016. Parity and osteoporotic fracture risk in postmenopausal women: a dose-response meta-analysis of prospective studies. Osteoporos Int 27(1):319–330, PMID: 26439242, 10.1007/s00198-015-3351-3. [DOI] [PubMed] [Google Scholar]
- Warensjö E, Byberg L, Melhus H, Gedeborg R, Mallmin H, Wolk A, et al. 2011. Dietary calcium intake and risk of fracture and osteoporosis: prospective longitudinal cohort study. BMJ 342:d1473, PMID: 21610048, 10.1136/bmj.d1473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weaver CM, Alexander DD, Boushey CJ, Dawson-Hughes B, Lappe JM, LeBoff MS, et al. 2016. Calcium plus vitamin D supplementation and risk of fractures: an updated meta-analysis from the National Osteoporosis Foundation. Osteoporos Int 27(1):367–376, PMID: 26510847, 10.1007/s00198-015-3386-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- WHO (World Health Organization). 2006. Fluoride in Drinking Water. Geneva, Switzerland: WHO. [Google Scholar]
- WHO. 2016. International Statistical Classification of Diseases and Related Health Problems, 10th Revision. http://apps.who.int/classifications/icd10/browse/2016/en [accessed 21 March 2021].
- Willett W, Stampfer MJ. 1986. Total energy intake: implications for epidemiologic analyses. Am J Epidemiol 124(1):17–27, PMID: 3521261, 10.1093/oxfordjournals.aje.a114366. [DOI] [PubMed] [Google Scholar]
- Wolk A, Bergström R, Hansson LE, Nyrén O. 1997. Reliability of retrospective information on diet 20 years ago and consistency of independent measurements of remote adolescent diet. Nutr Cancer 29(3):234–241, PMID: 9457745, 10.1080/01635589709514630. [DOI] [PubMed] [Google Scholar]
- Yin XH, Huang GL, Lin DR, Wan CC, Wang YD, Song JK, et al. 2015. Exposure to fluoride in drinking water and hip fracture risk: a meta-analysis of observational studies. PLoS One 10(5):e0126488, PMID: 26020536, 10.1371/journal.pone.0126488. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.