

Sir,
Scrub typhus is a mite-borne human infection caused by the bacteria Orientia tsutsugamushi. It has become a public health problem in Asia, where about 1 million new cases are identified annually and 1 billion people may be at risk of becoming infected.[1] Reported complications of scrub typhus include interstitial pneumonia, acute renal failure, meningoencephalitis, gastrointestinal bleeding, and multiple organ failure.[2,3] We report two cases of scrub typhus infection presenting as abdominal pain because of splenic infarction.
The first case was of a 21-year-old male, who presented to us with a history of high-grade intermittent fever for 3 days and pain in the left upper abdomen for 2 days. He was febrile (102°F) and the pulse rate was 125/min. There was no petechial rash on the body. Abdominal examination was normal. Investigations showed that complete blood count (CBC), total leukocyte count, and differential leukocyte count were normal. Peripheral smear for malarial parasite, malarial antigen test, IgM/IgG dengue, and IgM leptospira were negative. IgM ELISA was positive for scrub typhus. Contrast-enhanced computed tomography (CECT) abdomen revealed splenic infarct [Figure 1a]. The patient was started on tablet doxycycline 100 mg twice a day. He became afebrile on the 3rdday of initiation of treatment and was discharged on the 5thday.
Figure 1.
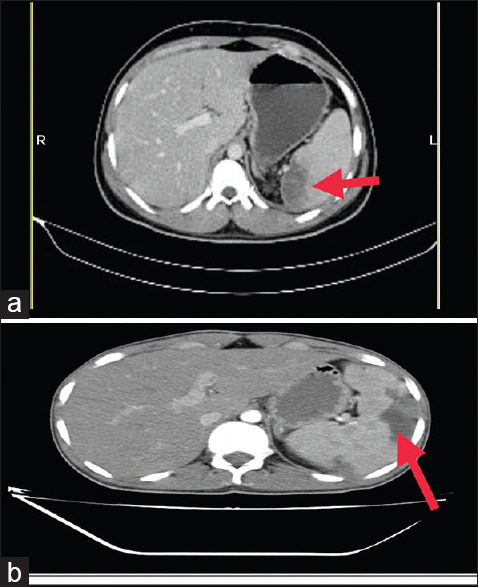
(a and b) Contrast-enhanced computed tomography of the abdomen showing splenic infarction of the respective cases
The second case was of a 48-year-old male who presented with high-grade fever for 15 days. He had left hypochondriac pain for 5 days and mild dry cough for 5 days. General and systemic examination was normal. CBC was normal. Periphe ral smear for malarial parasite, malarial antigen test, and IgM/IgG dengue were negative. CECT abdomen was done which revealed splenic infarct [Figure 1b]. His scrub typhus IgM ELISA was positive, confirming the diagnosis of scrub typhus. He responded to the treatment with doxycycline.
Scrub typhus is an acute febrile illness caused by Rickettsia O. tsutsugamushi. It is grossly underdiagnosed due to its nonspecific clinical presentations, limited awareness, and low index of suspicion among clinicians. Splenic infarcts have been very rarely reported in scrub typhus.[4,5] Fever is the most common feature of scrub typhus. Eschar is pathognomonic. Severe manifestations include acute respiratory distress syndrome, meningitis/meningoencephalitis hepatic failure, renal failure, and multiple organ failure syndromes.[6]
Serological tests remain an indispensable tool in the diagnosis. Weil–Felix test detects cross-reacting antibodies to Proteus mirabilis OX-K, but has 30%–50% sensitive. Ig M ELISA has specificity and sensitivity of ~ 90%.
Current treatment for scrub typhus is based on antibiotic therapy with doxycycline or azithromycin. Duration of treatment should be 1 week–10 days for mild-to-moderate infection if doxycycline is used.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Watt G, Parola P. Scrub typhus and tropical rickettsioses. Curr Opin Infect Dis. 2003;16:429–36. doi: 10.1097/00001432-200310000-00009. [DOI] [PubMed] [Google Scholar]
- 2.Kim SJ, Chung IK, Chung IS, Song DH, Park SH, Kim HS, et al. The clinical significance of upper gastrointestinal endoscopy in gastrointestinal vasculitis related to scrub typhus. Endoscopy. 2000;32:950–5. doi: 10.1055/s-2000-9621. [DOI] [PubMed] [Google Scholar]
- 3.Thap LC, Supanaranond W, Treeprasertsuk S, Kitvatanachai S, Chinprasatsak S, Phonrat B. Septic shock secondary to scrub typhus: Characteristics and complications. Southeast Asian J Trop Med Public Health. 2002;33:780–6. [PubMed] [Google Scholar]
- 4.Jung JO, Jeon G, Lee SS, Chung DR. Two cases of tsutsugamushi disease complicated with splenic infarction. Korean J Med. 2004;67(Supp 3):S932–6. [Google Scholar]
- 5.Hwang JH, Lee CS. Incidentally discovered splenic infarction associated with scrub typhus. Am J Trop Med Hyg. 2015;93:435. doi: 10.4269/ajtmh.15-0140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rajapakse S, Rodrigo C, Fernando D. Scrub typhus: Pathophysiology, clinical manifestations and prognosis. Asian Pac J Trop Med. 2012;5:261–4. doi: 10.1016/S1995-7645(12)60036-4. [DOI] [PubMed] [Google Scholar]