

Abstract
Cryolipolysis is a nonsurgical body sculpting technique that uses controlled cooling for localized fat reduction. The aim of the present study was to assess whether an intensive regimen of CoolSculpting based on multiple cycles/sessions on the same body area(s) could yield greater (more clinically significant) improvements in body contour. This was a prospective analysis of consecutive, healthy, adult patients undergoing CoolSculpting in routine practice across a variety of treatment areas. Patients underwent ≤4 cycles of CoolSculpting per body area during an initial treatment session, and ≤4 further cycles 4 weeks later (if required). They were followed up for ≥12 weeks. Twenty‐eight patients were enrolled (n = 26 female; mean age: 51.6 ± 9.0 years; mean body weight: 69.4 ± 13.7 kg). They were treated across 58 body areas: 48 in a single session; 10 across two sessions. The mean number of cycles per area was 2.8 ± 1.5. Twenty‐seven patients (54 body areas) were considered as treatment “responders.” In these individuals, mean skinfold thickness decreased from 35.4 ± 9.9 mm pretreatment to 22.2 ± 7.6 mm at 12 weeks (mean change: −40%; P < .001). Mean change in skinfold thickness was greater with ≥3 vs 1 to 2 cycles of CoolSculpting (P = .01). Patient satisfaction was high (n = 51/58; 88%). No adverse events were recorded. The study shows that multiple cycles/sessions of CoolSculpting can safely improve overall treatment benefit in body contouring, with greater decreases in skinfold thickness than have typically been previously observed.
Keywords: body contouring, body sculpting, CoolSculpting, cryolipolysis, liposuction
1. INTRODUCTION
Cryolipolysis is a body sculpting technique based on the application of controlled cooling for localized fat reduction. Lipid‐rich adipocytes are more susceptible to the effects of cold than other cell types, and hence cryolipolysis can induce the apoptosis of adipocytes without causing significant damage to other local structures. 1 , 2 , 3 From a technical standpoint, the procedure uses a surface or vacuum applicator with no use of instruments that penetrate the dermis, and is therefore entirely noninvasive.
Although adipocytes are metabolized internally following cryolipolysis, there is no evidence of any resulting increases in serum lipid levels or altered liver function tests. 4 , 5 Several months may be required for complete metabolization and elimination of lipids, but results can be observable within a month of the procedure. 6
A systematic review of 19 studies and case reports found that mean reductions in caliper‐assessed skinfold thickness ranged from 14.7% to 28.5%, while mean reductions by ultrasound were in the order of 10.3% to 25.5%. 4 Levels of patient satisfaction were high, and side effects were typically mild and of short duration. 4
This profile compares favorably with more invasive methods of localized spot fat reduction, such as liposuction, which also have much greater convalescence time and carry a greater risk of complications. Indeed, cryolipolysis offers an important advantage with regard to rapid recovery and hence minimal “down time” away from work and other commitments.
The first cryolipolysis system approved for use by national and international regulatory bodies was CoolSculpting, which has now been available for almost 10 years and has been used for millions of treatment cycles worldwide. 7 A number of studies have demonstrated that CoolSculpting is safe and effective across a wide variety of areas of the body—including the abdomen, back, flanks, thighs, arms, and the submental area—with high levels of resulting patient satisfaction. 4 , 5 , 8 , 9 , 10 , 11 , 12 Treatment of multiple sites during a single patient visit does not appear to have any detrimental effect on overall safety and tolerability. 5
However, to date, published data have typically demonstrated modest efficacy compared with traditional surgical interventions such as liposuction. 4 , 5 , 8 , 9 , 10 , 11 , 12 These studies often either did not specify how many treatment cycles were used, or they used low numbers of cycles (eg, one cycle per area or one per side). 4 , 5 , 8 , 10 In our clinical practice, we commonly use multiple overlapping cycles on the same area of the body with the aim of achieving more clinically significant reductions in localized adiposity and greater improvements in body contour. The present study assessed the impact of this method on patient outcomes.
2. METHODS
2.1. Study design
This was a prospective, single‐arm, and single‐center study of consecutive patients undergoing nonsurgical cryolipolysis treatment in routine clinical practice using the CoolSculpting device (Allergan, Dublin, Ireland) between April and July 2019. The study was conducted in accordance with the Declaration of Helsinki.
Eligible individuals were females and males aged ≥25 years wishing to receive fat‐reducing body sculpting treatment in at least one area of their body. Patients were required to be in good general health with no contraindications for cryolipolysis (eg, cryoglobulinemia, paroxysmal cold hemoglobinuria, or cold agglutinin disease).
2.2. Techniques
Treatment needs were assessed in partnership with the individual patient. Cryolipolysis was then carried out in one or more of the following areas of the body: abdomen, back, flanks, beneath the buttocks (“banana rolls”), inner thighs, medial knees, upper arms, and/or submental area.
The procedure, applicator used, and duration of each cycle (Table 1) were as per the manufacturer's instructions. The area to be treated was first marked out using the applicator stencils provided by the manufacturer. The skin was then cleansed and a protective membrane was placed on the skin before the applicator was used and cooling commenced.
TABLE 1.
CoolSculpting applicators
| Applicator | Body areas | Standard cycle duration |
|---|---|---|
| CoolAdvantage | Upper arms (large), upper back (large), upper flanks (large), lower flanks, inner thighs, banana roll (large), upper abdomen, lower abdomen | 35 min |
| CoolAdvantage Plus | Upper abdomen (large), lower abdomen (large), lower flanks (large) | 45 min |
| CoolAdvantage Petite | Upper arms, upper back, upper flanks, lower flanks, inner thigh, banana roll, upper abdomen, lower abdomen, medial knee | 35 min |
| CoolMini | Submental, axillary puff, distal thigh, medial knee (small) | 45 min |
| CoolSmooth Pro | Upper abdomen (flat), outer thigh | 75 min |
Decisions on the number of cycles/sessions required were incorporated into the treatment plan from the outset. During the initial treatment session, patients could undergo up to 4 cycles of treatment (ie, up to four separate applications of the applicator) on any given area of the body, as per the judgment of the clinician. Key factors when determining the number of cycles required included the size and contour of the treatment area. When warranted, a second session of up to four further cycles of treatment could be given 4 weeks after the initial session—eg, in body areas where there was significant localized adiposity at baseline or when the patient wished to achieve the maximum possible reduction in fat.
2.3. Assessments
Prior to treatment, age, sex, and weight were recorded for all patients. During the pretreatment marking up process, skinfold thickness was measured for all treatment areas at the point of maximal adipose projection using a standard set of calipers; skinfold thickness may be considered as an indirect measure of subcutanous fat presence. Measurements were taken three times, and the mean value recorded. For consistency, all measurements were made by the same assessor using the same standardized set of calipers. Treatment area(s) and the number of sessions and cycles undertaken were documented for all patients.
Follow‐up visits were scheduled at 6 and 12 weeks posttreatment. At the 12‐week visit, weight and skinfold thickness measurements were repeated using the same methods as pretreatment. All patients were photographed pre‐ and posttreatment in a dedicated photography studio using fixed lighting and a foot positioning mat to control image quality.
Patients were categorized as treatment “responders” or “nonresponders” depending on whether there were any clinically significant changes from baseline in caliper‐assessed skinfold thickness or clinical photographs. Patients were also asked at the 12‐week visit whether or not they were satisfied with the results at each separate treatment area. They were monitored for adverse events (AEs) throughout treatment and follow‐up.
2.4. Statistical analyses
Descriptive statistics are provided throughout, including mean, SD and range for continuous variables, and frequency and percentage for categorical variables.
Absolute and percentage changes in skinfold thickness and patient weight before and after CoolSculpting treatment are provided with 95% confidence intervals (CI). Change in skinfold thickness was assessed per treatment area using multilevel statistical methods. Change in weight was assessed per patient using the t‐test. Additional analyses were performed using multilevel models to examine whether there was any association between change in skinfold thickness and the number of CoolSculpting cycles/sessions received. Statistical significance was determined based on P < .05.
3. RESULTS
3.1. Patients and treatment
A total of 28 patients were enrolled, of whom 26 were female and two were male. The mean age was 51.6 ± 9.0 years (range: 32‐69 years). Mean body weight at baseline was 69.4 ± 13.7 kg (range: 49.4‐97.1 kg; Table 2).
TABLE 2.
Patient characteristics and treatments
| Characteristic | Patients (N = 28) |
|---|---|
| Sex, n | |
| Female | 26 |
| Male | 2 |
| Age, years, mean ± SD (range) | 51.6 ± 9.0 (32–69) |
| Weight, a kg, mean ± SD (range) | 69.4 ± 13.7 (49.4‐97.1) |
| Total number of treatment areas, n | |
| 1 | 14 |
| 2 | 8 |
| 3 | 1 |
| 4 | 2 |
| 5 | 1 |
| 6 | 2 |
N = 25 (data missing for three remaining patients).
Fourteen patients were treated in a single area of the body, and eight were treated in two areas; the remaining six were treated in three or more areas of the body (Table 2). Thus, there was a total of 58 separate treatment areas across the 28 patients (equivalent to 2.1 per patient).
The most commonly treated parts of the body were the lower abdomen (n = 11; 19%), the upper abdomen (n = 8; 14%), the submental area (n = 8; 14%), the upper arms (n = 7; 12%) and the lower flanks (n = 7; 12%; Figure 1).
FIGURE 1.
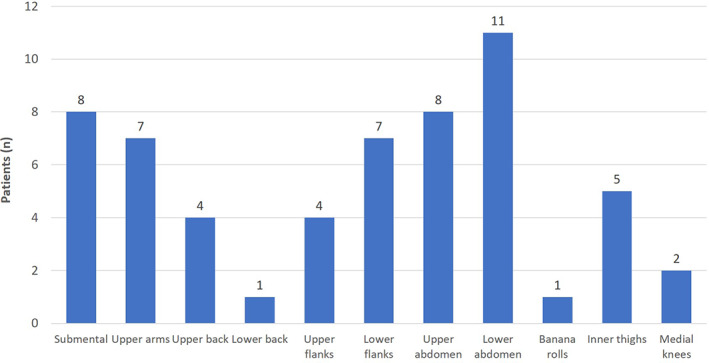
Treatment areas. N = 58
Forty‐eight of the 58 treatments were administered in a single session; the other 10 underwent a second treatment session around 4 weeks later. Whether given in 1 or 2 sessions, the mean number of treatment cycles per treatment area was 2.8 ± 1.5 (range: 1‐8; Figure 2).
FIGURE 2.
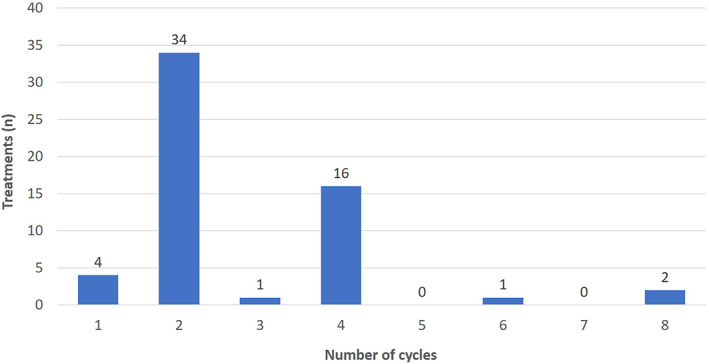
Total number of cycles of CoolSculpting in each treatment. N = 58 treatment areas
3.2. Treatment outcomes
Skinfold thickness measurements were taken for each of the 58 separate treatment areas. Most patients showed substantial reductions across all treatment areas. Indeed, 27 of the 28 patients were considered to be “responders”, and example pre‐ and posttreatment images are provided in Figures 3, 4, 5, 6. One individual was categorized as a “nonresponder”, achieving no clinically significant changes in either caliper measurements of skinfold thickness or clinical before‐and‐after images.
FIGURE 3.
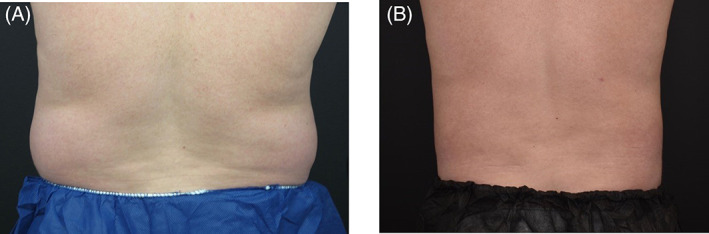
CoolSculpting of the flanks. A, A 42‐year‐old woman before treatment with 4 cycles (1 session) of CoolSculpting and B, at 12 weeks after treatment
FIGURE 4.
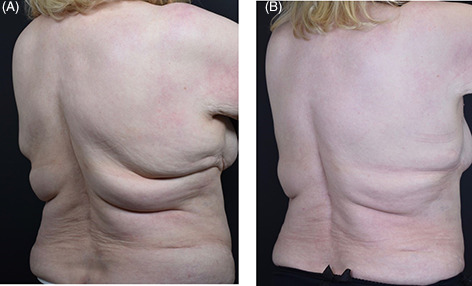
CoolSculpting of the upper and lower back. A, A 68‐year‐old woman before treatment with 12 cycles (1 session) of CoolSculpting and B, at 8 weeks after treatment
FIGURE 5.
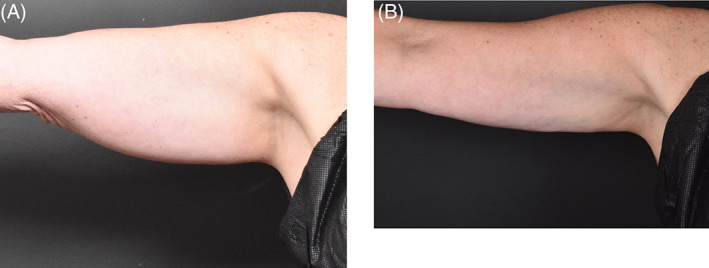
CoolSculpting of the upper arms. A, A 58‐year‐old woman before treatment with 4 cycles (1 session) of CoolSculpting and B, at 12 weeks after treatment
FIGURE 6.
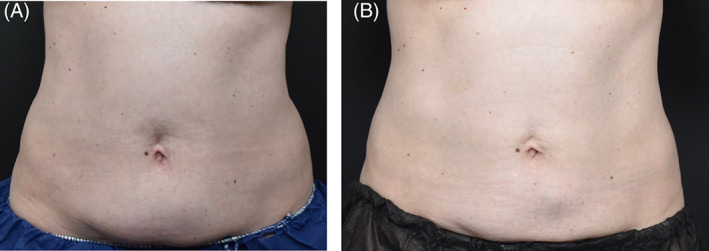
CoolSculpting of the abdomen. A, A 58‐year‐old woman before treatment with 4 cycles (1 session) of CoolSculpting and B, at 12 weeks after treatment
Among responders, mean skinfold thickness was 35.4 ± 9.9 mm pretreatment and 22.2 ± 7.6 mm at 12 weeks posttreatment. This equates to a mean absolute change of −13.7 mm (95% CI: −16.1, −11.3; P < .001) and a mean percentage change of −40% (95% CI: −45, −35; P < .001; Figure 7).
FIGURE 7.
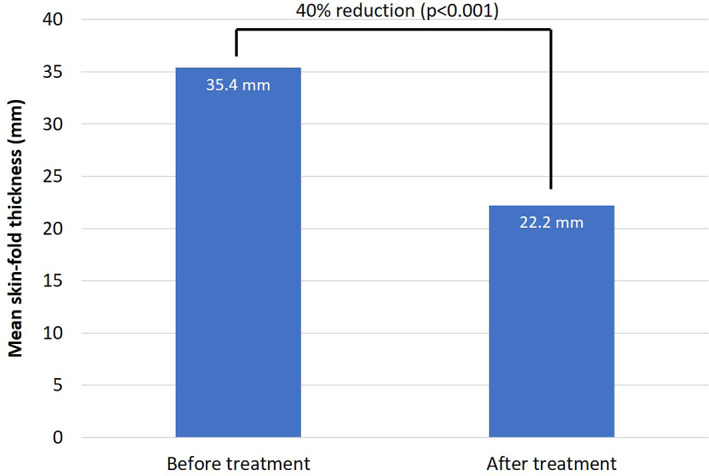
Mean skinfold thickness before and after CoolSculpting treatment in treatment responders. N = 54 treatment areas among 27 patients who were considered to be responders
A subanalysis was performed among responders based on whether CoolSculpting treatment was given over a single session (n = 44) or two sessions (n = 10). The absolute change in skinfold thickness was −16.6 mm in the subgroup receiving two sessions compared with −13.1 mm in those receiving one session (P = .06).
A similar responder subanalysis comparing results based on 1 to 2 cycles (n = 35) vs ≥3 cycles (n = 19) of CoolSculpting suggested that the mean absolute change in skinfold thickness was greater with ≥3 vs 1 to 2 cycles (−16.1 mm vs −12.4 mm, respectively; P = .01).
Among 25 patients with available measurements, mean weight changed from 69.4 ± 13.7 kg before CoolSculpting to 69.6 ± 13.1 kg at 12 weeks posttreatment. The mean absolute change was +0.1 kg (95% CI: −0.5, 0.8; P = .64).
When asked at their 12‐week posttreatment visit whether or not they were satisfied with the results in each treatment area, the 28 included patients said that they were satisfied in 51 instances (88%) and not satisfied in the other 7 (12%). Among the 27 responders, patients said they were satisfied in 51 instances (94%) and not satisfied in 3 (6%).
There were no AEs recorded throughout all treatment sessions and follow‐up visits.
4. DISCUSSION
This study demonstrated that multiple cycles/sessions of CoolSculpting can be safely used to maximize the treatment benefit of body contouring in routine clinical practice. For all of the included individuals, the use of several cycles/sessions was agreed within the original treatment plan based on localized adiposity at baseline, the wishes of the patient, and the size and contour of the treatment area.
It is perhaps not surprising that providing more treatment cycles leads to more clinically significant results. Nonetheless, the mean decrease in skinfold thickness of 40% was substantially greater than the reductions of 14.7‐28.5% noted in a systematic review of previous studies. 4 The overall clinical significance of the results achieved is further demonstrated in the patient photographs in Figures 3, 4, 5, 6. Furthermore, a subanalysis of the present data suggested that reductions in skinfold thickness were significantly larger in patients receiving greater numbers of treatment cycles. There was also a trend towards larger reductions in those receiving two rather than one session of treatment. Previous studies have also observed that a second session of treatment a few weeks after the first may increase the magnitude of effect on skinfold thickness. 13 , 14
The analysis was not large enough to distinguish which body areas benefitted most from multiple cycles/sessions of treatment. The areas in which ≥4 cycles were most commonly used were the lower flank (n = 5) and the upper arm (n = 4); anecdotally, we have also observed that the thighs often benefit from larger numbers of cycles. However, this requires further study.
Some of the improvement in outcomes in the present analysis relative to previous studies could relate to recent changes in the design of the CoolSculpting applicators. The new versions (used in the current study) apply more even cooling to a greater surface area, and hence should be more effective than previous applicators (used in earlier studies). However, this would be expected to provide an incremental benefit rather than the substantial improvements in outcomes noted here and cannot alone explain the difference.
Indeed, almost all subjects showed substantial improvements in skinfold thickness and corresponding clinically significant improvements in body contour, with only one of 28 patients considered to be a nonresponder. Importantly, the greater improvements in body contouring observed in the skinfold thickness assessment also appeared to enhance patient‐reported outcomes: the patient satisfaction rate (88%) was higher than has been previously observed. 7 , 15
The one patient who did not respond to treatment had received 10 cycles of CoolSculpting to the abdomen and flanks with no improvement in either skinfold thickness measurements or clinical photographs. That individual was excluded from the statistical analyses of skinfold thickness reduction. She was re‐treated with an additional 16 cycles of treatment 12 weeks following her initial treatment and still showed no clinical improvements at 12 weeks following the second session of treatment. The issue of nonresponders to CoolSculpting treatment has not previously been addressed in the literature although it seems likely that there is a small proportion of patients who do not respond. The reasons why particular patients are resistant to the effects of this treatment are not well understood but may relate to an unknown survival mechanism that confers an advantage for surviving in extreme cold temperatures. Each treatment cycle currently lasts 35 to 45 min, and it is unclear whether nonresponders might benefit from either more prolonged exposure or exposure to lower temperatures than the present device allows. Larger studies will be needed to determine more accurately the proportion of patients who do not respond.
No complications were recorded in the current analysis. Other studies have typically noted only mild AEs, such as erythema, bruising, swelling, sensitivity, and pain, which have generally resolved rapidly. 4 We considered these minor and short‐lived effects as expected sequelae of the treatment and did not record them as AEs. However, importantly, there were no unexpected, longer‐lasting AEs. An uncommon but clinically significant AE that has been observed with increasing frequency in recent years is paradoxical adipose hyperplasia (PAH). 16 , 17 , 18 The etiology of PAH remains unclear but may involve a form of “natural selection” for survival of some adipocytes that have greater inherent tolerance for cryolipolysis. 19 Cases typically develop within 2 to 6 months postprocedure, 18 , 20 and the most commonly recommended treatment is power‐assisted liposuction. 16 , 21 , 22 All enrolled subjects in the current study had at least 3 months of follow‐up, but there were no cases of PAH.
Appropriate patient selection is essential for optimizing outcomes and minimizing complications. Key criteria that should be considered include age, anthropometric data, skin characteristics, cutaneous sensitivity, and risk pathologies for this treatment. 6 In addition, patients should be educated on potential complications before therapy is initiated. They should also understand that CoolSculpting is not a treatment for obesity, 23 but rather for the reduction of discrete, persistent, localized fat. 6 This was evident in the lack of mean weight loss in our study despite large reductions in local skinfold thickness. It has been suggested elsewhere that more intensive treatment could be used as a weight‐loss strategy, 24 but that possibility remains to be fully explored.
We should acknowledge the limitations of this work. First, it was a single‐center study conducted in the context of routine practice, with no control arm; randomized controlled trials would of course be valuable for confirming our results. Second, there is inevitably some variability in the measurement of skinfold thickness using calipers. However, to minimize this, all measurements were made in triplicate by the same assessor using the same calipers. Furthermore, alternative methods for analyzing tissue reduction with cryolipolysis treatment, such as ultrasound, are also associated with technical drawbacks. Overall, the use of calipers remains a sound, objective method and is consistent with other studies. Third, the assessment of patient satisfaction was subjective and open to influence by a placebo effect. Nonetheless, the results align with the objective assessments made using skinfold thickness.
5. CONCLUSIONS
This study showed that multiple cycles/sessions of CoolSculpting can safely improve overall treatment benefit in body contouring. Decreases in skinfold thickness were greater than has typically been observed in previous studies, 4 and rates of patient satisfaction were also high. Cryolipolysis may offer a nonsurgical alternative to traditional liposuction in many instances. This approach warrants further study in controlled trials.
CONFLICT OF INTEREST
Darren J. McKeown has been a consultant for Allergan. Joanne Payne reports nothing to disclose.
ACKNOWLEDGMENTS
The authors thank Dr Timothy Ryder from Biological Communications Limited (London, UK) for assistance in editing and submitting the final draft, funded by Allergan at the request of the investigator. Neither honoraria nor payments were made for authorship.
McKeown DJ, Payne J. Significant improvement in body contour with multiple cycles of CoolSculpting: Results of a prospective study. Dermatologic Therapy. 2021;34:e14850. 10.1111/dth.14850
[The copyright line for this article was changed on 9 March 2021 after original online publication.]
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- 1. Manstein D, Laubach H, Watanabe K, Farinelli W, Zurakowski D, Anderson RR. Selective cryolysis: a novel method of non‐invasive fat removal. Lasers Surg Med. 2008;40:595‐604. [DOI] [PubMed] [Google Scholar]
- 2. Avram MM, Harry RS. Cryolipolysis for subcutaneous fat layer reduction. Lasers Surg Med. 2009;41:703‐708. [DOI] [PubMed] [Google Scholar]
- 3. Zelickson B, Egbert BM, Preciado J, et al. Cryolipolysis for noninvasive fat cell destruction: initial results from a pig model. Dermatol Surg. 2009;35:1462‐1470. [DOI] [PubMed] [Google Scholar]
- 4. Ingargiola MJ, Motakef S, Chung MT, Vasconez HC, Sasaki GH. Cryolipolysis for fat reduction and body contouring: safety and efficacy of current treatment paradigms. Plast Reconstr Surg. 2015;135:1581‐1590. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Klein KB, Bachelor EP, Becker EV, Bowes LE. Multiple same day cryolipolysis treatments for the reduction of subcutaneous fat are safe and do not affect serum lipid levels or liver function tests. Lasers Surg Med. 2017;49:640‐644. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Meyer PF, Davi Costa E, Silva J, Santos de Vasconcellos L, et al. Cryolipolysis: patient selection and special considerations. Clin Cosmet Investig Dermatol. 2018;11:499‐503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. CoolSculpting . The innovative science of CoolSculpting. 2018. https://int.coolsculptinghcp.com/uk/#. Accessed 15 October 2020.
- 8. Dierickx CC, Mazer JM, Sand M, Koenig S, Arigon V. Safety, tolerance, and patient satisfaction with noninvasive cryolipolysis. Dermatol Surg. 2013;39:1209‐1216. [DOI] [PubMed] [Google Scholar]
- 9. Stevens WG, Pietrzak LK, Spring MA. Broad overview of a clinical and commercial experience with CoolSculpting. Aesthet Surg J. 2013;33:835‐846. [DOI] [PubMed] [Google Scholar]
- 10. Zelickson BD, Burns AJ, Kilmer SL. Cryolipolysis for safe and effective inner thigh fat reduction. Lasers Surg Med. 2015;47:120‐127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Kilmer SL, Burns AJ, Zelickson BD. Safety and efficacy of cryolipolysis for non‐invasive reduction of submental fat. Lasers Surg Med. 2016;48:3‐13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Jain M, Savage NE, Spiteri K, Snell BJ. A 3‐dimensional quantitative analysis of volume loss following submental cryolipolysis. Aesthet Surg J. 2020;40:123‐132. [DOI] [PubMed] [Google Scholar]
- 13. Shek SY, Chan NP, Chan HH. Non‐invasive cryolipolysis for body contouring in Chinese: a first commercial experience. Lasers Surg Med. 2012;44:125‐130. [DOI] [PubMed] [Google Scholar]
- 14. Pinto HR, Garcia‐Cruz E, Melamed GE. A study to evaluate the action of lipocryolysis. Cryo Letters. 2012;33:177‐181. [PubMed] [Google Scholar]
- 15. Talasila S, Evers‐Meltzer R, Xu S. Social media ratings of minimally invasive fat reduction procedures: benchmarking against traditional liposuction. Dermatol Surg. 2018;44:971‐975. [DOI] [PubMed] [Google Scholar]
- 16. Singh SM, Geddes ER, Boutrous SG, et al. Paradoxical adipose hyperplasia secondary to cryolipolysis: an underreported entity? Lasers Surg Med. 2015;47:476‐478. [DOI] [PubMed] [Google Scholar]
- 17. Kelly E, Rodriguez‐Feliz J, Kelly ME. Paradoxical adipose hyperplasia after cryolipolysis: a report on incidence and common factors identified in 510 patients. Plast Reconstr Surg. 2016;137:639e‐640e. [DOI] [PubMed] [Google Scholar]
- 18. Stroumza N, Gauthier N, Senet P, Moguelet P, Nail Barthelemy R, Atlan M. Paradoxical adipose hypertrophy (PAH) after cryolipolysis. Aesthet Surg J. 2018;38:411‐417. [DOI] [PubMed] [Google Scholar]
- 19. Ho D, Jagdeo J. A systematic review of paradoxical adipose hyperplasia (PAH) post‐cryolipolysis. J Drugs Dermatol. 2017;16:62‐67. [PubMed] [Google Scholar]
- 20. Wang E, Kaur R, Jagdeo J. Commentary on: paradoxical adipose hypertrophy (PAH) after cryolipolysis. Aesthet Surg J. 2018;38:418‐420. [DOI] [PubMed] [Google Scholar]
- 21. Khan M. Complications of cryolipolysis: paradoxical adipose hyperplasia (PAH) and beyond. Aesthet Surg J. 2019;39:NP334‐NP342. [DOI] [PubMed] [Google Scholar]
- 22. Kelly ME, Rodríguez‐Feliz J, Torres C, Kelly E. Treatment of paradoxical adipose hyperplasia following cryolipolysis: a single‐center experience. Plast Reconstr Surg. 2018;142:17e‐22e. [DOI] [PubMed] [Google Scholar]
- 23. CoolSculpting . About CoolSculpting. 2016. www.coolsculpting.com/pdfs/CoolSculpting_Important_Safety_Information_IC02192-A.pdf. Accessed 15 October 2020.
- 24. Loap S, Lathe R. Mechanism underlying tissue cryotherapy to combat obesity/overweight: triggering thermogenesis. J Obes. 2018;2018:5789647. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.