

Summary
Although new multiple myeloma (MM) therapies are effective in alleviating some disease‐associated symptoms (e.g. bone pain, fatigue, functional decline), they can result in additional toxicities, further impacting health‐related quality of life (HRQoL). Here, we compared HRQoL and safety of lenalidomide‐bortezomib‐dexamethasone [RVd (n = 445)], bortezomib‐melphalan‐prednisone [VMP (n = 77)] and Vd or VMP (n = 588) in patients with newly diagnosed MM (NDMM) from the Connect® MM Registry, a large, USA, multicentre, prospective observational cohort study. Functional Assessment of Cancer Therapy‐Multiple Myeloma subscale, EuroQol‐5D overall score and Bone Pain Inventory HRQoL scores were significantly improved with RVd versus Vd/VMP. Serious adverse event rates were similar in all groups. Treatment with RVd maintained HRQoL in this real‐world, largely community‐based population of patients with NDMM.
Keywords: health‐related quality of life, lenalidomide, multiple myeloma, real‐world evidence
Introduction
Health‐related quality of life (HRQoL) can be impaired in patients with multiple myeloma (MM) from the time of diagnosis. Compared with reference populations or those with other haematological malignancies, patients with MM have a notably higher symptom and psychological burden due to bone involvement, fatigue, mood disturbances, bacterial infections, impaired renal function and anaemia. 1 , 2 , 3 , 4 Thus, patient‐reported HRQoL assessment adds an important dimension to study endpoints, providing information on treatment tolerability from a patient perspective. 5 The growing importance of considering patient HRQoL as a clinical endpoint in MM is further underscored by the recent publication of the American Society of Clinical Oncology/Cancer Care Ontario Joint Clinical Practice Guideline. It recommends that QoL assessment including symptom management and treatment tolerability should be assessed at each visit in transplant‐ineligible patients to determine whether therapeutic goals are being maintained/met, and that this should influence the intensity and duration of treatment. 6
For fit patients with newly diagnosed MM (NDMM) with or without immediate stem cell transplant (SCT) intent, lenalidomide‐bortezomib‐dexamethasone (RVd) is a standard‐of‐care in the United States per National Comprehensive Cancer Network Clinical Practice Guidelines (NCCN Guidelines®). 7 The NCCN Guidelines are the recognised standard for clinical direction and policy in cancer care. Recently, RVd has also been approved in Europe for adult patients with previously untreated MM who are ineligible for transplant. The efficacy and safety of this triplet therapy was established by results from the randomised, open‐label, Phase III Southwest Oncology Group (SWOG) S0777 trial in which RVd was associated with a higher response rate (82% vs. 72%) and significantly longer progression‐free survival (PFS) versus lenalidomide‐dexamethasone [Rd; median 41 months vs. 29 months; hazard ratio (HR) 0·742; P = 0·003]. 8 , 9 While RVd is a standard‐of‐care for transplant‐ineligible patients in the United States, melphalan‐prednisone‐thalidomide (MPT) and bortezomib‐melphalan‐prednisone (VMP) are common induction regimens used in Europe. 10
Few community‐based studies have reported the effects on HRQoL with regimens in patients with NDMM without transplant intent to date. One example is the USA community‐based Phase IIIb UPFRONT trial (ClinicalTrials.gov Identifier: NCT00507416), where HRQoL of three bortezomib‐based induction regimens [bortezomib‐dexamethasone (Vd), bortezomib‐thalidomide‐dexamethasone (VTd) and VMP] in patients with transplant‐ineligible NDMM was studied. 11 Mean global health status, as measured by the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC‐QLQ C30), briefly decreased during induction with all regimens (with largest reduction observed in patients with VTd), followed by improvement or stabilisation of symptoms during maintenance therapy. The authors concluded that this reflected treatment‐associated toxicities during induction, followed by the positive impact of response during maintenance. In that study, individual functioning and symptom scores failed to improve or stabilise for cognitive functioning, nausea and vomiting, and diarrhoea.
The Connect® MM Registry (NCT01081028) is a large, USA, multicentre, prospective observational cohort study of patients with NDMM designed to examine real‐world diagnostic patterns, 12 treatment patterns, 13 clinical outcomes, 14 and HRQoL patient‐reported outcomes in patients with NDMM. 15 Approximately 84% of patients are enrolled from community sites, thereby reflecting the heterogeneity observed in routine clinical practice. 14 The Registry provides an opportunity to assess the impact of commonly used regimens on HRQoL in a real‐world setting. Thus, we evaluated the effect of initial treatment on changes in HRQoL and safety in patients with NDMM without immediate SCT intent, comparing a USA standard of care (RVd) versus current standard European treatment regimens with adequate patient numbers in this USA registry (Vd, VMP). 16 , 17
Methods
Study design and patient population
The study design and patient population of the Connect MM Registry have previously been described in detail. 12 Eligible patients were aged ≥18 years and had symptomatic MM diagnosed as defined by the International Myeloma Working Group criteria 18 within 2 months prior to enrolment. No exclusion criteria were applied. Patients with NDMM were enrolled from 250 community, academic and government sites: Cohort 1 (n = 1493) from September 2009 to December 2011, Cohort 2 (n = 1518) from December 2012 to April 2016. The gap in enrolments between cohorts was not planned, the decision to begin enrolment for Cohort 2 was made a year after completion of enrolment for Cohort 1, and reflects the same inclusion criteria. To minimise bias, enrolment was competitive, and consecutive patients with MM presenting to the sites were evaluated for potential enrolment. The median time from diagnosis to enrolment was 25 days.
The Connect MM Registry is non‐interventional, with all medical care performed solely at the discretion of the treating clinician in accordance with standard clinical practice at each site. Participation is voluntary and patients can withdraw at any time without affecting their ongoing medical care. Patients are followed‐up for treatment and outcomes until early discontinuation or end of study, expected in 2024. All patients were required to provide written informed consent. The Connect MM Registry was approved by a central Institutional Review Board (IRB; Advarra, Columbia, MD, USA) or the IRB at the individual study site.
HRQoL assessments
This analysis focussed on the subset of treated patients who had HRQoL assessments and no SCT (to avoid gaps in HRQoL data collection and remove the potential bias of adverse effects of SCT on HRQoL 19 ) before quarter (Q) 4 of patient follow‐up (with a window of ± 1·5 months at 12 months), untreated patients (n = 69) and those without HRQoL assessments (n = 61) were excluded. Patients who received initial treatment with RVd were compared with those who received VMP or those who received Vd or VMP (Vd/VMP). Patients included in the analysis were followed starting from study baseline (first treatment dose date) to the minimum (Q4, end date of first induction, progressive disease, death, discontinuation, data cut‐off), and HRQoL was obtained quarterly within this period.
The HRQoL data were collected using the Functional Assessment of Cancer Therapy‐Multiple Myeloma (FACT‐MM) and the Brief Pain Inventory (BPI). Health utilities were assessed using the EuroQol‐5D (EQ‐5D) overall index. The FACT‐MM questionnaire comprises four core subscales measuring emotional, social/family and functional well‐being. FACT‐MM includes a 14‐item subscale measuring MM‐specific concerns. 4 The 28‐item FACT‐MM Trial Outcome Index (TOI) includes FACT subscales measuring physical and functional well‐being and the FACT‐MM subscale. Items are rated on a scale of 1–4 (‘Not at all’–‘Very much’) based on the past 7 days. The nine‐item BPI measures severity of pain and its effect on functioning on a scale of 1–10 (‘No pain’–‘Pain as bad as you can imagine’). 20 The EQ‐5D overall index questionnaire defines health status using five dimensions: ‘Mobility’, ‘Self‐Care’, ‘Usual Activities’, ‘Pain/Discomfort’ and ‘Anxiety/Depression’. Summary assessments use a visual analogue scale of 0–100 (‘worst imaginable’–‘best imaginable health statue’) and an index score representing level of perceived problems, with level 1 = no problems, level 2 = some problems and level 3 = extreme problems.
Statistical analysis
Changes in HRQoL during Q1–4 of initial treatment and safety [serious adverse events (SAEs)] were compared across treatment groups.
Mixed‐effect model repeated measures (MMRM) with inverse probability weighting (IPW) using propensity scores was used to analyse differences in HRQoL scores change‐from‐baseline between treatment groups. Multiple imputation method was used to mitigate missing data on baseline covariates before using them to generate propensity scores. The baseline covariates used were: age group, cohort, income level, transplant intent, Eastern Cooperative Oncology Group Performance Status (ECOG PS), hypertension medical history (MH), diabetes MH, other relevant MHs, and creatinine and platelet levels.
Statistically significant differences in HRQoL scores do not necessarily translate into clinically meaningful changes for patients. The minimal clinically important difference (MCID) score has been developed to incorporate statistical validity and patient‐derived perception of QoL change 21 , 22 and is defined as the smallest difference in the HRQoL score from a treatment outcome that a patient identifies as important and beneficial, which would mandate a change in the patient’s management. 23 Because different instruments were used for HRQoL assessment and the ranges of these HRQoL scores obtained were different, values were normalised to MCID units. Further, since BPI changes reflecting improvement carry a negative value, we considered improvements in HRQoL instead of just a differential scale.
Results
As of 7 January 2019, 2942 patients had been treated. Of these, 1895 patients without immediate SCT within Q4 had HRQoL assessments. In this group, 445 had received RVd, 77 had received VMP, 511 had received Vd, 21 had received VTd [not included in analysis due to small sample size and potential dilution of observed effects (due to presence of thalidomide) versus RVd], and 609 had received other treatments. The median (range) duration of first induction therapy in first line was 5·4 (0·1–99·6) months for RVd, 5·8 (0·4–71·4) months for VMP, and 4·5 (0·01–107·4) months for Vd or VMP. Baseline characteristics were generally similar among included treatment groups except that patients receiving RVd were younger than those receiving VMP and VMP/Vd I. The EQ‐5D completion rates, defined as five/five questions answered, were similar among treatment groups [1‐year: 71·1% (RVd) vs. 79·7% (VMP) vs. 66·7% (Vd/VMP)] Table II.
Table I.
Baseline characteristics.
| Characteristic | RVd (n = 445) | Vd/VMP (n = 588) | VMP (n = 77) |
|---|---|---|---|
| Age, years | |||
| Median (range) | 67 (35–90) | 74 (32–94) | 76 (52–91) |
| <65, n (%) | 182 (40·9) | 134 (22·8) | 6 (7·8) |
| 65 to <75, n (%) | 163 (36·6) | 181 (30·8) | 22 (28·6) |
| ≥75 years, n (%) | 100 (22·5) | 273 (46·4) | 49 (63·6) |
| Men, n (%) | 262 (58·9) | 333 (56·6) | 39 (50·6) |
| Race, n (%) | |||
| White | 365 (82·0) | 485 (82·5) | 68 (88·3) |
| Black | 63 (14·2) | 85 (14·5) | 7 (9·1) |
| ECOG PS, n (%) | |||
| 0–1 | 288 (64·7) | 338 (57·5) | 40 (51·9) |
| 2–3 | 59 (13·3) | 94 (16·0) | 14 (18·2) |
| Not specified | 98 (22·0) | 154 (26·2) | 21 (27·3) |
| Calculated ISS stage, n (%) | |||
| I | 67 (15·1) | 63 (10·7) | 10 (13·0) |
| II | 130 (29·2) | 143 (24·3) | 24 (31·2) |
| III | 111 (24·9) | 206 (35·0) | 22 (28·6) |
| Unknown* | 137 (30·8) | 176 (29·9) | 21 (27·3) |
| IMWG risk 24 | |||
| Low | 20 (4·5) | 11 (1·9) | 0 (0·0) |
| Standard | 234 (52·6) | 301 (51·2) | 40 (51·9) |
| High | 52 (11·7) | 43 (7·3) | 7 (9·1) |
| Missing/not specified | 139 (31·2) | 233 (39·6) | 30 (39·0) |
| Calcium ≥115 mg/l, n (%) | 43 (9·7) | 49 (8·3) | 6 (7·8) |
| Creatinine >20 mg/l, n (%) | 73 (16·4) | 169 (28·7) | 16 (20·8) |
| Hb <100 g/l or >20 g/l <LLN, n (%) | 217 (48·8) | 305 (51·9) | 37 (48·1) |
| MM bone involvement, n (%) | 351 (78·9) | 432 (73·5) | 60 (77·9) |
ECOG PS, Eastern Cooperative Oncology Group Performance Status; Hb, haemoglobin; IMWG, International Myeloma Working Group; ISS, International Staging System; RVd, lenalidomide‐bortezomib‐dexamethasone; Vd, bortezomib‐dexamethasone; VMP, bortezomib‐melphalan‐prednisone.
Data not specified/provided.
Table II.
Quarterly health‐related quality of life (HRQoL) completion rates through to 12 months.
| n/N (%)* | EQ‐5D overall index | ||
|---|---|---|---|
|
RVd (n = 445) |
VMP (n = 77) |
Vd/VMP (n = 588) |
|
| Baseline | 369/445 (82·9) | 66/77 (85·7) | 491/588 (83·5) |
| Q1 | 367/439 (83·6) | 65/77 (84·4) | 471/577 (81·6) |
| Q2 | 295/407 (72·5) | 59/70 (84·3) | 375/514 (73·0) |
| Q3 | 266/378 (70·4) | 47/64 (73·4) | 345/471 (73·2) |
| Q4 | 258/363 (71·1) | 47/59 (79·7) | 297/445 (66·7) |
RVd, lenalidomide‐bortezomib‐dexamethasone; Vd, bortezomib‐dexamethasone; VMP, bortezomib‐melphalan‐prednisone.
Completion rates were defined as five/five questions answered.
Comparing initial treatment groups, statistically significant improvements were noted in HRQoL with RVd versus Vd/VMP for the FACT‐MM subscale, EQ‐5D overall score and BPI indices Fig 1 . The FACT‐MM scores and EQ‐5D overall scores were not significantly different between the RVd versus VMP groups, although RVd significantly improved BPI scores compared with VMP (P = 0·0023).
Fig 1.
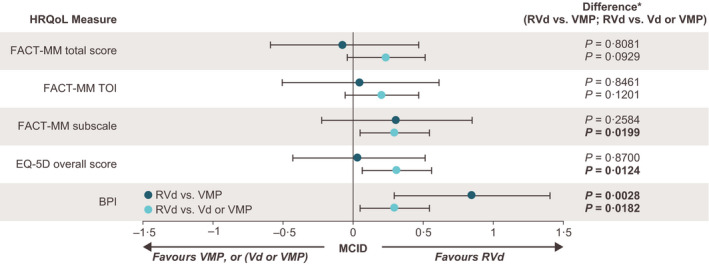
Changes in health‐related quality of life (HRQoL) assessments during Q1–4 of initial treatment. BPI, Brief Pain Inventory; EQ‐5D, EuroQol‐5D; FACT‐MM, Functional Assessment of Cancer Therapy‐Multiple Myeloma; FACT‐MM TOI, FACT‐MM Trial Outcome Index; MCID, minimally important clinical difference; Q, quarter;. Legend text: MCIDs for HRQoL indices are 13·0‐point increase for FACT‐MM total, 11·0‐point increase for FACT‐MM TOI, 6·0‐point increase for FACT‐MM subscale, 0·1‐point increase for EQ‐5D overall score, and 1·5‐point decrease for BPI (lower values indicate improved HRQoL). *Results are based on mixed‐effect model, repeat measurement analysis adjusted by propensity score. Nominal P values are reported without adjustments for multiple testing.
Recorded SAEs occurred similarly among initial treatment groups Table III. Incidence rates of SAEs by system organ class were also similar in all treatment groups. Blood and lymphatic disorder SAEs were more frequent in the RVd group than in the Vd/VMP group (5·2% vs. 1·4%), whereas cardiac disorder SAEs were more common in the Vd/VMP group than in the RVd group (5·8% vs. 2·0%). The rates of treatment discontinuation due to AEs were similar for patients receiving RVd (16·8%) and Vd/VMP (18·9%), but were slightly higher for patients receiving VMP alone (24·7%). The rates of discontinuation due to death were generally similar between the treatment groups (RVd: 4·0%, VMP: 7·8%, Vd/VMP: 6·8%).
Table III.
Serious adverse events (≥2% of patients) by initial treatment.
| System organ class event, n (%)* |
RVd (n = 445) |
Vd/VMP (n = 588) |
VMP (n = 77) |
|---|---|---|---|
| Patients with ≥1 specified event | 200 (44·9) | 234 (39·8) | 34 (44·2) |
| Blood and lymphatic system disorders | 23 (5·2) | 8 (1·4) | 3 (3·9) |
| Cardiac disorders | 9 (2·0) | 34 (5·8) | 3 (3·9) |
| Gastrointestinal disorders | 18 (4·0) | 33 (5·6) | 4 (5·2) |
| General disorders and administration site conditions | 37 (8·3) | 35 (6·0) | 4 (5·2) |
| Infections and infestations | 74 (16·6) | 67 (11·4) | 14 (18·2) |
| Injury, poisoning and procedural complications | 11 (2·5) | 13 (2·2) | 3 (3·9) |
| Metabolism and nutrition disorders | 23 (5·2) | 21 (3·6) | 2 (2·6) |
| Musculoskeletal and connective tissue disorders | 18 (4·0) | 17 (2·9) | 5 (6·5) |
| Neoplasms benign, malignant and unspecified (including cysts and polyps) | 23 (5·2) | 21 (3·6) | 2 (2·6) |
| Nervous system disorders | 27 (6·1) | 23 (3·9) | 0 (0) |
| Renal and urinary disorders | 15 (3·4) | 28 (4·8) | 2 (2·6) |
| Respiratory, thoracic and mediastinal disorders | 35 (7·9) | 30 (5·1) | 2 (2·6) |
| Vascular disorders | 15 (3·4) | 14 (2·4) | 2 (2·6) |
RVd, lenalidomide‐bortezomib‐dexamethasone; Vd, bortezomib‐dexamethasone; VMP, bortezomib‐melphalan‐prednisone.
Numbers do not add up to the overall due to each patient having multiple adverse events.
Discussion
The present analysis is the first providing real‐world evidence on the effects of commonly used regimens on HRQoL in patients with NDMM without immediate SCT intent. In the present analysis of the Connect MM Registry, initial treatment of MM with RVd maintained HRQoL versus regimens commonly used as initial treatment in Europe. Among HRQoL measures, the FACT‐MM subscale, BPI indices and the EQ‐5D overall score were significantly improved with RVd during Q1–4 of initial treatment compared with Vd/VMP. Improved FACT‐MM total score and FACT‐MM TOI were observed in the RVd group versus the Vd/VMP groups; however, the difference was non‐significant. Although different instruments were used to assess HRQoL, our present findings are similar to previous reports of improved HRQoL with the RVd induction regimen among clinical trials in patients with MM. 25 , 26 , 27 In young (≤65 years) patients with NDMM from the Phase III IFM/DFCI 2009 trial (ClinicalTrials.gov Identifier: NCT01191060) who did not receive SCT, domains from the EORTC QLQ‐C30 and EORTC QLQ‐MY20 instruments that were suboptimal at baseline were significantly improved (P < 0·05) at the end of induction with RVd treatment. 27 This study also identified improvements from baseline in global HRQoL, physical functioning, role functioning, pain and disease symptoms following RVd treatment. In another Phase II trial of transplant‐ineligible patients with MM, a modified regimen of RVd (RVd lite) significantly improved physical functioning (P = 0·013), future perspective (P = 0·023) and disease symptoms (P = 0·001) compared with baseline. 26 Similarly, global health status, as assessed by EORTC scores, improved compared with baseline, although the difference was not statistically significant. Collectively, RVd has not been associated with significant impairments in patient‐reported HRQoL and may be associated with improved MM‐related symptoms.
During HRQoL assessment, the EQ‐5D completion rates dropped from Q1 through to Q4; in Q1, 369 of the 445 patients (82·9%) completed the EQ‐5D, and the frequency dropped to 258 of 363 patients (71·1%) completing the EQ‐5D at the end of Q4. The drop in the EQ‐5D completion rates from Q1 through to Q4 can be attributed to: (i) patients (n = 86) who were no longer in the cohort as a result of treatment discontinuation, death, progressive disease or change in regimen, and (ii) patients (n = 106) who remained in the cohort but did not provide EQ‐5D assessment forms. The decrease in EQ‐5D completion rates from Q1 to Q4 was similar across treatment groups except for VMP, which was a smaller cohort (n = 77). Finally, patients who received RVd were generally younger than those who received VMP or Vd/VMP (median age 67 vs. 76/74 years), and as a result, may have fewer comorbidities and overall better health, which may have contributed to the observed differences in HRQoL.
The rate of SAEs was similar with all three regimens (RVd, Vd, Vd/VMP) and patient HRQoL was maintained within the groups. Completion of induction regimen and toxicity were the common reasons for discontinuing treatment for all three treatment groups and occurred with similar frequencies; rates of treatment discontinuations due to death were also similar within the groups. In the SWOG S0777 trial, 23% patients receiving RVd as induction treatment discontinued because of AEs (vs. 10% in the Rd arm), which could be attributable to the higher occurrence of Grade ≥3 AEs (particularly neurological toxicities) in the RVd arm versus the Rd arm (33% vs. 11%; P < 0·0001). 8 In the community‐based UPFRONT study, SAEs occurred in 47% of patients during induction with VMP and in 48% of patients during induction with Vd, 11 which was comparable to that observed in the present analysis. However, in melphalan‐containing regimens, such as VMP, myelosuppression and risk of secondary malignancies attributed to melphalan along with its safety profile limit its duration of use. 11 , 28 In the UPFRONT trial, incidence of haematological AEs was generally higher in patients receiving VMP, compared with VTd or Vd, and the rate of discontinuation due to AEs was 38% in the VTd arm, 29% in the Vd arm, and 34% in the VMP arm. 11
Findings from the present analysis provide meaningful real‐world evidence on the effects of initial treatment choice on HRQoL for patients with NDMM without immediate SCT intent. In interpreting these results, however, the well‐known limitations of real‐world studies must be acknowledged. Patients were not randomised to treatment, no protocol‐mandated specific treatments or formal response assessment criteria were applied, the collection of AE data was limited (e.g. AE grades were collected only for events of special interest starting in 2012 and not for the entire duration of the study), and treatment durations and intensities varied. Also, the Connect MM Registry is geographically restricted to the United States and is not a global study. As in any observational study, the potential exists for missing or erroneous data because monitoring of individual sites for data verification is limited. However, to address this issue, the Connect MM Registry has the ability to query sites for more information on questionable or missing data; the use of multiple imputation methods in the analyses also mitigates the impact of missing data. The rate of HRQoL assessment completion was also high at baseline and remained so through to Q4, despite the study being non‐interventional. Although the present analysis did not address the association between baseline patient characteristics and HRQoL, it accounted for baseline variables in propensity score generation when analysing change‐from‐baseline HRQoL scores between treatment groups. Moreover, previously published data from this Registry have shown the associations of some baseline patient and disease characteristics on HRQoL. 29 , 30 , 31 , 32 Finally, a potential selection factor between the treatment populations is based on the typical use of doublets like Vd in frail, older patients in the USA who cannot tolerate triplet regimens such as RVd. Despite these limitations, the Connect MM Registry, which is one of the largest prospective cohort studies of patients with MM, including those from multiple geographically diverse (e.g. 49 USA States) and predominantly community‐based centres, provides important insights into the real‐world experiences of patients.
In conclusion, these real‐world data from the Connect MM Registry demonstrate that induction treatment with RVd in patients with NDMM without SCT intent maintains HRQoL compared with the induction regimens, VMP or Vd/VMP, which have been commonly used in Europe. These data also support the potential use of HRQoL assessments to inform treatment decisions at baseline or, if HRQoL appears to decline during treatment, adjustments to the treatment regimen. With the recent approval of RVd by the European Commission for transplant‐ineligible patients with previously untreated MM, HRQoL data from a real‐world setting will provide further guidance for the use of this regimen in community‐based practices.
Conflicts of interest
This study was funded by Celgene Corporation, and is currently supported by Bristol Myers Squibb. Rafat Abonour: member of steering committees for Celgene, a Bristol Myers Squibb Company and Takeda, research funding from Celgene, a Bristol Myers Squibb Company, Takeda and Prothena. Robert M. Rifkin: consultancy services to Amgen, Boehringer Ingelheim, Celgene, a Bristol Myers Squibb Company, EMD Serono, Sandoz and Takeda and owns stock with McKesson. Cristina Gasparetto: honoraria from Janssen, Bristol Myers Squibb, Celgene, a Bristol Myers Squibb Company and Takeda; provided consultancy services to Janssen, Bristol Myers Squibb and Celgene, a Bristol Myers Squibb Company; travel reimbursement from Janssen, Bristol Myers Squibb and Celgene, a Bristol Myers Squibb Company; and research funding from Celgene. Kathleen Toomey: consultancy services to Celgene, a Bristol Myers Squibb Company. Brian G. M. Durie: consultancy services to Takeda and Janssen. James W. Hardin: consultancy services to Celgene, a Bristol Myers Squibb Company. Howard R. Terebelo: consultancy services to Celgene, a Bristol Myers Squibb Company and participated in speakers’ bureaus for Janssen, Takeda and Pharmacyclics LLC, an AbbVie Company. Sundar Jagannath: consultancy services to Celgene, a Bristol Myers Squibb Company, Bristol Myers Squibb, Novartis and Merck and speakers’ bureaus for MMRF and Medicom. Mohit Narang: consultancy services and speakers’ bureaus for Celgene, a Bristol Myers Squibb Company and speakers’ bureaus for Janssen. Sikander Ailawadhi: consultancy services to Takeda, Novartis, Celgene, a Bristol Myers Squibb Company and Amgen, and research funding from Pharmacyclics, LLC, an AbbVie Company. James L. Omel: honoraria from Takeda Oncology and Celgene, a Bristol Myers Squibb Company, and on the board of directors/advisory committee for Takeda Oncology and Celgene, a Bristol Myers Squibb Company. Hans C. Lee: consultancy services for Adaptive Biotechnologies, Amgen, Celgene, a Bristol Myers Squibb Company, GlaxoSmithKline, Janssen, Sanofi and Takeda Pharmaceutical, and research funding from Amgen, Celgene, a Bristol Myers Squibb Company, Daiichi Sankyo, Eutropics Pharmaceuticals, GlaxoSmithKline, Janssen Pharmaceutical and Takeda Pharmaceutical. Shankar Srinivasan, Amani Kitali and Amit Agarwal: employed by Bristol Myers Squibb. Lynne Wagner: consultancy services to EveryFit, Gilead and Janssen.
Acknowledgements
The authors thank the patients and their families, nurses, study personnel and investigators who participated in the Connect MM Registry. The authors acknowledge Liang Liu for assistance with statistical analyses and Jay Cao, Fei Tan, David Wang and Rick Soong for programming support. Maryann Obiorah, PhD provided editorial assistance to the authors during the preparation of this manuscript, supported by funding from Bristol Myers Squibb. All authors contributed to the acquisition, analysis or interpretation of data for this article and drafts of the article; revised the manuscript critically for important intellectual content; approved the final version to be published; and agreed to be accountable for all aspects of the article.
References
- 1. Gulbrandsen N, Hjermstad MJ, Wisløff F, Nordic Myeloma Study Group . Interpretation of quality of life scores in multiple myeloma by comparison with a reference population and assessment of the clinical importance of score differences. Eur J Haematol. 2004;72:172–80. [DOI] [PubMed] [Google Scholar]
- 2. Johnsen AT, Tholstrup D, Petersen MA, Pedersen L, Groenvold M. Health related quality of life in a nationally representative sample of haematological patients. Eur J Haematol. 2009;83:139–48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Robinson D Jr, Esseltine DL, Regnault A, Meunier J, Liu K, van de Velde H. The influence of baseline characteristics and disease stage on health‐related quality of life in multiple myeloma: findings from six randomized controlled trials. Br J Haematol. 2016;174:368–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Wagner LI, Robinson D Jr, Weiss M, Katz M, Greipp P, Fonseca R, et al. Content development for the functional assessment of cancer therapy‐multiple myeloma (FACT‐MM): use of qualitative and quantitative methods for scale construction. J Pain Symptom Manage. 2012;43:1094–104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Thanarajasingam G, Minasian LM, Baron F, Cavalli F, De Claro RA, Dueck AC, et al. Beyond maximum grade: modernising the assessment and reporting of adverse events in haematological malignancies. Lancet Haematol. 2018;5:e563–98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Mikhael J, Ismaila N, Cheung MC, Costello C, Dhodapkar MV, Kumar S, et al. Treatment of Multiple Myeloma: ASCO and CCO Joint Clinical Practice Guideline. J Clin Oncol. 2019;37:1228–63. [DOI] [PubMed]
- 7. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Multiple Myeloma vol 2.2020. © National Comprehensive Cancer Network, Inc. 2019. All rights reserved. Accessed [March 10, 2020]. To view the most recent and complete version of the guideline, go online to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.
- 8. Durie BG, Hoering A, Abidi MH, Rajkumar SV, Epstein J, Kahanic SP, et al. Bortezomib with lenalidomide and dexamethasone versus lenalidomide and dexamethasone alone in patients with newly diagnosed myeloma without intent for immediate autologous stem‐cell transplant (SWOG S0777): a randomised, open‐label, phase 3 trial. Lancet. 2017;389:519–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Durie BG, Hoering A, Sexton R, Abidi MH, Epstein J, Rajkumar SV, et al. Longer Term Follow up of the  Randomized Phase III Trial SWOG S0777: Bortezomib, Lenalidomide and Dexamethasone Vs. Lenalidomide and Dexamethasone in Patients (Pts) with Previously Untreated Multiple Myeloma without an Intent for Immediate Autologous Stem Cell Transplant (ASCT). Blood. 2018;132 (Suppl 1):1992. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Paul B, Lipe B, Ocio EM, Usmani SZ. Induction therapy for newly diagnosed multiple myeloma. Am Soc Clin Oncol Educ Book. 2019;39:e176–86. [DOI] [PubMed] [Google Scholar]
- 11. Niesvizky R, Flinn IW, Rifkin R, Gabrail N, Charu V, Clowney B, et al. Community‐based Phase IIIB trial of three UPFRONT bortezomib‐based myeloma regimens. J Clin Oncol. 2015;33:3921–9. [DOI] [PubMed] [Google Scholar]
- 12. Rifkin RM, Abonour R, Terebelo H, Shah JJ, Gasparetto C, Hardin J, et al. Connect MM registry: the importance of establishing baseline disease characteristics. Clin Lymphoma Myeloma Leuk. 2015;15:368–76. [DOI] [PubMed] [Google Scholar]
- 13. Jagannath S, Abonour R, Durie BG, Gasparetto C, Hardin JW, Narang M, et al. Heterogeneity of second‐line treatment for patients with multiple myeloma in the Connect MM Registry (2010–2016). Clin Lymphoma Myeloma Leuk.2018;18:480–485.e3. [DOI] [PubMed]
- 14. Jagannath S, Abonour R, Durie BG, Narang M, Terebelo HR, Gasparetto CJ, et al. Impact of post‐ASCT maintenance therapy on outcomes in patients with newly diagnosed multiple myeloma in Connect MM. Blood Adv. 2018b;2:1608–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Abonour R, Wagner L, Durie BG, Jagannath S, Narang M, Terebelo HR, et al. Impact of post‐transplantation maintenance therapy on health‐related quality of life in patients with multiple myeloma: data from the Connect(R) MM Registry. Ann Hematol. 2018;97:2425–36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Ludwig H, Avet‐Loiseau H, Blade J, Boccadoro M, Cavenagh J, Cavo M, et al. European perspective on multiple myeloma treatment strategies: update following recent congresses. Oncologist. 2012;17:592–606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Moreau P, San Miguel J, Sonneveld P, Mateos MV, Zamagni E, Avet‐Loiseau H, et al. Multiple myeloma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow‐up. Ann Oncol. 2017;28:iv52–61. [DOI] [PubMed] [Google Scholar]
- 18. Kyle RA, Rajkumar SV. Criteria for diagnosis, staging, risk stratification and response assessment of multiple myeloma. Leukemia. 2009;23:3–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Chakraborty R, Hamilton BK, Hashmi SK, Kumar SK, Majhail NS. Health‐related quality of life after autologous stem cell transplantation for multiple myeloma. Biol Blood Marrow Transplant. 2018;24:1546–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Poquet N, Lin C. The brief pain inventory (BPI). J Physiother. 2016;62:52. [DOI] [PubMed] [Google Scholar]
- 21. King MT. A point of minimal important difference (MID): a critique of terminology and methods. Expert Rev Pharmacoecon Outcomes Res. 2011;11:171–84. [DOI] [PubMed] [Google Scholar]
- 22. Wright A, Hannon J, Hegedus EJ, Kavchak AE. Clinimetrics corner: a closer look at the minimal clinically important difference (MCID). J Man Manip Ther. 2012;20:160–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Pouchot J, Kherani RB, Brant R, Lacaille D, Lehman AJ, Ensworth S, et al. Determination of the minimal clinically important difference for seven fatigue measures in rheumatoid arthritis. J Clin Epidemiol. 2008;61:705–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Chng WJ, Dispenzieri A, Chim CS, Fonseca R, Goldschmidt H, Lentzsch S, et al. International Myeloma Working, G . IMWG consensus on risk stratification in multiple myeloma. Leukemia. 2014;28:269–77. [DOI] [PubMed] [Google Scholar]
- 25. O'Donnell EK, Laubach JP, Yee AJ, Chen T, Huff CA, Basile FG, et al. A phase 2 study of modified lenalidomide, bortezomib and dexamethasone in transplant‐ineligible multiple myeloma. Br J Haematol. 2018;182:222–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. O'Donnell EK, Laubach JP, Yee AJ, Redd R, Huff CA, Basile F, et al. Updated results of a Phase 2 study of modified lenalidomide, bortezomib, and dexamethasone (RVd‐lite) in transplant‐ineligible multiple myeloma. Blood. 2019;134:3178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Roussel M, Hebraud B, Hulin C, Perrot A, Caillot D, Macro M, et al. The impact of lenalidomide, bortezomib, and dexamethasone treatment on health‐related quality of life in transplant‐eligible patients with newly‐diagnosed multiple myeloma: results from the IFM/DFCI 2009 trial. Blood. 2018;132:716. [DOI] [PubMed] [Google Scholar]
- 28. Musto P, Anderson KC, Attal M, Richardson PG, Badros A, Hou J, et al. Second primary malignancies in multiple myeloma: an overview and IMWG consensus. Ann Oncol. 2017;28:228–45. [DOI] [PubMed] [Google Scholar]
- 29. Pashos CL, Durie BG, Rifkin RM, Terebelo HR, Abonour R, Toomey K, et al. Association of health‐related quality of life (HRQOL) with bone disease in multiple myeloma. Haematologica. 2011;96:S139–40. [Google Scholar]
- 30. Pashos CL, Durie BG, Rifkin RM, Shah JJ, Street TK, Sullivan KA, et al. Variation in health‐related quality of life (HRQOL) by ISS stage and ECOG status among multiple myeloma patients. Blood. 2010;116:3828.20668230 [Google Scholar]
- 31. Pashos CL, Durie BG, Rifkin R, Terebelo H, Gasparetto C, Mehta J, et al. Association of race with health‐related quality of life (HRQOL) among multiple myeloma patients. Blood. 2011a;118:5070. [Google Scholar]
- 32. Pashos CL, Durie BG, Rifkin R, Terebelo H, Gasparetto C, Mehta J, et al. Variation in health‐related quality of life (HRQOL) among multiple myeloma patients by insurance coverage. Blood. 2011;118:3150. [Google Scholar]