

Abstract
Background:
“Trap door” orbital floor fractures are usually seen in children. In the linear fracture type, a break occurs in the bones of the orbital floor that permits orbital tissue to prolapse into the fracture site during fracture formation. The bony fragments of the fracture then return to their original position, entrapping the prolapsed orbital tissue. In the hinged fracture type, the fractured part of the floor is minimally displaced into the maxillary sinus and acts as the hinge of a “swinging door” entrapping the orbital tissue.
Methods:
We report on a series of 10 adult patients with hinged orbital floor fractures.
Results:
The mean patient age was 35 years. Seven patients had a pure orbital floor fracture and the remaining 3 patients had fractures of both the orbital floor and the inferior orbital rim. All 10 patients had diplopia in the upgaze. None of the patients had signs of the oculocardiac reflex. None of the CT scans showed a “tear-drop” sign. However, the sagittal CT scans showed evidence of entrapment of the inferior rectus. All patients had a small area of a slightly depressed orbital floor at the site of entrapment, without a bony defect. All patients underwent surgery through an infraorbital incision and a titanium mesh was used in all patients. There were no postoperative complications. All patients regained full range of motion of the globe.
Conclusion:
This is the first series in the literature that reports on the characteristics and outcome of trap door orbital floor fractures in adults.
INTRODUCTION
“Trap door” orbital floor (blowout) fractures are classified into 2 types: the linear and the hinged fracture types.1 In the linear fracture type, a break occurs in the bones of the orbital floor that permits orbital tissue (the inferior rectus muscle or the inferior periorbital fat) to prolapse into the fracture site during fracture formation. The bony fragments of the fracture then return to their original position, entrapping the prolapsed orbital tissue and creating what is known as the “tear drop” sign. In the hinged fracture type, the fractured part of the floor is minimally displaced and acts as the hinge of a “swinging door” entrapping the orbital tissue. The latter type may be associated with minor comminution and the minor displacement creates a minor gap in the floor of the bony orbit (Fig. 1). Computed tomography (CT) scan findings of trap door fractures are known to be subtle.2–8 However, the tear drop sign in the linear fracture type is the main radiological evidence of entrapment. In the hinged fracture type, the change in the normal orientation of the inferior rectus muscle (which is best seen in the sagittal CT scan views) is the main radiological evidence of entrapment (Fig. 2).
Fig. 1.

A coronal cut in the orbit showing the entrapment by the hinged fracture. There is a gap; but no defect in the orbital floor.
Fig. 2.

A sagittal cut in the orbit showing the loss of the normal orientation of the inferior rectus muscle because of its entrapment in the “hinge” in hinged orbital floor fractures.
Trap door fractures have several characteristic features. First, they tend to occur in the pediatric population because of the distensibility of the immature facial bones.2 Second, besides the limitation in supraduction of the globe, they are known to be associated with signs of the oculocardiac reflex (bradycardia, nausea, and vomiting).3 Third, they occur only with pure (isolated orbital floor) blowout fractures in the pediatric population. Fourth, there is no significant injury of the periorbital soft tissue leading to a relatively “quiet eye.” This led some authors to name these fractures as the “white-eyed” orbital blowout fractures.4,5 Finally, the CT scan in pediatric patients usually show the tear drop sign.2,6–8
In this communication, we report on a unique series of 10 adult patients with trap door orbital floor fractures treated by the senior author (M.M.A.) over the last 20 years. The unique features of the series include: the age group of the patients (all were adults; 25–50 years old), the absence of the oculocardiac reflex in all cases, the occurrence of concurrent orbital rim fractures with severe periorbital soft-tissue injury in some cases, and the absence of the classic tear drop sign in the CT scan in all cases. We believe that the unique features of our series demonstrate for the first time in the literature that trap door blowout fractures in adults have different features from the classic pediatric trap door fractures.
PATIENTS AND METHODS
This is a retrospective review of all adult patients with trap door orbital floor fractures treated by the senior author over the last 20 years.
Patient Selection
All patients had orbital trauma with diplopia on upward gaze secondary to the entrapment of orbital tissue in the orbital floor, without the presence an orbital floor defect. The absence of an orbital floor defect qualified the patient to be included in the series.
Data Collection
Demographic data (age, sex, mechanism of injury, other concurrent injuries, and time of presentation to the author) were documented. Findings on examination were also documented with special attention to the presence of diplopia, forced duction test, enophthalmos, signs of oculocardiac reflex, the degree of periorbital soft-tissue injury, and sensory defects along the inferior orbital nerve distribution. The subtype of the orbital floor fracture (pure fractures involving the orbital floor only versus impure fractures involving both the inferior orbital rim and the orbital floor) was also documented along with the CT scan findings. The subtype of the trap door orbital floor fracture was also classified as per the classification of Gerbino et al1: Type I linear fracture type versus type II hinged fracture type. Finally, management, intraoperative findings, and outcome were documented.
RESULTS
There was a total of 10 cases. They were all males with a mean age of 35 years (range = 25–50 years). The fractures in all patients were sustained following a direct trauma by an object to the orbital area. All patients had unilateral injuries. There were no concurrent injuries outside the face in any of the patients. All patients presented to the senior author (M.M.A.) within 24 hours of injury. Seven patients had a pure orbital floor fracture (involving the orbital floor only), and the remaining 3 patients had fractures of both the orbital floor and the inferior orbital rim. The fractures in the latter 3 patients were isolated rim factures and were not a part of a zygomatic complex fracture. All 10 patients had diplopia in the upgaze (limited supraduction of the globe) only, with a positive forced duction test. None of the patients had enophthalmos or signs of the oculocardiac reflex. The 7 patients with pure fractures had minimal periorbital edema/ecchymosis, and there were no complaints of any sensory disturbances along the distribution of the inferior orbital nerve. In contrast, the 3 patients with impure fractures had evidence of significant soft-tissue injury (edema, hematoma, and ecchymosis) and numbness along the distribution of the inferior orbital nerve. CT scan findings of the orbital floor were subtle in all patients. None of the scans showed a tear-drop sign. All patients had a small area of a slightly depressed orbital floor at the site of entrapment, but without any orbital floor defect. The only radiological evidence of entrapment was the change in the normal orientation of the inferior rectus muscle in the sagittal CT scan cuts as demonstrated in Figure 2.
All patients underwent surgery (within 48 hours of injury) through an infraorbital incision. Intraoperative findings confirmed the trap door entrapment without the presence of a defect in the orbital floor. A small area of orbital floor depression with a hinge fracture was present in all patients. Hence, all 10 cases had Gerbino Type II fractures. In 5 patients, a linear orbital floor fracture was also seen adjacent to the depressed area in the floor. In pure fractures, the site of entrapment was at or just adjacent to the depressed area of the orbital floor. In these cases, release of the entrapped orbital tissue was done and the depressed part of the orbital floor was supported with a titanium mesh. The mesh was “wedged” (without fixation) between the borders of the depressed area in the orbital floor. In the 3 patients with concurrent orbital rim fractures, the area of depression and entrapment in the orbital floor was in the anterior part of the orbital floor. Following the reduction of the orbital rim fracture, the titanium mesh was used to stabilize the reduced orbital rim (using 1.5 mm self-tapping screws) and to support the depression in the anterior aspect of the orbital floor as demonstrated in Figure 3.
Fig. 3.
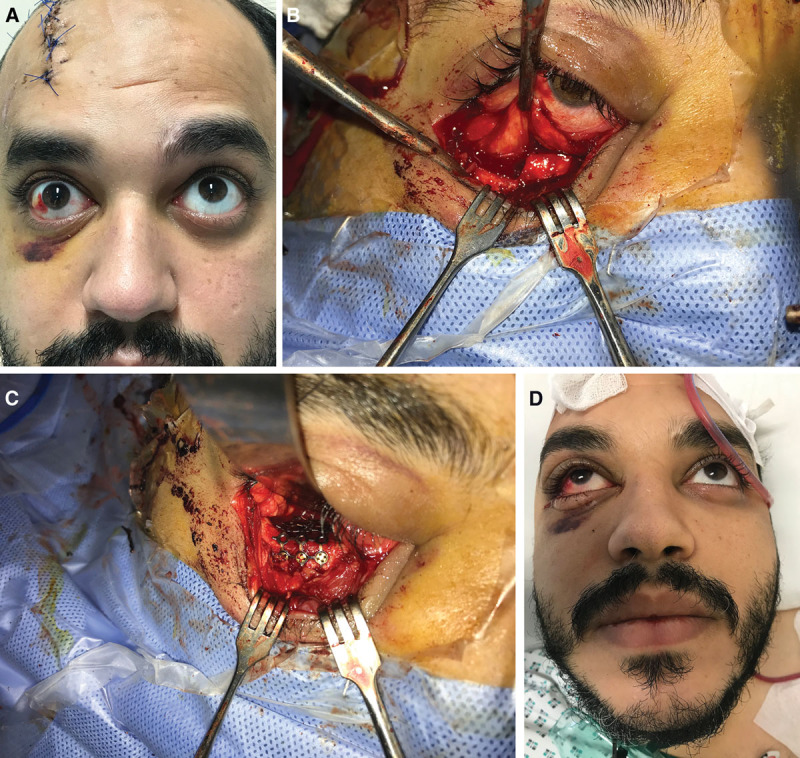
A demonstration of mesh application in a patient with an orbital rim fracture and an adjacent anterior floor trap door hinged blowout fracture. The patient fell from a significant height and also sustained a scalp laceration and a depressed skull fracture. This patient is a recent patient and is not included in the series, but is shown here to demonstrate the surgical technique. Combined plastic surgery and neurosurgery was done. A, Preoperative appearance with limitation of supraduction of the right orbit. B, Using a trans-conjunctival approach, the orbital rim fracture is subperiosteally dissected, and the entrapped orbital tissue is identified. C, The entrapped orbital tissue is released, the orbital rim fracture is reduced, and a titanium mesh is used to stabilize the reduced orbital rim (using 1.5 mm self-tapping screws) as well as to support the orbital floor. D, Immediate postoperative view showing the recovery of a normal supraduction of the eye (with complete resolution of the diplopia).
There were no postoperative complications. Follow-up ranged from 6 to 16 months (mean = 11 months). There was full range of motion of the globe in all patients, with no diplopia or enophthalmos. There was sensory recovery of the infraorbital nerve in the 3 patients with impure fractures. None of the patients developed hypertrophic scarring at the site of the infraorbital incision (Fig. 4). Two demonstrative examples (1 pure and 1 impure blowout fracture) are shown in Figures 4–6.
Fig. 4.

A case demonstration of a pure orbital floor trapdoor fracture. A, Preoperative sagittal CT scan showing a slightly depressed orbital floor (with no orbital floor defect and no tear drop sign) and entrapment of the inferior rectus. Note the loss of the normal orientation of the inferior rectus muscle (compare with Fig. 2). There is also entrapment of air in the orbital cavity just above the depressed orbital floor. B, Preoperative coronal CT scan view. Note the absence of the tear drop sign despite the presence of blood in the maxillary sinus. C, Preoperative 3D CT scan showing the intact orbital rim. D, Postoperative CT Scan showing the titanium mesh used to augment the area of depressed orbital floor after releasing the entrapped inferior rectus muscle. Note the receovery of the normal orientation of the inferior rectus muscle (compare with A).
Fig. 6.

A case demonstration of an impure (orbital rim and floor) fracture. A, Preoperative clinical photograph showing the severe periorbital soft-tissue injury and subcutaneous hematoma. B, Preoperative 3D CT scan showing the orbital rim fracture. C, Preoperative sagittal CT scan view showing the adherence of the inferior orbital tissue at the anterior aspect of the orbital floor (adjacent to the orbital rim fracture). The patient had diplopia on the upward gaze and a positive forced duction test. D, Preoperative coronal CT scan view showing the extensive periorbital hematoma and a hinged (Gerbino type II) fracture in the orbital floor. E, Postoperative 3D CT scan showing the reduced orbital rim fracture fixed with the titanium mesh which also extended to the area of depressed floor similar to the demonstration shown in Figure 3. F, Postoperative CT scan showing the titanium mesh in place. G, Postoperative clinical view showing the full orbital range of motion in the upward gaze.
DISCUSSION
The main aim of the current communication is to demonstrate the unique features and outcome of trap door orbital floor fractures in adults. We found no similar studies in the literature. It is important to realize that such fractures are rare in adults and our series of 10 patients were seen over a period of 20 years. In children, these fractures are commonly associated with signs of the oculocardiac reflex. This was not seen in any of our adult patients. This is hard to explain because the pathophysiology of the oculocardiac reflex is theoretically the same in all age groups: impulses from the ophthalmic division of the trigeminal nerve go to the visceral motor nuclei of the vagus nerve and finally to the heart (causing bradycardia) and stomach (causing nausea and vomiting).9,10 We reviewed the literature on trap door blowout fractures in adults. Although nausea was reported in some cases, bradycardia was only reported in a single case.11
The concept of “pure” (isolated orbital floor) and “impure” (orbital floor with concurrent rim) blowout fractures was introduced over 6 decades ago.12 In pure fractures, a direct force to the globe will result in a sudden increase in the intraorbital pressure leading to an isolated orbital floor fracture. In impure fractures, the direct force is to the orbital rim leading to a secondary compression force on the orbital floor. Trap door blowout fractures in children have been reported only with pure fractures. Our series demonstrates that impure fractures may also result in a trap door entrapment in adults. As expected, these patients will not have the classic “quite eye” seen with pure fractures.
In children, trap door fractures are associated with subtle CT scan findings although a tear drop sign is frequently seen.1 None of the CT scans showed a tear drop sign in our adult patients. Furthermore, there was an area of depression in the orbital floor at or adjacent to the entrapment site.
Our series included 10 adults (over 20 years of age), and we could not find a similar series in the literature. Our review of the English literature revealed a total of 11 well-documented adult cases over 20 years of age; and these 11 cases were reported by 9 different authors in the form of case reports.11,13–20
Both linear15 and hinged19 fracture types were reported in adults, and both types were associated with subtle or negative CT scan findings. It is important to realize that documentation of diplopia in the upgaze in the absence of classic CT scan findings of entrapment does not support early surgical intervention from the medico-legal point of view because edema of the inferior rectus (without entrapment) may be the cause of diplopia. Hence, surgery is only done in these cases if there is persistent diplopia for 2–3 weeks. An example is the case reported by Kum et al.15 A 37-year-old man had a blunt trauma to the right eye resulting in diplopia in the upgaze. CT scan did not show any fracture, and there was no CT scan evidence of any entrapment. Diplopia persisted for 3 weeks and surgical exploration revealed a linear fracture with entrapment of the inferior rectus muscle sheath (the muscle itself was not entrapped). One month after surgery, the diplopia had improved, but it was still present in extreme supraduction. Our article stresses on the fact that hinged fractures in adults are associated with a change in the normal shape/direction of the inferior rectus muscle (Figs. 2 and 4A). We believe that a positive forced duction test along with the change in the shape/direction of the inferior rectus muscle should be considered as sufficient evidence of entrapment despite the absence of all other classic CT scan findings of entrapment. Our recommendations are also supported by other authors who reported on hinged fractures in adults. Zavattero et al19 reported on a 30-year-old woman with orbital blow out fracture and diplopia. CT scan showed a minimally displaced hinged fracture and negative classic CT findings of entrapment. However, the patient had a positive forced duction test and there was a change in the shape of the inferior rectus muscle on the sagittal CT scan view. Early surgical intervention (at 72 hours) showed entrapment of the inferior rectus muscle at the hinged fracture. Release of the muscle and patching of the orbital floor was done with a good outcome.
Previous authors emphasized the time interval from trauma to intervention as a crucial factor determining the postoperative recovery of muscle function.15 All patients in the current series underwent surgery within 48 hours of injury, and residual diplopia was not observed. Papadiochos et al20 stated that ischemia of the entrapped inferior rectus muscle is irreversibly established within few hours. Hence, it may be almost impossible to timely perform the operation in these patients. We agree with these authors and believe that fibrosis of the inferior rectus muscle is mainly related to the severity of injury and the volume of muscle entrapped into the trap door fracture. In trap door blowout fractures, the injury is generally less severe. Furthermore, the entrapment in adults usually involves the perimuscular tissue with or without a small part of the muscle. This explains the full recovery of all patients in our series. Of the 11 previously reported adult cases,11,13–20 only 3 patients had residual diplopia in the extreme upward gaze.
We have utilized an infraorbital incision in our series. We are aware that this incision may be associated with a higher risk of lower lid malposition when compared to the trans-conjunctival approach.21,22 We have not observed lid retraction or hypertrophic scars in our series (Fig. 5). The author has recently switched to the trans-conjunctival approach because its skin scar (5 mm transverse scar at the lateral canthus as shown in Fig. 3) is much less conspicuous than the infraorbital scar.
Fig. 5.

Demonstration of the post-operative clinical result in the patient shown in Figure. 4. A, Postoperative clinical photograph at 1 week demonstrating the incision and the minimal edema/ecchymosis. B, There is no more diplopia with full orbital movements in the upward gaze. C, The infraorbital scar is linear at 7 months after surgery.
Most pediatric trap door fractures are of the Gerbino Type I linear fracture type,1 and there is generally no need to reconstruct the orbital floor. In adults, the fracture is usually of the hinged (Gerbino II) type with a small bony gap at the site of the hinge. We have used a titanium mesh to cover this gap in our patients. However, one may argue that this small bony gap does not reach the “critical” size for placement of an alloplastic implant. However, the sharp bony edge of the hinge and the small area of depression may cause postoperative injury to the contused and edematous inferior rectus muscle. We reviewed the method of orbital floor reconstruction in the 11 previously reported cases of adult trap door fractures11,13–20; and found that reconstruction was done in all 11 cases. The type of material was not specified in 2 cases. The materials used in the remaining 9 cases were: silastic sheet (n = 3), macropore (n = 3), collagen sheet (n = 1), titanium-reinforced polyethylene sheet (n = 1), and bone graft (n = 1).
There is still a debate in the literature regarding the best material to be used in the management of orbital floor fractures.23,24 We used the titanium mesh in our cases. We believe that there are several advantages of the titanium when compared to autologous bone grafts and other absorbable alloplasts. The mesh has the ability to confirm to the contour of the bony depression easily, it can be used for pure and impure fractures, it omits donor-site morbidity, it is radio-opaque and hence the position can be checked post-operatively, and it does not carry the risk of resorption. However, a rare, but well-known late complication may occur with use of the titanium mesh for orbital fractures, which is known as the orbital adherence syndrome.25 In this syndrome, excessive fibrosis occurs around the mesh leading to cicatricial eyelid retraction or restrictive diplopia. The pathophysiology is thought to be related to the formation of an oxide film over the surface of the titanium which induces excessive proliferation of fibroblasts.25 This complication is known to occur after a mean interval of 6 months from the insertion of the mesh (with a range of 2–12 months).25 Patients generally do well after removal of the mesh. We have not encountered this complication in our patients.
Persistent postoperative diplopia is the most common complication encountered in patients treated for orbital floor fractures.26,27 This was not seen in our series, and this may be partly related to the relatively mild injury to the inferior rectus muscle.
In conclusion, this is the first series in the literature that specifically reports on the characteristics and outcome of trap door orbital floor fractures in adults. The series also highlights the unique features of trap door blowout fractures in children versus adults, and these are summarized in Table 1.
Table 1.
A Comparison of the Features of Trap Door Blowout Fractures in Children and Adults
| Children with Trap Door Fractures | Adults with Trap Door Fractures | |
|---|---|---|
| Epidemiology | Trap door fractures are almost exclusively seen in children | Trap door fractures are very rare in adults |
| Pure vs impure subtype | Trap door fractures in children are only seen with pure fractures | Trap door fractures in adults are usually associated with pure fractures. Some cases are associated with impure fractures |
| Gerbino subtype | Most cases are Type 1 linear fractures | Most cases are Type II hinged fractures |
| The main presenting clinical picture | Limitation in supraduction of the globe with minimal periorbital soft-tissue injury | In patients with pure fractures: similar to children |
| In patients with impure fractures: significant periorbital soft-tissue injury | ||
| Oculocardiac reflex and bradycardia | Very common | Bradycardia is very rarely seen. Some patients may have mild nausea |
| The tear drop sign on CT scan | Commonly seen and indicates the entrapment of a large piece of the inferior rectus muscle | Much less common and indicates the entrapment of the perimuscular tissue with or without a small piece of muscle |
PATIENT CONSENT
Patients provided written consent for the use of their images.
ACKNOWLEDGMENT
Illustrations (Figs. 1 and 2) in this article were drawn by Dr. Mariam W. K. Fikri (MD), Faculty of Medicine, Sohag University, Egypt. queenie.illustration@gmail.com.
Footnotes
Published online 15 April 2021
Disclosure: The authors have no financial interest to declare in relation to the content of this article.
REFERENCES
- 1.Gerbino G, Roccia F, Bianchi FA, et al. Surgical management of orbital trapdoor fracture in a pediatric population. J Oral Maxillofac Surg. 2010; 68:1310–1316 [DOI] [PubMed] [Google Scholar]
- 2.Silverman N, Spindle J, Tang SX, et al. Orbital floor fracture with entrapment: Imaging and clinical correlations in 45 cases. Orbit. 2017; 36:331–336 [DOI] [PubMed] [Google Scholar]
- 3.Mehmood N, Hasan A. Oculocardiac reflex: an underrecognized but important association with orbital trap door fractures. Pediatr Emerg Care. [published online ahead of print August 9, 2019] [DOI] [PubMed] [Google Scholar]
- 4.Jordan DR, Allen LH, White J, et al. Intervention within days for some orbital floor fractures: the white-eyed blowout. Ophthalmic Plast Reconstr Surg. 1998; 14:379–390 [DOI] [PubMed] [Google Scholar]
- 5.McInnes AW, Burnstine MA. White-eyed medial wall orbital blowout fracture. Ophthalmic Plast Reconstr Surg. 2010; 26:44–46 [DOI] [PubMed] [Google Scholar]
- 6.Kwon JH, Moon JH, Kwon MS, et al. The differences of blowout fracture of the inferior orbital wall between children and adults. Arch Otolaryngol Head Neck Surg. 2005; 131:723–727 [DOI] [PubMed] [Google Scholar]
- 7.Su Y, Shen Q, Bi X, et al. Delayed surgical treatment of orbital trap door fractures in paediatric patients. Br J Opthalmol. 2019; 103:523–526 [DOI] [PubMed] [Google Scholar]
- 8.Yew CC, Shaari R, Rahman SA, et al. White-eyed blowout fracture: diagnostic pitfalls and review of literature. Injury. 2015; 46:1856–1859 [DOI] [PubMed] [Google Scholar]
- 9.Criden MR, Ellis FJ. Linear nondisplaced orbital fractures with muscle entrapment. J Aapos. 2007; 11:142–147 [DOI] [PubMed] [Google Scholar]
- 10.Wei LA, Durairaj VD. Pediatric orbital floor fractures. J Aapos. 2011; 15:173–180 [DOI] [PubMed] [Google Scholar]
- 11.Sires BS, Stanley RB, Jr, Levine LM. Oculocardiac reflex caused by orbital floor trapdoor fracture: an indication for urgent repair. Arch Ophthalmol. 1998; 116:955–956 [PubMed] [Google Scholar]
- 12.Converse JM, Smith B. Blowout fracture of the floor of the orbit. Trans Am Acad Ophthalmol Otolaryngol. 1960; 64:676–688 [PubMed] [Google Scholar]
- 13.Kakizaki H, Zako M, Katori N, et al. Adult medial orbital wall trapdoor fracture with missing medial rectus muscle. Orbit. 2006; 25:61–63 [DOI] [PubMed] [Google Scholar]
- 14.Mehanna P, Mehanna D, Cronin A. White-eyed blowout fracture: another look. Emerg Med Australas. 2009; 21:229–232 [DOI] [PubMed] [Google Scholar]
- 15.Kum C, McCulley TJ, Yoon MK, et al. Adult orbital trapdoor fracture. Ophthalmic Plast Reconstr Surg. 2009; 25:486–487 [DOI] [PubMed] [Google Scholar]
- 16.Yano H, Suzuki Y, Yoshimoto H, et al. Linear-type orbital floor fracture with or without muscle involvement. J Craniofac Surg. 2010; 21:1072–1078 [DOI] [PubMed] [Google Scholar]
- 17.Ethunandan M, Evans BT. Linear trapdoor or “white-eye” blowout fracture of the orbit: not restricted to children. Br J Oral Maxillofac Surg. 2011; 49:142–147 [DOI] [PubMed] [Google Scholar]
- 18.Noh WJ, Park TJ, Kim JY, et al. Isolated trapdoor-type medial blowout fracture in an adult presenting horizontal diplopia treated by endoscopic endonasal approach. J Surg Case Rep. 2013; 2013:rjt009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Zavattero E, Roccia F, Benech R, et al. Orbital trapdoor fracture: can it occur also in adults? J Craniofac Surg. 2015; 26:e6–e8 [DOI] [PubMed] [Google Scholar]
- 20.Papadiochos I, Petsinis V, Tasoulas J, et al. Pure orbital trapdoor fractures in adults: tight entrapment of perimuscular tissue mimicking true muscle incarceration with successful results from early intervention. Craniomaxillofac Trauma Reconstr. 2019; 12:54–61 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Ridgway EB, Chen C, Colakoglu S, et al. The incidence of lower eyelid malposition after facial fracture repair: a retrospective study and meta-analysis comparing subtarsal, subciliary, and transconjunctival incisions. Plast Reconstr Surg. 2009; 124:1578–1586 [DOI] [PubMed] [Google Scholar]
- 22.Subramanian B, Krishnamurthy S, Suresh Kumar P, et al. Comparison of various approaches for exposure of infraorbital rim fractures of zygoma. J Maxillofac Oral Surg. 2009; 8:99–102 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Bourry M, Hardouin JB, Fauvel F, et al. Clinical evaluation of the efficacy of materials used for primary reconstruction of orbital floor defects: meta-analysis. Head Neck. 2021; 43:679–690 [DOI] [PubMed] [Google Scholar]
- 24.Gunarajah DR, Samman N. Biomaterials for repair of orbital floor blowout fractures: a systematic review. J Oral Maxillofac Surg. 2013; 71:550–570 [DOI] [PubMed] [Google Scholar]
- 25.Lee HB, Nunery WR. Orbital adherence syndrome secondary to titanium implant material. Ophthalmic Plast Reconstr Surg. 2009; 25:33–36 [DOI] [PubMed] [Google Scholar]
- 26.Hsu CK, Hsieh MW, Chang HC, et al. Anatomic factors predicting postoperative strabismus in orbital wall fracture repair. Sci Rep. 2019; 9:14785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Balaji SM. Residual diplopia in treated orbital bone fractures. Ann Maxillofac Surg. 2013; 3:40–45 [DOI] [PMC free article] [PubMed] [Google Scholar]