

Abstract
Background:
Previous studies have shown that adequate physical activity (PA, defined as any bodily movement that requires energy expenditure) related awareness and knowledge is crucial to promote regular PA. Therefore, this study aims to characterize PA awareness and knowledge, and to quantify its association with sociodemographic characteristics, health literacy and frequency of exercise.
Methods:
In a cross-sectional study conducted in 2012, a total of 1624 Portuguese-speaking residents of mainland Portugal (16–79 years old) were assessed through face-to-face interviews using a structured questionnaire. Adjusted prevalence ratios, calculated using Poisson regression, were used to quantify associations with PA awareness and knowledge.
Results:
The most reported benefits of PA were “reduces abdominal fat accumulation” (95.8%), “reduces myocardial infarction risk” (92.9%) and “improves bone health” (90.7%), these were less referred by older participants, while more often identified by those who exercise daily. The most referred barrier for people to not practice PA regularly was “lack of time” (33.9%) with differences observed by sex, age, education, employment and health literacy. Over two-thirds of participants correctly identified at least 2 of 3 PAs (“running”, “soccer” and “tennis”) that require the most energy, particularly males, those with higher health literacy and who exercise twice or more times a week.
Conclusions:
An adequate PA-related awareness and knowledge was observed, and differences according to age, health literacy levels and frequency of exercise were found. As such, awareness-raising interventions to increase regular PA through improving physical literacy and motivation should focus on older adults, those with limited health literacy and who do not exercise.
Keywords: exercise, health literacy, health surveys, physical activity, public health
Introduction
Physical inactivity is the fourth leading risk factor for global mortality, accounting for over 5% of deaths worldwide.1 In particular, regular physical activity (PA), which is defined as “any bodily movement by skeletal muscles that requires energy expenditure (…) during leisure time, for transport to get to and from places, or as part of a person's work”,2 is associated with a lower risk of hypertension, coronary artery disease, type 2 diabetes, osteoporosis, and breast and colon cancers.3–6 Additionally, regular PA can also help to promote overall quality of life and to maintain a healthy weight.7,8
Although the general population may recognize the relationship between regular PA and health, recent estimates indicate that the majority of adults do not engage in a sufficient amount of health-enhancing regular PA as specified in the guidelines.9,10 In 2015 to 2016, almost half of the adult Portuguese population was sedentary or inactive, that is, they did not perform at least about 30 minutes of moderate activity most days, and only 27% spent 30 minutes per day in vigorous activities or 1 hour per day in moderate activities.11
Previous studies have shown that changes in behaviour may also depend on awareness and knowledge of the action to initiate change.12 Accordingly, it is crucial that populations have more and better knowledge about regular PA through health promotion as well as PA interventions to increase the practice of regular PA.13,14 As such, the Portuguese National Health Plan 2011 to 2016 (revised and extended to 2020) focused on the promotion of health literacy as an important factor in the adoption of healthier lifestyles.15 In particular, the Portuguese National Program for the Promotion of Physical Activity was created in 2016 to increase the population's awareness regarding the importance of regular PA in health, and the implementation of policies that aimed to decrease sedentary behaviour and increase the practice of regular PA.9 Nevertheless, while there is generally information about regular PA behaviour, there is a lack of information about awareness and knowledge of regular PA among the general population.16 Therefore, understanding the current status of regular PA-related awareness and knowledge as well as its main associated factors will provide a benchmark to plan and monitor the effects of awareness-raising interventions aiming to increase the practice of regular PA.
Hence, the aim of this study is to characterize regular PA-related awareness and knowledge, and its association with sociodemographic characteristics, health literacy and frequency of exercise, among the Portuguese population.
Methods
Study design
This study is based on a national survey conducted in 2012, with the purpose of assessing the knowledge and health behaviours of the Portuguese population aged between 16 and 79 years old, as previously described.17,18 Briefly, this cross-sectional study evaluated a representative sample of the Portuguese-speaking residents, regardless of their nationality and literacy, in mainland Portugal obtained through a multistage sampling design defined according to the results of the 2001 Portuguese Census.19 A stratified probabilistic sampling procedure by NUTS II—Territorial Nomenclature Units for Statistical Purposes, level II (North, Center, Lisbon and Tagus Valley, Alentejo and Algarve) and the number of inhabitants in geographical units with at least 10 dwellings (<2000, 2000–9999, 10,000–19,999, 20,000–100,000 and >100,000) was used to select 150 neighborhoods from which 585 starting points were designated for the selection of households through standard random route procedures. Finally, the individual with the most recent birthday from each selected household was invited to participate. A total of 1624 valid interviews were obtained (response rate: 70.8%).
Data collection
Data were collected through face-to-face interviews using a structured questionnaire. Sociodemographic characteristics included sex, age, education and employment status. Participant's age was collected as a continuous variable, and was categorized as <30, 30 to 39, 40 to 49, 50 to 59, 60 to 69 and 70 to 79 years. Education was collected and categorized as 0 to 4, 5 to 9, 10 to 12 and >12 completed years of schooling. Employment status was evaluated by asking participants “Considering your work situation, what is your current employment status?”, and was characterized as employed including full time, part time, non-paid family worker, and unemployed including retired, housewife, sick leave, others. Frequency of exercise was evaluated by asking participants “How often do you exercise?”, and was characterized as never, less than twice a week including less than once a month, once to 3 times a month and once a week, twice or more times a week, and daily.
Health literacy was assessed using the Newest Vital Sign (NVS) instrument.20,21 This tool was designed to evaluate health literacy, reading and numeracy skills, and has shown high reliability and sensitivity. The number of correct answers was used to calculate a score ranging from 0 to 6 [0–1: High Likelihood of Limited Health Literacy (HLLL), 2–3: Possibility of Limited Health Literacy (PLL) and 4–6: Adequate Health Literacy (AL)]. Participants who reported that they were unable to read or write were classified as having HLLL.
To evaluate regular PA-related awareness and knowledge, participants were asked about: (1) potential benefits of regular PA; (2) barriers for people to not practice regular PA; (3) types of PA that require the most energy.
Potential benefits of regular PA
Participants were read several sentences related to possible benefits of regular PA. They were asked for each one whether or not they agreed that regular PA: (a) “reduces depression symptoms”, (b) “reduces myocardial infarction risk”, (c) “reduces diabetes risk”, (d) “reduces abdominal fat accumulation”, (e) “improves bone health”, (f) “decreases hip fracture risk” and (g) “decreases lung cancer risk”. The answers considered for each were “yes”, “no”, “does not know” and “did not answer”. The answers “does not know” and “did not answer” were recoded as “no” for data analysis.
Barriers for people to not practice regular PA
To evaluate barriers for people to not practice regular PA, participants were asked “What reason do you think most contributes to a person to not participate in regular PA?”. They could select the reason from the following list: “lack of time”, “do not like exercising/lack of motivation”, “prefer doing other things”, “physical exertion at work/chores”, “health problems”, “simply do not want to exercise”, “excess weight”, “lack of appropriate spaces”, “age” and “no one to go with/lack of company”. The options “excess weight”, “lack of appropriate spaces”, “age” and “no one to go with/lack of company” were recoded as “others” as few participants selected these. Participants who did not know or did not answer were recoded as “do not know/answer” for data analysis.
Types of PA that require the most energy
To assess the participants’ ability to identify PAs that require the most energy, participants were asked: “Of the following types of PA, in your opinion, which three require more energy?”. They could select 3 types of PA from among the following list: “fast paced walking”, “running”, “biking (less than 15 kilometers per hour)”, “soccer”, “basketball”, “tennis” and “ballroom dancing”. The answers “running”, “soccer” and “tennis” were taken as correct considering the metabolic equivalent of each.22 For the purposes of this study, analyses were conducted considering the number of correct answers: none, at least 1, at least 2 and all 3.
Statistical analysis
Sample characteristics are presented as counts and proportions for categorical variables.
The associations between sociodemographic characteristics, health literacy or frequency of exercise and the 3 different indicators of regular PA-related awareness or knowledge were quantified using prevalence ratios (PR) with 95% confidence intervals (95% CI) calculated using Poisson regression. Analyses were adjusted for sex, age, educational level, employment status, health literacy and frequency of exercise.
All estimates were weighted to be representative of the Portuguese population using 2 weights. The first are population weights that correct for differences between the sample and the entire population of Portuguese-speaking dwellers regarding sex, age, education, marital status, NUTS II and size of the geographical units. The second are design weights that correct for discrepancies arising from a multistage sampling design regarding the unequal probability of selection of an individual.
Statistical analyses were performed using Stata 15.1 (StataCorp LP, College Station, TX, USA).
Ethical approval
The survey was approved by the Ethics Committee of the University of Porto (33/CEUP/2012) and all participants provided informed consent.
Results
The sample included a similar weighted proportion of males and females, almost two-thirds of the participants were under 50 years of age (63.4%), 42.5% had <5 years of education, 54.4% were employed and 45.9% had HLLL. Regarding the frequency of exercise, almost half of the participants did not exercise (43.6%) and 17.9% exercised daily (Table 1).
Table 1.
Characteristics of participants
| N | Unweighted % | Weighted % | |
|---|---|---|---|
| Overall | 1624 | – | – |
| Sex | |||
| Females | 998 | 61.4 | 50.3 |
| Males | 626 | 38.6 | 49.7 |
| Age (yr) | |||
| <30 | 233 | 14.4 | 27.7 |
| 30–39 | 224 | 13.8 | 16.6 |
| 40–49 | 236 | 14.5 | 19.1 |
| 50–59 | 283 | 17.4 | 14.4 |
| 60–69 | 358 | 22.0 | 12.9 |
| 70–79 | 290 | 17.9 | 9.3 |
| Education (yr) | |||
| 0–4 | 793 | 48.9 | 42.5 |
| 5–9 | 301 | 18.6 | 18.4 |
| 10–12 | 313 | 19.3 | 25.2 |
| >12 | 216 | 13.3 | 13.9 |
| Employment status | |||
| Employed | 740 | 45.7 | 54.4 |
| Unemployed | 879 | 54.3 | 45.6 |
| Health literacy—NVS | |||
| HLLL | 786 | 48.4 | 45.9 |
| PLL | 471 | 29.0 | 28.6 |
| AL | 367 | 22.6 | 25.5 |
| Frequency of exercise | |||
| Never | 750 | 46.3 | 43.6 |
| Less than twice a week | 259 | 16.0 | 18.2 |
| Twice or more times a week | 319 | 19.7 | 20.3 |
| Daily | 291 | 18.0 | 17.9 |
For education and frequency of exercise, the total does not add up to 1624 due to missing data. Percentages may not add up to 100.0% due to rounding.
AL = Adequate Health Literacy, HLLL = High Likelihood of Limited Health Literacy, NVS = Newest Vital Sign, PLL = Possibility of Limited Health Literacy.
Overall, most participants identified the benefits of regular PA as “reduces abdominal fat accumulation” (95.8%), “reduces myocardial infarction risk” (92.9%), “improves bone health” (90.7%), “reduces depression symptoms” (87.8%) and “reduces diabetes risk” (80.7%) (Fig. 1A). The benefit that regular PA “reduces abdominal fat accumulation” was identified less often by the oldest participants (PR = 0.87; 95% CI: 0.78–0.97). “Reduces myocardial infarction risk” was referred more frequently by unemployed participants (PR = 1.04; 95% CI: 1.01–1.08), and by those who exercise less than twice a week (PR = 1.08; 95% CI: 1.03–1.13) and daily (PR = 1.06; 95% CI: 1.01–1.12). Likewise, “decreases lung cancer risk” was identified more frequently by those who exercise less than twice a week (PR = 1.22; 95% CI: 1.06–1.41) and daily (PR = 1.20; 95% CI: 1.05–1.38); while “improves bone health” and “reduces diabetes risk” were identified more often by those who exercise daily (PR = 1.06; 95% CI: 1.01–1.12 and PR = 1.14; 95% CI: 1.06–1.23, respectively). “Reduces depression symptoms” was referred more frequently by more educated participants (10-12 vs. 0–4years: PR = 1.11; 95% CI: 1.03–1.20) and those who exercise less than twice a week (PR = 1.11; 95% CI: 1.04–1.19), though less often by older individuals (PR = 0.84; 95% CI: 0.72–0.98). Individuals with PLL and AL identified “decreases hip fracture risk” less often (PR = 0.88; 95% CI: 0.79–0.99 and PR = 0.82; 95% CI: 0.72–0.93, respectively; Table 2).
Figure 1.
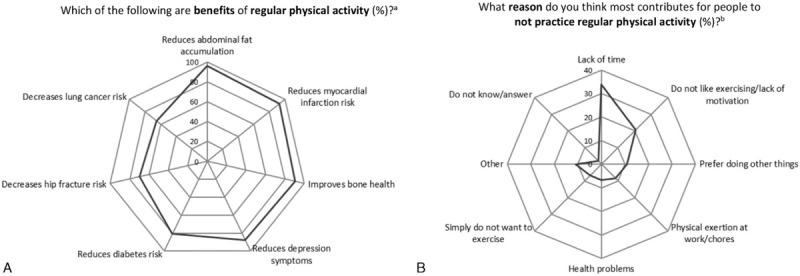
Knowledge of benefits of regular physical activity (A) and reasons for not practicing regular physical activity (B). aPercentage of participants identifying each as a possible benefit of regular physical activity. bPercentage of participants identifying each as the main reason for not practicing regular physical activity. Other reasons include excess weight; lack of appropriate spaces; age; no one to go with/lack of company.
Table 2.
Knowledge of benefits of regular physical activity, according to sociodemographic characteristics, health literacy and frequency of exercise
| Reduces abdominal fat accumulation | Reduces myocardial infarction risk | Improves bone health | Reduces depression symptoms | Reduces diabetes risk | Decreases hip fracture risk | Decreases lung cancer risk | |
|---|---|---|---|---|---|---|---|
| PR (95% CI)∗ | PR (95% CI)∗ | PR (95% CI)∗ | PR (95% CI)∗ | PR (95% CI)∗ | PR (95% CI)∗ | PR (95% CI)∗ | |
| Sex | |||||||
| Females | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) |
| Males | 0.99 (0.97–1.02) | 0.98 (0.95–1.02) | 1.02 (0.97–1.07) | 0.96 (0.91–1.01) | 0.96 (0.90–1.03) | 0.95 (0.87–1.05) | 1.03 (0.94–1.14) |
| Age (yr) | |||||||
| <30 | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) |
| 30–39 | 0.96 (0.91–1.01) | 1.03 (0.96–1.09) | 1.04 (0.98–1.11) | 0.94 (0.87–1.02) | 1.08 (0.98–1.19) | 1.12 (0.97–1.30) | 1.05 (0.88–1.25) |
| 40–49 | 0.96 (0.91–1.00) | 1.04 (0.98–1.11) | 1.03 (0.95–1.12) | 1.03 (0.95–1.12) | 1.03 (0.92–1.16) | 1.15 (0.98–1.35) | 0.99 (0.84–1.17) |
| 50–59 | 0.99 (0.96–1.03) | 1.02 (0.95–1.08) | 1.05 (0.98–1.13) | 1.01 (0.93–1.09) | 1.03 (0.93–1.16) | 1.11 (0.94–1.32) | 0.99 (0.84–1.17) |
| 60–69 | 0.97 (0.94–1.01) | 1.02 (0.95–1.08) | 1.06 (0.98–1.15) | 1.05 (0.97–1.15) | 1.01 (0.90–1.14) | 1.13 (0.93–1.38) | 1.07 (0.86–1.33) |
| 70–79 | 0.87 (0.78–0.97) | 0.89 (0.78–1.03) | 0.91 (0.78–1.06) | 0.84 (0.72–0.98) | 0.84 (0.70–1.01) | 0.87 (0.69–1.09) | 0.84 (0.62–1.15) |
| Education (yr) | |||||||
| 0–4 | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) |
| 5–9 | 0.99 (0.95–1.02) | 1.01 (0.95–1.07) | 1.03 (0.96–1.10) | 1.04 (0.95–1.14) | 0.99 (0.89–1.09) | 0.94 (0.82–1.08) | 1.02 (0.87–1.02) |
| 10–12 | 1.00 (0.97–1.04) | 1.04 (0.98–1.11) | 1.05 (0.98–1.11) | 1.11 (1.03–1.20) | 1.08 (0.97–1.19) | 1.12 (0.98–1.28) | 1.15 (0.98–1.36) |
| >12 | 0.97 (0.91–1.03) | 1.01 (0.93–1.09) | 1.00 (0.92–1.09) | 1.09 (1.00–1.20) | 1.04 (0.91–1.18) | 0.99 (0.83–1.19) | 1.07 (0.89–1.29) |
| Employment status | |||||||
| Employed | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) |
| Unemployed | 1.00 (0.98–1.03) | 1.04 (1.01–1.08) | 1.01 (0.95–1.07) | 1.02 (0.96–1.08) | 1.07 (0.99–1.16) | 0.95 (0.84–1.07) | 0.98 (0.87–1.11) |
| Health literacy—NVS | |||||||
| HLLL | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) |
| PLL | 1.01 (0.98–1.03) | 1.01 (0.97–1.06) | 1.00 (0.95–1.06) | 1.04 (0.98–1.10) | 1.05 (0.97–1.13) | 0.88 (0.79–0.99) | 1.09 (0.97–1.23) |
| AL | 1.02 (0.99–1.05) | 1.02 (0.98–1.06) | 0.99 (0.95–1.05) | 1.05 (0.97–1.12) | 1.01 (0.92–1.10) | 0.82 (0.72–0.93) | 0.93 (0.80–1.07) |
| Frequency of exercise | |||||||
| Never | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) |
| Less than twice a week | 1.01 (0.97–1.05) | 1.08 (1.03–1.13) | 1.06 (1.00–1.13) | 1.11 (1.04–1.19) | 1.09 (1.00–1.19) | 1.08 (0.96–1.22) | 1.22 (1.06–1.41) |
| Twice or more times a week | 1.00 (0.96–1.05) | 1.03 (0.97–1.09) | 1.06 (0.99–1.13) | 1.05 (0.97–1.14) | 0.97 (0.87–1.09) | 1.06 (0.93–1.21) | 1.07 (0.91–1.25) |
| Daily | 1.00 (0.95–1.04) | 1.06 (1.01–1.12) | 1.06 (1.01–1.12) | 1.06 (0.98–1.13) | 1.14 (1.06–1.23) | 1.03 (0.91–1.17) | 1.20 (1.05–1.38) |
AL = Adequate Health Literacy, CI = confidence interval, HLLL = High Likelihood of Limited Health Literacy, NVS = Newest Vital Sign, PLL = Possibility of Limited Health Literacy, PR = prevalence ratio.
Adjusted for all variables in the table.
Regarding the barriers for people to not practice regular PA, over one-third of participants identified “lack of time” (33.9%), followed by “do not like exercising/lack of motivation” (20.5%) and “prefer doing other things” (10.8%) (Fig. 1B). “Lack of time” was identified less often by males (PR = 0.80; 95% CI: 0.66–0.96) and unemployed participants (PR = 0.53; 95% CI: 0.41–0.68) as a barrier for not practicing regular PA. The reason “do not like exercising/lack of motivation” was referred more frequently by unemployed participants (PR = 1.70; 95% CI: 1.28–2.24) and those with AL (PR = 1.78; 95% CI: 1.21–2.61). Older (60–69 vs <30 years: PR = 0.34; 95% CI: 0.15–0.76 and 70–79 vs <30 years: PR = 0.35; 95% CI: 0.15–0.83) and more educated (>12 vs 0–4 years: PR = 0.31; 95% CI: 0.13–0.72) individuals less often selected “prefer doing other things”; while unemployed participants identified it more often (PR = 1.92; 95% CI: 1.21–3.03). The reason “physical exertion at work/chores” was identified more often by participants aged between 40 and 49 years (PR = 2.51; 95% CI: 1.13–5.67), while “health problems” was more frequently selected by older participants (PR = 2.51; 95% CI: 1.22–5.17), though less often referred by those with AL (PR = 0.42; 95% CI: 0.19–0.95). Finally, “simply do not want to exercise” was identified more often by older participants (50–59 vs <30 years: PR = 2.06; 95% CI: 1.03–4.12; 60–69 vs <30 years: PR = 2.43; 95% CI: 1.19–4.97; 70–79 vs <30 years: PR = 2.21; 95% CI: 1.04–4.68); while those aged between 30 and 39 years referred “other reasons” less often (PR = 0.38; 95% CI: 0.17–0.85; Table 3).
Table 3.
Knowledge of reasons that most contribute for people to not practice regular physical activity, according to sociodemographic characteristics, health literacy and frequency of exercise
| Lack of time | Do not like exercising/lack of motivation | Prefer doing other things | Physical exertion at work/chores | Health problems | Simply do not want to exercise | Others† | |
|---|---|---|---|---|---|---|---|
| PR (95% CI)∗ | PR (95% CI)∗ | PR (95% CI)∗ | PR (95% CI)∗ | PR (95% CI)∗ | PR (95% CI)∗ | PR (95% CI)∗ | |
| Sex | |||||||
| Females | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) |
| Males | 0.80 (0.66–0.96) | 1.16 (0.87–1.54) | 1.34 (0.86–2.07) | 1.24 (0.74–2.07) | 1.17 (0.69–1.98) | 0.77 (0.47–1.28) | 0.99 (0.65–1.53) |
| Age (yr) | |||||||
| <30 | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) |
| 30–39 | 1.22 (0.92–1.61) | 1.04 (0.71–1.53) | 0.74 (0.38–1.43) | 1.78 (0.73–4.35) | 0.87 (0.36–2.13) | 1.06 (0.42–2.65) | 0.38 (0.17–0.85) |
| 40–49 | 1.25 (0.92–1.70) | 0.76 (0.47–1.22) | 0.83 (0.41–1.66) | 2.51 (1.13–5.67) | 0.56 (0.22–1.39) | 0.95 (0.41–2.22) | 0.58 (0.30–1.10) |
| 50–59 | 1.24 (0.91–1.70) | 0.66 (0.42–1.05) | 0.65 (0.33–1.28) | 1.50 (0.58–3.90) | 0.97 (0.46–2.06) | 2.06 (1.03–4.12) | 0.86 (0.45–1.64) |
| 60–69 | 1.37 (0.95–1.97) | 0.71 (0.45–1.10) | 0.34 (0.15–0.76) | 1.40 (0.46–4.21) | 0.96 (0.42–2.17) | 2.43 (1.19–4.97) | 1.03 (0.52–2.02) |
| 70–79 | 1.07 (0.66–1.73) | 0.59 (0.33–1.05) | 0.35 (0.15–0.83) | 0.94 (0.27–3.31) | 2.51 (1.22–5.17) | 2.21 (1.04–4.68) | 1.18 (0.51–2.73) |
| Education (yr) | |||||||
| 0–4 | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) |
| 5–9 | 1.22 (0.96–1.57) | 0.77 (0.52–1.16) | 0.79 (0.47–1.34) | 0.51 (0.24–1.09) | 1.51 (0.75–3.04) | 1.22 (0.64–2.32) | 1.05 (0.55–2.01) |
| 10–12 | 0.98 (0.73–1.30) | 0.92 (0.61–1.38) | 0.64 (0.36–1.14) | 1.65 (0.79–3.46) | 1.57 (0.71–3.48) | 0.67 (0.30–1.50) | 1.25 (0.66–2.34) |
| >12 | 1.12 (0.84–1.51) | 1.33 (0.87–2.04) | 0.31 (0.13–0.72) | 0.63 (0.24–1.65) | 0.64 (0.22–1.82) | 0.82 (0.32–2.11) | 1.26 (0.57–2.80) |
| Employment status | |||||||
| Employed | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) |
| Unemployed | 0.53 (0.41–0.68) | 1.70 (1.28–2.24) | 1.92 (1.21–3.03) | 0.75 (0.42–1.33) | 1.19 (0.67–2.12) | 0.82 (0.48–1.41) | 1.48 (0.90–2.43) |
| Health literacy—NVS | |||||||
| HLLL | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) |
| PLL | 0.87 (0.70–1.07) | 1.20 (0.84–1.72) | 1.18 (0.72–1.93) | 1.17 (0.64–2.13) | 0.70 (0.34–1.42) | 1.12 (0.66–1.91) | 1.03 (0.61–1.73) |
| AL | 0.99 (0.80–1.22) | 1.78 (1.21–2.61) | 0.98 (0.54–1.78) | 0.67 (0.35–1.28) | 0.42 (0.19–0.95) | 0.70 (0.30–1.67) | 0.73 (0.40–1.34) |
| Frequency of exercise | |||||||
| Never | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) | (Reference) |
| Less than twice a week | 1.07 (0.86–1.34) | 0.67 (0.42–1.06) | 1.40 (0.74–2.64) | 0.93 (0.46–1.90) | 0.70 (0.29–1.69) | 1.40 (0.77–2.56) | 1.06 (0.56–1.99) |
| Twice or more times a week | 0.83 (0.63–1.09) | 1.29 (0.91–1.82) | 1.12 (0.59–2.14) | 0.92 (0.44–1.93) | 1.16 (0.61–2.21) | 1.37 (0.70–2.66) | 0.72 (0.38–1.36) |
| Daily | 0.85 (0.65–1.13) | 1.13 (0.77–1.66) | 0.95 (0.51–1.78) | 1.31 (0.70–2.42) | 0.87 (0.42–1.78) | 1.46 (0.82–2.60) | 0.89 (0.52–1.52) |
AL = Adequate Health Literacy, CI = confidence interval, HLLL = High Likelihood of Limited Health Literacy, NVS = Newest Vital Sign, PLL = Possibility of Limited Health Literacy, PR = prevalence ratio.
Adjusted for all variables in the table.
Includes excess weight, lack of appropriate spaces, age, no one to go with/lack of company.
Nearly two-thirds of participants correctly identified at least 2 PAs that require the most energy, while only 8.6% correctly selected all 3 (“running”, “soccer” and “tennis”). Most participants referred to “running” (72.5%) and “soccer” (69.5%) as those with the most amount of energy required, while fewer participants identified tennis (23.9%). Over half incorrectly selected “biking (less than 15 kilometers per hour)” (53.2%). Males (PR = 1.14; 95% CI: 1.02–1.27), participants with PLL and AL (PR = 1.32; 95% CI: 1.18–1.47 and PR = 1.29; 95% CI: 1.12–1.48, respectively) and those who exercise twice or more times a week (PR = 1.15; 95% CI: 1.02–1.30) more often correctly identified at least 2 PAs. On the contrary, those aged 40–49 and 70–79 years less frequently correctly selected at least 2 PAs (PR = 0.84; 95% CI: 0.71–0.99 and PR = 0.65; 95% CI: 0.50–0.85, respectively). There were no significant differences according to sociodemographic characteristics, health literacy and frequency of exercise in the correct identification of all 3 PAs with the most energy required (Table 4).
Table 4.
Number of correctly identified physical activities with the most energy required,∗ according to sociodemographic characteristics, health literacy and frequency of exercise
| None correct (8.2%) | At least 1 out of 3 correct (91.8%) | At least 2 out of 3 correct (65.5%) | All 3 correct (8.6%) | |
|---|---|---|---|---|
| PR (95% CI)† | PR (95% CI)† | PR (95% CI)† | PR (95% CI)† | |
| Sex | ||||
| Females | (Reference) | (Reference) | (Reference) | (Reference) |
| Males | 0.23 (0.13–0.42) | 1.11 (1.07–1.15) | 1.14 (1.02–1.27) | 0.90 (0.55–1.48) |
| Age (yr) | ||||
| <30 | (Reference) | (Reference) | (Reference) | (Reference) |
| 30–39 | 1.41 (0.51–3.88) | 0.99 (0.96–1.03) | 0.95 (0.82–1.10) | 0.71 (0.33–1.52) |
| 40–49 | 2.75 (1.04–7.27) | 0.96 (0.92–1.01) | 0.84 (0.71–0.99) | 0.62 (0.25–1.50) |
| 50–59 | 2.74 (1.00–7.55) | 0.96 (0.91–1.01) | 0.86 (0.73–1.00) | 0.66 (0.25–1.69) |
| 60–69 | 2.51 (0.90–7.00) | 0.96 (0.91–1.02) | 0.90 (0.77–1.06) | 0.82 (0.25–2.74) |
| 70–79 | 6.15 (2.14–17.71) | 0.75 (0.63–0.88) | 0.65 (0.50–0.85) | 0.31 (0.07–1.40) |
| Education (yr) | ||||
| 0–4 | (Reference) | (Reference) | (Reference) | (Reference) |
| 5–9 | 0.63 (0.31–1.28) | 1.03 (0.99–1.08) | 0.96 (0.83–1.10) | 0.83 (0.40–1.73) |
| 10–12 | 0.60 (0.29–1.26) | 1.03 (0.99–1.07) | 0.96 (0.84–1.10) | 0.72 (0.33–1.56) |
| >12 | 1.34 (0.65–2.79) | 1.00 (0.95–1.06) | 0.95 (0.82–1.11) | 0.85 (0.37–1.92) |
| Employment status | ||||
| Employed | (Reference) | (Reference) | (Reference) | (Reference) |
| Unemployed | 1.27 (0.79–2.05) | 0.99 (0.95–1.02) | 1.01 (0.90–1.13) | 0.83 (0.47–1.47) |
| Health literacy—NVS | ||||
| HLLL | (Reference) | (Reference) | (Reference) | (Reference) |
| PLL | 0.49 (0.30–0.82) | 1.06 (1.02–1.10) | 1.32 (1.18–1.47) | 1.52 (0.81–2.85) |
| AL | 0.72 (0.35–1.46) | 1.04 (0.99–1.08) | 1.29 (1.12–1.48) | 1.38 (0.73–2.61) |
| Frequency of exercise | ||||
| Never | (Reference) | (Reference) | (Reference) | (Reference) |
| Less than twice a week | 0.43 (0.21–0.89) | 1.04 (1.00–1.09) | 1.00 (0.85–1.17) | 1.15 (0.49–2.71) |
| Twice or more times a week | 0.93 (0.52–1.64) | 1.00 (0.95–1.07) | 1.15 (1.02–1.30) | 1.05 (0.49–2.25) |
| Daily | 0.72 (0.38–1.35) | 1.03 (0.98–1.08) | 1.03 (0.88–1.20) | 1.74 (0.87–3.47) |
AL = Adequate Health Literacy, CI = confidence interval, HLLL = High Likelihood of Limited Health Literacy, NVS = Newest Vital Sign, PLL = Possibility of Limited Health Literacy, PR = prevalence ratio.
“Running”, “soccer” and “tennis” were taken as correct considering the metabolic equivalent of each.22
Adjusted for all variables in the table.
Discussion
The present study provides a characterization of key aspects of regular PA-related awareness and knowledge in the Portuguese population. The majority of participants correctly identified the main health benefits of regular PA, as well as at least one of the exercises that uses the most energy. Overall, younger participants, those who have higher levels of health literacy and who exercise tended to present better knowledge on regular PA. The most referred barriers for people to not practice regular PA were “lack of time”, “do not like exercising/lack of motivation” and “prefer doing other things”, with differences observed depending on sex, age, education, employment status and health literacy.
It has been shown that regular PA is associated with a better overall quality of life,8 and decreases the risk of various chronic diseases.3–6 In the present study, most participants correctly identified the benefits of regular PA as reducing abdominal fat accumulation and depression symptoms, decreasing the risk of myocardial infarction and diabetes, as well as improving bone health. Previous studies have found that the majority of participants strongly agree that regular PA is beneficial for overall health, although most are not able to correctly identify the specific diseases associated with a lack of regular PA.23,24 Regarding the mental health benefits of regular PA specifically, 1 study conducted among university students found that over two-thirds of participants reported that it could “help improve wellbeing”, while just under three-quarters reported that it could “help manage depression and anxiety/stress”.25 In particular, female students were significantly more likely than males to identify depression and anxiety/stress,25 which was also observed in our study, though not statistically significant. This may be due to the fact that as women have a higher lifetime prevalence of mood or anxiety disorders than men,26 they may have a greater knowledge of self-management strategies including the practice of regular PA. Additionally, among health professionals, a prior investigation found that “reducing the risk of cardiovascular disease”, “an effective treatment for depression” and “can help treat type two diabetes” were correctly referred as benefits of regular PA.27 However, there was also a proportion who agreed with fictitious statements that were included, such as regular PA “could reduce the risk of glaucoma” and that “the only benefit of regular PA is weight loss”.27 This result is particularly relevant since health professionals have a key role in providing PA-related knowledge to patients and promoting regular PA.
Although most participants of the present study had knowledge of the health benefits related with regular PA, over 60% engage in exercise never or less than twice a week, indicating a high level of sedentary behaviour among this population. This is in line with recent results observed in Portugal, with the prevalence of insufficient regular PA estimated to be nearly 50% among adults.11,28 As a result, in recent years, the Portuguese National Health Plan and the Portuguese National Program for the Promotion of Physical Activity have implemented policies to decrease sedentary behaviour through campaigns to improve physical literacy as well as motivate the Portuguese population in order to increase the adoption of healthier lifestyles.9,15
Previous studies have shown that lack of time and motivation are the most common barriers for regular PA.29–33 Likewise, we found that the main reasons why people do not practice regular PA were “lack of time”, “do not like exercising/lack of motivation” and “prefer doing other things”. Females were significantly more likely to report “lack of time” as the reason that most contributes to not practicing regular PA, which is in line with previous results.29,30 Generally, men report exercising for enjoyment more than women,32,34 this may be due to the fact that women usually spend more time on housework and they have also become more active in the workplace over the past decades leaving them with less time for regular PA.32 The main reasons for not practicing sport regularly may also depend on age, education and employment status.29,30,33 In particular, we found that older participants more often referred “health problems” and “simply do not want to exercise” as barriers to regular PA. This has also been observed previously, where “having an illness” was a more common barrier to regular PA for older people.33 Regarding education, a prior investigation found that participants with a lower educational level reported “lack of social support”, “lack of resources” and “fear of injury” more often, while “lack of time” was not identified as a barrier.30 Accordingly, we did not find statistically significant results for “lack of time” though participants with a higher education were significantly less likely to report “prefer doing other things” as a barrier to practicing regular PA. Finally, we found that participants with AL were more likely to refer “prefer doing other things” and less likely to refer “health problems” as barriers to practicing regular PA, which is likely due to their overall higher literacy.21
Regarding knowledge on PAs that use the most energy, we found that most participants correctly identified running and soccer, while fewer participants identified tennis. Males were more likely to accurately report at least 1 or 2 PAs, which may be due to the fact that males prefer PA that is vigorous, and requires skill and practice,35 or group activities such as soccer, volleyball and basketball,36 which generally use more energy. Although there are no previous studies that have specifically examined knowledge about energy expenditure with which to compare our results, in 1 study most participants identified walking as a PA, which leads to a greater weight loss from options that include soccer, tennis, hydro-gymnastics and localized exercises.37
The major strength of this study is relying on a representative sample of Portuguese-speaking residents of mainland Portugal. However, some limitations must be acknowledged. Data regarding the knowledge of the benefits of regular PA was obtained from the recognition of possible benefits from a list, which may have led to an overestimation of knowledge in this domain. In fact, it has been shown that closed-ended questions generally yield higher percentages of responses than open-ended questions,38 and the low proportion of non-respondents in this question appears to support this assumption. Finally, although we evaluated various aspects of regular PA-related awareness and knowledge, we did not evaluate knowledge regarding specific guidelines for regular PA, or whether or not participants engaged in a sufficient amount of health-enhancing PA as specified in the guidelines.9
The present study shows an adequate awareness and knowledge of regular PA among the Portuguese population with differences observed according to age, health literacy levels and frequency of exercise. As such, health education strategies and practices should focus on older individuals, those who have lower levels of health literacy and who do not exercise to improve PA-related awareness and knowledge. Furthermore, considering the most common barriers for regular PA referred, it is important that recommendations for strategies that facilitate regular PA, such as decreasing the price of exercise equipment and gym fees, and increasing access to green spaces in cities, as well as encouraging active transportation along with the creation of safe built environments, be put into practice. Finally, this study provides benchmark data to plan and monitor the effects of health promotion aiming to increase regular PA levels. In fact, considering that nearly half of the population did not exercise, the implementation of public health strategies to overcome barriers, and to improve the population's awareness and knowledge of regular PA are particularly important, as this may lead to increases in regular PA levels.
Acknowledgements
Financial support and sponsorship: This study was supported by FEDER funds through Operational Programme Competitiveness and Internationalization and by national funding from The Portuguese Foundation for Science and Technology – FCT (Portuguese Ministry of Education and Science) within the project (HMSPIISE/SAU-ICT/0004/2009) and the Epidemiology Research Unit – Institute of Public Health, University of Porto (EPIUnit; UIDB/04750/2020). SM was funded under the scope of the project "NEON-PC - Neuro-oncological complications of prostate cancer: longitudinal study of cognitive decline" (POCI-01-0145-FEDER-032358; Ref. PTDC/SAU-EPI/32358/2017). An individual grant attributed to ARC (SFRH/BD/102181/2014) was co-funded by FCT and the “Programa Operacional Capital Humano” (POCH/FSE). The funding sources had no role in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Conflicts of interest
The authors declare no conflicts of interest.
References
- [1].World Health Organization. Global Recommendations on Physical Activity for Health. Geneva, Switzerland: 2010. Available from: https://www.who.int/dietphysicalactivity/global-PA-recs-2010.pdf. [PubMed] [Google Scholar]
- [2].World Health Organization. Physical Activity 2020. Available from: https://www.who.int/news-room/fact-sheets/detail/physical-activity. [Accessed 31 December 2020]. [Google Scholar]
- [3].Popkin B, Kim S, Rusev E, Du S, Zizza C. Measuring the full economic costs of diet, physical activity and obesity-related chronic diseases. Obes Rev. 2006;7:271–293. [DOI] [PubMed] [Google Scholar]
- [4].Hamasaki H. Daily physical activity and type 2 diabetes: a review. World J Diabetes. 2016;7:243–251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Kyu HH, Bachman VF, Alexander LT, et al. Physical activity and risk of breast cancer, colon cancer, diabetes, ischemic heart disease, and ischemic stroke events: systematic review and dose-response meta-analysis for the Global Burden of Disease Study 2013. BMJ. 2016;354:i3857. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Rezende LFM, Sa TH, Markozannes G, et al. Physical activity and cancer: an umbrella review of the literature including 22 major anatomical sites and 770 000 cancer cases. Br J Sports Med. 2018;52:826–833. [DOI] [PubMed] [Google Scholar]
- [7].Swift DL, Johannsen NM, Lavie CJ, Earnest CP, Church TS. The role of exercise and physical activity in weight loss and maintenance. Prog Cardiovasc Dis. 2014;56:441–447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Martin CK, Church TS, Thompson AM, Earnest CP, Blair SN. Exercise dose and quality of life: a randomized controlled trial. Arch Intern Med. 2009;169:269–278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Direção-Geral da Saúde [Directorate-General of Health of Portugal]. Estratégia Nacional para a Promoção da Atividade Física, da Saúde e do Bem-Estar [National Strategy for the Promotion of Physical Activity, Health and Well-Being]. Lisbon, Portugal, 2016. Report No.: Impresso—978-972-675-243-1. [Google Scholar]
- [10].Piercy KL, Troiano RP, Ballard RM, et al. The physical activity guidelines for Americans. JAMA. 2018;320:2020–2028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Lopes C, Torres D, Oliveira A, et al. National Food, Nutrition, and Physical Activity Survey of the Portuguese General Population, IAN-AF 2015-2016, Summary of Results. Porto, Portugal: University of Porto; 2018. [Google Scholar]
- [12].Sarafino EP, Smith TW. Health Psychology: Biopsychosocial Interactions. New Jersey, USA: John Wiley & Sons Inc; 2011. [Google Scholar]
- [13].Kay MC, Carroll DD, Carlson SA, Fulton JE. Awareness and knowledge of the 2008 Physical Activity Guidelines for Americans. J Phys Act Health. 2014;11:693–698. [DOI] [PubMed] [Google Scholar]
- [14].Morrow JR, Jr, Krzewinski-Malone JA, Jackson AW, Bungum TJ, Fitzgerald SJ. American adults’ knowledge of exercise recommendations. Res Q Exerc Sport. 2004;75:231–237. [DOI] [PubMed] [Google Scholar]
- [15].Direção-Geral da Saúde [Directorate-General of Health of Portugal]. Plano Nacional de Saúde Revisão e Extensão a 2020 [National Health Plan Review and Extension to 2020]. Lisbon, Portugal, 2015. [Google Scholar]
- [16].Knox ECL, Esliger DW, Biddle SJH, Sherar LB. Lack of knowledge of physical activity guidelines: can physical activity promotion campaigns do better? BMJ Open. 2013;3:e003633. doi: 10.1136/bmjopen-2013-003633. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Costa AR, Silva S, Moura-Ferreira P, et al. Cancer screening in Portugal: sex differences in prevalence, awareness of organized programmes and perception of benefits and adverse effects. Health Expect. 2017;20:211–220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Moura-Ferreira P, Lunet N, Silva S. A informação sobre saúde dos Portugueses: fontes, conhecimentos e comportamentos [Health information of the Portuguese: sources, knowledge and behavior]. Lisbon, Portugal: Associação para Investigação e Desenvolvimento da Faculdade de Medicina [Association for Research and Development of the Faculty of Medicine]; 2017. [Google Scholar]
- [19].Instituto Nacional de Estatística [Statistics Portugal]. Censos 2001, Resultados Definitivos, XIV Recenseamento Geral da População, IV Recenseamento Geral da Habitacão [2001 Census, Definitive Results, XIV General Population Census, IV General Housing Census]. 2002;Instituto Nacional de Estatística [Statistics Portugal], Lisbon, Portugal., [Google Scholar]
- [20].Weiss BD, Mays MZ, Martz W, et al. Quick assessment of literacy in primary care: the Newest Vital Sign. Ann Fam Med. 2005;3:514–522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Paiva D, Silva S, Severo M, Moura-Ferreira P, Lunet N, Azevedo A. Limited health literacy in Portugal assessed with the Newest Vital Sign. Acta Med Port. 2017;30:861–869. [DOI] [PubMed] [Google Scholar]
- [22].Ainsworth BE, Haskell WL, Herrmann SD, et al. 2011 Compendium of Physical Activities: a second update of codes and MET values. Med Sci Sports Exerc. 2011;43:1575–1581. [DOI] [PubMed] [Google Scholar]
- [23].Fredriksson SV, Alley SJ, Rebar AL, Hayman M, Vandelanotte C, Schoeppe S. How are different levels of knowledge about physical activity associated with physical activity behaviour in Australian adults? PLoS One. 2018;13:e0207003. doi: 10.1371/journal.pone.0207003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Veluswamy SK, Maiya AG, Nair S, Guddattu V, Nair NS, Vidyasagar S. Awareness of chronic disease related health benefits of physical activity among residents of a rural South Indian region: a cross-sectional study. Int J Behav Nutr Phys Act. 2014;11:27.doi: 10.1186/1479-5868-11-27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Doyle CB, Khan A, Burton NW. Knowledge of physical activity guidelines and mental health benefits among Emirati university students. Perspect Public Health. 2019;139:316–319. [DOI] [PubMed] [Google Scholar]
- [26].Riecher-Rossler A. Sex and gender differences in mental disorders. Lancet Psychiatry. 2017;4:8–9. [DOI] [PubMed] [Google Scholar]
- [27].Wheeler PC, Mitchell R, Ghaly M, Buxton K. Primary care knowledge and beliefs about physical activity and health: a survey of primary healthcare team members. BJGP Open. 2017;1: doi: 10.3399/bjgpopen17X100809. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].World Health Organization. Prevalence of Insufficient Physical Activity Among Adults; 2018. Available from: http://apps.who.int/gho/data/node.main.A893?lang=en. [Accessed 01 August 2019]. [Google Scholar]
- [29].Cerin E, Leslie E, Sugiyama T, Owen N. Perceived barriers to leisure-time physical activity in adults: an ecological perspective. J Phys Act Health. 2010;7:451–459. [DOI] [PubMed] [Google Scholar]
- [30].Herazo-Beltran Y, Pinillos Y, Vidarte J, Crissien E, Suarez D, Garcia R. Predictors of perceived barriers to physical activity in the general adult population: a cross-sectional study. Braz J Phys Ther. 2017;21:44–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Hoare E, Stavreski B, Jennings GL, Kingwell BA. Exploring motivation and barriers to physical activity among active and inactive Australian adults. Sports (Basel). 2017;5:47.doi: 10.3390/sports5030047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Azevedo MR, Araújo CL, Reichert FF, Siqueira FV, da Silva MC, Hallal PC. Gender differences in leisure-time physical activity. Int J Public Health. 2007;52:8–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].European Commission. Special Eurobarometer 472 “Sport and Physical Activity”. Brussels, Belgium: 2018. Available from: https://ec.europa.eu/commfrontoffice/publicopinion/index.cfm/survey/getsurveydetail/instruments/special/surveyky/2164. [Google Scholar]
- [34].Craft BB, Carroll HA, Lustyk MK. Gender differences in exercise habits and quality of life reports: assessing the moderating effects of reasons for exercise. Int J Lib Arts Soc Sci. 2014;2:65–76. [PMC free article] [PubMed] [Google Scholar]
- [35].van Uffelen JGZ, Khan A, Burton NW. Gender differences in physical activity motivators and context preferences: a population-based study in people in their sixties. BMC Public Health. 2017;17:624. doi: 10.1186/s12889-017-4540-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [36].Monteiro CA, Conde WL, Matsudo SM, Matsudo VR, Bonsenor IM, Lotufo PA. A descriptive epidemiology of leisure-time physical activity in Brazil. Rev Panam Salud Publica. 2003;14:246–254. [DOI] [PubMed] [Google Scholar]
- [37].Domingues MR, Araújo CP. Conhecimento e percepção sobre exercício físico em uma população adulta urbana do sul do Brasil [Knowledge and perception about physical exercise in an urban adult population in southern Brazil]. Cad Saúde Pública. 2004;20:204–215. [DOI] [PubMed] [Google Scholar]
- [38].Reja U, Manfreda K, Hlebec V, Vehovar V. Open-ended vs. close-ended questions in web questionnaires. Adv Methodol Stats (Metodoloski zvezki). 2003;19:159–177. [Google Scholar]