

The University of Alberta Pediatric HIV Clinic serves an area with an estimated population of 1.2 million, with 25 000 births annually. Records were reviewed from Jan. 1, 1988, to Dec. 31, 1999, for all children born in northern Alberta to women with HIV infection to determine our success rate at preventing perinatal HIV transmission. A child was considered to be HIV infected if he or she had 2 positive HIV polymerase chain reaction (PCR) results from tests performed on separate blood samples. A child was considered to be uninfected if she or he had seroreverted or had 2 negative HIV PCR results at 1 or more months of age, with 1 being obtained at 4 or more months.1 Indeterminate HIV status was assigned to a child who had a single negative HIV PCR result or had not been tested at 4 or more months of age. The ethnicity of the mothers was also recorded by clinic physicians to determine whether there was an identifiable high-risk group that could be targeted in programs aimed at preventing the transmission of HIV to young women.
Forty-three women had HIV infection that was diagnosed prior to labour (Fig. 1). The antiretrovirals given during pregnancy consisted of zidovudine alone in 20 cases, 2 reverse transcriptase inhibitors in 6 cases, a protease inhibitor with 2 reverse transcriptase inhibitors in 7 cases and a nonnucleotidase reverse transcriptase inhibitor with 2 reverse transcriptase inhibitors in 4 cases. When mothers were treated with antiretrovirals during pregnancy and intrapartum, 31 of 36 babies (86%) were not HIV infected. All infants received at least some oral zidovudine in the first 6 weeks of life, except in 2 cases in which the mothers refused all treatment. Five infants received more than one antiretroviral drug as HIV perinatal prophylaxis.
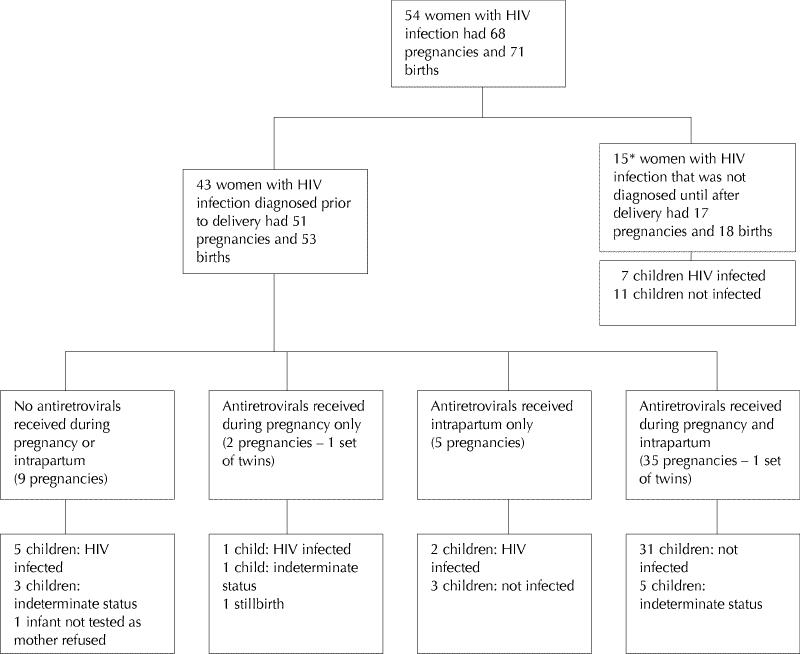
Fig. 1: HIV status of 71 infants born to HIV-infected women in northern Alberta. *Two of these women had 2 pregnancies before being tested. Four of these women had further pregnancies and births and are, therefore, also included in the group whose HIV infection was diagnosed prior to delivery.
Fig. 1 also shows the HIV status of 18 children born to women who had HIV infection at the time of delivery but whose infection was diagnosed after delivery (2 women had 2 pregnancies before being tested). Forty percent of these children (n = 7) were HIV infected. Positive HIV status before delivery was deduced either because older siblings were subsequently found to be HIV infected or because these children were still HIV seropositive when first seen in our clinic. These children were all under 6 years of age when first seen and had no other risk factors for acquiring HIV infection.
Routine screening for HIV during pregnancy was in place for 16 months prior to these data being compiled. Eleven of the women in our study (20%) were found to be HIV infected through this screening process.
Whereas only about 6% of the population of northern Alberta are Aboriginal, 68% of all the children in the study were Aboriginal (Fig. 2). Furthermore, 62% (n = 21) of the 34 Aboriginal women who were tested for hepatitis C were positive (55% [n =28] of the 51 HIV-infected women who were tested for hepatitis C were positive). This is much higher than the 30% hepatitis C seroprevalence that has been reported in nonpregnant HIV-infected women at the southern Alberta HIV clinic.2 This suggests that injection drug use is an important HIV risk factor for Aboriginal women in northern Alberta.
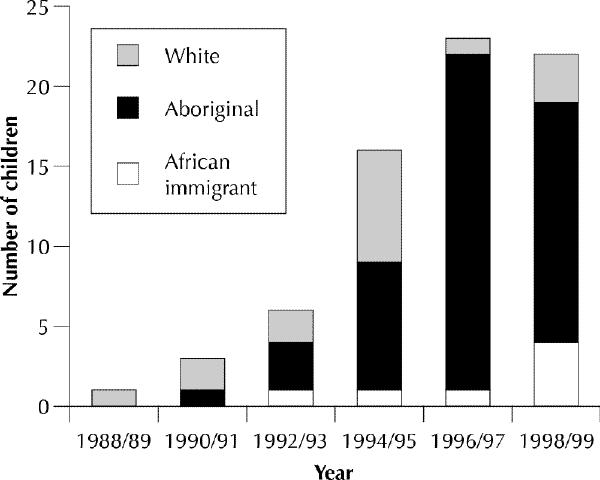
Fig. 2: Maternal ethnicity of 71 children born to 54 HIV-infected mothers in northern Alberta, as recorded by clinic physicians.
This group of women with HIV infection also included 6 immigrants from Africa. Physicians may fail to recognize the high prevalence of HIV infection in women of childbearing age from sub-Saharan Africa. The 6 such mothers in our study were diagnosed through prenatal screening (4 cases), screening for insurance purposes (1 case) and contact tracing (1 case) rather than because a physician recognized that they were at high risk for HIV infection.
Our study provides information confirming the usefulness of screening for HIV in pregnancy given the availability of effective treatments to prevent perinatal transmission. Furthermore, our findings regarding the ethnicity of HIV-positive and hepatitis C-positive mothers suggest a need for public health programs aimed at reducing the burden of these illnesses among Aboriginal women of reproductive age.
Footnotes
Acknowledgement: We thank Dr. Stan Houston for suggesting we do this study.
Reprint requests to: Dr. Joan L. Robinson, 2C3 Walter Mackenzie Centre, Edmonton AB T6R 2B7; fax 780 407-7136; jr3@gpu.srv.ualberta.ca
References
- 1.Antiretroviral therapy and medical management of pediatric HIV infection. A 1997 USPHS/IDSA report on the prevention of opportunistic infections in persons infected with human immunodeficiency virus. Pediatric AIDS Foundation, the National Institute of Child Health & Human Development, NIH and USDHHS. Pediatrics 1998;102(Suppl 4):1009. [PubMed]
- 2.Johns DG, Gill MG. Seroprevalence of cytomegalovirus, Toxoplasma gondii, syphilis and hepatitis B and C virus infections in a regional population seropositive for HIV infection. Can J Infect Dis 1998;9:209-14. [DOI] [PMC free article] [PubMed]