

Abstract
This national cohort study examines changes in the number of vascular surgical procedures completed in the US before and during the COVID-19 pandemic.
Multicenter reports suggest that emergency coronary and cerebral revascularizations have decreased in the US during the COVID-19 pandemic, prompting concerns about unmet cardiovascular care needs.1,2,3 This study sought to quantify national trends in vascular surgical practice during the COVID-19 pandemic.
Methods
Monthly volumes for aortic interventions, carotid interventions, and lower extremity interventions (LEIs) from June 2018 to June 2020 were queried from the Vascular Quality Initiative, a prospectively maintained national database. The study was approved by the Stanford University institutional review board with a waiver of consent (because of the retrospective review of deidentified data) and followed STROBE guidelines for observational studies. Of 620 centers, 206 were included for continuous participation. We compared monthly procedure rates by urgency in a pandemic cohort (January 2020 through June 2020) with a historical cohort (January 2019 through June 2019) using χ2 and t tests. Data analysis was completed with Pycharm version 2020.1.4 (JetBrains). A significant threshold of P < .05 was used for 2-tailed tests.
Results
The pandemic cohort included 24 979 procedures: 14 292 LEIs (57.2%), 7475 carotid interventions (29.9%), and 3212 aortic interventions (12.9%). Patients treated during the pandemic were more likely to use Medicare as a primary insurer (carotid interventions: pandemic, 4783 [64.2%] vs historical, 5198 [53.4%]; aortic interventions: pandemic, 2070 [64.4%] vs historical, 2459 [54.4%]; LEIs: pandemic, 8422 [58.9%] vs historical, 8830 [49.8%]; all P < .001) (Table). In the LEI cohort, patients treated during the pandemic were more likely to be transferred (pandemic, 341 [11.8%] vs historical, 323 [8.7%]) and have a history of congestive heart failure (pandemic, 3334 [23.3%] vs historical, 3654 [20.6%]; P < .001), dialysis (pandemic, 1428 [10.5%] vs historical, 1633 [9.7%]; P = .02), or anticoagulation (pandemic, 3459 [24.1%] vs historical, 3825 [21.6%]; P < .001).
Table. Comparison of Historical Cohort (January 2019-June 2019) and Pandemic Cohort (January 2020-June 2020) by Urgency.
| Characteristic | Carotid interventiona | Aortic intervention | Lower extremity intervention | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Pandemic | Historical | P value | Pandemic | Historical | P value | Pandemic | Historical | P value | |
| No. | 7475 | 9747 | NA | 3212 | 4521 | NA | 14 292 | 17 716 | NA |
| Urgency | |||||||||
| Emergency | 3319 (44.4) | 3863 (39.6) | <.001 | 330 (10.3) | 427 (9.4) | .008 | 330 (2.3) | 371 (2.1) | <.001 |
| Urgent | NA | NA | 420 (13.1) | 477 (10.5) | 2692 (18.8) | 2325 (13.1) | |||
| Elective | 4156 (55.6) | 5884 (61.4) | 2462 (76.6) | 3617 (80.0) | 11 270 (78.8) | 15 020 (84.8) | |||
| Age, mean (SD), y | 70.7 (9.6) | 70.6 (9.6) | .62 | 70.9 (11.3) | 71.4 (10.7) | .03 | 68.2 (11.2) | 68.2 (11.1) | .65 |
| Female | 2762 (36.9) | 3628 (37.2) | .73 | 827 (25.7) | 1086 (24.0) | .10 | 5371 (37.5) | 6713 (37.9) | .51 |
| BMI, mean (SD) | 28.6 (5.8) | 28.6 (5.9) | .74 | 28.1 (6.4) | 28.1 (6.3) | .96 | 27.7 (6.2) | 27.8 (6.2) | .03 |
| Primary insurer | |||||||||
| Medicare | 4783 (64.2) | 5198 (53.4) | <.001 | 2070 (64.4) | 2459 (54.4) | <.001 | 8422 (58.9) | 8830 (49.8) | <.001 |
| Medicaid | 285 (3.8) | 404 (4.1) | 158 (4.9) | 174 (3.8) | 1195 (8.4) | 1397 (7.9) | |||
| Commercial | 2136 (28.7) | 3867 (39.7) | 860 (26.8) | 1709 (37.8) | 3767 (26.4) | 6668 (37.6) | |||
| Military/Veterans Affairs | 133 (1.8) | 134 (1.4) | 62 (1.9) | 80 (1.8) | 237 (1.7) | 232 (1.3) | |||
| Non-US | 6 | 3 | 1 | 1 | 1 | 2 | |||
| Self-pay | 109 (1.5) | 133 (1.4) | 59 (1.8) | 96 (2.1) | 268 (1.9) | 290 (1.6) | |||
| Transferred | 755 (10.1) | 857 (8.8) | .003 | 530 (16.5) | 696(15.4) | NA | 341 (11.8) | 323 (8.7) | NA |
| Residential status | |||||||||
| Home | 7379 (98.7) | 9619 (98.7) | .92 | 3178 (98.9) | 4477 (99.0) | .65 | 13 219 (92.4) | 16 650 (94.0) | .41 |
| Nursing home | 87 (1.2) | 118 (1.2) | 30 (0.9) | 34 (0.8) | 553 (3.9) | 684 (3.9) | |||
| Homeless | 8 (0.1) | 9 | 4 (0.1) | 7 (0.2) | 55 (0.4) | 54 (0.3) | |||
| Coronary artery disease | 2555 (34.2) | 3176 (32.6) | .03 | 810 (25.2) | 1155 (25.6) | .74 | 4144 (34.3) | 5330 (47.9) | <.001 |
| Congestive heart failure | 1014 (13.6) | 1297 (13.3) | .62 | 408 (12.7) | 583 (12.9) | .79 | 3334 (23.3) | 3654 (20.6) | <.001 |
| Chronic obstructive pulmonary disease | 1709 (22.9) | 2441 (25.0) | .25 | 1085 (33.8) | 1518 (33.6) | .86 | 4030 (28.2) | 5040 (28.5) | .64 |
| Diabetes | 1741 (36.0) | 2485 (37.2) | .001 | 590 (18.4) | 874 (19.4) | .28 | 7805 (87.6) | 9441 (86.8) | .12 |
| Dialysis | 104 (2.1) | 118 (1.8) | .14 | 56 (12.2) | 82 (13.4) | .57 | 1428 (10.5) | 1633 (9.7) | .02 |
| Hypertension | 6677 (89.4) | 8762 (90) | .22 | 2702 (85.0) | 3815 (84.8) | .82 | 12 573 (88.9) | 15 613 (88.3) | .08 |
| Smoking history | 5458 (73.1) | 7197 (73.8) | .23 | 2656 (82.8) | 3801 (84.3) | .08 | 11 294 (79.1) | 14 229 (80.3) | .006 |
| Statin | 6826 (91.4) | 8803 (90.3) | .02 | 2309 (72.0) | 3171 (70.4) | .13 | 11 657 (81.6) | 14 263 (80.5) | .02 |
| P2Y12 inhibitor use | 4293 (57.4) | 5253 (53.9) | <.001 | 474 (14.8) | 651 (14.5) | .71 | 6351 (44.4) | 7767 (43.9) | .30 |
| Anticoagulation | 1013 (13.6) | 1359 (13.9) | .46 | 488 (15.2) | 691 (15.3) | .91 | 3459 (24.1) | 3825 (21.6) | <.001 |
Abbreviations: BMI, body mass index (calculated as weight in kilograms divided by height in meters squared); NA, not applicable.
Carotid revascularizations were categorized as urgent or elective.
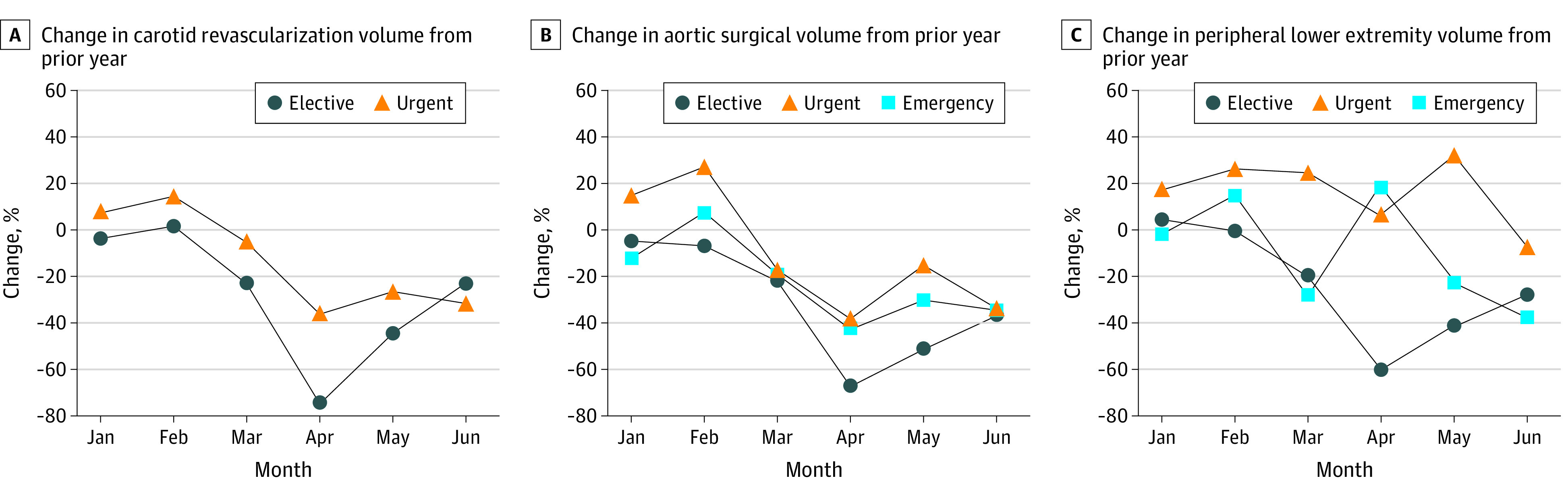
Pandemic-period elective LEI volumes fell by 20.3% (before the pandemic, 2442 procedures; during the pandemic, 1945 procedures) to 60.0% (before, 2590; during, 1036) from March to June 2020 (P < .001), while emergency LEIs increased by 18.6% (before, 53; during, 63) in April 2020 (P = .03) and urgent LEI volumes increased by 20.3% (before, 364; during, 452) and 32.4% (before, 392; during, 519) in March and May 2020, respectively (P < .001). Conversely, pandemic-period carotid procedures demonstrated statistically significant decline across elective procedures (April: before, 1071; during, 263; decline, 75.4%; May: before, 1027; during, 556; decline, 45.8%; June: before, 943; during, 732; decline, 22.3%; P < .001) and urgent procedures (March: before, 626; during, 594; decline, 5.1%; April: before, 660; during, 423; decline, 35.9%; May: before, 684; during, 503; decline, 26.5%; June: before, 679; before, 461; decline, 32.1%; P < .001). Aortic procedures declined significantly across elective indications (March: before, 598; during, 463; decline, 22.5%; P = .04; April: before, 596; during, 191; decline, 68.0%; May: before, 666; during, 324; decline, 51.4%; June: before, 561; during, 358; decline, 36.2%; P < .001 for April through June), urgent indications (March: before, 77; during, 65; decline, 17.7%; P = .01; April: before, 81; during, 55; decline, 38.8%; P = .01; May: before, 101; during, 86; decline, 14.9%; June: before, 62; during, 40; decline, 36.1% decline; P < .001 for May and June), and emergency indications (May: before, 63; during, 44; decline, 30.1%; June: before, 63; during, 41; decline, 34.8%; P < .001) (Figure).
Figure. Percentage Difference in Monthly National Surgical Volumes From January to June 2020, Compared With the Year Prior.
Discussion
Compared with historical volumes, urgent and emergency LEIs increased in March, April, and May 2020 as the COVID-19 pandemic surged in the US. Possible causes for increased urgent and emergency LEIs include COVID-19 infection, which has been associated with thrombotic complications, including lower extremity ischemia. Additionally, delayed care may contribute to urgent or emergency LEIs. In a national survey from the National Center for Health Statistics from April to July 2020, 38.7% to 41.5% of households reported a delay in medical care in the prior month because of COVID-19. In Italy and the Netherlands, a reduction in elective LEIs during the pandemic was associated with patients presenting with higher peripheral artery disease severity and increased rates of major amputations.4,5 That patients treated during the pandemic in this analysis were more likely to have severe comorbidities and be transferred from another institution may indicate a shift toward treating those in more dire medical states than in the prepandemic period.
While declines in elective procedures were expected, concurrent declines in urgent and emergency aortic and carotid interventions throughout the study period were not expected. Because the pandemic is unlikely to reduce incidence of aortic rupture or symptomatic carotid disease, this is more likely because to reduced access to care. Aortic rupture in particular is a time-sensitive condition with significant prehospital mortality, and the additional burden of COVID-19 may hinder expedient transfer and resuscitation efforts, causing excess deaths. Indeed, national reports have identified that 34% of excess deaths during the pandemic cannot be attributed to COVID-19 alone.6
Limitations
Study limitations include the retrospective observational approach, which prohibits the determination of causality. Variables such as surgical urgency were clinician reported and thus vulnerable to error. Additionally, the COVID-19 status of patients is unknown. Reduced surgical volumes could be confounded by reduced reporting during quarantine, although this would be expected to negatively affect urgent and emergency volumes, where an increase was actually observed for LEIs.
Conclusions
While elective and emergency interventions for aortic and carotid disease decreased throughout the COVID-19 pandemic, nonelective revascularization for acute limb ischemia increased in March to May 2020. Future research should examine potential adverse effects of these trends.
References
- 1.Garcia S, Albaghdadi MS, Meraj PM, et al. Reduction in ST-segment elevation cardiac catheterization laboratory activations in the United States during COVID-19 pandemic. J Am Coll Cardiol. 2020;75(22):2871-2872. doi: 10.1016/j.jacc.2020.04.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Uchino K, Kolikonda MK, Brown D, et al. Decline in stroke presentations during COVID-19 surge. Stroke. 2020;51(8):2544-2547. doi: 10.1161/STROKEAHA.120.030331 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.National Center for Health Statistics, US Centers for Disease Control and Prevention . Reduced access to care: household pulse survey. Published September 22, 2020. Accessed October 1, 2020. https://www.cdc.gov/nchs/covid19/pulse/reduced-access-to-care.htm
- 4.Schuivens PME, Buijs M, Boonman-de Winter L, et al. Impact of the COVID-19 lockdown strategy on vascular surgery practice: more major amputations than usual. Ann Vasc Surg. 2020;69:74-79. doi: 10.1016/j.avsg.2020.07.025 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Sena G, Gallelli G. An increased severity of peripheral arterial disease in the COVID-19 era. J Vasc Surg. 2020;72(2):758. doi: 10.1016/j.jvs.2020.04.489 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rossen LM, Branum AM, Ahmad FB, Sutton P, Anderson RN. Excess deaths associated with COVID-19, by age and race and ethnicity—United States, January 26-October 3, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:1522-1527. doi: 10.15585/mmwr.mm6942e2 [DOI] [PMC free article] [PubMed] [Google Scholar]