

Abstract
Background:
Herbal supplements and particularly multi-ingredient products have become increasingly common causes of acute liver injury. Green tea is a frequent component in implicated products, but its role in liver injury is controversial.
Methods:
Among 1414 patients enrolled in the U.S. Drug Induced Liver Injury Network who underwent formal causality assessment, 40 cases (3%) were attributed to green tea, 202 to dietary supplements without green tea, and 1142 to conventional drugs. The clinical features of green tea cases and representation of HLA class I and II alleles in cases and controls were analyzed in detail.
Results:
Patients with green tea-associated liver injury ranged in age from 17 to 69 years (median = 40) and developed symptoms 15 to 448 days (median = 72) after starting the implicated agent. The liver injury was typically hepatocellular (95%) with marked serum aminotransferase elevations and only modest increases in alkaline phosphatase. Most patients were jaundiced (83%) and symptomatic (88%). The course was judged as severe in 14 patients (35%), necessitating liver transplantation in 3 (8%), but rarely resulting in chronic injury (3%). In three instances, injury recurred upon re-exposure to green tea with similar clinical features but shorter time to onset. HLA typing revealed a high prevalence of HLA-B*35:01, found in 72% (95% CI: 58% to 87%) of green tea cases but only 15% (95% CI: 10% to 20%) caused by other supplements and 12% (95% CI: 10% to 14%) attributed to drugs, the latter rate being similar to population controls (95% CI: 11%: 10.5% to 11.5%).
Conclusions:
Green tea-related liver injury has distinctive clinical features and close association with HLA-B*35:01 suggesting that it is idiosyncratic and immune-mediated.
Introduction
Herbal and dietary supplements have become common causes of drug-induced liver injury in the United States and now are implicated in 15% to 20% of cases (1,2). This change coincides with the increasing use of herbal medications (3), particularly for conditions such as obesity, fatigue and complications of aging that are poorly responsive to conventional drugs.
From a regulatory standpoint, herbal supplements are considered “generally safe” and are not regulated as drugs or subjected to rigorous assessment of efficacy and safety (4,5). In the past, herbal supplements were typically single botanical entities, such as ginseng, saw palmetto or turmeric, which are widely used and have a long history of safety. A recent change has been the popularity of multi-ingredient products, containing mixtures of botanicals, vitamins, minerals, and other nutrients. In ongoing analyses of dietary supplement-associated liver injury from the U.S. Drug-Induced Liver Injury Network (DILIN), multi-ingredient products accounted for 68% of implicated dietary supplements, whereas single component botanicals accounted for only 16% (3). In addition, chemical analyses show that product labels of these multi-ingredient products are often inaccurate: many containing unlisted substances and not containing many of those that are listed (6,7).
Green tea (Camellia sinensis) is a frequent component in multi-ingredient products and has been implicated in several dozen instances of liver injury (8–18). These reports were initially viewed with skepticism (11,19), as green tea is one of the most frequently consumed beverages world-wide and has been used for centuries without known ill effects. Indeed, epidemiological surveys suggest that drinking green tea may have health benefits (19–21) and in vivo studies in animal models show that it may protect against hepatotoxicity (22). Importantly, most reports on hepatotoxicity have implicated tablets or capsules with green tea extract rather than its ingestion as a beverage. Aqueous/alcohol extracts from leaves of Camellia sinensis concentrate the polyphenolic catechins of green tea leaves and remove other components such as caffeine. The catechins in a single commercial tablet labelled as green tea extract may be equivalent to 3 to 10 cups of green tea (23). Epigallocatechin gallate (EGCG) is the most common catechin in green tea and is widely believed to be responsible for the liver injury (19,24,25).
The aim of the current study was to better characterize the frequency, risk factors, clinical features, outcomes, and pathogenesis of green tea-associated liver injury. Using a large prospective U.S. database, we have analyzed cases of dietary supplement-associated liver injury for the role of green tea and describe the clinical features of the injury as well as results of HLA typing of patients and chemical analysis of implicated products.
Materials and Methods
DILIN is an NIH-funded, prospective study of incident cases of suspected drug-induced liver injury presenting at 5 to 8 medical centers in the United States (26) (Supplementary Table 1). The clinical protocols and methods of DILIN have been described in detail (26–28). In brief, patients presenting with suspected drug-induced liver injury are offered enrollment in a prospective, observational study (NCT00345930). After informed consent, patients undergo medical history, physical examination and chart review for relevant data on the liver injury. Blood samples are obtained for routine liver tests and storage for future mechanistic studies. If a liver biopsy was done as a part of clinical care, unstained slides are requested for standardized central reading (29). Starting in 2009, patients were asked to provide samples of the implicated supplements which were sent to a repository, entered into a database, photographed, and aliquoted (6). All details of the DILIN Prospective Study were approved by Institutional Review Boards at participating centers and by an independent Data Safety and Monitoring Board established by NIDDK to supervise the study.
For this analysis, all cases of dietary supplement-related liver injury were reviewed for evidence from the medical history and product labels that green tea was taken. When the product label was not available, the ingredients were sought from the Dietary Supplement Label Database (30) or the internet. All cases with suspected exposure were then re-adjudicated specifically for green tea causality using the procedures established by DILIN, in which 3 investigators review the narrative history and case report forms and score the likelihood that green tea played a role in causation, as 1 (definite, >95% likelihood), 2 (highly likely, 75–95% likelihood), 3 (probable, 50–74%), 4 (possible, 25–49%) or 5 (unlikely, <25%) (26). The investigators based the scores on clinical information only, without knowledge of the chemical analyses or genetic results. Severity was graded using pre-established criteria: 1+ or mild indicating anicteric liver injury (bilirubin <2.5 mg/dL); 2+ moderate indicating jaundice but without hospitalization; 3+ moderate indicating jaundice and hospitalization; 4+ severe indicating jaundice and signs of liver failure (such as INR above 1.5); and 5+ fatal indicating death or urgent liver transplantation within 6 months of onset (27).
Cases scored as definite, highly likely or probable liver injury due to green tea were assessed for demographic, clinical, biochemical and histologic features (29) and for the chemical constituents found on testing product samples. Chemical analysis was performed at the National Center for Natural Products Research of the University of Mississippi using ultra-high-performance liquid chromatography coupled to quadrupole time-of-flight mass spectrometry (6).
To investigate HLA associations, patients who consented for genetic research had high resolution Class I and II HLA sequencing done on DNA extracted from whole blood using the Illumina MiSeq platform at the Vanderbilt University Medical Center Immunogenomics, Microbial Genetics and Single Cell Technologies core (31). Two disease control groups were used: (1) patients enrolled in DILIN with liver injury related to dietary supplements without green tea and (2) patients with liver injury attributed to conventional drugs. For population controls, the Illumina Human660W-Quad chip genotype data from the Electronic Medical Record and Genomics Study (eMERGE) network (phs000360.v3.p1) were obtained from dbGaP (32). The eMERGE cohort consisted of individuals residing in the United States of diverse racial and ethnic background, but with predominantly Americans of European ancestry. The chromosome 6 single nucleotide polymorphisms (SNPs) in the major histocompatibility region were used to impute four-digit HLA alleles using the HLA Genotype Imputation with Attribute Bagging (HIBAG) program (33). Analysis of HLA class I and II associations between green tea cases and each control group was conducted using Fisher exact tests. To correct for multiple testing, top alleles were selected based on a false discovery rate of <0.05 (34). The major associations were also examined separately for European-American and Hispanic subgroups of the green tea cases and population controls from eMERGE. Statistical analyses used SAS9.4 (SAS Inc., Cary, NC) and R. Allele frequencies were also compared to those of large ethnic-matched U.S. population cohorts reported in public databases (35).
Results
Among 1987 patients enrolled in the DILIN Prospective Study between September 2004 and April 2018, 1768 had undergone follow up and causality assessment, of which 1414 were judged as probable, highly likely or definite drug induced liver injury. Of these verified cases, 272 (19%) were attributed to dietary supplements and 1142 to conventional drugs (Figure 1). Review of product labels of implicated agents for mention of green tea or its component catechins identified 70 patients as possibly having taken at least one product containing green tea.
Figure 1.
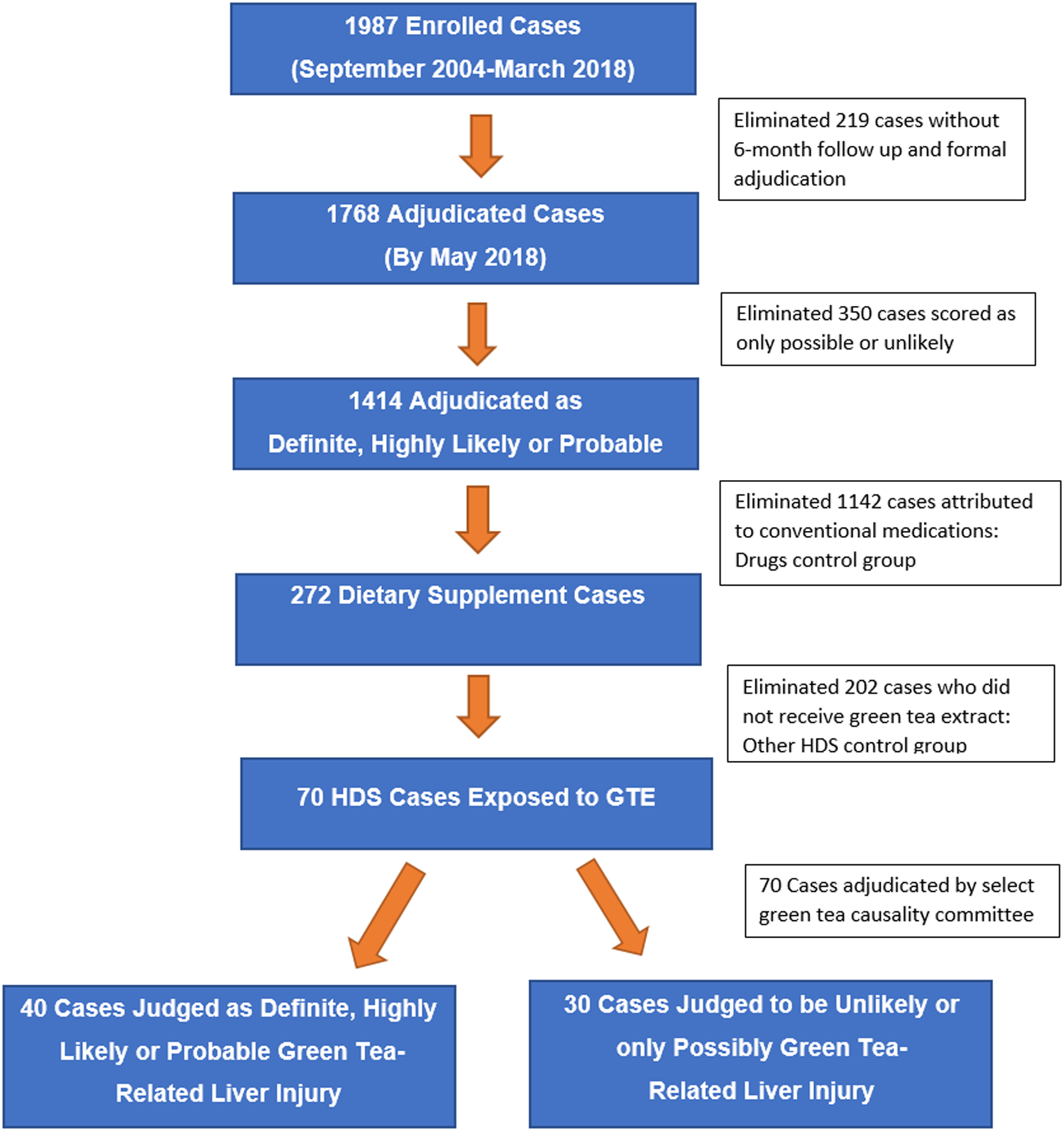
Consort diagram showing the development of the control groups and final cases adjudicated for green tea causality.
Formal adjudication of the 70 potential cases by the green tea causality assessment committee scored 3 as definite,11 as highly likely and 26 as probable-green tea related. The 30 cases scored as only possible or unlikely included 7 for which further analysis could not demonstrate that green tea was taken, while in the remaining cases, alternative diagnoses were judged more or equally likely.
The demographic, clinical, and biochemical features of the 40 cases of green tea-related liver injury are given in Table 1. Three patients had a previous history of liver injury after taking a green tea containing supplement, two of whom were enrolled in DILIN twice, the second episode 1 to 4 years after the initial one. Thus, there were 40 episodes of liver injury in 38 different patients. The patients’ median age at the time of onset was 40 years, 74% were women, most were white, and 36% were of self-reported Hispanic ethnicity. The primary implicated product was green tea extract alone in 8 (20%) and a multi-ingredient product in 32 (80%) instances. The multi-ingredient supplements had 4 to 60 active ingredients (median = 11.5) and only 7 (22%) had “green tea” in their commercial names (Supplementary Table 2). Green tea was present as an extract in tablet or capsule form in all products except 2, one of which was provided as a powder to make tea and the other as a liquid spray. The stated reason for taking the supplement was weight loss in 29 (73%), boosting energy in 4 (10%), promoting “wellness” in 2 (5%), body building in 2 (5%) and miscellaneous or unknown in 3. Nine patients were found to be taking 2 separate green tea-containing products. Only 17 products (from 15 patients) had labels that provided the dose of green tea extract per serving. Total estimated daily doses ranged from 50 to 2000 mg (median = 800 mg). In this small subset, there was no clear correlation between the total estimated daily intake and the severity of the injury as assessed by severity scores or peak bilirubin levels (data not shown).
Table 1.
Features of 40 Cases of Green Tea Related Liver Injury in 38 Patients
| Feature | Median (range) or No. (%) |
|---|---|
| Age | 40 (17–69) years |
| Sex, Female | 28/38 (74%) |
| Race, White | 26/38 (70%) |
| Hispanic ethnicity | 13/37 (36%) |
| Multi-ingredient supplement | 32 (80%) |
| Weight Loss Indication | 29 (73%) |
| Symptoms, any | 38 (95%) |
| Jaundice | 33 (83%) |
| Rash | 5 (13%) |
| Fever | 3 (8%) |
| Eosinophilia (>500/μL) | 1 (3%) |
| Initial Alanine Aminotransferase | 1621 (396–4185) U/L |
| Initial Asparate Aminotransferase | 1298 (162–3400) U/L |
| Initial Alkaline Phosphatase | 155 (80–550) U/L |
| Initial Total Bilirubin | 7.0 (0.4–30.1) mg/dL |
| Peak Total Bilirubin | 13.6 (0.6–46.0) mg/dL |
| Peak INR | 1.2 (1.0–7.0) |
| Antinuclear or Smooth Muscle Antibody | 18/39 (46%) |
| Initial R ratio | 24.0 (3.3–67.0) |
| Hepatocellular (R > 5) | 38 (95%) |
| Mixed (R 2–5) | 2 (5%) |
| Cholestatic (R < 2) | 0 (0%) |
| Severity: Mild (1+: Anicteric) | 5 (13%) |
| Chronicity | 1/29 (3%) |
Two patients were enrolled twice, having two episodes of liver injury after separate exposures to green tea. All results are median (range) or number (proportion) with denominator given when there are missing data. Severity was scored in the DILIN Prospective Study as mild (1+, anicteric), moderate (2+, jaundiced or 3+, jaundiced and hospitalized), or severe (4+, jaundiced and INR >1.5) or fatal (5+, death from liver failure or liver transplantation within 6 months of onset). R = alanine aminotransferase ÷ alkaline phosphatase, both expressed as multiples of the upper limit of the normal range.
Laboratory results demonstrated marked elevations in serum alanine and aspartate aminotransferase (ALT and AST) levels with only modest increases in alkaline phosphatase levels so that all except two subjects (95%) had a hepatocellular pattern of enzyme elevations; two subjects having a “mixed” and none a cholestatic pattern (25). Immunologic features were not prominent, only 5 patients reported rash and 3 fever with none having both, and only one subject had peripheral eosinophilia, which was mild (7.3%: 511/μL). The severity of the liver injury was scored as mild in 5 (13%), moderate in 21 (52%), and severe in 14 (35%) cases; 3 of the latter developing hepatic failure and undergoing liver transplantation. No patient died. Follow up of 4 to 12 months after onset was available for 29 patients, 28 of whom had normal liver tests, while one had a modest increase in ALT levels (57 U/L) 10 months after onset. Overall, green tea accounted for 15% of dietary supplement-related and 3% of all cases in the DILIN Prospective Study.
Selected clinical and laboratory features of the patients with green tea injury are compared to those with liver injury due to other HDS products (n=202) and those with injury attributed to a conventional medication (n=1142) in Supplementary Table 3. The patients with green tea injury differed from the other groups in being younger than patients with drug-induced liver injury, more likely to be women than the other HDS cases and somewhat more likely to be Hispanic compared to both groups. These differences were probably related to differences in reasons for taking the products – for weight loss rather than a specific medical condition. Most strikingly, the green tea cases were mostly hepatocellular (95%) and none were cholestatic, whereas other HDS cases and those due to drugs included more cholestatic (22% and 24%) and mixed cases (25% and 23%). The severity and outcome of green tea cases was somewhat worse than those of other HDS- and drug-related cases, but evidence for chronicity was less common in green tea cases (3%), particularly in comparison of those due to conventional drugs (18%).
Liver biopsies from 15 patients (38%) were reviewed centrally. An acute hepatitis-like pattern was seen in 12 subjects, 4 of which showed mild cholestasis. Eosinophils were prominent in 11 biopsies and mild to moderate steatosis in 6 cases while fibrosis was rare. An explant from a patient undergoing liver transplantation revealed severe hepatitis with massive necrosis. The remaining 2 patients had atypical findings with minimal inflammation and necrosis; one had bland cholestasis and one glycogenosis.
Chemical analyses were available on 16 products provided by 15 patients. Catechins typical of green tea were detected in all but 1 product (Supplementary Table 4), the amount per serving ranging from 6.6 to 384 mg. The product without detectable catechins was a “diet spray” labelled as having green tea but without providing its concentration.
HLA testing was performed on 36 of the 38 patients judged to have definite, highly likely or probable green tea-related liver injury, as well as 17 possible and 12 unlikely cases, 192 control cases receiving other supplements, and 1113 cases attributed to conventional drugs. In addition, HLA alleles were imputed for 15,094 controls from eMERGE. Four HLA alleles showed significant association with green-tea cases in comparison to the three control groups of which HLA-B*35:01 and HLA-C*04:01 consistently ranked highest (Table 2). These two alleles are known to be in linkage disequilibrium which was also found in the green tea cases (r2 = 0.428). Because of their linkage disequilibrium, the allele frequency of HLA-B*35:01 was similar to that of HLA-C*04:01 among green tea cases (0.42 vs 0.46). However, because the HLA-B*35:01 allele was less prevalent than HLA-C*04:01 in population controls (0.06 vs 0.12), its frequency in green tea cases was proportionally higher (6.8-fold compared to 3.7-fold) and the association had higher degrees of significance. For these reasons, HLA-B*35:01 was the focus for further analyses.
Table 2.
Major HLA Allele Frequencies in Patients with Liver Injury due to Green Tea Supplements that Differed Significantly from at least one of the Control Groups
| HLA | Green Tea Supplements (n=36) | Other Dietary Supplements (n=193) | Conventional Drugs (n=1143) | Population Controls eMERGE (n=15,094) | LD with B*35:01 (r2) |
|---|---|---|---|---|---|
| B*35:01 | 0.417 | 0.076 p=5.8×10−12* |
0.062 p=6.7×10−17* |
0.057 p=9.7×10−19* |
--- |
| C*04:01 | 0.458 | 0.117 p=2.3×10−10* |
0.132 p=4.7×10−11* |
0.121 p=1.47×10−12* |
0.428 |
| A*11:01 | 0.15 | 0.086 p=0.084 |
0.052 p=0.002* |
0.053 p=0.001* |
0.05 |
| DPB1*04:02 | 0.22 | 0.143 p=0.110 |
0.127 p=0.030 |
0.096 p=0.002* |
0.0007 |
P values from Fisher exact tests compare allele frequency differences between green tea related cases and each control group. The sample sizes for each group were based on the subjects with HLA data.
indicates false discovery rate < 0.05
Linkage disequilibrium (LD) between each top allele and HLA-B*35:01 was computed by r2 based on green tea supplement group.
Among green tea cases, 26 had at least 1 copy of the HLA-B*35:01 allele yielding a carrier frequency of 72% (95% CI = 58% to 87%), a rate 5- to 7-fold higher than in control groups, including patients with non-green tea HDS related liver injury (15%: 95% CI = 10% to 20%), conventional drug related liver injury (12%: 95% CI = 10% to 14%) and the eMERGE derived population controls (11%: 95% CI = 10.5% to 11.5%). Furthermore, the carrier frequency was higher in green tea cases judged to be definite or highly likely (91%) than those considered probable (64%), or only possible or unlikely (24%) (p<.001) (Figure 2).
Figure 2.

Carrier frequency of HLA-B*35:01 among cases of green tea-associated liver injury by causality score compared to other HDS (herbal and dietary supplement) cases and to conventional drugs enrolled in DILIN, as well as in the population controls from eMERGE. The carriage rates among the green tea associated cases were higher in those with higher causality scores (“definite” and “highly likely”) compared to those considered “probable” and those judged to be only “possible” and “unlikely”.
The 26 patients with HLA-B*35:01 included 4 who were homozygous, yielding an allele frequency of 0.417 which is 7-fold higher than the frequency among the eMERGE derived population controls (0.057) and 5- to 19-fold higher than that in different U.S. racial groups (0.022 in Chinese Americans, 0.056 in European Americans, 0.067 in African Americans and 0.078 in Mexican Americans) as reported in public databases (34).
Comparison of cases of green tea-related liver injury with and without HLA-B*35:01 showed that those with the risk allele were younger (median age 40 vs 47 years), had a shorter time to onset (median 66 vs 139 days), higher initial median ALT values (2329 vs 696 U/L), and higher severity scores (Table 3). Those with HLA-B*35:01 were also more likely to have rash and fever (27% vs 0%). Other features, such as race, Hispanic ethnicity, body mass index, and symptoms were similar. Strikingly, the isolated cases with atypical features, such the one case in which the implicated product did not have detectable green tea, the two cases with a mixed rather than hepatocellular pattern of liver enzyme elevations, the two patients with atypical histology, the single patient with evidence of chronic liver injury during follow up, and 4 of the 5 patients with mild, anicteric disease were HLA-B*35:01 negative.
Table 3.
Comparison of HLA-B*35:01 Positive and Negative Green Tea-related Liver Injury
| Feature | HLA-B*35:01 Positive (n=26) | HLA-B*35:01 Negative (n=10) | P value |
|---|---|---|---|
| Age | 40 (17–69) years | 47 (24–59) years | 0.29 |
| Female Sex | 21 (81%) | 5 (50%) | 0.10 |
| Race: White | 18/25 (72%) | 7 (70%) | |
| Black | 1/25 (4%) | 2 (20%) | |
| Asian | 0/25 (0%) | 1 (10%) | |
| Other | 6/25 (24%) | 0 (0%) | |
| Hispanic ethnicity | 9 (35%) | 3 (30%) | 1.0 |
| Body Mass Index | 28.1 (21–42) k/m2 | 28.4 (20–32) k/m2 | 0.78 |
| Time to Onset | 66 (22–376) days | 139 (35–448) days | 0.08 |
| Symptoms at onset | 26 (100%) | 8 (80%) | 0.07 |
| Initial ALT | 2329 (836–4185) U/L | 696 (396–3801) U/L | <0.01 |
| Initial alkaline phosphatase | 172 (80–550) U/L | 169 (92–276) U/L | 0.47 |
| Initial total bilirubin | 8.4 (0.4–22.0) mg/dL | 6.6 (1.0–30.1) mg/dL | 0.94 |
| Peak INR | 1.2 (1.0–7.0) | 1.2 (1.0–2.1) | 0.26 |
| Initial R ratio | 26.7 (7.5–67.0) | 15.8 (3.3–47.3) | 0.06 |
| Rash or Fever | 7 (27%) | 0 (0%) | 0.16 |
| ANA or SMA | 11 (42%) | 5 (50%) | 0.72 |
| Severity score | |||
| Hepatocellular (R > 5) | 26 (100%) | 8 (80%) | 0.07 |
| Liver Transplantation | 2 (8%) | 0 (0%) | 1.0 |
| Chronicity | 0/21 (0%) | 1/7 (14%) | 0.25 |
All results are median (range) or number (proportion) with denominator given when there are missing data.
The clinical features of patients with 1 copy of HLA-B*35:01 (heterozygotes) resembled those with 2 copies (homozygotes) (Table 4). All 3 patients with two episodes of liver injury after green tea exposure were heterozygous for HLA-B*35:01. The two episodes were similar in clinical and biochemical features, but the time to onset of symptoms of the second episode (14, 16 and 21 days) was shorter than the first (1, 3 and 4 months) consistent with re-challenge (8). Concise clinical summaries with the chemical analyses and HLA results of 12 cases are provided in the supplementary material.
Table 4.
Comparison of Green Tea-Associated Liver Injury in Patients with One versus Two Copies of HLA-B*35:01
| Feature | One Copy of HLA-B*35:01 n=22 | Two Copies of HLA-B*35:01 n=4 |
|---|---|---|
| Age | 38 (17–69) | 42 (34–48) |
| Female Sex | 18 (82%) | 3 (75%) |
| Race: White | 16/21 (76%) | 2 (50%) |
| Hispanic Ethnicity | 7 (32%) | 2 (50%) |
| Body Mass Index | 28.1 (20.5–42.4) | 25.4 (20.6–40.7) |
| Time to Onset | 66 (22–335) | 69 (39–376) |
| Initial ALT | 2364 (968–4185) | 1810 (836–2701) |
| Initial alkaline phosphatase | 152 (80–550) | 255 (117–391) |
| Initial total bilirubin | 9.3 (0.4–22.0) | 6.7 (3.3–11.6) |
| Peak total bilirubin | 13.0 (0.6–38.2) | 14.8 (3.7–26.7) |
| Peak INR | 1.2 (1.0–7.0) | 1.2 (1.0–1.8) |
| Initial R ratio | 29.9 (7.5–67) | 17.6 (10.0–35.7) |
| Hepatocellular | 22 (100%) | 4 (100%) |
| Rash or Fever | 7 (32%) | 0 |
| ANA or SMA | 9 (41%) | 2 (50%) |
| Severity Score | ||
| Liver Transplant | 2 (9%) | 0 |
| Chronicity | 0/18 | 0/3 |
| Heterozygous | Homozygous |
All results are median (range) or number (proportion) with denominator given if there were missing data. None of the differences were statistically significant.
Discussion
In an ongoing study of drug-induced liver injury in the United States, green tea was judged to be the most likely cause in 40 cases, making it the major single cause of herbal supplement-related liver injury (1) and the sixth most common among all causes (28). The clinical, biochemical and histologic features of green tea liver injury were remarkably consistent and resembled those of acute viral hepatitis with hepatocellular injury, marked serum ALT and AST elevations, and variable degrees of severity and clinical outcomes. The rate of death or liver transplantation was typical for acute, icteric hepatocellular drug-induced liver injury (3 of 33 hepatocellular and jaundiced cases: 9%) as would be predicted by “Hy’s Law” (36).
Green tea was usually being taken for weight loss and most commonly as a component of a multi-ingredient product without green tea in its name. The average daily and total accumulated dose were difficult to estimate as most product labels did not provide concentrations of green tea extract or catechins, and patients were often uncertain about dates of starting and stopping and number of pills taken daily. Finally, 9 subjects were taking two green tea containing supplements concurrently. Chemical analysis indicated that catechins and ECGC were present in most products. Three patients with documented recurrence of liver injury after taking the same (1 case) or another (2 cases) green tea-containing product had similar clinical features and outcome but with a shorter latency as would be expected from an immune-mediated reaction to re-challenge.
A striking finding in the analysis was a close association of green tea related liver injury and the HLA allele B*35:01. This allele is carried by 5% to 15% of U.S. populations, rates being lowest in Asian Americans, intermediate in European and African Americans and modestly higher in Hispanics (35). In contrast, this allele was found in 72% of patients with green tea-associated liver injury and more than 90% of those in whom the injury was judged as highly likely or definite. Furthermore, cases carrying HLA-B*35:01 more closely fit the typical phenotype: a latency of 1 to 6 months, occurrence of rash or fever, a hepatocellular enzyme pattern, and a moderate to severe course with jaundice. The 2 subjects with atypical histology on liver biopsy, the 2 with “mixed” rather than hepatocellular enzyme elevations, the one with evidence of chronic liver injury in follow up, and the one taking a product without detectable catechins were all negative for HLA-B*35:01. Importantly, in this study, green tea causality was scored before the chemical analyses or the HLA typing results were known. The accumulated findings suggest that the presence of HLA-B*35:01 is a more reliable indicator of green tea liver injury than expert opinion, at least in cases not considered to be definite or highly likely.
HLA associations have been made with several forms of liver injury from conventional drugs such as flucloxacillin, amoxicillin-clavulanate, terbinafine and fenofibrate (31,37,38). Interestingly, HLA-B*35:01 has been associated with another herbal cause of liver injury, reported to be present in 89% of 27 Chinese patients with Polygonum multiflorum-induced liver injury compared to 5% of controls (39). In addition, the phenotype of the injury resembled that of green tea, with a mean age of 45 years, latency of 1 to 6 months, and hepatocellular injury. Thus, this allele may be a risk factor for liver injury from several herbal components.
Studies of rodent models of green tea extract-associated liver injury have generally focused on its direct hepatotoxicity when given in high doses (24,25) which, however, were far higher than those used in humans (17,19). Furthermore, the clinical features of green tea-associated liver injury suggest that it is idiosyncratic (18,40). In a recent clinical trial of green tea extract for prevention of breast cancer, monitoring of ALT levels revealed de novo elevations in 8.6% of treated patients compared to 1.8% of placebo-treated controls (41). The elevations were mild-to-moderate in degree, were not associated with symptoms or jaundice, arose a median of 3 months (range 1 to 12 months) after starting green tea, resolved upon stopping the supplement, and recurred rapidly after restarting, features typical of idiosyncratic and immune-mediated liver injury.
In summary, analysis of cases of drug-induced liver injury from a prospective study in the United States has identified green tea as the major cause of dietary supplement-related liver injury. The clinical phenotype was an acute-viral-hepatitis-like syndrome arising 1 to 6 months after starting green tea that was occasionally severe, but otherwise self-limiting in course. Green tea-related liver injury was strongly associated with carriage of the HLA B*35:01 allele, a risk factor that may be helpful in diagnosis and which is likely to provide new insights and directions for research into the nature of drug- and dietary supplement-induced liver injury.
Supplementary Material
Acknowledgements:
The authors would like to acknowledge the invaluable help of Hoss Rostami, BSMSE, for administration of the green tea causality assessment process and identifying product labels.
Funding:
Funded as a Cooperative Agreement by National Institute of Diabetes and Digestive and Kidney Diseases with support from the Intramural Division of the National Cancer Institute, National Institutes of Health, Bethesda, MD
Disclosures:
Drs. Ahmad, Barnhart, Gu, Hoofnagle, Khan, Koh, Li, Serrano, and Stolz have no financial disclosures to report.
Dr. Bonkovsky has no disclosures relevant to this manuscript. Within the past three years, he has served as a consultant to Alnylam Pharma, Mitsubishi-Tanabe, NA, and Recordati Rare Chemicals, NA, regarding porphyrias; and he serves as principal investigator at Wake Forest University for clinical trials in acute hepatic porphyria, erythropoietic protoporphyria, and primary sclerosing cholangitis, funded, respectively by Alnylam, Mitsubishi-Tanabe, and Gilead Sciences.
Dr. Durazo has no disclosures relevant to this manuscript. Within the past three years, he has served as a member of the Drug Monitoring Committee of Intercept Pharmaceuticals.
Dr. Fontana has no disclosures relevant to this manuscript. Within the past three years he had received research support from Gilead Sciences, Abbvie Inc., and Bristol-Myers Squibb and consulting fees from Sanofi-Aventis.
Dr. Navarro has no disclosures relevant to this manuscript. Within the past 3 years he had received research grant support from the Patient Centered Outcomes Research Institute and the Albert Einstein Society of the Albert Einstein Medical Center.
Dr. Phillips has no disclosures relevant to this manuscript. Within the past three years she has served as a consultant to Biocryst Pharma; she serves as Section Editor for Drug Allergy for UpToDate. She is co-director of IIID Pty Ltd that holds a patent for a method for identification and determination of hypersensitivity of a patient to abacavir.
Dr. Rockey has no disclosures relevant to this manuscript. Within the past 3 years he has received research grants support for his institution from Connatus Pharmaceuticals, Cumberland Pharmaceuticals, Galectin Pharmaceuticals, Genfit, Gilead Sciences, Ironwood Pharmaceuticals, Mallinckrodt Pharmaceuticals, Salix Pharmaceuticals, Sequana Medical, and has written chapters for UpToDate.
Dr. Seeff has no disclosures relevant to this manuscript. Within the past three years, he has served as a member of the Drug Monitoring Committee for Second Genome, Lipocine, Enyo Pharmaceuticals, Intercept Pharmaceuticals, and KPB Pharmaceuticals.
Dr. Tillman has no disclosures relevant to this manuscript. Within the past three years, he has served as a consultant to Trevena Inc, and his wife is an employee of Abbvie Inc and holds stock in AbbVie Inc, Abbott Laboratories, and Gilead Sciences.
Dr. Vuppalanchi has no disclosures relevant to this manuscript. Within the past three years he has received consulting fees for serving on Data Safety Monitoring Boards for Covance, Enyio and Enanta. He also received research grant support to his institution from Gilead Sciences, Zydus Discovery, Cara Therapeutics and Intercept.
Abbreviations:
- DILIN
Drug-induced Liver Injury Network
- NIH
National Institutes of Health
- NIDDK
National Institute of Diabetes and Digestive and Kidney Diseases
- HLA
human leukocyte antigen
- eMERGE
the Electronic Medical Records and Genomics Network
- ALT
alanine aminotransferase
- AST
aspartate aminotransferase
Footnotes
Clinical Trials.gov number: NCT00345930
References
- 1.Navarro VJ, Barnhart H, Bonkovsky HL, Davern T, Fontana RJ, Grant L, et al. Liver injury from herbals and dietary supplements in the U.S. Drug-Induced Liver Injury Network. Hepatology. 2014; 12(4): 1069–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Vega M, Verman M, Beswick D, Bey S, Hossack J, Merriman N, et al. ; Drug Induced Liver Injury Network (DILIN). The incidence of drug- and herbal and dietary supplement-induced liver injury: preliminary findings from gastroenterologist-based surveillance in the population of the State of Delaware. Drug Saf. 2017; 40(9): 783–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Navarro VJ, Khan I, Bjӧrnsson E, Seeff LB, Serrano J, Hoofnagle JH. Liver injury from herbal and dietary supplements. Hepatology. 2017; 65(1): 363–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Cohen PA, Sharfstein J. The opportunity of CBD – reforming the law. N Engl J Med. 2019; 381(4): 297–9. [DOI] [PubMed] [Google Scholar]
- 5.U.S. Food and Drug Administration. Dietary supplements. Available at: http://www.fda.gov/Food/DietarySupplements/default.htm. Accessed January 3, 2020. [Google Scholar]
- 6.Navarro V, Avula B, Khan I, Verma M, Seeff L, Serrano J, et al. The contents of herbal and dietary supplements implicated in liver injury in the United States are frequently mislabeled. Hepatol Commun. 2019; 3(6): 792–794. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Painter D, Perwaiz S, Murty M. Black cohosh products and liver toxicity: update. Can Adverse Reaction Newsletter. 2010; 20(1): 1–2. [Google Scholar]
- 8.Bonkovsky HL. Hepatotoxicity associated with supplements containing Chinese green tea (Camellia sinensis). Ann Intern Med. 2006; 144(1): 68–71. [DOI] [PubMed] [Google Scholar]
- 9.Jimenez-Saenz M, Martinez-Sanchez M del C. Acute hepatitis associated with the use of green tea infusions. J Hepatol. 2006; 44(3): 616–7. [DOI] [PubMed] [Google Scholar]
- 10.Björnsson E, Olsson R. Serious adverse liver reactions associated with herbal weight-loss supplements. J Hepatol. 2007(2); 47: 295–7. [DOI] [PubMed] [Google Scholar]
- 11.Sarma DN, Barrett ML, Chavez ML, Gardiner P, Ko R, Mahady GB, et al. Safety of green tea extracts: a systematic review by the US Pharmacopeia. Drug Saf. 2008; 31(6): 469–84. [DOI] [PubMed] [Google Scholar]
- 12.Dara L, Hewett J, Lim JK. Hydroxycut hepatotoxicity: a case series and review of liver toxicity from herbal weight loss supplements. World J Gastroenterol. 2008; 14(45): 6999–7004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.McDonnell WM, Bhattacharya R, Halldorson JB. Fulminant hepatic failure after use of the herbal weight-loss supplement Exilis. Ann Intern Med. 2009; 151(9): 673–4. [DOI] [PubMed] [Google Scholar]
- 14.Mazzanti G, Menniti-Ippolito F, Moro PA, Cassetti F, Raschetti R, Santuccio C, et al. Hepatotoxicity from green tea: a review of the literature and two published cases. Eur J Clin Pharmacol. 2009; 65(4): 331–41. [DOI] [PubMed] [Google Scholar]
- 15.Fong TL, Klontz KC, Canas-Coto A, Casper SJ, Durazo FA, Davern TJ 2nd, et al. Hepatotoxicity due to hydroxycut: a case series. Am J Gastroenterol. 2010; 105(7): 1561–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mazzanti G, Di Sotto A, Vitalone A. Hepatotoxicity of green tea: an update. Arch Toxicol. 2015; 89(8): 1175–91. [DOI] [PubMed] [Google Scholar]
- 17.Zheng EX, Rossi S, Fontana RJ, Vuppalanchi R, Hoofnagle JH, Khan I, et al. Risk of liver injury associated with green tea extract in SLIMQUICK® weight loss products: results from the DILIN Prospective Study. Drug Saf. 2016; 39(8): 749–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.LiverTox: Green Tea [Updated 2018 Mar 12]. https://www.ncbi.nlm.nih.gov/books/
- 19.Oketch-Rabah HA, Roe AL, Rider CV, Bonkovsky HL, Giancaspro GI, Navarro V, et al. United States Pharmacopeia (USP) comprehensive review of the hepatotoxicity of green tea extracts. Toxicology Reports. 2020: 7: 386–402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Saaed M, Naveed M, Arif M, Kakar MU, Mazoor R, Abd El-Hack ME, et al. Green tea (Camellia sinensis) and l-theanine: medicinal values and beneficial applications in humans – a comprehensive review. Biomed Pharmacother. 2017; 95: 1260–75. [DOI] [PubMed] [Google Scholar]
- 21.Kuriyama S, Shimazu T, Ohmori K, Kikuchi N, Nakaya N, Nishino Y, et al. Green tea consumption and mortality due to cardiovascular disease, cancer, and all causes in Japan. JAMA. 2006; 296(10): 1255–65. [DOI] [PubMed] [Google Scholar]
- 22.Oz HS, McClain CJ, Nagasawa HT, Ray MB, de Villiers WJS, Chen TS. Diverse antioxidants protect against acetaminophen hepatotoxicity. J Biochem Mol Toxicol. 2004; 18(6): 361–8. [DOI] [PubMed] [Google Scholar]
- 23.Henning SM, Fajardo-Lira C, Lee HW, Youssefian AA, Go VL, Heber D. Catechin content of 18 teas and a green tea extract supplement correlates with the antioxidant capacity. Nutr Cancer 2003; 45: 226–35. [DOI] [PubMed] [Google Scholar]
- 24.Lambert JD, Kennett MJ, Sang S, Reuhl KR, Ju J, Yang CS. Hepatotoxicity of high oral dose (1)-epigallocatechin-3-gallate in mice. Food Chem Toxicol. 2010; 48(1): 409–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Galati G, Lin Al, Sultan AM, O’Brien PJ. Cellular and in vivo hepatotoxicity caused by green tea phenolic acids and catechins. Free Radic Biol Med. 2006; 40(4): 570–580. [DOI] [PubMed] [Google Scholar]
- 26.Fontana RJ, Watkins PB, Bonkovsky HL, Chalasani N, Davern TJ, Serrano J, et al. Drug induced liver injury network (DILIN) prospective study: rationale, design and conduct. Drug Saf. 2009; 32(1): 55–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Rockey DC, Seeff LB, Rochon J, Freston J, Chalasani N, Bonacini M, et al. US Drug-induced Liver Injury Network. Causality assessment in drug-induced liver injury using a structured expert opinion process: comparison to the Roussel-Uclaf causality assessment method. Hepatology. 2010; 51(6): 2117–26., [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Chalasani N, Bonkovsky HL, Fontana RJ, Lee W, Stolz A, Talwalkar J, et al. Drug-induced liver injury in the United States: A report of 899 events prospectively assessed. Gastroenterology. 2015; 148(7):1340–1352 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kleiner DE, Chalasani NP, Lee WM, Fontana RJ, Bonkovsky HL, Watkins PB, et al. Hepatic histological findings in suspected drug-induced liver injury: systematic evaluation and clinical associations. Hepatology. 2014; 59(2): 661–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Dwyer JT, Bailen RA, Saldanha LG, Gahche JJ, Costello RB, Beta JM, et al. The Dietary Supplement Label Database: recent developments and applications. J Nutr. 2018; 148(Suppl 2): 1428S–1435S. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Fontana RJ, Cirulli ET, Gu J, Kleiner D, Ostrov D, Phillips E, et al. The role of HLA-A*33:01 in cholestatic hepatitis attributed to terbinafine. J Hepatol. 2018; 69(6): 1317–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. https://www.genome.gov/Funded-Programs-Projects/Electronic-Medical-Records-and-Genomics-Network-eMERGE.
- 33.Zheng X, Shen J, Cox C, Wakefield JC, Ehm MG, Nelson MR, et al. HIBAG-HLA genotype imputation with attribute bagging. Pharmacogenomics J. 2014; 14(2): 192–200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J Royal Stat Soc Ser B. 1995; 57: 289–300. [Google Scholar]
- 35.www.allelefrequencies.net (accessed December 3, 2019).
- 36.Temple R Hy’s law: predicting serious hepatotoxicity. Pharmacoepidemiol Drug Saf. 2006; 15(4): 241–3. [DOI] [PubMed] [Google Scholar]
- 37.Daly AK, Donaldson PT, Bhatnagar P, Shen Y, Pe’er I, Floratos A, et al. HLA-B*57:01 genotype is a major determinant of drug-induced liver injury due to flucloxacillin. Nat Genet. 2009; 41(7): 816–9. [DOI] [PubMed] [Google Scholar]
- 38.Nicoletti P, Aithal GP, Bjӧrnsson ES, Andrade RJ, Sawle A, Arrese M, et al. Association of liver injury from specific drugs, or groups of drugs, with polymorphisms in HLA and other genes in a genome-wide association study. Gastroenterology. 2017; 152(5): 1078–1089. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Li C, Rao T, Chen X, Wei A, Tang J, Xiong P, et al. HLA-B*35:01 allele is a potential biomarker for predicting Polygonum multiflorum-induced liver injury. Hepatology. 2019; 70(1): 346–57. [DOI] [PubMed] [Google Scholar]
- 40.Hoofnagle JH, Bjӧrnsson ES. Drug-induced liver injury: types and phenotypes. N Engl J Med 2019; 381(3): 764–73. [DOI] [PubMed] [Google Scholar]
- 41.Yu Z, Samavat H, Dostal AM, Wang R, Torkelson CJ, Yang CS, et al. Effect of green tea supplements on liver enzyme elevation: results from a randomized intervention study in the United States. Cancer Prev Res. 2017; 10(10): 571–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.