

Abstract
Background:
Tobacco smokers and companies are well aware that smoking increases the risks for cancers, vascular morbidity, and early mortality. This is a review of the plethora of adverse effects chronic smoking has on spinal tissues and spinal surgery.
Methods:
Medline (PubMed) and Google Scholar databases were searched for pertinent literature through keywords related to smoking, spondylosis, and spinal surgery.
Results:
Smoking accelerates spondylosis by impairing spinal tissue vascular supply through atherosclerosis and thrombosis, while inducing local hypoxia, inflammation, proteolysis, and cell loss. It, thus, compromises disc, cartilage, synovium, bone, and blood vessels. It can lead to early surgery, delayed wound healing, increased surgical site infection, failed fusion, more re-operations, and chronic spinal pain.
Conclusion:
There is ample evidence to support surgeons’ declining to operate on chronic smokers. The need for immediate and permanent smoking cessation and its potential benefits should be emphasized for the patient considering or who has undergone spinal surgery.
Keywords: Pseudarthrosis, Smoking, Spinal fusion, Spondylosis, Surgery, Tobacco

INTRODUCTION
Mainstream cigarette smoke drawn into a smoker’s mouth consists of 8% tar and 92% gaseous components and contains thousands of toxic chemical compounds, about 1015 free radicals per puff, and the addictive substance, nicotine.[1,7,13] Anti-smoking media campaigns usually emphasize the adverse health effects of cigarette smoking as including emphysema and chronic bronchitis, lung and other cancers, and cardiovascular diseases.[21] Here, the substantial negative impact of smoking on the spine and spinal surgery is emphasized, as cigarette smoke toxins compromise spinal blood flow and nutritional supply,[1,9] accelerate spondylosis,[12] and increase other surgical complications such as skin incision necrosis and dehiscence, delayed wound healing, and infection [Table 1].[15,20,26]
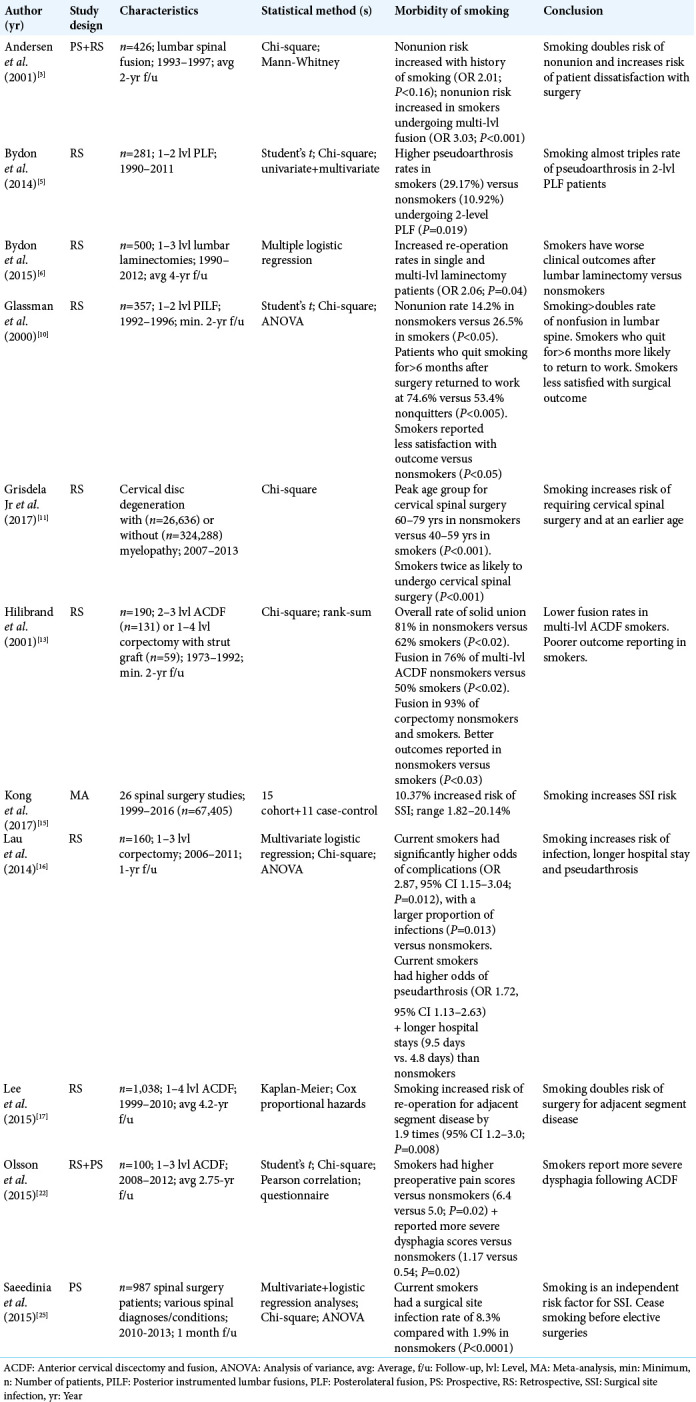
Table 1:
Adverse effects of smoking on spinal surgery.
METHODS
The literature was reviewed using keyword searches on Medline (PubMed) and Google Scholar search engines. Keywords included smoking, complications of spinal surgery, disc arthroplasty, disc degeneration, facet joint arthropathy, infection, pseudarthrosis, spinal fusion, spondylosis, vertebral bone, and wound healing.
RESULTS
Disc degeneration
The nutritional supply of intervertebral discs, which are nonvascular tissues, depends on diffusion from adjacent vertebral bodies.[8,9,27] That supply is compromised by smoking-induced vascular atherosclerosis in both local arteries and arterioles, thus promoting generalized tissue ischemia.[9] Smoking also induces a hypoxic and low pH state in intervertebral discs, leading to a reduction in normal cellular activity that impairs collagen and proteoglycan production, while enhancing enzymatic proteolysis.[8,9,12] Smoking’s disruption of cells, extracellular matrix, and the ordered histological architecture in spinal discs contributes to fissures/tears and fibrotic macroscopic hardening of the nucleus pulposus.[27] Together, these adverse factors advance the loss of disc height/hydration (desiccation) and promote the onset of earlier and more severe symptomatic lumbar spondylosis. In studies of identical twins where one smoked and the other did not, the smoker was found to have higher disc degeneration and lower bone mineral density (BMD) scores.[8-10,12,27]
Cartilage degradation and facet arthropathy
Smoking alters joint tissue gene expression toward promotion of autoimmunity and chronic inflammation.[23] In vitro studies show that cigarette smoke extract induces (in a dose- and time-dependent manner) impaired function and viability of chondrocytes found in articular cartilage.[7] The rheumatological and orthopedic literature reports increased articular cartilage loss and peripheral joint pain in smokers versus nonsmokers.[2] Further, smokers with osteoarthritis also have relatively decreased polymer molecular size and concentration of hyaluronic acid, critical for synovial joint lubrication.[7]
Bone compromise
Osteoblast function, cellularity, bone mineral content, tensile strength, and vertebral body blood supply are all compromised by smoking/tobacco use.[12] Smoking increases osteoporosis, avascular osteonecrosis, fractures, and impaired bone formation (e.g., both natural healing and fusion).[12,24] Meta-analyses have found that smokers have greater dose-dependent deficiencies in bone mass, with more adverse effects noted in men, and the elderly.[28] Further, women smoking one packet of cigarettes per day through adulthood have relatively reduced oestrogen levels and an approximate 5–10% lower BMD by the time; they become menopausal, which also typically occurs earlier.[12,28]
Vascular compromise
The gas and tar components of cigarette smoke contribute to oxidative stress attributed to reactive oxygen species that, in turn, contribute to atherosclerosis, increased inflammation, platelet aggregation, and thrombosis.[1] Circulating inflammatory pro-oxidative cytokines such as interleukin-6 and tumor necrosis factor-alpha are found to be present at higher levels in smokers versus nonsmokers.[19] In the microcirculation, this leads to increased endothelial cell damage with impaired vasorelaxation (e.g., from nitric oxide and prostacyclin signaling compromise), activation of circulating white cells, arteriolar thickening, and increased platelet adhesion.[18] Further, smoking directly or indirectly contributes to spinal tissue ischemia and degradation of bone, endplates, the synovia, and discs.[7-9,12,27]
Infection and impaired wound healing
Meta-analyses have shown that smokers have significantly increased rates of spinal surgical site complications including more skin incision necrosis, delayed wound healing, more wound dehiscence, and increased susceptibility to infection [Table 1].[15,16,20,25,26] The higher risk of infection is typically attributed to smoking impairing the normal phagocytic activity of neutrophils and macrophages against, for example, Staphylococcus aureus and Escherichia coli pathogens.[26]
Earlier operation and increased reoperation rate
Tobacco smokers are more likely to develop symptomatic cervical spondylotic myelopathy, typically warranting spinal surgery approximately two decades earlier than their nonsmoking counterparts.[11] Cessation of smoking for those undergoing cervical spine surgery is critical to avoid the two-fold greater incidence for developing “surgical” adjacent segment disease versus nonsmokers.[4,14,17] Further, smoking serves as an independent predictor for re-operation following single or multi-level lumbar laminectomies, where re-operations include surgery for other nondegenerative complications (e.g., adjacent segment disease, wound infection, dehiscence, and pseudarthrosis) [Table 1].[6,14]
Smoking increases rates of fusion failure
Smoking is known to impede all stages of bone healing and fusion.[4,12,14] Smoking initially inhibits the normal inflammatory response (first stage) and decreases fibroblast and osteoblast proliferation and function (first and second stages).[4,12] It then disrupts the normal vascular supply and neovascularization (second stage), while promoting bone’s net resorption instead of its net formation (third stage).[4,14] Notably, smokers have a twofold greater rate of pseudarthrosis following lumbar or cervical fusion surgery.[3,4,10,13,16] In addition, lower rates of fusion are encountered in smokers undergoing multilevel posterolateral fusions versus single-level arthrodesis [Table 1].[5]
CONCLUSION
Through a multitude of pathophysiological mechanisms, smoking negatively impacts the structure of the spine and the results of spinal surgery.[3,6,10,11,13,14,22] Patients anticipating undergoing spinal procedures should therefore quit smoking immediately and permanently.[3,4,10,14,25]
Footnotes
How to cite this article: Khurana VG. Adverse impact of smoking on the spine and spinal surgery. Surg Neurol Int 2021;12:118.
Declaration of patient consent
Patient consent not required as patient identity not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Ambrose JA, Barua RS. The pathophysiology of cigarette smoking and cardiovascular disease: An update. J Am Coll Cardiol. 2004;43:1731–7. doi: 10.1016/j.jacc.2003.12.047. [DOI] [PubMed] [Google Scholar]
- 2.Amin S, Niu J, Guermazi A, Grigoryan M, Hunter DJ, Clancy M, et al. Cigarette smoking and the risk for cartilage loss and knee pain in men with knee osteoarthritis. Ann Rheum Dis. 2007;66:18–22. doi: 10.1136/ard.2006.056697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Andersen T, Christensen FB, Laursen M, Høy K, Hansen ES, Bünger C. Smoking as a predictor of negative outcome in lumbar spinal fusion. Spine (Phila Pa 1976) 2001;26:2623–8. doi: 10.1097/00007632-200112010-00018. [DOI] [PubMed] [Google Scholar]
- 4.Berman D, Oren JH, Bendo J, Spivak J. The effect of smoking on spinal fusion. Int J Spine Surg. 2017;11:229–38. doi: 10.14444/4029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bydon M, de la Garza-Ramos R, Abt NB, Gokaslan ZL, Wolinsky JP, Sciubba DM, et al. Impact of smoking on complication and pseudarthrosis rates after single-and 2-level posterolateral fusion of the lumbar spine. Spine (Phila Pa 1976) 2014;39:1765–70. doi: 10.1097/BRS.0000000000000527. [DOI] [PubMed] [Google Scholar]
- 6.Bydon M, Macki M, de la Garza-Ramos R, Sciubba DM, Wolinsky JP, Gokaslan ZL, et al. Smoking as an independent predictor of reoperation after lumbar laminectomy: A study of 500 cases. J Neurosurg Spine. 2015;22:288–93. doi: 10.3171/2014.10.SPINE14186. [DOI] [PubMed] [Google Scholar]
- 7.Chen T, Ehnert S, Tendulkar G, Zhu S, Arnscheidt C, AsperaWerz RH, et al. Primary human chondrocytes affected by cigarette smoke-therapeutic challenges. Int J Mol Sci. 2020;21:1901. doi: 10.3390/ijms21051901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Chen Z, Li X, Pan F, Wu D, Li H. A retrospective study: Does cigarette smoking induce cervical disc degeneration? Int J Surg. 2018;53:269–73. doi: 10.1016/j.ijsu.2018.04.004. [DOI] [PubMed] [Google Scholar]
- 9.Fogelholm RR, Alho AV. Smoking and intervertebral disc degeneration. Med Hypotheses. 2001;56:537–9. doi: 10.1054/mehy.2000.1253. [DOI] [PubMed] [Google Scholar]
- 10.Glassman SD, Anagnost SC, Parker A, Burke D, Johnson JR, Dimar JR. The effect of cigarette smoking and smoking cessation on spinal fusion. Spine (Phila Pa 1976) 2000;25:2608–15. doi: 10.1097/00007632-200010150-00011. [DOI] [PubMed] [Google Scholar]
- 11.Grisdela P, Jr, Buser Z, D’Oro A, Paholpak P, Liu JC, Wang JC. Trends analysis of surgical procedures for cervical degenerative disc disease and myelopathy in patients with tobacco use disorder. Eur Spine J. 2017;26:2386–92. doi: 10.1007/s00586-017-5120-9. [DOI] [PubMed] [Google Scholar]
- 12.Hadley MN, Reddy SV. Smoking and the human vertebral column: A review of the impact of cigarette use on vertebral bone metabolism and spinal fusion. Neurosurgery. 1997;41:116–24. doi: 10.1097/00006123-199707000-00025. [DOI] [PubMed] [Google Scholar]
- 13.Hilibrand A, Fye MA, Emery SE, Palumbo MA, Bohlman HH. Impact of smoking on the outcome of anterior cervical arthrodesis with interbody or strut-grafting. J Bone Joint Surg Am. 2001;83:668–73. doi: 10.2106/00004623-200105000-00004. [DOI] [PubMed] [Google Scholar]
- 14.Jackson KL 2nd, Devine JG. The effects of smoking and smoking cessation on spine surgery: A systematic review of the literature. Global Spine J. 2016;6:695–701. doi: 10.1055/s-0036-1571285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kong L, Liu Z, Meng F, Shen Y. Smoking and risk of surgical site infection after spinal surgery: A systematic review and meta-analysis. Surg Infect (Larchmt) 2017;18:206–14. doi: 10.1089/sur.2016.209. [DOI] [PubMed] [Google Scholar]
- 16.Lau D, Chou D, Ziewacz JE, Mummaneni PV. The effects of smoking on perioperative outcomes and pseudarthrosis following anterior cervical corpectomy: Clinical article. J Neurosurg Spine. 2014;21:547–58. doi: 10.3171/2014.6.SPINE13762. [DOI] [PubMed] [Google Scholar]
- 17.Lee JC, Lee SH, Peters C, Riew KD. Adjacent segment pathology requiring reoperation after anterior cervical arthrodesis: The influence of smoking, sex, and number of operated levels. Spine (Phila Pa 1976) 2015;40:571–7. doi: 10.1097/BRS.0000000000000846. [DOI] [PubMed] [Google Scholar]
- 18.Lehr HA. Microcirculatory dysfunction induced by cigarette smoking. Microcirculation. 2000;7:367–84. [PubMed] [Google Scholar]
- 19.Miķelsone I, Bormane I, Simsone Z, Jurka A, Tretjakovs P. The effect of chronic cigarette smoking on microvascular function, insulin resistance and inflammatory state. Environ Exp Biol. 2011;9:23–8. [Google Scholar]
- 20.Mills E, Eyawo O, Lockhart I, Kelly S, Wu P, Ebbert JO. Smoking cessation reduces postoperative complications: A systematic review and meta-analysis. Am J Med. 2011;124:144–54. doi: 10.1016/j.amjmed.2010.09.013. [DOI] [PubMed] [Google Scholar]
- 21.Office on Smoking and Health. National Centre for Chronic Disease Prevention and Health Promotion. Centers for Disease Control and Prevention. Tips from Former Smokers. US Department of Health and Human Services. 2021. Available from: https://www.cdc.gov/tobacco/campaign/tips [Last accessed on 2021 Jan 02]
- 22.Olsson EC, Jobson M, Lim MR. Risk factors for persistent dysphagia after anterior cervical spine surgery. Orthopedics. 2015;384:319–23. doi: 10.3928/01477447-20150402-61. [DOI] [PubMed] [Google Scholar]
- 23.Ospelt C, Camici GG, Engler A, Kolling C, Vogetseder A, Gay RE, et al. Smoking induces transcription of the heat shock protein system in the joints. Ann Rheum Dis. 2014;73:1423–6. doi: 10.1136/annrheumdis-2013-204486. [DOI] [PubMed] [Google Scholar]
- 24.Patel RA, Wilson RF, Patel PA, Palmer RM. The effect of smoking on bone healing: A systematic review. Bone Joint Res. 2013;2:102–11. doi: 10.1302/2046-3758.26.2000142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Saeedinia S, Nouri M, Azarhomayoun A, Hanif H, Mortazavi A, Bahramian P, et al. The incidence and risk factors for surgical site infection after clean spinal operations: A prospective cohort study and review of the literature. Surg Neurol Int. 2015;6:154. doi: 10.4103/2152-7806.166194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Sørensen LT. Wound healing and infection in surgery: The pathophysiological impact of smoking, smoking cessation, and nicotine replacement therapy: A systematic review. Ann Surg. 2012;255:1069–79. doi: 10.1097/SLA.0b013e31824f632d. [DOI] [PubMed] [Google Scholar]
- 27.Wang ZC, Shi JG, Chen XS, Xu GH, Li LJ, Jia LS. The role of smoking status and collagen IX polymorphisms in the susceptibility to cervical spondylotic myelopathy. Genet Mol Res. 2012;11:1238–44. doi: 10.4238/2012.May.9.2. [DOI] [PubMed] [Google Scholar]
- 28.Wong PK, Christie JJ, Wark JD. The effects of smoking on bone health. Clin Sci (Lond) 2007;113:233–41. doi: 10.1042/CS20060173. [DOI] [PubMed] [Google Scholar]