

Coronavirus disease 2019 (COVID-19) has led to active infections and relatively high morbidity and mortality across the world, including the United States.1 The pandemic has challenged the US healthcare system, and rapid treatment adaptations have had to be made to stabilize public health and provide effective medical care. The Centers for Disease Control and Prevention and the Surgeon General of the United States early on in the crisis announced the cancellation of all elective surgical procedures, a policy that was subsequently revised. Along with social distancing and stay-at-home–shelter-in-place orders in many states, hospital systems and healthcare providers have rapidly redesigned testing, diagnosis, and treatment to contain the pandemic.2
COVID-19 has negatively affected the management of osteoporosis, which includes patient access to healthcare providers, laboratory testing, dual-energy X-ray absorptiometry (DEXA), and osteoporosis medications. A relatively few patients may require laboratory testing and medications, whereas in others, it may be safely postponed. The following paragraphs offer a discussion of strategies to overcome barriers to provide safe, effective, and timely care for patients with osteoporosis.
Access to a Healthcare Provider
Across many states, healthcare systems have cancelled in-clinic appointments and adapted to telehealth, a concept that requires using alternative online or telephonic platforms. Fortunately, osteoporosis is a condition that can be effectively managed via telehealth in most new and established patients because medical decision making rests on reviews of laboratory and DEXA results.
Telehealth visits include patients’ audio and video streaming consultations with physicians in clinics or home offices. Digital communication technologies are a boon when visits to clinics, hospitals, or emergency departments can be avoided to preempt any potential exposure to COVID-19. In addition, many states have imposed travel restrictions, which makes virtual telehealth visits ideal.3 Patients need to have a smart phone, tablet, or computer with camera and microphone, and the ability to use it, along with effective Internet service, to benefit from telehealth. The challenges to telehealth include situations in which patients or families do not have networked electronic devices, so that providers must cope with an audio-only telephone visit. Physicians have found it prudent to include family members during virtual visits to assist with not only technological challenges but also discussions of medical history.
A dental evaluation in selected patients is ideal before the initiation of antiresorptive medications. Many dental clinics were closed temporarily, which may have delayed treatment, but that situation is changing in every state. Weight-bearing and balance exercises, all of which are important for osteoporosis management, should be continued at home, if fitness centers remain closed.
Effective in March 2020, the Centers for Medicare & Medicaid Services (CMS) announced it would temporarily pay for telehealth services that otherwise would have been provided in a physician’s office, clinic, or hospital.4 Providers would be reimbursed for telehealth evaluation and management services as though services were taking place in person, and audio-only telephone visits would receive lower payments. CMS also allowed medication administration to be performed in a patient’s home by Medicare Part B or Part D. Regulations across US states, especially those for private insurance providers, may be different.
Access to Laboratory Testing or DEXA
A majority of the laboratories in the United States are performing phlebotomy, even though some may require patients to seek appointments to control patient crowding. Laboratories are required to strictly follow COVID-19 precautions for phlebotomy during the pandemic, to minimize exposure. Providers should determine whether the benefit of laboratory testing and medication administration is high when compared with the lower acceptable risk of potential COVID-19 exposure and proceed accordingly. If a provider determines that medication can be safely put off, then routine laboratory values and secondary evaluation may be performed later.
DEXAs are a mainstay imaging for the diagnosis of low bone density and osteoporosis. Early in the pandemic, DEXA centers were closed, operating at lower volume, or offering DEXAs on a case-by-case basis, a situation that has been in flux since then. In patients already taking anti-osteoporosis medication, DEXAs usually may be safely postponed. Patients with a new fragility fracture of the hip or spine highlight new challenges because some insurance companies require a DEXA before they reimburse certain medications. Cases should be determined individually.
Access to Anti-Osteoporosis Medication Administration
The updated 2019 Endocrine Society guidelines recommend prescribing bisphosphonates, denosumab, estrogen, raloxifene, tibolone, estrogen/bazedoxifene, or calcitonin for patients at high risk of fractures, and abaloparatide, teriparatide, or romosozumab for patients at very high risk of fractures.5 The administration of medications such as zoledronate, ibandronate, denosumab, and romosozumab must be done in a clinic or an infusion center. A few clinics continue to administer these medications and most infusion centers are functional, with COVID-19 precautions. Some clinics/infusion centers are offering “drive-through” subcutaneous denosumab injections.
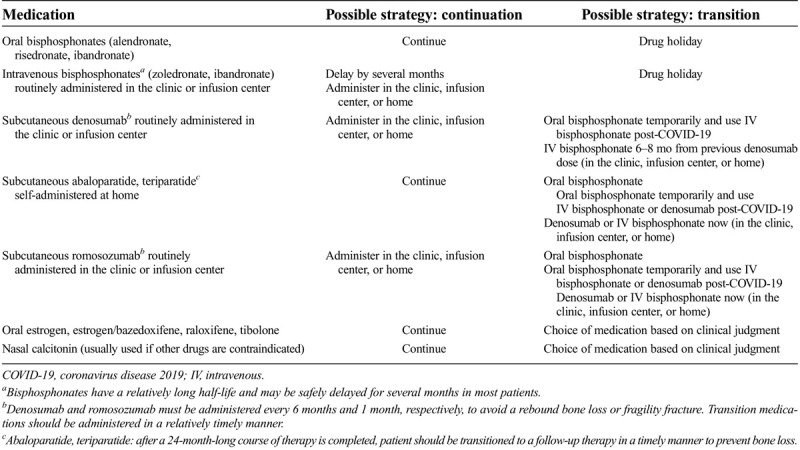
Patients may be divided into two categories; (a) not treated with medications in the recent past, and (b) currently being treated. For the former category, oral bisphosphonates (alendronate, risedronate, ibandronate) and self-injectable anabolic agents (abaloparatide, teriparatide) are reasonable options, for they are easily administered by the patients themselves. Patients with a fragility fracture may be treated with the same medications or arrangements made for the administration of zoledronate, ibandronate, denosumab, or romosozumab in a clinic, in an infusion center, or at home. For the latter category, the physician must decide whether to initiate a drug holiday or transition to a different medication. The Table summarizes the choices of medication and possible treatment strategies for patients already receiving treatment.
Table.
Choices of medication and possible treatment strategies for patients already receiving treatment
This review of osteoporosis management intends to offer a brief response to an ongoing medical challenge triggered by the COVID-19 pandemic, which continues to escalate. Clinicians managing patients with osteoporosis should continue to exercise clinical judgment and decide diagnosis or disease management by the individual patient. They should continually review rapidly changing CMS and multiple insurance provider policies to care for patients during the pandemic. They should check National Osteoporosis Foundation resources for updated information, including webinars about osteoporosis management and policies.6 Benefits, harms, cost, and patient preferences should be considered during the shared decision-making process to treat osteoporosis and prevent fragility fractures and also keep patients and their communities safe from COVID-19.
Footnotes
V.S. has received patient education research grant from Radius Health Inc. (unrelated to this manuscript).
References
- 1.Omer SB, Malani P, Del Rio C. The COVID-19 pandemic in the US: a clinical update. JAMA 2020;323:1767–1768. [DOI] [PubMed] [Google Scholar]
- 2.Keesara S, Jonas A, Schulman K. COVID-19 and health care’s digital revolution. N Engl J Med 2020;382:e82. [DOI] [PubMed] [Google Scholar]
- 3.Centers for Disease Control and Prevention . Public health professionals gateway. State and territorial health department websites. https://www.cdc.gov/publichealthgateway/healthdirectories/healthdepartments.html. Accessed April 27, 2020.
- 4.Centers for Medicare & Medicaid Services . Medicare telemedicine health care provider fact sheet. https://www.cms.gov/newsroom/fact-sheets/medicare-telemedicine-health-care-provider-fact-sheet. Published March 17, 2020. Accessed April 27, 2020.
- 5.Eastell R Rosen CJ Black DM, et al. Pharmacological management of osteoporosis in postmenopausal women: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2019;104:1595–1622. [DOI] [PubMed] [Google Scholar]
- 6.National Osteoporosis Foundation . Ask the Expert: Dr. Lewiecki Shares Invaluable Insight on Best Telemedicine Practices During the Pandemic. https://www.nof.org/covid-19-updates. Accessed April 27, 2020.