

Abstract
Purpose/objectives
Treatment planning systems (TPS) for Gamma Knife stereotactic radiosurgery (GK-SRS) include TMR10 algorithms, which assumes tissue homogeneity equivalent to water, and collapsed-cone convolutional (CCC) algorithms, which accounts for tissue inhomogeneity. This study investigated dosimetric differences between TMR10 and CCC TPS for acoustic neuromas (ANs) treated with GK-SRS.
Materials/methods
A retrospective review of 56 AN treated with GK-SRS was performed. All patients underwent MRI and CT imaging during their initial treatment and were planned using TMR10. Each plan was recalculated with CCC using electron density extracted from CT. Parameters of interest included Dmax, Dmin, D50%, cochlea Dmax, mean cochlea dose, target size, and laterality (>20 mm from central axis).
Results
Median target volume of patients was 1.5 cc (0.3 cc-2.8 cc) with median dose of 12 Gy prescribed to the 50% isodose line. Compared to CCC algorithms, the TMR10 calculated dose was higher: Dmax was higher by an average 6.2% (p < 0.001), Dmin was higher by an average 3.1% (p < 0.032), D50% was higher by an average of 11.3%. For lateralized targets, calculated Dmax and D50% were higher by 7.1% (p < 0.001) and 10.6% (p < 0.001), respectively. For targets <1 cc, Dmax and D50% were higher by 8.9% (p ≤ 0.009) and 12.1% (p ≤ 0.001), respectively. Cochlea Dmax was higher, by an average of 20.1% (p < 0.001).
Conclusion
There was a statistically significant dosimetric differences observed between TMR10 and CCC algorithms for AN GK-SRS, particularly in small and lateralized ANs. It may be important to note these differences when relating GK-SRS with standard heterogeneity-corrected SRS regimens.
Keywords: Gamma Knife, acoustic neuroma, radiosurgery, treatment planning
INTRODUCTION
The Leksell Gamma Knife (GK) Co-60 unit has historically used the TMR10 dose calculation algorithm, which assumes a global tissue density equivalent to water, in contrast to the vast majority of conventional treatment planning systems (TPS), which use CT datasets to assign electron density to tissues, allowing unique patient-specific heterogeneity corrections.
Prior studies have demonstrated that targets near the bone-tissue interface may receive a lower dose than predicted by a TPS using TMR10 1-3. The region of the internal auditory canal (IAC) represents the most heterogeneous region of the skull, with adjacent mastoid air cells and thick petrous temporal bone. Therefore, a target based in the IAC, such as an acoustic neuroma (AN) may represent a distinct clinical scenario where heterogeneity corrections would be particularly important. The aim of this study was to investigate the dosimetric differences between TMR10 and CCC – the heterogeneity-corrected dose calculation algorithm used in the GK TPS.
METHODS
Dataset
A prospectively maintained institutional review board (IRB)-approved Gamma Knife database was used to identify 56 patients diagnosed with acoustic neuroma treated between 2015 and 2018.
Current institutional procedure – TMR10
All patients underwent T1-weighted gadolinium contrast-enhanced MRI imaging with stereotactic headframe followed by CT imaging. Patients with intact hearing were prescribed 12 Gy prescribed to 50% isodose line (IDL). Patients without hearing were prescribed 13 Gy prescribed to 50% IDL.
All treatment planning was based on the TMR10 dose calculation algorithm.
Experimental procedure – heterogeneity-corrected calculations
Scanner-specific look-up tables for electron density mappings were created using a Gammex (Gammex-Sun Nuclear, Middleton, WI) RMI 465 electron density CT phantom, which is a solid water phantom with material plugs with electron density from 0.29 to 6.58 and physical density from 0.30 to 8.00 g/cm3. Mappings were benchmarked against results available from the annual QA and commissioning values. For this investigation, each patient’s clinically-approved plan (based on TMR10) was retrospectively copied and the dose distributions were re-calculated using CCC. Resultant DICOM-RT dose distribution files were exported to our analysis database.
Statistical Analysis
DICOM-RT files were analyzed using Python v3.7 with the pydicom software library 4. Dosimetric parameters of interest included: target maximum dose (Dmax), target minimum dose (Dmin), highest dose to 50% volume (D50%) of target, and cochlea Dmax. Differences in dosimetric outcomes between TMR10 and CCC plans were analyzed using paired t-tests. To better understand the effect of GTV size and GTV location on TMR-CCC dosimetric differences, sub-analysis based on target laterality (>20 mm from central axis) and target volume (<1 cc) was also evaluated.
Voxel Level Analysis
Voxel level differences in the 50% IDL between TMR10 and CCC plans were paired with measurements from the central axis at the brainstem. Kernel density estimation5 was used to generate predicted differences in the 50% IDL for each voxel based on distance from central axis at the brainstem. Voxel level predicted differences in the 50% IDL were super-imposed on a representative MRI image to qualitatively identify potential anatomic locations associated with greatest dosimetric differences.
RESULTS
Patient characteristics for the 56 patients treated for acoustic neuroma within our institution from 2015-2018 are summarized in Table 1. The median dose prescribed to the target was 12 Gy (12-13 Gy) prescribed to the 50% isodose line. The mean target volume (defined by 50% IDL) was 1.5 cm3 (0.3-2.8 cm3) and was broadly divided into two groups for statistical analyses: large (>1 cm3, n = 24) and small (≤1 cm3, n = 32). Similarly, after determining the edge of the acoustic neuroma closest to midline, targets were broadly defined as either centralized (edge ≤20 mm from midline, n = 18) or lateralized (edge >20 mm from midline, n = 38).
Table 1.
Patient cohort characteristics
| Total Patients | 56 |
|---|---|
| Sex | 35 Male (62.5%) 21 Female (39.2%) |
| Age Median (Range) |
62.5 (21-89) |
| Median Target Volume (cm3) |
0.766 (0.069-10.5) |
| Tumor laterality † (mm) |
31.2 (11.1-48.2) |
| Median Prescription Dose (cGy) |
12 (12-13) |
| Prescribed isodose | 50% |
† Tumor laterality was defined by measuring the distance from midline to the closest edge of the acoustic neuroma
Patient-specific dose distributions were compared between TMR10 and CCC dose calculation algorithms within the database (Table 2). Compared with the CCC calculation, the calculated target Dmax was higher using the TMR10 dose calculation by an average of 6.2% (3.4-10.1%, p < 0.001). Similarly, the calculated target Dmin was higher using the TMR10 dose calculation by an average of 3.1% (1.1-7.3%, p < 0.032). The calculated D50% was higher in the TMR10 calculation, by an average of 11.3% (4.7-16.1%, p < 0.001). The differences are shown individually for each patient in Figure 1. With respect to organs at risk, the TMR10 calculation of cochlea Dmax was higher than that calculated by the CCC algorithm, by an average of 20.1% (12.9-38.3%, p < 0.001).
Table 2.
Calculated TMR10 dose with respect to CCC dose calculation algorithm
| % Dose of CCC calculation(range) | p-value | |
|---|---|---|
| Target Dmax Small (<1 mm) Lateralized (>20 mm) |
+3.1% (1.1-7.3) +8.9% (6.2-10.4) +7.1% (5.1-8.7) |
<0.001 <0.009 <0.001 |
| Target D50% Small (<1 mm) Lateralized (>20 mm) |
+11.3% (4.7- 16.1) +12.1% (9.6-12.9) +10.6% (8.3-11.2) |
<0.001 <0.001 <0.001 |
| Cochlea | +20.1% (12.9-38.3) | <0.001 |
TMR = tissue maximum ratio; CCC = collapsed-cone convolution; Dmax = maximum dose; Target D50% = percentage of target receiving 50% prescribed dose
Figure 1.

Cohort differences between TMR10 and CCC dose calculations for various parameters. a) % difference in GTV Dmax, b) % difference in GTV Dmin, c) % difference in GTV D50%, d) % difference in cochlea Dmax. (TMR= tissue maximum ratio; CCC= collapsed-cone convolution; GTV= gross tumor volume; Dmax = maximum dose; Dmin = minimum dose, D50% = dose covering 50% of target volume)
The differences between TMR10 and CCC calculations for Dmax and D50% were most pronounced in lateralized and/or small targets. Isodose lines comparing small versus large targets are shown in Figure 2. For lateralized targets, the calculated Dmax and D50% was higher with TMR10, by an average of 7.1% (p < 0.001) and 10.6% (p < 0.001). Similarly, for small targets, Dmax and D50% were higher with TMR10 plan, by an average of 8.9% (p ≤ 0.009) and 12.1% (p ≤ 0.001).
Figure 2.

Prescription isodose line coverage (50% isodose line) for TMR10 vs CCC dose calculation algorithms. Red = TMR10, Blue = CCC : a) and c) represent small (<1 cc) target lesions and b) B represents a large (>1 cc) target. TMR= tissue maximum ratio; CCC= collapsed-cone convolution)
After performing voxel level analysis, a heat map as shown in Figure 3, was generated to visually identify the regions most impacted by heterogeneity. The gradient in the heat map suggested that centralized targets had similar results, with 0-4% difference between TMR10 and CCC algorithm. Moving laterally, this difference increased to more than 10%.
Figure 3.
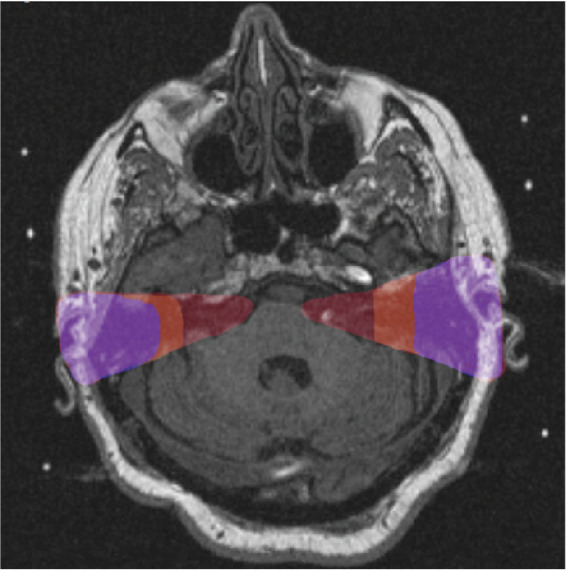
Voxel Level Predicted differences in 50% isodose line based on distance from central axis. Red (0-4%), Orange (4-10%), Purple (>10%).
DISCUSSION
This work is the largest series to date investigating differences observed in the calculated dose delivered to ANs and the cochlea comparing CCC TPS to the current GK TPS dose calculation algorithm, TMR10. Further, this work is the first to perform voxel level analysis between patients to produce a qualitative visual heat-map which shows not only the region but also the approximate magnitude of discrepancies observed in our cohort. This visualization technique – especially of the gradient – may lead to additional insight regarding unexpected clinical outcomes which were based on historical dose calculations such as TMR10, and where the dosimetry would be expected to deviate significantly when applying historical GK-SRS dosing regimens to LINAC-based SRS.
The differences observed between TMR10 and CCC agree with prior studies 1,3,6-10 which observed 4%-9% differences between the two dose calculation algorithms. The cases most affected by different dose calculations were well-lateralized targets in close proximity to the skull and mastoid air cells. Our results also corroborate previous studies which observed the greatest difference for lesions within 1 cm of the skull 6, and for lesions near the sphenoid wing and sagittal sinus 3. Similarly, Boari et al. noted that cochlear dosimetry was significantly different with CCC compared to TMR10.9
While the improved dosimetric accuracy of CCC in extracranial/LINAC-based radiation has been widely accepted11,12 and adopted in practice since 2010, the majority of GK users continue to exclusively use the TMR10 dose calculation algorithm, which does not account for intracranial features and uniformly assigns water-equivalence to the entire calculation volume. Depending on the clinical equipment available in a clinic, any given patient could have dose distributions calculated with (LINAC, CCC) or without (GK, TMR10) heterogeneity correction for the same clinical presentation. Because TMR10 overestimates dose delivered to the target in this scenario, when the same prescription dose is applied to CCC, it is unlikely the tumor control will be compromised. In fact, based on our findings, the tumor will likely be treated with a higher dose, as the TPS can optimize by accounting for heterogeneity. However, this may pose a safety risk as the dose constraint of the cochlea used for SRS are based on historical GK (TMR10) treatment, when in reality the cochlea has not actually been exposed to the constraint dose, since the dose reaching that structure is actually less than projected by the TMR algorithm. If the same constraint is applied to CCC algorithm treatment, there may be higher risks of toxicity.
Our findings may have clinical implications for patients who will receive SRS to lateralized intracranial lesions for two reasons. First, dose distributions presented to the physician could be significantly different based solely on the type of calculation algorithm (currently associated with treatment machine, GK versus LINAC TPS) being employed by the specific clinic. The heat map created by our voxel level analysis may help identify a subset of AN cases which are potentially impacted the most by algorithm choice, and therefore radiation modality technology. Secondly, the clinical outcomes for GK-based SRS may need to be reexamined given much of the prior literature is based on data using the historical TMR10 13-16. We have demonstrated more than 10% differences in dose in certain intracranial regions after incorporating heterogeneity corrections. Based on these findings, the current 12-13 Gy AN prescription dose is apparently and overestimation of dose actually reaching the target. Applying this dose, which has been historically quite safe with TMR10 TPS, to a machine equipped with CCC will result in a relative increase in dose delivered, as the TPS can optimize for full prescription dose delivery accounting for heterogeneity corrections. Likewise, relying on TMR10 may result in a higher dose delivered to nearby structures, which could impact the risk of hearing loss, tinnitus, or facial nerve injury, though this has not been analyzed in a prospective fashion. This is a phenomenon that should be acknowledged by clinicians and physicists and our results suggest when evaluating SRS dose in the treatment of intracranial lesions, and particularly ANs, an important parameter could be the dose calculation algorithm used.
CONCLUSION
This study has demonstrated a statistically significant difference in dose distributions in both the target and ipsilateral cochlea for ANs after incorporating heterogeneity corrections. Plans based on the currently employed TMR10 overestimated the dose delivered by >10% in some regions, with respect to the CCC dose calculation algorithm. The largest discrepancies were observed in small and/or lateralized ANs. The significance of this finding is its relevance to the scenario of applying historical GK-SRS (TMR10) dosing to LINAC-based SRS (CCC), or GK newly equipped with CCC, for any intracranial lesion but particularly those in the regions highlighted in the provided heatmap (Figure 3). CCC dose calculation algorithms have been nearly universally adopted for extracranial radiosurgery and shown to be more dosimetrically accurate,6 along with the practice of modifying dose prescription based on the use of heterogeneity corrections. Physicians and physicists should be aware of the inherent difference in the TPS and how this translates to target and OAR dosimetry. Further investigation of whether prescription dosing should be adapted to account for the TPS is warranted. To that end, our results suggest when evaluating SRS dose in the treatment of AN, an important parameter to specify could be the dose calculation algorithm used.
ACKNOWLEDGMENTS
James Bond, PhD assisted in logistical aspects of this project.
Funding:
Agency for Healthcare Research and Quality (AHRQ K12 HS023000- 05): Aneja
American Cancer Society (ACS-IRG 17-172-57): Aneja
Authors’ disclosure of potential conflicts of interest
Dr Aneja receives research support from the National Science Foundation, American Society for Clinical Oncology, National Cancer Institute, and Agency for Healthcare Research and Quality. Dr. Yu reports personal fees for consulting from Augment/Boston Scientific and is on the advisory board of Galera Pharmaceuticals, all of which are outside the submitted work. Dr. Chiang reports personal fees for consulting and speaking for Monteris Medical Inc, MRI Interventions, and Brainlab, all of which are outside the submitted work. Dr. Hansen reports stock options from Patrys Limited and has various patents outside of the submitted work. The remaining authors have nothing to disclose.
Author contributions
Conception and design: Sanjay Aneja, Gabrielle W Peters
Data collection: Gabrielle W Peters, Christopher J Tien, Sanjay Aneja
Data analysis and interpretation: Christopher J Tien, Sanjay Aneja
Manuscript writing: Gabrielle W Peters, Christopher J Tien, Sanjay Aneja
Final approval of manuscript: Gabrielle W Peters, Christopher J Tien; Veronica Chiang, James Yu, James Hansen, Sanjay Aneja
REFERENCES
- 1.Rojas-Villabona A, Kitchen N, Paddick I. Investigation of dosimetric differences between the TMR 10 and convolution algorithm for Gamma Knife stereotactic radiosurgery.. J Appl Clin Med Phys 2016;17(6):217-229. DOI: 10.1120/jacmp.v17i6.6347 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Shields LBE, Bond C, Odom A, Sun DA, Spalding AC. Heterogeneity correction for intensity-modulated frameless SRS in pituitary and cavernous sinus tumors: a retrospective study. Radiat Oncol 2015;10(1):193. DOI: 10.1186/s13014-015-0500-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Xu AY, Bhatnagar J, Bednarz G, Niranjan A, Flickinger J, Lunsford LD, Huq MS. Dose differences between the three dose calculation algorithms in Leksell GammaPlan. J Appl Clin Med Phys 2014;15(5):4844. DOI: 10.1120/jacmp.v15i5.4844 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.D.L. M. Pydicom: An Open Source DICOM Library. https://github.com/pydicom/pydicom. Accessed 2/21/2020.
- 5.Terrell GR, Scott DW. Variable Kernel Density Estimation. Ann Statist. 1992;20(3):1236-1265. [Google Scholar]
- 6.Fallows P, Wright G, Harrold N, Bownes P. A comparison of the convolution and TMR10 treatment planning algorithms for Gamma Knife® radiosurgery.. J Radiosurg SBRT. 2018;5(2):157-167. [PMC free article] [PubMed] [Google Scholar]
- 7.Xu AY, Bhatnagar J, Bednarz G, Niranjan A, Kondziolka D, Flickinger J, Lunsford LD, Huq MS. Gamma Knife radiosurgery with CT image-based dose calculation. J Appl Clin Med Phys 2015;16(6):119-129. DOI: 10.1120/jacmp.v16i6.5530 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Nakazawa H, Komori M, Shibamoto Y, Tsugawa T, Mori Y, Kobayashi T. Dosimetric comparison of absolute and relative dose distributions between tissue maximum ratio and convolution algorithms for acoustic neurinoma plans in Gamma Knife radiosurgery. Acta Neurochir. 2014;156(8):1483-1489. [DOI] [PubMed] [Google Scholar]
- 9.Boari N, Bailo M, Gagliardi F, Franzin A, Gemma M, del Vecchio A, Bolognesi A, Picozzi P, Mortini P. Gamma Knife radiosurgery for vestibular schwannoma: clinical results at long-term follow-up in a series of 379 patients.. J Neurosurg. 2014;121 Suppl: 123-142. DOI: 10.3171/2014.8.GKS141506 [DOI] [PubMed] [Google Scholar]
- 10.Moskvin V, Timmerman R, DesRosiers C, Randall M, DesRosiers P, Dittmer P, Papiez L. Monte carlo simulation of the Leksell Gamma Knife: II. Effects of heterogeneous versus homogeneous media for stereotactic radiosurgery. Phys Med Biol 2004;49(21):4879-4895. DOI: 10.1088/0031-9155/49/21/003 [DOI] [PubMed] [Google Scholar]
- 11.Xiao Y, Papiez L, Paulus R, Timmerman R, Straube WL, Bosch WR, Michalski J, Galvin JM. Dosimetric evaluation of heterogeneity corrections for RTOG 0236: stereotactic body radiotherapy of inoperable stage I-II non-small-cell lung cancer.. Int J Radiat Oncol Biol Phys 2009;73(4):1235-1242. DOI: 10.1016/j.ijrobp.2008.11.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Solberg TD, Holly FE, De Salles AAF, Wallace RE, Smathers JB. Implications of tissue heterogeneity for radiosurgery in head and neck tumors. Int J Radiat Oncol Biol Phys 1995;32(1):235-239. DOI: 10.1016/0360-3016(94)00495-7 [DOI] [PubMed] [Google Scholar]
- 13.Flickinger JC, Kondziolka D, Maitz AH, Lunsford LD. Gamma knife radiosurgery of imaging-diagnosed intracranial meningioma. Int J Radiat Oncol Biol Phys. 2003;56(3):801-806. DOI: 10.1016/s0360-3016(03)00126-3 [DOI] [PubMed] [Google Scholar]
- 14.Kondziolka D, Lunsford LD, McLaughlin MR, Flickinger JC. Long-term outcomes after radiosurgery for acoustic neuromas. New Eng J Med 1998;339(20):1426-1433. DOI: 10.1056/NEJM199811123392003 [DOI] [PubMed] [Google Scholar]
- 15.Pollock BE, Driscoll CL, Foote RL, Link MJ, Gorman DA, Bauch CD, Mandrekar JN, Krecke KN, Johnson CH. Patient outcomes after vestibular schwannoma management: a prospective comparison of microsurgical resection and stereotactic radiosurgery. Neurosurg. 2006;59(1):77-85. DOI: 10.1227/01.NEU.0000219217.14930.14 [DOI] [PubMed] [Google Scholar]