

Abstract
Mobility-impaired persons, either very old or younger but suffering with systemic neuromuscular disorders or chronic organ failures, spend small amounts of time for daily physical activity, contributing to aggravate their poor mobility by resting muscle atrophy. Sooner or later the limitations to their mobility enforce them to bed and to more frequent hospitalizations. We include among these patients at risk those who are negative for the SARS-COV-2 infection, but suffering with COVID-19 pandemic syndrome. Beside managements of psychological symptoms, it is mandatory to offer to the last group physical rehabilitation approaches easy to learn and self-managed at home. Inspired by the proven capability to recover skeletal muscle contractility and strength by home-based volitional exercises and functional electrical stimulation, we suggest also for chronic COVID-19 pandemic syndrome a 10–20 min long daily routine of easy and safe physical exercises that can activate, and recover from weakness, the main 400 skeletal muscles used for every-day mobility activities. Persons can do many of them in bed (Full-Body in-Bed Gym), and hospitalized patients can learn this light training before leaving the hospital. It is, indeed, an extension of well-established cardiovascular-respiratory rehabilitation training performed after heavy surgical interventions. Blood pressure readings, monitored before and after daily routine, demonstrate a transient decrease in peripheral resistance due to increased blood flow of many muscles. Continued regularly, Full-Body in-Bed Gym may help maintaining independence of frail people, including those suffering with the COVID-19 pandemic syndrome.
Key Words: skeletal muscle weakness, home-based Full-Body in-Bed Gym, older olds, borderline mobility impaired persons, COVID-19 pandemic syndrome
Ethical Publication Statement
Authors confirm that they have read the Journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
There are about 700 named skeletal muscles in the human body, including 400 that are important only for medical specialists. Better known are the roughly 200 skeletal muscles that are serious bone-movers, plus another 100 little muscles of hands, feet, and face. The aim of this report is to convince persons-in-need, and their practitioners, to counteract muscle atrophy-sarcopenia-cachexia, maintaining at their best function and shape of the majority of their body muscles.1 Geriatric subjects, due to advanced age and/or associated diseases, spend only a short amount of time for daily physical activity. The consequent disuse muscle atrophy contributes to limit their independence ultimately enforcing them to bed and to hospitalization for long periods. Low mobility-related muscle atrophy is associated with neuromuscular weakness, functional limitations, thromboembolism, and high costs.2-4 All progressive muscle contractile impairments need permanent management. Besides eventual pharmacological treatment, a home-based physical exercise approach is helpful in counteracting muscle atrophy. Awaiting development of implantable devices for muscle stimulation, as effective as pacemakers for cardiac arrhythmias,5 implantable stimulators for ventilatory supports,6,7 or cochlear implants for hearing loss,8,9 education of sedentary patients to perform home physical exercises could be an effective low-cost alternative during and after hospitalization.10-12
Fig 1.
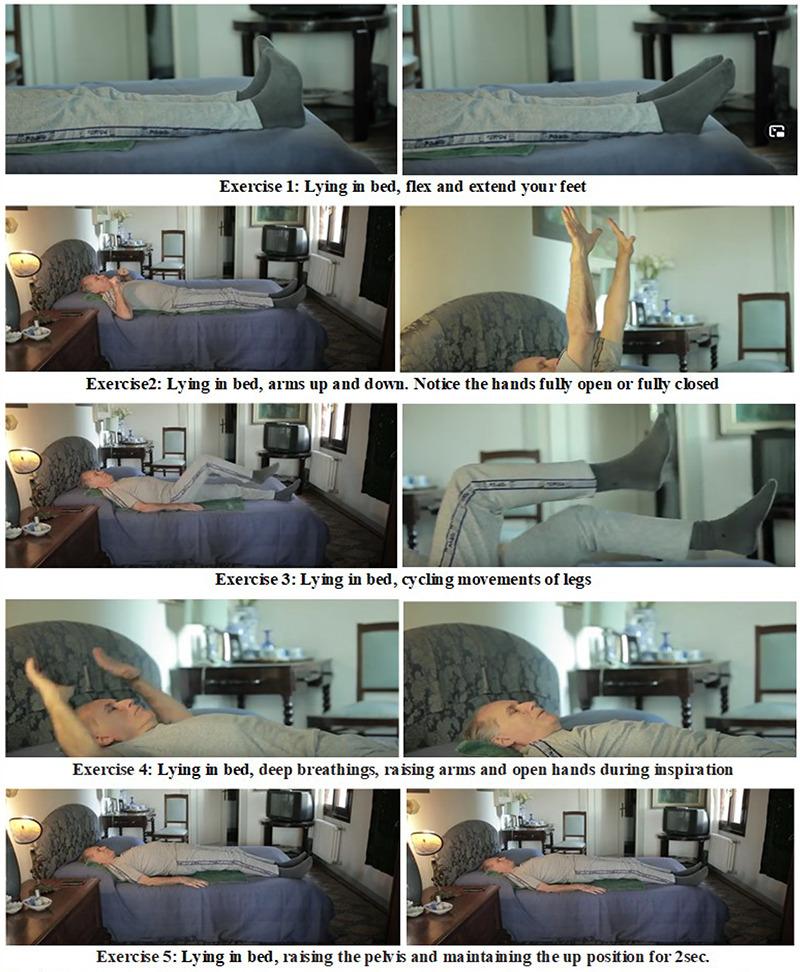
The purpose of the routine is to contract all major skeletal muscles, alternating exercises to mobilize arms and legs, spine and neck, diaphragm and accessory ventilation muscles Duration of the routine (i.e., the number of repetitions and subsequently their speed of execution) must always reach the fatigue threshold.
Fig 2.
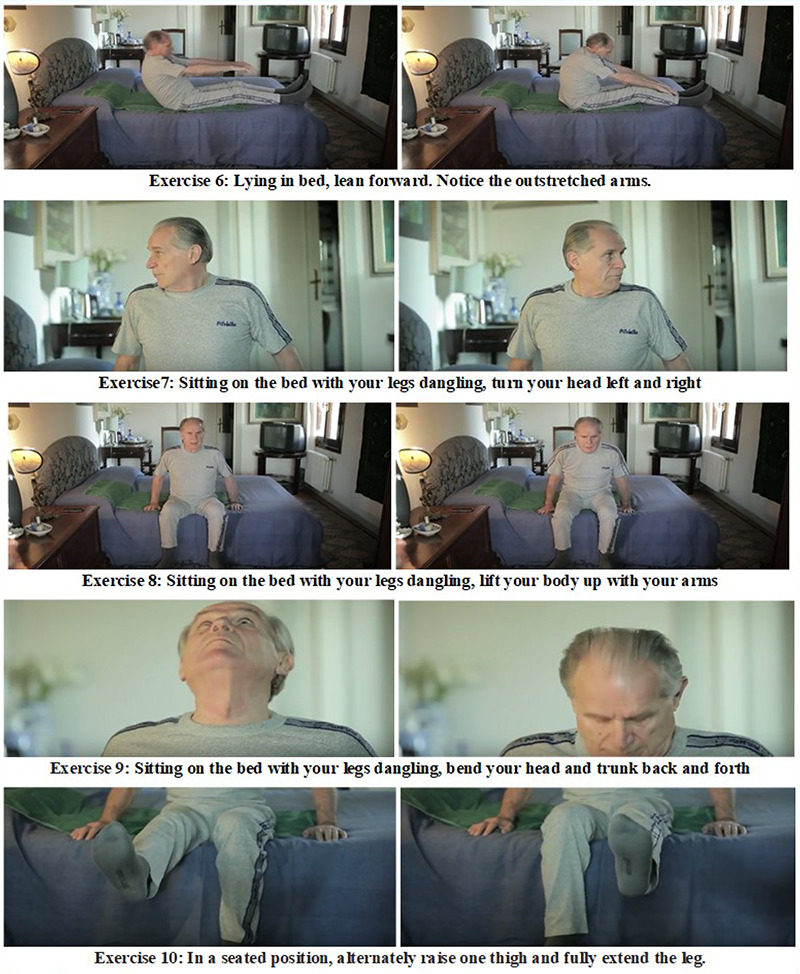
The aim of the routine is to contract all main skeletal muscles, alternating exercises to mobilize arms and legs, spinal cord and neck, diaphragm and ventilation accessory muscles. Intensity of the routine (as number of repetitions and then speed) must be up to fatigue threshold.
Fig 3.
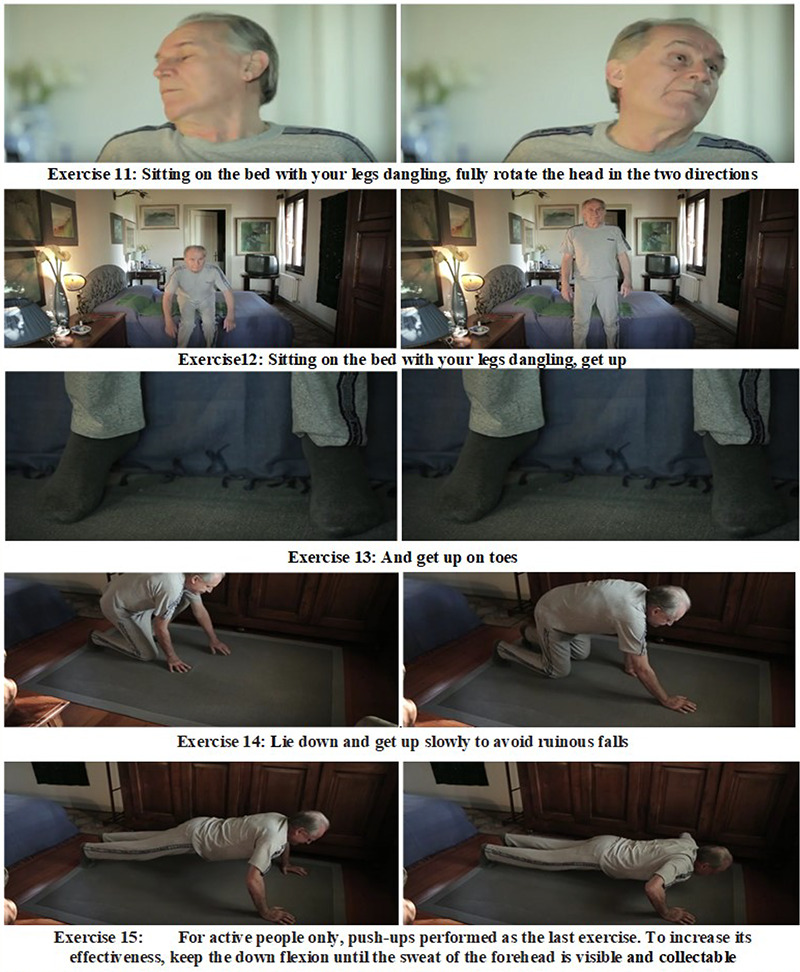
The aim of the routine is to contract all main skeletal muscles, alternating exercises to mobilize arms and legs, spinal cord and neck, diaphragm and ventilation accessory muscles. Intensity of the routine (as number of repetitions and then speed) must be up to fatigue threshold.
Cardiovascular and respiratory physical rehabilitation protocols of surgical patients are well established approaches, whose main goal is to reverse muscle weakness/atrophy.13,14 We extended those routines to a daily short (10–20 min) sequence of easy-to-learn and safe volitional physical exercises to be performed in bed (Full-Body in-Bed Gym) to improve muscles and, hence, mobility of impaired persons.
Chronic COVID-19 pandemic syndrome is characterized by the psychological response to the global problem of COVID-19 pandemic, and often by muscle weakness that negatively influences the quality of life of persons for weeks or months before or after resolution of the infection.15-17 This syndrome is believed to affect up to 10% of the population, because it could already be observed as an acute stress reaction to the spread of the SARS-CoV-2 infection. Certainly it changes in people the ordinary lifestyle for the forced lockdown measures imposed to control the epidemics.18,19 However, the most severe responses are expected later on after recovering COVID-19. In this case the pandemic syndrome is similar to post-traumatic stress disorders. The problem is that pandemic syndrome will affect the working capacity of population even when economic recovery will be possible and essential. Adequate prophylaxis and management of the syndrome in high-risk groups are important for maintaining global mental health and economy. Beside pharmacological support and psychotherapy in the acute phases, it will be mandatory to prevent and control the mild cases by general prophylactic measures and healthy lifestyle, i.e., by normalization of sleep-wake schedule, by controlling dietary intake of vitamins and microelements and by inducing moderate physical activity. All these measures are important to maintain a good physical condition that improves body adaptive potentials and the immune system.
Here our contribution is to convince practitioners,20-23 and the population at large that Full-Body in-Bed Gym is an option to be taken seriously, despite its apparent minimal requested effort.10-12
Fig 4.
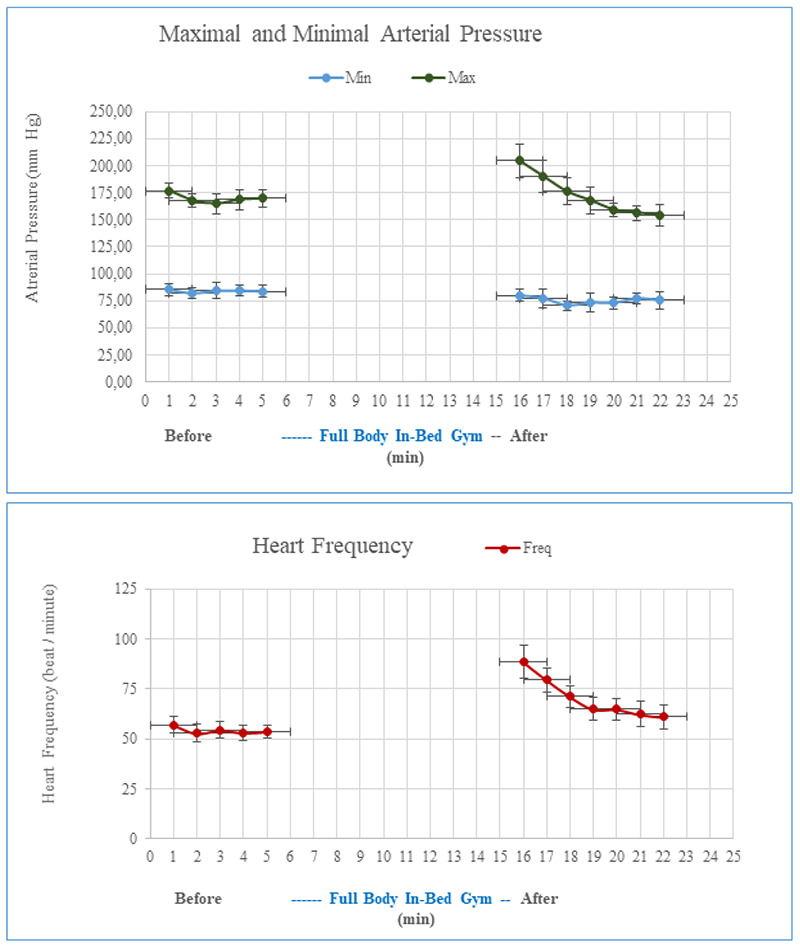
Arterial pressure and cardiac frequency before and after 10 minutes of Full Body in-Bed Gym (25 repetitions of each exercise, including push-up) during seven consecutive days (November 8 to 14, 2016). Mean +/- SD. After a self-challenging routine, cardiac and ventilatory frequency increased together with the maximal, but not the minimal arterial pressure. Indeed, the latter is more related to peripheral blood resistance. The exercise-induced increase of blood perfusion of all the main skeletal muscle of the body occurs if the series of exercise reach the level of fatigue threshold.
Suggested workout
In Figures 1, 2 and 3, the Exercises 1 to 14 show the routine that could be a seasonal warm up also for active persons (typically at early spring after a long winter to recover fitness for demanding physical activities), i. e, those able to make at least 20 consecutive push-ups in 3 min (Figure 3, Exercise 15). After advice of his/her family physician to avoid the very low risks of exercise pain and eventual muscle and joint damage, any sedentary people may start with five repetitions of each exercise. After one-two weeks of training, they may add groups of five additional repetitions, up to 30, every additional week. If compliant, even older olds will progressively increase their muscle strength, if they reach and maintain 15 or 20 daily repetitions. It is safer to start performing the exercises at very slow speed, but when the maximum number of each exercise is reached (15 or 20 repetitions), improving effects will be obtained by speeding up each exercise and thus increasing intensity.
The daily routine may last from 10 min (in the beginning) to 30 min (for complete session in accustomed persons). Figures 1, 2 and 3, show the exercises and the captions provide some details.
A video,24 describes them dynamically: https://www.youtube.com/watch?v=N1RuG3371-Y&feature=youtu.be
If sedentary persons without major comorbidities, but with rest-related muscle weakness, avoiding much stress, challenge themselves in a few weeks of Full-Body in-Bed Gym may increase their muscle strength, fatigue resistance and independence in daily life activities.
Cautious Full-Body in-Bed Gym may help patients to recover earlier after hospitalization, decreasing the risk of thromboembolism after surgical interventions, and concurring to reduce eventual arterial hypertension.25 Indeed, after a routine that challenge personal fitness, i. e., like inducing sweat to the forehead, increasing cardio-respiratory rates, and maximal, but not minimal blood pressure, in a few minutes the increased values return to the pre-exercise values, as the minimal arterial pressure. One example of those behaviors of the cardiovascular responses to a challenging series of a week of trainings are exemplified in Figure 4. There is strong evidence that peripheral arterial resistance decreased during the series of challenging exercises because blood perfusion is increased by relaxation of the perforating arteries of the main skeletal muscles of the body, i.e. for the systemic functional hyperemia of the main body muscles.12
Furthermore, Full-Body in-Bed Gym routine mitigates the bad mood that is usually associated to mobility limitations,26,27 strengthening confidence of patient in recovering partial or total independence, and it reduces risks of accidental falls. Eventually, during hospitalizations the monitoring of the responses to challenging trainings could include oxygen saturation and many more fitness variables. Furthermore to speed-up positive changes, the trainings could be performed twice a day to improve fatigue resistance and cardio-respiratory reserve.28,29 Wearable devices are an emerging and cost-effective technology that allows to monitor several biometric data,30 and have been tested in many diseases.31 It might be interesting to add one of these devices (e.g. smartwatches, fitbands, smartphones, etc.) which could represent a guide for the patient during workout (heart rate monitoring and oxyhemoglobin saturation, reminder to perform exercises every day, stopwatch for timing her/his workout.32 In any case, during the initial learning period of Full Body In-bed Gym, all seniors, if not hospitalized, must be supervised by at least one trainer, if not a health professional to avoid harmful exercise. These, in fact, are linked to their fitness and, nothing to say, to comorbidities often present in elderly population. If elderly persons cannot, or are reluctant to perform volitional physical rehabilitation protocols, functional electrical stimulation may mimic those exercises and be almost equally effective.33-41 As detailed in Kern et al., in 2014,36 old persons may be exposed to regular neuromuscular electrical stimulation training. Stimulators for surface electrical stimulation (ES) that are especially suited for elderly people requirements were designed and implemented in Vienna, Austria.42 These constant voltage stimulation devices can be safely applied during home use. Starting two times a week, for a total amount of 24 training sessions (3 × 10 minutes for each session) ES is safe and effective. The subjects ought to be instructed to increase the stimulation intensity until their maximal tolerance is reached. Using this approach a full knee extension is achieved in all subjects. The outcome is a significant increase in muscle strength, associated with an increase of fast muscle fibers, which are the first to respond to ES and are well related to the power of skeletal muscle. ES significantly increased the size of fast type muscle fibers, and the number of Pax7- and NCAM-positive satellite cells. Moreover, analyzed muscle biopsies did not presented signs of muscle damage and/or cellular inflammation.36,43 Altogether, previous results demonstrated that physical exercise, either voluntary or induced by electrical stimulation, improves the functional performance of skeletal muscles, including those essential for ventilation, a main problem in COVID-19 patients. Indeed, it is worth noting that one of the most successful clinical application of skeletal muscles ES is the ventilatory support to person-in-need by pacing of a conditioned diaphragm in quadriplegia and beyond.6,7,44-47 In conclusion, it is never too early and it is never too late to increase daily levels of volitional or FES-induced muscle contractions in aging and early-aging syndromes.19-22 Full-Body in-Bed Gym could help patients suffering with mild cases to prevent chronic COVID-19 syndrome and to recover from weakening of skeletal muscles.
Acknowledgments
A&C M-C Foundation for Translational Myology, Padova, Italy and PAGEpress, Scientific Publications, Pavia, Italy sponsored publication of this typescript.
List of acronyms
- COVID-19
Coronavirus disease 2019
- FES
functional electrical stimulation
- SARS
Severe Acute Respiratory Syndrome
Funding Statement
Funding None
Contributor Information
Ugo Carraro, Email: ugo.carraro@unipd.it.
Giovanna Albertin, Email: giovanna.albertin@unipd.it.
Alessandro Martini, Email: alessandromartini@unipd.it.
Walter Giuriati, Email: walter.giuriati@unipd.it.
Stefano Masiero, Email: stef.masiero@unipd.it.
Helmut Kern, Email: helmut@kern-reha.at.
Christian Hofer, Email: christian.hofer@rehabilitation.lbg.ac.at.
Andrea Marcante, Email: andrea.marcante@aulss8.veneto.it.
References
- 1.Gava P, Kern H, Carraro U. Age-associated power decline from running, jumping, and throwing male masters world records. Exp Aging Res. 2015;41(2):115-35. doi: 10.1080/0361073X.2015.1001648. [DOI] [PubMed] [Google Scholar]
- 2.Hopkins RO, Mitchell L, Thomsen GE, Schafer M, Link M, Brown SM. Implementing a mobility program to minimize post-intensive care syndrome. AACN Adv Crit Care. 2016. Apr-Jun;27(2):187-203. doi: 10.4037/aacnacc2016244. [DOI] [PubMed] [Google Scholar]
- 3.Camillo CA, Osadnik CR, van Remoortel H, Burtin C, Janssens W, Troosters T. Effect of “add-on” interventions on exercise training in individuals with COPD: a systematic review. ERJ Open Res. 2016. Mar 29;2(1):00078-2015. doi: 10.1183/23120541.00078-2015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Czyrny JJ, Kaplan RE, Wilding GE, Purdy CH, Hirsh J. Electrical foot stimulation: a potential new method of deep venous thrombosis prophylaxis. Vascular. Jan-Feb 2010;18(1):20-7. doi: 10.2310/ 6670.2010.00001. Erratum in Vascular 2010. Mar–Apr;18(2): 121. [DOI] [PubMed] [Google Scholar]
- 5.Saleem-Talib S, van Driel VJ, Chaldoupi SM, Nikolic T, van Wessel H, Borleffs CJW, Ramanna H. Leadless pacing: Going for the jugular. Pacing Clin Electrophysiol. 2019. Apr;42(4):395-399. doi: 10.1111/pace.13607. Epub 2019. Feb 25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Glenn WW, Hogan JF, Loke JS, Ciesielski TE, Phelps ML, Rowedder R. Ventilatory support by pacing of the conditioned diaphragm in quadriplegia. N Engl J Med. 1984. May 3;310(18):1150-5. doi: 10.1056/NEJM1984050 33101804. [DOI] [PubMed] [Google Scholar]
- 7.Skalsky AJ, Lesser DJ, McDonald CM. Evaluation of phrenic nerve and diaphragm function with peripheral nerve stimulation and M-mode ultrasonography in potential pediatric phrenic nerve or diaphragm pacing candidates. Phys Med Rehabil Clin N Am. 2015. Feb;26(1):133-43. doi: 10.1016/j.pmr.2014.09.010. [DOI] [PubMed] [Google Scholar]
- 8.Eskridge HR, Park LR, Brown KD. The impact of unilateral, simultaneous, or sequential cochlear implantation on pediatric language outcomes. Cochlear Implants Int. 2021. Jan 12:1-8. doi: 10.1080/14670100.2020.1871267. Online ahead of print. [DOI] [PubMed] [Google Scholar]
- 9.Gallo S, Trevisi P, Rigon C, Caserta E, Seif Ali D, Bovo R, Martini A, Cassina M. Auditory Outcome after Cochlear Implantation in Children with DFNB7/11 Caused by Pathogenic Variants in TMC1 Gene. Audiol Neurootol. 2020. Dec 22:1-7. doi: 10.1159/000510156. Online ahead of print. [DOI] [PubMed] [Google Scholar]
- 10.Carraro U, Gava K, Baba A, Piccione F, Marcante A. Fighting muscle weakness in advanced aging by takehome strategies: Safe anti-aging full-body in-bed gym and functional electrical stimulation (FES) for mobility compromised elderly people. Biol Eng Med. 2016;1:1-4. doi: 10.15761/BEM.1000106. [Google Scholar]
- 11.Carraro U, Gava K, Musumeci A, Baba A, Piccione F, Marcante A. Safe Antiaging Full-Body In-Bed Gym and FES for Lazy Persons: Home In-Bed Exercises for Fighting Muscle Weakness in Advanced Age. In: Rehabilitation Medicine for Elderly Patients, Masiero S, Carraro U, Eds., pag. 43-52. ISBN 978-3-319-57405-9 ISBN 978-3-319-57406-6 (eBook). doi 10.1007/978-3-319-57406-6. [Google Scholar]
- 12.Carraro U, Gava K, Baba A, Marcante A, Piccione F. To Contrast and Reverse Skeletal Muscle Atrophy by Full-Body In-Bed Gym, a Mandatory Lifestyle for Older Olds and Borderline Mobility-Impaired Persons. Adv Exp Med Biol. 2018;1088:549-560. doi: 10.1007/978-981-13-1435-3_25. [DOI] [PubMed] [Google Scholar]
- 13.Ades PA, Keteyian SJ, Wright JS, Hamm LF, Lui K, Newlin K, Shepard DS, Thomas RJ. Increasing Cardiac Rehabilitation Participation From 20% to 70%: A Road Map From the Million Hearts Cardiac Rehabilitation Collaborative. Mayo Clinic proceedings. 2017;92(2):234-242. doi: 10.1016/j. mayocp.2016.10.014. Epub 2016. Nov 15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Vorona S, Sabatini U, Al-Maqbali S, Bertoni M, Dres M, Bissett B, Van Haren F, Martin AD, Urrea C, Brace D, Parotto M, Herridge MS, Adhikari NK, Fan E, Melo LT, Reid WD, Brochard LJ, Ferguson ND, Goligher EC. Inspiratory Muscle Rehabilitation in Critically Ill Adults: A Systematic Review and Meta-Analysis. Ann Am Thorac Soc. 2018. Jun;15(6):735-744. doi: 10.1513/AnnalsATS.201712-961OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Soloveva NV, Makarova EV, Kichuk IV. Coronavirus syndrome: COVID-19 psychotrauma. Eur J Transl Myol. 2020; 30(4): 9302. doi: 10.4081/ejtm.9302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mohsen Khosravi. COVID-19 quarantine: Two-way interaction between physical activity and mental health. Eur J Transl Myol. 2020; 30(4): 9509. doi: 10.4081/ejtm.2020.9509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Angelini C, Siciliano G. Neuromuscular diseases and Covid-19: Advices from scientific societies and early observations in Italy. Eur J Transl Myol. 2020. Jun 22;30(2):9032. doi: 10.4081/ejtm.2019.9032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Moro T, Paoli A. When COVID-19 affects muscle: effects of quarantine in older adults. Eur J Transl Myol. 2020. Jun 17;30(2):9069. doi: 10.4081/ejtm.2019.9069. eCollection 2020. Jul 13. PMID: 32782767 Free PMC article. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.O’Hara Jennifer. Rehabilitation after COVID-19. Mayo Clinic News Network. 2020. October 3. Available: https://newsnetwork.mayoclinic.org/discussion/rehabilitation-after-covid-19/ [Google Scholar]
- 20.Fiorenzato E, Zabberoni S, Costa A, Cona G. Cognitive and mental health changes and their vulnerability factors related to COVID-19 lockdown in Italy. PLoS One. 2021. Jan 27;16(1):e0246204. doi: 10.1371/journal.pone.0246204.eCollection 2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Demeco N, Marotta M, Barletta I, Pino C, Marinaro A, Petraroli L, Moggio L, Ammendolia A. Rehabilitation of patients post-COVID-19 infection: a literature review. J Int Med Res. 2020. Aug;48(8):300060520948382. doi: 10.1177/03000 60520948382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22 Wang TJ, Chau B, Lui M, Lam GT, Lin N, Humbert S. Physical Medicine and Rehabilitation and Pulmonary Rehabilitation for COVID-19. Am J Phys Med Rehabil. 2020. Sep;99(9):769-774. doi: 10.1097/PHM.0000000000001505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Smith JM, Lee AC, Zeleznik H, Coffey Scott JP, Fatima A, Needham DM, Ohtake PJ. Home and Community-Based Physical Therapist Management of Adults With Post-Intensive Care Syndrome. Phys Ther. 2020. Jul 19;100(7):1062-1073. doi: 10.1093/ptj/pzaa059. PMID: 32280993; PMCID: PMC7188154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Available: https://www.youtube.com/watch?v=N1RuG3371-Y&feature=youtu.be [Google Scholar]
- 25.Börjesson M, Onerup A, Lundqvist S, Dahlöf B. Physical activity and exercise lower blood pressure in individuals with hypertension: narrative review of 27 RCTs. Br J Sports Med. 2016. Mar;50(6):356-61. doi: 10.1136/bjsports-2015-095786. Epub 2016. Jan 19. [DOI] [PubMed] [Google Scholar]
- 26.Carneiro LS, Fonseca AM, Serrão P, Mota MP, Vasconcelos-Raposo J, Vieira-Coelho MA. Impact of physical exercise on catechol-O-methyltransferase activity in depressive patients: a preliminary communication Affect Disord. 2016. Mar 15;193:117-22. doi: 10.1016/j.jad.2015.12.035. [DOI] [PubMed] [Google Scholar]
- 27.Simõe Seguro C, Silva Rebelo AC, Silva AG, Malaquias M, dos Santos A, Cardoso JS, Apolinário V, Veiga Jardim PC, Gentil P. Use of low volume, high effort resistance training to manage blood pressure in hypertensive patients inside a public hospital: a proof of concept study Eur J Transl Myol. Eur J Transl Myol. 31(1): 9547, 2021. doi: 10.4081/ejtm.2021.9547 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Masiero S, Maccarone MC, Agostini F. Health resort medicine can be a suitable setting to recover disabilities in patients tested negative for COVID-19 discharged from hospital? A challenge for the future. Int J Biometeorol. 2020. Oct;64(10):1807-1809. doi: 10.1007/s00484-020-01947-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Masiero S, Zampieri D, Del Felice A. The Place of Early Rehabilitation in Intensive Care Unit for COVID-19. Am J Phys Med Rehabil. 2020. Aug;99(8):677-678. doi: 10.1097/PHM.000000000 0001478. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Khoshmanesh F, Thurgood P, Pirogova E, Nahavandi S, Baratchi S. Wearable sensors: At the frontier of personalised health monitoring, smart prosthetics and assistive technologies. Biosens Bioelectron. 2021. Mar 15;176:112946. doi: 10.1016/j.bios.2020.112946. Epub 2020. Dec 30. [DOI] [PubMed] [Google Scholar]
- 31.Gatsios D, Antonini A, Gentile G, Marcante A, Pellicano C, Macchiusi L, Assogna F, Spalletta G, Gage H, Touray M, Timotijevic L, Hodgkins C, Chondrogiorgi M, Rigas G, Fotiadis DI, Konitsiotis S. Feasibility and Utility of mHealth for the Remote Monitoring of Parkinson Disease: Ancillary Study of the PD_manager Randomized Controlled Trial. JMIR Mhealth Uhealth. 2020. Jun 29;8(6):e16414. doi: 10.2196/16414. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Graña Possamai C, Ravaud P, Ghosn L, Tran VT. Use of wearable biometric monitoring devices to measure outcomes in randomized clinical trials: a methodological systematic review BMC Med. 2020. Nov 6;18(1):310. doi: 10.1186/s12916-020-01773-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Kern H, Carraro U, Adami N, Biral D, Hofer C, Forstner C, Mödlin M, Vogelauer M, Pond A, Boncompagni S, Paolini C, Mayr W, Protasi F, Zampieri S. Home-based functional electrical stimulation rescues permanently denervated muscles in paraplegic patients with complete lower motor neuron lesion. Neurorehabil Neural Repair. 2010. Oct;24(8):709-21. doi: 10.1177/1545968310366129. [DOI] [PubMed] [Google Scholar]
- 34.Carraro U, Kern H. Severely atrophic human muscle fibers with nuclear misplacement survive many years of permanent denervation. Eur J Transl Myol. 2016. Jun 13;26(2):5894. doi: 10.4081/ejtm.2016.5894. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Carraro U, Kern H, Gava P, Hofer C, Loefler S, Gargiulo P, Mosole S, Zampieri S, Gobbo RB, Piccione P, Marcante A, Baba A, Schils S, Pond A, Gava F. Biology of muscle atrophy and of its recovery by FES in aging and mobility impairments: roots and by-products. Eur J Transl Myol. 2015. Aug 25;25(4):221-30. doi: 10.4081/ejtm.2015.5272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Kern H, Barberi L, Löfler S, Sbardella S, Burggraf S, Fruhmann H, Carraro U, Mosole S, Sarabon N, Vogelauer M, Mayr W, Krenn M, Cvecka J, Romanello V, Pietrangelo L, Protasi F, Sandri M, Zampieri S, Musaro A. Electrical stimulation counteracts muscle decline in seniors. Front Aging Neurosci. 2014. Jul 24;6:189. doi: 10.3389/fnagi.2014.00189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Carraro U, Kern H, Gava P, Hofer C, Loefler S, Gargiulo P, Edmunds K, Árnadóttir ÍD, Zampieri S, Ravara B, Gava F, Nori A, Gobbo V, Masiero S, Marcante A, Baba A, Piccione F, Schils S, Pond A, Mosole S. Recovery from muscle weakness by exercise and FES: lessons from Masters, active or sedentary seniors and SCI patients. Aging Clin Exp Res. 2017. Aug;29(4):579-590. doi: 10.1007/s40520-016-0619-1. [DOI] [PubMed] [Google Scholar]
- 38.Zampieri S, Mosole S, Löfler S, Fruhmann H, Burggraf S, Cvečka J, Hamar D, Sedliak M, Tirptakova V, Šarabon N, Mayr W, Kern H. Physical exercise in aging: nine weeks of leg press or electrical stimulation training in 70 years old sedentary elderly people. Eur J Transl Myol. 2015. Aug 25;25(4):237-42. doi: 10.4081/ejtm.2015 .5374.eCollection 2015. Aug 24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Kern H, Carraro U. Home-Based Functional Electrical Stimulation of Human Permanent Denervated Muscles: A Narrative Review on Diagnostics, Managements, Results and Byproducts Revisited 2020. Diagnostics (Basel). 2020. Jul 29;10(8): 529. doi: 10.3390/diagnostics 10080529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Recenti M, Ricciardi C, Edmunds K, Gislason MK, Gargiulo P. Machine learning predictive system based upon radiodensitometric distributions from mid-thigh CT images. Eur J Transl Myol. 2020. Apr 1;30(1):8892. doi: 10.4081/ejtm.2019.8892. eCollection 2020. Apr 7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Albertin G, Ravara B, Kern H, Hofer C, Loefler S, Jurecka W, Guidolin D, Rambaldo A, Porzionato A, De Caro R, Zampieri S, Pond A, Alaibac M, Carraro U. Two-years of home based functional electrical stimulation recovers epidermis from atrophy and flattening after years of complete Conus-Cauda Syndrome. Medicine (Baltimore). 2019. Dec;98(52):e18509. doi: 10.1097/MD. 0000000000018509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Krenn M, Haller M, Bijak M, Unger E, Hofer C, Kern H, Mayr W. Safe neuromuscular electrical stimulator designed for the elderly. Artif Organs. 2011. Mar;35(3):253-6. doi: 10.1111/j.1525-1594.2011.01217.x. [DOI] [PubMed] [Google Scholar]
- 43.Zampieri S, Pietrangelo L, Loefler S, Fruhmann H, Vogelauer M, Burggraf S, Pond A, Grim-Stieger M, Cvecka J, Sedliak M, Tirpáková V, Mayr W, Sarabon N, Rossini K, Barberi L, De Rossi M, Romanello V, Boncompagni S, Musarò A, Sandri M, Protasi F, Carraro U, Kern H. Lifelong physical exercise delays age-associated skeletal muscle decline. J Gerontol A Biol Sci Med Sci. 2015. Feb;70(2):163-73. doi: 10.1093/Gerona/ glu006. Epub 2014. Feb 18. [DOI] [PubMed] [Google Scholar]
- 44.Glenn WW, Phelps ML. Diaphragm pacing by electrical stimulation of the phrenic nerve. Neurosurgery. 1985. Dec;17(6):974-84. doi: 10.1227/00006123-198512000-00021. [DOI] [PubMed] [Google Scholar]
- 45.Berger D, Bloechlinger S, von Haehling S, Doehner W, Takala J, Z'Graggen WJ, Schefold JC. Dysfunction of respiratory muscles in critically ill patients on the intensive care unit. J Cachexia Sarcopenia Muscle. 2016. Sep;7(4):403-12. doi: 10.1002/jcsm.12108. Epub 2016. Mar 9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Peñuelas O, Keough E, López-Rodríguez L, Carriedo D, Gonçalves G, Barreiro E, Lorente JÁ. Ventilator-induced diaphragm dysfunction: translational mechanisms lead to therapeutical alternatives in the critically ill. Intensive Care Med Exp. 2019. Jul 25;7(Suppl 1):48. doi: 10.1186/s40635-019-0259-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Marrero HDJG, Stålberg EV, Cooray G, Corpeno Kalamgi R, Hedström Y, Bellander BM, Nennesmo I, Larsson L. Neurogenic vs. Myogenic Origin of Acquired Muscle Paralysis in Intensive Care Unit (ICU) Patients: Evaluation of Different Diagnostic Methods. Diagnostics (Basel). 2020. Nov 18;10(11):966. doi: 10.3390/ diagnostics10110966. [DOI] [PMC free article] [PubMed] [Google Scholar]