

Abstract
Emerging research tests the impact of United States Medicaid home and community-based (HCBS) waiver policy on outcomes for people with intellectual and developmental disabilities; however, this body of work has yet to be synthesized. We conducted a scoping review to establish what is known about the impact of Medicaid HCBS policy on the lives of people with intellectual and developmental disabilities. Seven studies met final inclusion criteria. Their findings contribute to preliminary evidence that Medicaid HCBS waivers provide economic benefit at the state- and federal-level, reduce unmet healthcare needs, increase the likelihood that parents will be able to continue working, and reduce racial disparities in access to care. Additional work should compare HCBS waiver programmes, and their causal pathways, as well as draw international comparisons to similar programing, to determine essential infrastructure needed for a successful HCBS programme.
Keywords: home and community-based services, intellectual and developmental disabilities, disability policy, Medicaid, autism
Introduction
Policy research is undertaken to inform, influence, and change public policy. Its goal is to find solutions to fundamental problems, map alternative approaches, and advance major public policy programmes. Key to policy research is that it explicitly examines differences in the intent, effect, and cost of a programme (Moran, 2008). Policy research seeks to determine which policy decision is most appropriate for addressing needs and developing programmes that are beneficial and cost-effective. Given the impact of policy on the lives of everyday people and the financial cost of social programmes, policy research is a necessary tool to understand how to optimize the impact of policies and reduce their cost. This scoping review examines the impact of an integral and complex disability policy: U.S. Medicaid home and community-based services waivers.
Medicaid Research in the General Population
Medicaid provides health care coverage to more than 40 million people in the U.S. (Bruen & Holahan, 2001). Medicaid serves low-income adults, children, pregnant women, elderly adults, and individuals with disabilities (Centers for Medicare and Medicaid Services, 2019). According to the Medicaid and CHIP Payment and Access Commission (MACPAC) 2018 report to Congress, over 10 million people qualify for Medicaid on the basis of disability. This population includes adults with disabilities that present at birth and those who have acquired disabling conditions through illness, injury, or trauma. These disabilities include physical disabilities, intellectual and developmental disabilities (I/DD), and serious behavioral disorders or mental illness (Centers for Medicare and Medicaid Services, 2019).
This paper will focus specifically on U.S. Medicaid policy for a primary group of beneficiaries, people with intellectual and developmental disabilities (I/DD). U.S. Medicaid policy for people with I/DD, and in particular, Medicaid home and community-based services, seeks to address barriers to affordable, quality care for people with I/DD. An understanding of how this programme is or is not working for people with I/DD will help to fill research gaps and contribute to evidence that will lead to better overall health outcomes for all people with disabilities. All countries, both low and high-income, need to improve their systems of care for the global population of people with disabilities.
The vast majority of Medicaid policy research conducted to date has analyzed the impact of the Medicaid expansion on outcomes for uninsured poor adults, pregnant women, and children (Haber et al., 2000; Howell, 2001; Howell et al., 2012). Previous research examines direct impacts in utilization, access to care, and health outcomes as a result of a change in Medicaid policy at the federal or state-level. The Oregon Health Insurance Experiment, which used a randomized design to provide health insurance to a group of low-income uninsured adults, considered additional indirect impacts of Medicaid on labor market activity and uptake of government benefits (Baicker et al., 2011). The field of Medicaid policy research has been established and synthesized (Howell, 2001; Howell & Kenney, 2012; Wysocki et al., 2015); however, a primary group of Medicaid beneficiaries, people with I/DD, are often not explicitly studied in Medicaid research though they would be included by default in studies that leverage full samples of Medicaid beneficiaries.
Medicaid Home and Community-Based Services
Advances in medicine and technology are enabling many people with I/DD to live longer and more independently than ever before. Recent estimates show that about 17% of children have one or more I/DD (Zablotsky et al., 2019). These I/DDs last throughout a person’s lifetime and occur across all racial, ethnic, and socioeconomics groups. The number of individuals aging with these lifelong I/DDs are increasing and expected to double by 2030 (Hahn et al., 2012).
Medicaid is intended to provide a broad range of medical and long-term care services to people with I/DD to support them to live in their homes and communities. These are also known as home and community-based services (HCBS). Medicaid HCBS waivers are the largest, and often the only, provider of long-term services and supports for people with I/DD in the United States. These services and supports include in-home nursing, non-medical and medical transportation, respite care, wheelchairs, meals, and assistive technology (Kitchener et al., 2005).
Through these services and supports, HCBS help to ensure that people with disabilities are fully integrated into community life, rather than living in costly, isolated, and segregated institutions. In 2009, the most recent year for which data are available, the average annual expenditure for state institutions was $188,318, compared to an average of $42,486 for Medicaid-funded home and community-based services (Lakin et al., 2010). Even in states with publicly funded long-term care systems, such as HCBS, government funds are still allotted to institutions despite this difference in cost. Some states have taken aggressive steps to change this imbalance of care. States have expanded their HCBS waivers in response to advocate pressure to close institutions for people with disabilities, the Supreme Court’s Olmstead decision, and as a result of increasing nursing home costs (Shirk, 2006). Increasing the use of HCBS is a high priority to consumers with disabilities and the payers of these services. Most Medicaid beneficiaries express a strong preference for HCBS: they want to live in their own homes, participate in their communities, and have greater control over daily decisions (Shirk, 2006).
Because Medicaid is funded jointly by states and the U.S. federal government, these HCBS programmes vary greatly from state-to-state. Research has examined various outcomes of Medicaid HCBS in the general population. It has shown better clinical outcomes for those provided community-based, long-term services rather than institutional care in the aging population (Marek et al., 2005). Marek et al. (2005) found that on measures of cognition, activities of daily living, depression, and incontinence, the group that aged in community-based, long-term care programmes stabilized or improved at statistically significant levels, compared to those aging in institutional-based care.
Reviews of Medicaid HCBS papers have been conducted in the general population already as well. A systematic review of literature from 1995 to 2012 on HCBS vs. institutional care for older adults by Wysocki and colleagues (2015) found that nursing home and assisted living residents did not differ in terms of physical function, cognition, mental health, or mortality outcomes; and evidence was insufficient for cost comparisons. They called for more and better research to draw more robust conclusions regarding service setting and outcome, and specifically emphasized the need for studies evaluating HCBS effectiveness (Wysocki et al., 2015).
Policy research on Medicaid programmes for which the main intent is to support people with I/DD is now needed to ensure HCBS programmes are addressing needs and functioning efficiently. Emerging research tests the impact of Medicaid HCBS policy on outcomes for children and adults with I/DD, however, this body of work has yet to be synthesized. A synthesis of Medicaid HCBS waiver policy research has two benefits. First, it will provide a better understanding of how we are serving children and adults with intellectual and developmental disabilities and help states to determine the extent to which their needs are being addressed. Second, it can aid in identifying key gaps in knowledge about the impact of Medicaid HCBS waiver policy on people with intellectual and developmental disabilities in order to inform future research efforts.
Aims of This Scoping Review
The overall purpose of this scoping review is to synthesize what is known about the impact of federal and state Medicaid HCBS policy on the lives of people with I/DD. To our knowledge, it is the first scoping review of its kind that will assess studies published to date that analyze the impact of Medicaid HCBS policy for those with I/DD. It aims to describe the state of the field of Medicaid research in relation to I/DD, in order to build a knowledge base using key findings across studies, to inform policy stakeholders, and to guide future research questions in this area. More specifically, this study aims to identify gaps in the literature and to synthesize existing knowledge in order to identify the ways in which Medicaid HCBS policy is currently addressing the overall needs of those with I/DD.
Method
We conducted a scoping review to broadly determine what is known about the impact of U.S. Medicaid HCBS policy on the lives of those with I/DD. In contrast to a systematic review, as defined in the Cochrane Handbook (2019), which critically appraises the relevant research and the quality of evidence for a narrowly defined question, the intent of a scoping review is to broadly review the literature to examine the extent, range, and nature of research activities and to identify gaps (Arksey & O’Malley, 2005). We employed the methodological framework for scoping reviews developed by Arksey and O’Malley (2005). We examined research that uses quantitative methods to test the impact of Medicaid HCBS waivers at the federal, state, or county-level on a concrete outcome for people with I/DD. We excluded studies that did not directly test the effect of Medicaid HCBS waiver policy but rather defined the scope of a policy or summarized the population the policy is intending to serve. In order to ensure we included the totality of studies in this specific area, we conducted this inclusive search of all studies related to Medicaid and I/DD first, without explicit date ranges. Then we further limited our search to only studies that more specifically tested an impact of Medicaid HCBS waiver policy.
Identification of Relevant Studies
We systematically searched PubMed, PsychInfo, the Cumulative Index to Nursing and Allied Health Literature (CINAHL), and the Education Resources Information Center (ERIC) with the guidance of a reference librarian who specializes in systematic and scoping review methodology. We comprehensively searched key terms related to I/DD, disability, Medicaid, and HCBS. These key terms were truncated and broadened to enable comprehensive coverage per guidelines of scoping review methodologies as well as to account for changes in disability diagnosis language (Arksey & O’Malley, 2005; Levac et al., 2010). I/DD was expanded to include keyword searches for disab* and (intellectual OR developmental), (impair* OR retard*) or autis*. For example, when we searched ERIC using the text “autis* AND Medicaid”, “(impair* OR retard*) and Medicaid”, “disab* AND (intellectual OR developmental) AND Medicaid”, OR “I/DD AND Medicaid”, we identified 231 articles.
We also hand-searched studies published ahead of print in the American Journal on Intellectual and Developmental Disabilities, Research in Developmental Disabilities, and the Journal of Policy and Practice in Intellectual Disabilities. Finally, we hand searched the reference lists of all included studies to ensure that there were no additional studies that might meet inclusion criteria. The first author performed the search with the help of the reference librarian and second author and managed and analyzed search results using EndNote® software.
Study Selection
After removing duplicates, the first and second author scanned titles to assess whether studies addressed I/DD and Medicaid policy (i.e., included any of our key terms). The first and second author then scanned abstracts to ensure that abstracts: (1) included participants with I/DD; (2) focused on Medicaid HCBS waivers; and (3) tested an aspect of Medicaid HCBS waiver policy on a given outcome. Studies that (1) described or summarized Medicaid HCBS waiver policy that serves those with I/DD or (2) did not test an aspect of Medicaid HCBS waiver policy on an outcome, but rather an externalized factor on Medicaid HCBS waiver use were excluded. For example, several studies looked at demographic and health characteristics of Medicaid beneficiaries while others looked at service use patterns without linking these patterns to an outcome. Additionally, several studies only tested an impact of Medicaid HCBS waiver policy for beneficiaries with autism spectrum disorder (ASD). Though it was unclear in the Medicaid data if those with ASD had co-occurring intellectual disabilities, we chose to include these studies because ASD is one of the most common I/DDs. Studies identified for inclusion after the abstract search were moved to a separate folder in EndNote for full-text analysis. All authors then analyzed full texts to identify the final list of included studies. Any disagreements were resolved by in-depth discussion and consensus.
Data Extraction and Reporting
After identifying the final list of studies included in this review, the first and second author extracted theoretically and/or methodologically relevant characteristics. These included data source and location, diagnostic group, sample, aims and purpose, type of analysis, and main findings. Additionally, all authors identified the primary policy questions and major themes addressed by each article. These characteristics were analyzed to synthesize the existing knowledge, to identify common themes and gaps in the literature, and to identify implications for future research, practice, and policy (Levac et al., 2010). When reporting results, we categorized studies based on whether they sought to assess the effect, cost, or intent of a policy on a key outcome, a grouping strategy aligned with established guidelines for categorization of policy research (Moran et al., 2008).
Results
Our search identified 764 unique studies. The study selection process, including specific inclusion and exclusion criteria, is presented in Figure 1. Studies were identified in PubMed (n=732), PsychInfo (n=491), CINAHL (n=360), and ERIC (n=231). Of the 1,814 studies identified by this search, 1,050 were duplicates (58%).
Figure 1.
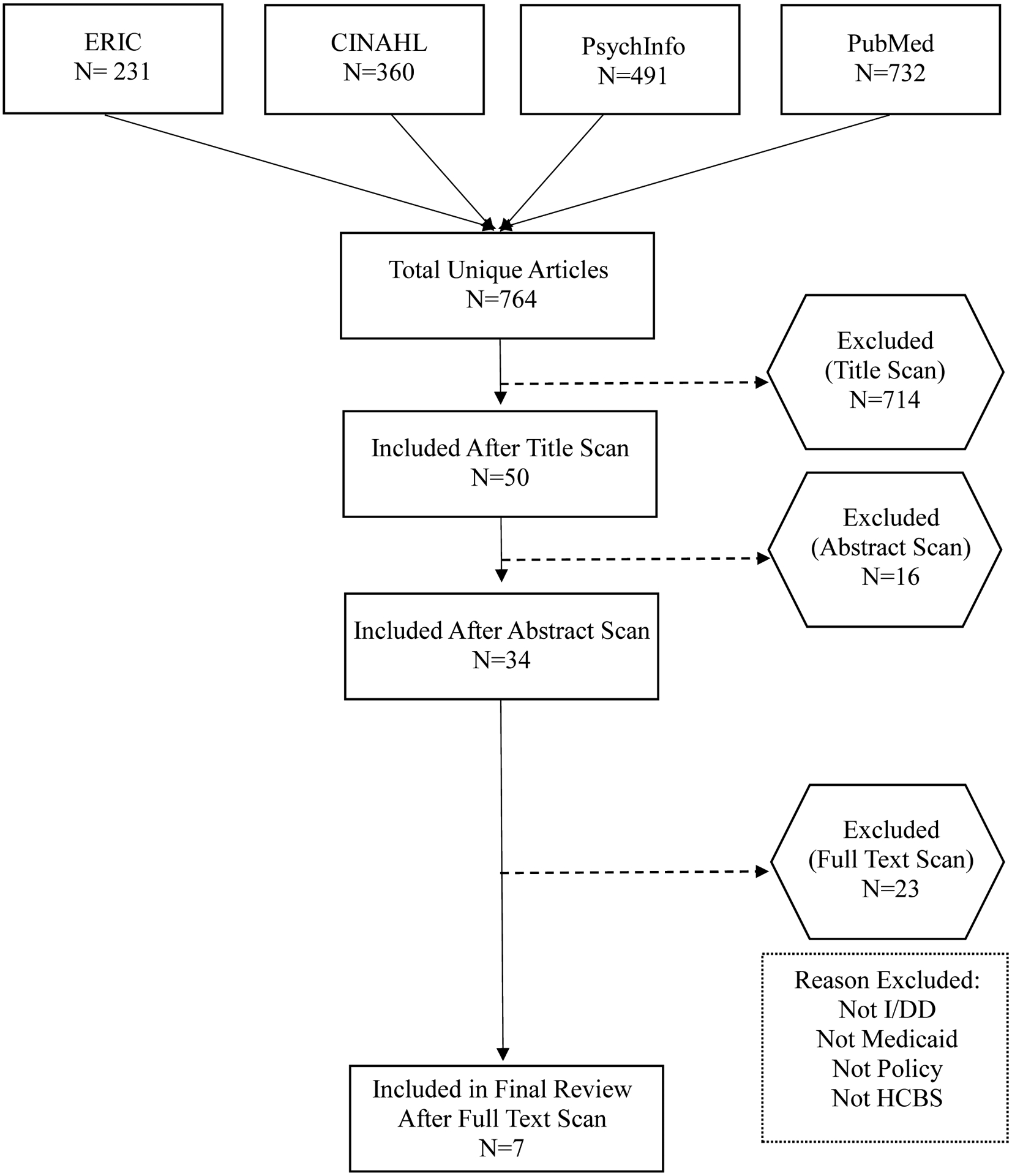
Flowchart of Article Selection
Studies were excluded in stages, as detailed in Figure 1. In total, 714 studies were excluded after the title scan, primarily because most were not related to I/DD and/or Medicaid. Sixteen additional studies were excluded after the abstract scan. At this step, we sought to specifically identify studies that tested an aspect of Medicaid policy to determine its effect on an outcome for those with I/DD. Full-text scan of studies excluded an additional 23 studies because the studies did not test an area of Medicaid policy, but rather summarized the scope of Medicaid policy or analyzed the effect of an external factor on Medicaid use. Eleven studies focused on measuring the effect of Medicaid policy on those with I/DD. Of these, seven studies were included in our final review (Table 1) because they focused on measuring the effect of Medicaid HCBS policy on those with I/DD.
Table 1.
Characteristics of Included Studies
| Study | Data Source | Diagnostic Group | Sample Size | Age Range | Purpose | Analysis | Findings & Recommendations | Policy Question |
|---|---|---|---|---|---|---|---|---|
| Barton & Gotto, (2016) | Missouri state-level economic data from 2012 in the form of IMPLAN regional economic and industry transaction data drawn from federal agencies responsible for data collection, including the Bureau of Economic Analysis, the U.S. Bureau of Labor Statistics, and the U.S. Census Bureau | Individuals with intellectual and developmental disabilities enrolled in Missouri’s PfH program | Year 1: 813, Year 2: 1325, Year 3: 2,004 | No age range | To explore the statewide economic and fiscal impact of Missouri’s Partnership for Hope (PfH) Medicaid waiver in the first 3 years of operation | IMPLAN input–output economic modeling data and software were used to assess the statewide economic and fiscal impacts of Missouri’s PfH Medicaid waiver | County and state investment of $3.5 million each leveraged $11.7 million in federal funds, contributed almost $22.2 million to Missouri’s gross state product (GSP), and was responsible for more than 435 jobs for Missourians. For each $1 spent by the state and counties (each), $5.31 worth of supports and services were provided to Missourians with I/DD through PfH. PfH HCBS spending facilitates economic growth | What is the economic impact of Missouri’s Medicaid HCBS waiver program, Partnership for Hope? |
| Eskow et al., (2011) | Maryland Autism Services Survey (MASS) | Families receiving Maryland HCBS autism waiver services and those on the registry waiting for waiver services | 861 (waiver: 229; registry: 632) | Families with children age 2–21 | To investigate how the Maryland Medicaid HCBS waiver for children with autism affects family quality of life and employment status | The survey was statistically analyzed, and a Wilk’s lambda multivariate analysis was used to determine the extent to which waiver status was a predictor of family quality of life and employment status | Waiver recipients report higher QoL and significantly more part time employment than those on the registry. Employment status improves after receiving waiver services | What is the effect of Maryland’s Medicaid HCBS waiver program for children with autism on family quality of life and employment? |
| Eskow et al., (2014) | Maryland Autism Services Survey-Revised (MASS-R) | Families receiving Maryland HCBS autism waiver services and those on the registry waiting for waiver services | 552 (waiver: 282; registry: 270) | Families with children age 2–21 | To establish additional and methodologically stronger evidence for the usefulness of the Maryland Medicaid HCBS waiver for children with autism | Statistical analyses were carried out to evaluate the effectiveness of Maryland waiver services compared to minimal services while waiting on the registry. Additional exploratory analyses were used to predict child improvement outcomes from the frequency of different types of waiver services | Waiver recipients reported more improvement in independent living skills and family quality of life over the last year compared to those on the registry. More frequent intensive individual support services and therapeutic integration were statistically predictive of improvement in a variety of domains. Waiver programs may be promising for improving child and family functioning | What are the outcomes of families participating in autism-specific Medicaid HCBS waiver services in Maryland? |
| Leslie et al., (2017a) | 2003, 2007, and 2011 waves of the National Survey of Children’s Health with detailed information on the Medicaid HCBS waiver programs of 35 states* | Autistic children | 154,060 over 3 waves of data (1,824 of which are autistic children) | 2–17 years | To address how well waivers meet the needs of autistic children and to better understand whether specific waiver features are more effective in meeting those needs | Quasi-difference-in-difference-in-differences models were used to determine the effects of waivers and their characteristics on parent report of unmet healthcare needs of children with ASD compared to children without ASD | Greater waiver cost limits per child, estimated costs of services, and enrollment limits are associated with significant decreases in the adjusted rate of unmet healthcare needs, with variation by household income. Medicaid HCBS waivers significantly decrease the unmet need for healthcare among children with ASD, most substantially among those who would not otherwise qualify for Medicaid | What are the effects of different state-specific HCBS waiver policies on the unmet healthcare needs of autistic children? |
| Leslie et al., (2017b) | Two consecutive waves (2005–06 and 2009–10) of the National Survey of Children with Special Health Care Needs with information on 35 state Medicaid HCBS waiver programs* | Autistic children | 17,693 children (2,647 autistic children, 15,521 with asthma alone, 275 autistic children with asthma) | 2–17 years | To determine the effects of waivers on whether parents of autistic children had to stop working because of their child’s condition | Standard multivariable logistic regression models, specified as quasi-difference-in-difference-in-differences models, were used with the unit of analysis as the child | Increases in the Medicaid HCBS waiver cost limit and enrollment limit significantly reduced the likelihood that a parent had to stop working, although results varied by household income. Medicaid waivers are effective policies to address the care-related needs of children with autism spectrum disorder | What are the effects of Medicaid HCBS waivers on labor-market participation of families of autistic children? |
| Mandell et al., (2012) | Medicaid Analytic eXtract database from 2004 and the Area Resource File | Medicaid-enrolled autistic children | 28,428 | 5–21 years | To examine whether increased provision of community-based services is associated with decreased psychiatric hospitalizations among children with ASD | Retrospective cohort study using discrete-time logistic regression was used to examine the association of service use in the preceding 60 days with the risk of hospitalization | Each $1000 increase in spending on respite care during the preceding 60 days resulted in an 8% decrease in the odds of hospitalization in adjusted analysis. Use of therapeutic services was not associated with reduced risk of hospitalization. States should increase the availability of respite care for Medicaid-enrolled children with ASD | How does spending on respite care for HCBS waivers impact the number of psychiatric hospitalizations for children and adolescents with ASD? |
| Shattuck et al, (2009) | Medicaid enrollment data from January 1, 2000, through November 30, 2006, obtained from Wisconsin’s Department of Health and Family Services | Medicaid-enrolled autistic children | 1,822 | 2–14 years | To examine the utilization of Wisconsin’s Medicaid funding for autism intervention before and after a major shift in program administration from the state-administered Early and Periodic Screening, Diagnosis, and Treatment program (EPSDT) to a county-managed HCBS waiver | Medicaid enrollment data were analyzed for 1,822 children with autism from 2000 through 2006, as were geocoded demographic data and decennial census data. Beneficiaries’ data were compared with demographic data for Wisconsin’s general population | Compared with averages for all Wisconsin families, new Medicaid beneficiaries in 2000 were more likely to be from census tracts with a high proportion of white families with high socioeconomic status. Disparities decreased by 2006, two years after a change from a Medicaid fee-for-service structure to a Medicaid HCBS waiver structure. As more states consider carve-out benefits for children with autism, close attention needs to be paid to the potential for disparities and the influence of mode of administration on utilization. | What was the effect on utilization when Wisconsin’s Medicaid program for autism intervention transferred funding from EPSDT to a county-managed HCBS waiver? |
The 35 states included in the National Survey of Children with Special Health Care Needs are Alabama, Alaska, Arizona, Arkansas, California, Colorado, Connecticut, Delaware District of Columbia, Florida, Georgia, Hawaii, Idaho, Illinois, Indiana, Iowa, Kansas, Kentucky, Louisiana, Maine, Maryland, Massachusetts, Michigan Minnesota, Mississippi, Missouri, Montana, Nebraska, Nevada, New Hampshire, New Jersey, New Mexico, New York, North Carolina, North Dakota, Ohio, Oklahoma, Oregon, Pennsylvania, Rhode Island, South Carolina, South Dakota, Tennessee, Texas, Utah, Vermont, Virginia, Washington, West Virginia, Wisconsin, Wyoming
Methodological Characteristics
The seven included studies (Barton et al., 2015; Eskow et al., 2011; Eskow et al., 2014; Leslie et al., 2017a; Leslie et al., 2017b; Mandell et al., 2012; Shattuck et al., 2009) employed a variety of methodologies to explore the cost, effect, and intent of aspects of Medicaid HCBS waiver policy. Each article addressed a gap in empirical research regarding outcomes of Medicaid HCBS policy for people with I/DD. Two of the studies (Leslie et al., 2017a; Leslie et al., 2017b) used data from the National Survey of Children with Special Health Care Needs. Another two studies (Eskow et al., 2011; Eskow et al., 2014) used family survey data associated with the Maryland Medicaid HCBS Waiver; both of these studies matched waiver recipients to those on the waiting list to examine the effect of Autism Waiver Services and state-specific HCBS waiver programmes.
One study (Mandell et al., 2012) used the Medicaid eXtract database for information on ASD diagnosis, service use, demographic characteristics, and state or county of residence. This study used discrete time logistic regression to compare the aforementioned factors. One study (Shattuck et al., 2009) obtained Medicaid enrollment claims data from state Medicaid agencies. Shattuck et al., (2009) additionally geocoded geographic data and decennial census data (the United States census collected every 10 years) to explore geographic disparities in the rollout of Medicaid in Wisconsin. Finally, one study (Barton et al., 2015) used IMPLAN input-output economic modeling data and software drawn from federal agencies.
Study Outcomes
All seven studies examined an area of Medicaid HCBS policy and its impact on an outcome for those with I/DD. Five of the studies (Barton et al., 2015; Eskow et al., 2011; Eskow et al., 2014; Leslie et al., 2017a; Leslie et al., 2017b) examined the effect of a state HCBS policy on outcomes for children, adults, and parents within the state. The remaining two studies (Mandell et al., 2012; Shattuck et al., 2009) used national level data to compare outcomes across state and county-level HCBS programmes. We identified which of our studies examined the cost, effect, and intent of Medicaid policy.
Effect.
All seven studies examined effects of Medicaid policy for those with I/DD. An effect is a finite, measurable outcome. Of these studies, four (Leslie et al., 2017a; Leslie et al., 2017b; Mandell et al., 2012; Shattuck et al., 2009) did not examine cost as the primary outcome and will therefore be discussed further in this section.
Two of the studies (Leslie et al., 2017a; Leslie et al., 2017b) looked at the effects of Medicaid HCBS waivers on children with ASD and their parents. Both relied on parent-reported surveys to determine if state Medicaid waivers are effective policies for addressing the care-related needs of children with ASD. The studies found that Medicaid HCBS waivers significantly decrease the unmet healthcare needs of children with ASD, especially among those who might not otherwise qualify for Medicaid. They also found the waivers reduce the likelihood that a parent had to stop working to care for their child.
Shattuck et al. (2009) found that among Medicaid beneficiaries in Wisconsin in 2000, children with ASD receiving Medicaid services were more likely to be from white families with high socioeconomic status. These racial disparities did however decrease after a 2006 change to a Medicaid HCBS waiver rather than the former fee-for-service structure. Lastly, Mandell et al. (2012) examined specific services provided through HCBS waivers and found that increasing respite and home and community aide services provided through Medicaid HCBS waivers decreased risk of psychiatric hospitalizations for children, adolescents, and young adults with ASD.
Cost.
Five of the seven articles (Barton et al., 2015; Leslie et al., 2017a; Leslie et al., 2017b; Mandell et al., 2012; Shattuck et al., 2009) examined cost as an outcome of a Medicaid policy. Of these five, only one of the studies (Barton et al., 2015) looked at changes in cost, or economic impact, as the primary outcome.
Barton et al. (2015) looked at the financial impact of specific state-level strategies or programmes. They examined Missouri’s Partnership for Hope (PfH) HCBS waiver that targets services for individuals with I/DD. The PfH programme seeks to prevent or delay institutional services for individuals who require minimal services to continue living in the community. Minimal services include assistive technology, community employment, and day services. They found that the PfH waiver programme contributed almost $22.2 million to Missouri’s gross state product and was responsible for more than 435 jobs for Missourians. PfH contributed greatly to the state’s overall economic growth.
Intent.
Two of the seven studies (Eskow et al., 2011; Eskow et al., 2014) examined whether the original intent of a Medicaid policy for children or adults with I/DD was being fulfilled. Medicaid HCBS waivers are intended to meet the needs of people who prefer to receive long-term care services and supports in their home or community, rather than in an institutional setting (Kitchener et al., 2005).
Both studies explored the impact of Maryland’s Medicaid HCBS waiver programme for children with ASD and their families. The studies found that families receiving services through the waiver programme reported higher family quality of life, improvement in independent living skills and better employment status. Furthermore, Eskow et al. (2014) found that more frequent intensive individual support services and therapeutic integration were associated with improvement in independent living skills, which is a primary outcome waiver services were designed to improve.
Discussion
The purpose of this scoping review was to synthesize what is known about the impact of U.S. federal and state Medicaid HCBS policy on the lives of those with I/DD. We assessed all studies published to date that analyzed concrete impacts of Medicaid HCBS policy on people with I/DD. Our overall intent was to build a preliminary knowledge base to inform policy stakeholders and to guide future research questions in this growing area of inquiry.
We included seven studies in this scoping review that included participants with I/DD, focused on Medicaid, and tested an aspect of Medicaid HCBS policy on a given outcome. The studies used a variety of methodologies to explore the cost, effect, and intent of some aspect of Medicaid HCBS policy. The overall goal of each paper was to address a gap in empirical research regarding outcomes for those with I/DD due to Medicaid. We only identified a relatively small number of studies that were published recently (2009–2018) despite searching for all studies published to date. This indicates that Medicaid policy research focused on I/DD is a recent and emerging area of research inquiry.
In contrast to a previous systematic review of Medicaid HCBS waiver policy in older adults that found few benefits (Wysocki et al., 2015), our findings provide preliminary evidence that Medicaid HCBS waivers provide economic benefit for states, reduce unmet healthcare needs for people with I/DD, increase the likelihood that parents will be able to continue working, and reduce racial disparities in access to care. For instance, research on Maryland’s HCBS programme demonstrated HCBS programmes facilitate statewide economic growth as well as contribute to improved independent living skills and higher quality of life for those with autism and their families. Similarly, the Leslie, Iskandarani, Velott, et al., (2017) and Leslie, Iskandarani, Dick, et al., (2017) built on this knowledge base looking at HCBS waiver services across 35 different states. These studies found increases to HCBS waiver services were associated with decreases in unmet healthcare needs of children with ASD and they reduced the likelihood that parents of those with disabilities would need to stop working to care for their child. Despite different programming across states, these findings remained consistent. Further, Shattuck et al. (2009) found that increasing Medicaid HCBS waivers for children with ASD reduced racial disparities in accessing care. Finally, Mandell et al. (2012), found increasing specific services covered through HCBS could decrease risk of psychiatric hospitalizations for those with ASD. The studies included in this scoping review demonstrate that HCBS programming for individuals with I/DD can improve equity and benefit the person with I/DD and their family, as well as the state as a whole, suggesting that Medicaid HCBS waivers as applied to people with I/DD are particularly effective.
Our findings must be interpreted in light of several limitations. First, our conclusions are limited by the scope of the research conducted to date. For instance, most of the studies focused on those with ASD as a diagnostic group rather than the larger community of those with I/DD. Autistic people are not representative of the entire I/DD community, yet most of the studies only include autistic people. Similarly, while using administrative data is a valuable tool for examining population-level effects, it can be unreliable and may not be able to measure all outcomes accurately. Second, scoping reviews do not formally evaluate the quality of evidence nor do they assess bias from different sources. Thus, this review represents a survey of the literature rather than an assessment of the relative quality and rigor of the included research. Finally, there was also a lack of information on causal pathways and modeling preventing an assessment of an unequivocal causal relationship between the policy change and effect on the community. That said, this scoping review provides useful information on a topic that has not been comprehensively reviewed and provides insight into future research directions. Through hand searching the literature, this scoping review provides a valid descriptive account of all available information in this area.
The implications of the findings of this scoping review are far-reaching in terms of identifying a knowledge base and determining areas for future research. Research on the economic and social impact of HCBS waivers is emerging and future research is needed to continue to make a case for these crucial services. Key findings of the seven studies in this review demonstrate that state-level Medicaid programmes are improving the lives of those with I/DD and their families. In many ways, HCBS waivers are working. Research that examines the differences between state HCBS waiver programmes, as well as draws international comparisons to similar programming, is now needed to determine which aspects of these programmes are working most efficiently and effectively, and for whom. Comparing characteristics of different state HCBS waiver programmes will help in determining the essential infrastructure needed for a successful HCBS programme. Furthermore, research looking specifically at the causal impact of Medicaid policy on specific outcomes such as independent living and deinstitutionalization is needed. Finally, policy research in general must expand to include outcomes for those with I/DD. As an example, do other social policies for housing, education, or healthcare improve the lives of those with I/DD as well?
This scoping review of Medicaid HCBS policy and I/DD is a strong starting point for researching and identifying the impacts of policy on the lives of those with I/DD. To date, most Medicaid policy research has analyzed the impact of the Medicaid expansion on outcomes for uninsured poor adults, pregnant women, and children. However, over 10 million people in the United States qualify for Medicaid on the basis of disability (MACPAC, 2018). Research on policies with the main intent to support people with disabilities is crucial for ensuring our current policies are appropriately addressing need and are functioning in the most beneficial, cost-effective way. This synthesis of Medicaid HCBS policy research demonstrates the ways in which several state Medicaid programmes are meeting some needs of children and adults with I/DD and identifies key gaps in knowledge that should be examined in future research.
Acknowledgements:
This study was supported by grants from the National Institute of Child Health and Human Development (U54HD090256) and the National Center for Advancing Translational Sciences (UL1TR002373; KL2TR002374; KL2TR000428).
Contributor Information
Kiley J. McLean, University of Wisconsin-Madison, School of Social Work & Waisman Center, 1350 University Ave, Madison, WI, 53706, USA.
Allison M. Hoekstra, University of Wisconsin-Madison School of Social Work & Waisman Center, Madison, WI, 53706, USA.
Lauren Bishop, University of Wisconsin-Madison School of Social Work & Waisman Center, Madison, WI, 53706, USA.
References
- Arksey H, & O’Malley L (2005). Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology, 8(1), 19–32. [Google Scholar]
- Baicker K, & Finkelstein A (2011). The effects of Medicaid coverage—learning from the Oregon experiment. The New England Journal of Medicine, 365(8), 683–685. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barton KN, & Gotto GS (2015). Economic impact of Missouri’s Partnership for Hope home and community-based Medicaid waiver for individuals with intellectual and developmental Disabilities. Journal of Disability Policy Studies, 27(3), 138–147. [Google Scholar]
- Bruen B, & Holahan J (2001). Medicaid Spending Growth Remained Modest in 1998, but Likely Headed Upward. Kaiser Commission on Medicaid and the Uninsured Issue Paper Retrieved from http://www.kff.org/medicaid/loader.cfm?url=/commonspot/security/getfile.cfm&pageId=13745
- Centers for Medicare & Medicaid Services (2019). Medicaid state waiver program demonstration projects: Medicaid waivers and demonstrations list. Retrieved from: http://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Waivers/Waivers.html.
- Cochrane. (2019). Cochrane Handbook for Systematic Reviews of Interventions. John Wiley & Sons. [Google Scholar]
- Eskow KG, Chasson GS, & Summers JA (2014). A cross-sectional cohort study of a large, statewide Medicaid home and community-based services autism waiver program. Journal of Autism and Developmental Disorders, 45(3), 626–635. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eskow K, Pineles L, & Summers JA (2011). Exploring the effect of autism waiver services on family outcomes. Journal of Policy and Practice in Intellectual Disabilities, 8(1), 28–35. [Google Scholar]
- Haber SG, Khatutsky G, & Mitchell JB (2000). Covering uninsured adults through Medicaid: Lessons from the Oregon health plan. Health Care Financing Review, 22(2), 1–17. [PMC free article] [PubMed] [Google Scholar]
- Hahn JE (2012). Minimizing health risks among older adults with intellectual and/or developmental disabilities: Clinical considerations to promote quality of life. Journal of Gerontological Nursing, 38(6), 11–17. [DOI] [PubMed] [Google Scholar]
- Howell EM (2001). The impact of the medicaid expansions for pregnant women: A synthesis of the evidence. Medical Care Research and Review, 58(1), 3–30. [DOI] [PubMed] [Google Scholar]
- Howell EM, & Kenney GM (2012). The impact of the Medicaid/CHIP expansions on children: A synthesis of the evidence. Medical Care Research and Review, 69(4), 372–396. [DOI] [PubMed] [Google Scholar]
- Kitchener M, Ng T, Miller N, & Harrington C (2005). Medicaid home and community-based services: National program trends. Health Affairs, 24(1), 206–212. [DOI] [PubMed] [Google Scholar]
- Lakin KC, Larson S, Salmi P, & Webster A (2010). Residential services for persons with developmental disabilities: Status and trends through 2009. University of Minnesota, Institute on Community Integration, Research and Training Center on Community Living. [Google Scholar]
- Leslie DL, Iskandarani K, Dick AW, Mandell DS, Yu H, Velott D, … Stein BD (2017a). The effects of medicaid home and community-based services waivers on unmet needs among children with autism spectrum disorder. Medical Care, 55(1), 57–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leslie DL, Iskandarani K, Velott DL, Stein BD, Mandell DS, Agbese E, & Dick AW (2017b). Medicaid waivers targeting children with autism spectrum disorder reduce the need for parents to stop working. Health Affairs (Millwood), 36(2), 282–288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Levac D, Colquhoun H, & O’Brien KK (2010). Scoping studies: Advancing the methodology. Implementation Science, 5, 69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mandell DS, Xie M, Morales KH, Lawer L, McCarthy M, & Marcus SC (2012). The interplay of outpatient services and psychiatric hospitalization among Medicaid-enrolled children with autism spectrum disorders. Archives Pediatrics and Adolescent Medicine, 166(1), 68–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marek KD, Popejoy L, Petroski G, Mehr D, Rantz M, & Lin WC (2005). Clinical outcomes of aging in place. Nursing Research, 54(3), 202–211. [DOI] [PubMed] [Google Scholar]
- Medicaid. (n.d.). Retrieved October 14, 2019, from https://www.medicaid.gov/medicaid/index.html.
- Medicaid and CHIP Payment and Access Commission (MACPAC) (U.S.). (2018). Report to the Congress on Medicaid and CHIP. Washington, DC: MACPAC, Medicaid and CHIP Payment and Access Commission. [Google Scholar]
- Moran M, Rein M, Goodin RE, & Etzioni A (2008). The unique methodology of policy research. In The Oxford Handbook of Public Policy. essay, : Oxford University Press. [Google Scholar]
- Shattuck PT, Grosse S, Parish S, Bier D (2009). Utilization of a Medicaid-funded intervention for children with autism. Psychiatric Services, 60(4), 549–552. [DOI] [PubMed] [Google Scholar]
- Shirk C (2006). Rebalancing Medicaid long-term services and supports. National Health Policy Forum. [Google Scholar]
- Wysocki A, Butler M, Kane RL, Kane RA, Shippee T, & Sainfort F (2015). Long-term services and supports for older adults: A review of home and community-based services versus institutional care. Journal of Aging & Social Policy, 27(3), 255–279. [DOI] [PubMed] [Google Scholar]
- Zablotsky B, Black LI, Maenner MJ, Schieve LA, Danielson ML, Bitsko RH, … Boyle CA (2019). Prevalence and trends of developmental disabilities among children in the United States: 2009–2017. Pediatrics, 144(4), e20190811. [DOI] [PMC free article] [PubMed] [Google Scholar]