

Abstract
We investigated the effects of parent warmth and behavioral control on externalizing and internalizing symptom trajectories from ages 8–14 in 1298 adolescents from 12 cultural groups. We did not find that single universal trajectories characterized adolescent externalizing and internalizing symptoms across cultures, but instead found significant heterogeneity in starting points and rates of change in both externalizing and internalizing symptoms across cultures. Some similarities did emerge. Across many cultural groups, internalizing symptoms decreased from ages 8–10, and externalizing symptoms increased from ages 10–14. Parental warmth appears to function similarly in many cultures as a protective factor that prevents the onset and growth of adolescent externalizing and internalizing symptoms, whereas the effects of behavioral control vary from culture to culture.
Internalizing problems (i.e., depression, anxiety, and social withdrawal; Pinquart, 2017a) and externalizing problems (i.e., aggression, noncompliance, rule-breaking, and impulsivity; Pinquart, 2017b) both begin to increase in their frequency and severity in adolescence (Collishaw, 2015). Mental health difficulties, including externalizing and internalizing problems, are the leading cause of disability in adolescence in every world region, contributing to 45% of adolescents’ overall disease burden and affecting 10–20% of the more than 1.2 billion adolescents in the world (Lancet Editorial, 2017). If untreated, externalizing and internalizing problems are likely to persist across ontogeny, generations, and cultures (Co-Author et al., 2018; Author et al., 2018; Author et al., 2017). Thus, identifying intervention targets that can ameliorate these problems is a priority for international health organizations (UNICEF, 2017).
Parenting behaviors are one such intervention target (Pinquart, 2017a; Pinquart, 2017b). Specifically, existing longitudinal work (e.g., Co-Author et al., 2018; McKee, Colletti, Rakow, Jones, & Forehand, 2008; Pinquart, 2017a, Pinquart, 2017b) has identified two types of parenting behaviors as especially effective in ameliorating externalizing and internalizing symptoms: parental warmth and parental behavioral control (McKee et al., 2008). Parental warmth (i.e., parents’ acceptance, caring, and positive support of children; McKee et al., 2008) and parental behavioral control (i.e., parents’ efforts to remain aware of, communicate clear and consistent expectations for, and redirect children’s behavior; Co-Author et al., 2018) have served as centerpieces for numerous parenting typologies that link parenting with child adjustment (McKee et al., 2008). However, a majority of existing work examines the effects of parent warmth and control on externalizing and internalizing behaviors almost exclusively in North American and European samples (Keilieng et al., 2011). Cross-cultural similarities or differences in a) the developmental courses of externalizing and internalizing problems throughout adolescence and b) the extent to which parent warmth and behavioral control alter such trajectories are not well known (AUTHOR et al., 2020). Yet, answering these questions is vital as international health organizations prioritize the development and large-scale deployment of parenting-based programs to prevent mental distress in adolescents worldwide (UNICEF, 2017).
Theory Guiding Investigation of Parenting Effects on Cross-Cultural Trajectories
Existing research examines cultural variability in externalizing and internalizing problems in cross-sectional fashion. In these cross-sectional studies, which encompass up to 44 cultures from all habitable continents, the effects of culture on adolescent externalizing and internalizing behaviors are larger in magnitude than those of other common demographic variables, including child gender or age (Rescorla et al., 2012; Rescorla et al., 2007a; Rescorla et al., 2007b). Moreover, investigators have noted that these cross-cultural differences in adolescent externalizing and internalizing behavior cannot be explained by common sociodemographic factors such as geographic region, ethnicity, religion, population, economic/political system, or collectivistic versus individualistic societal orientation (Rescorla et al., 2007a; Rescorla et al., 2007b) and that cross-cultural differences persist even after family socioeconomic status is controlled (Atilol, Balhara, Stenaovic, Avicenna, & Kandemir, 2013). This mystery of why cross-cultural differences in adolescent externalizing and internalizing problems persist has led cross-cultural researchers to advocate for two future directions in research.
First, researchers have called for longitudinal studies that investigate the developmental course of externalizing and internalizing problems (Atilol et al., 2013). It may be that cross-cultural differences in adolescent externalizing and internalizing behavior persist over time. Alternatively, it may be possible that cultural differences in cross-sectional work are an artifact of the cross-sectional methodology (Atilol et al., 2013), and that when examined across ontogeny cultural trajectories are relatively similar. Second, cross-cultural researchers have called for investigation of other hitherto unstudied factors that may account for these persistent cross-cultural differences, and suggest parenting practices as a great starting point (Atilol et al., 2013). The current study advances existing literature by answering both of these calls; it investigates trajectories of externalizing behavior and internalizing behavior in 12 cultural groups from 9 nations longitudinally from ages 8–14, and it investigates effects of parent warmth and control on these trajectories.
In considering how parenting may affect adolescent externalizing and internalizing trajectories, we were guided by the specificity principle of multicultural science (Bornstein, 2017). The specificity principle states that specific setting conditions at specific developmental time points can dictate ontological development (Bornstein, 2017). A conclusion drawn from this principle is that some parenting behaviors are likely to show cultural specificity in effects (i.e., parenting is more effective in some cultures than others in altering externalizing and internalizing trajectories) whereas others may show commonality across cultures (i.e., parenting alters externalizing and internalizing trajectories in similar ways across cultures; Bornstein, 2017). Existing theoretical frameworks posit that parent behavioral control may show specificity in effects across cultures, whereas parent warmth may show commonality in effects across cultures. Specifically, Interpersonal Acceptance-Rejection Theory (IPART; Rohner & COAUTHOR, 2017) posits that humans have developed a biologically-based need for warmth from their caregivers, and that consequently parent warmth may have universal protective effects on child development. In contrast, the specificity principle has led cross-cultural researchers to theorize that the effects of parent behavioral control may vary across culture because the extent to which parents are expected to relinquish control of their adolescents varies considerably across cultures (Lansford et al., 2017). Thus, the extent to which behavioral control is adaptive in preventing externalizing or internalizing behavior may depend on the cultural context.
In sum, the present study contributes to existing literature by examining the mystery surrounding persistent cultural differences in adolescent externalizing and internalizing symptoms with new longitudinal methods and a parenting focus that have been called for by cross-cultural researchers (Atilol et al., 2013). In investigating these questions, we invoke the specificity principle (for behavioral control) and IPART theory (for parent warmth) to understand the culturally-specific and common effects of parenting.
Worldwide Similarity in Adolescent Externalizing/Internalizing Trajectories
Existing literature is equivocal on the extent to which adolescents from different cultures are similar or different in their levels of externalizing and internalizing symptoms. Cross-sectional studies of both parent report (Rescorla et al., 2012; Rescorla et al., 2007a) and youth report (Rescorla et al., 2007b) of externalizing and internalizing symptoms in children ages 6–16 from 44 societies around found that effects of culture on adolescent externalizing and internalizing behaviors were larger in magnitude than those of other common demographic variables, including child gender or age. Moreover, depending on the study, between 29% and 39% of all cultures investigated fell 1 standard deviation below or above the overall mean on the Total Problems scale (which encompassed externalizing and internalizing symptoms; Rescorla et al., 2012; Rescorla et al., 2007a; Rescorla et al., 2007b). These pieces of cross-sectional evidence indicate meaningful cross-cultural differences in externalizing and internalizing symptoms.
This assertion is further supported by a smaller body of longitudinal work investigating externalizing trajectories across cultures. For instance, in an investigation of six longitudinal studies of child aggressive behavior across ages 7–13 in three nations (the United States, Canada, and New Zealand) initial levels of aggression and trajectories of change over time varied widely (Broidy et al., 2003). Similarly, in prior work with the present 12-culture sample, we utilized a multilevel modeling approach to identify that although child-reported externalizing behavior increased over ages 8–14, increase slowed over time and showed significant cross-cultural variability (Co-Author et al., 2018). However, due to the modeling framework used, we could not identify exactly how these trajectories varied in different cultures. Notably, no studies have investigated whether adolescent internalizing problems differ over time across cultures.
In contrast to this evidence for cultural differences in adolescent externalizing and internalizing symptoms, there is also evidence from the aforementioned cross-sectional studies that cultural difference in externalizing and internalizing behavior are ultimately small. For instance, although cultural effects were larger than those of gender and age, they were still characterized as small by researchers, and only explained anywhere between 3% and 14% of variance in total adolescent problems (Rescorla et al., 2012). The small magnitude of societal differences led researchers to conclude that externalizing and internalizing behavior scores were similar and consistent across societies (Rescorla et al., 2007a; Rescorla et al., 2007b).
These somewhat contradictory findings highlight the importance of investigating cross-cultural adolescent externalizing and internalizing trajectories longitudinally (Atilol et al., 2013). Cross-sectional cultural differences in adolescent externalizing and internalizing symptoms may be large enough and persistent enough over time that they lead to notable cultural-specific trajectories of these problems. Alternately, these cross-cultural differences might be negligible and it may be that adolescents around the world share one general trajectory of externalizing and internalizing symptoms. We attempt to evaluate these alternative hypotheses in the current study. Cross-cultural differences in adolescent externalizing and internalizing behavior that defy sociodemographic explanation may be attributable to parenting behaviors that share commonality across cultures (like parent warmth) or demonstrate specificity across cultures (like parent behavioral control; AUTHOR, 2018; Bornstein, 2017).
Culturally-Universal Protective Functions of Parent Warmth
Much existing theoretical work suggests that parent warmth might protect against the emergence and escalation of internalizing and externalizing symptoms in adolescence similarly in many different cultures (Rohner & Co-Author, 2017). From a theoretical perspective, Interpersonal Acceptance-Rejection Theory (IPART) posits that parental warmth has a universally positive effect on child adjustment (Rohner & Co-Author, 2017). According to IPART, people have developed an evolutionarily-adaptive, enduring biologically-based need for warmth from their caregivers, and therefore provision of warmth improves psychological adjustment in children around the world (Rohner & Co-Author, 2017).
Existing meta-analyses largely based on cross-sectional or two time-point longitudinal work appear to support this theoretical supposition. Specifically, meta-analyses collectively capturing the study of over 1 million children found that warmth predicted declines in subsequent externalizing and internalizing behavior in both cross-lagged models controlling for prior levels of externalizing and internalizing behavior, and in models that predicted effects on externalizing and internalizing behavior approximately 3 years later (Pinquart, 2017a; Pinquart, 2017b). Aligning with these meta-analytic findings, in our own prior longitudinal work utilizing the present 12-culture sample, we found that in all cultures, greater parent warmth demonstrated in one year predicted fewer child externalizing and internalizing behaviors the next year when children were ages 8–10, even after controlling for previous-year externalizing and internalizing behaviors (Co-Author et al., 2018). Notably, however, these year-over-year effects did not endure past age 10 (Co-Author et al., 2018).
Yet, existing cross-cultural work on the effects of warmth is largely cross-sectional in nature (Khaleque & Rohner, 2012). Therefore, existing evidence concerning the cross-cultural effects of warmth is limited and mixed. For instance, the Pinquart (2017a, b) meta-analyses found the largest correlations between warmth and externalizing/internalizing symptoms in older children, but our own longitudinal work found effects were largest prior to age 10 (Co-Author et al., 2018). Moreover, both of these studies only examined how warmth in one year predicted child externalizing or internalizing problems at another time point either one (Co-Author et al., 2018) or three (Pinquart, 2017a, b) years later. No work has examined how warmth predicts entire developmental trajectories of adolescent externalizing and internalizing behavior across cultures, and therefore no work captures the cumulative effects of parent warmth over time.
Culturally-Specific Functions of Parent Behavioral Control
In contrast to the posited culturally-generalizable effects of parent warmth, existing theoretical and empirical work indicates that the effects of parent behavioral control might be considerably more mixed across cultures (Co-Author et al., 2018). In line with the specificity principle (Bornstein, 2017), cross-cultural researchers have posited that the degree to which parents are expected to relinquish behavioral control and allow adolescents to develop autonomy from their families varies considerably, perhaps due to different cultural perceptions of children’s family obligations (Dwairy & Achoui, 2010; Lansford et al., 2016). Thus, whether the same level of behavioral control is adaptive or makes little difference in adolescent development might vary considerably depending on cultural context (Lansford et al., 2017).
This hypothesis appears to be supported by several lines of existing research. In a cross-sectional study of 2884 adolescents from 12 nations, greater parental control was associated with adolescent psychological disorders in Western (i.e., French and Argentine), but not Eastern (i.e., Arab and Indian) cultures (Dwairy & Achoui, 2010). The authors explained these differences by hypothesizing that parent control was more normative in Eastern cultures where family harmony was highly prized, and parents therefore exerted more control to maintain harmony (Dwairy & Achoui, 2010). Additionally, our own previous work with the current sample revealed that the effects of behavioral control on internalizing behaviors were only significant at age 9 (where higher behavioral control predicted greater child internalizing problems at age 10 in all cultures), but that behavioral control was not predictive of next-year internalizing behaviors at any other time point in any culture through age 13 (Co-Author et al., 2018). Crucially, however, both of these studies (including our own prior work) are either cross-sectional or only investigate associations between behavioral control and externalizing/internalizing behavior from one time point to the next. Therefore, they cannot reveal how continuous trajectories of externalizing and internalizing behavior are disrupted or enhanced by behavioral control as drives towards autonomy increase throughout adolescence across cultures.
The Importance of Studying the Transition to Adolescence
In sum, our study attempts to answer three major research questions. First, we ask whether trajectories of externalizing and internalizing behavior are the same or different across cultures. Second, we ask whether parent warmth has cross-culturally generalizable effects on these trajectories. Third, we ask whether behavioral control has culturally variable effects on these trajectories. These questions are critical to evaluate across the transition to adolescence.
The first trajectories question is critical to evaluate in adolescence because though prior work clearly indicates that externalizing and internalizing behaviors increase in adolescence (Collishaw, 2015; Rescorla, 2007), the exact nature of this growth over adolescence in different cultures is unknown. Adolescents across the world typically transition to new schools, begin to seek greater autonomy, and begin to experience profound neurobiological changes in the executive functioning and decision-making centers of the prefrontal cortex at approximately age 10 (Duell et al., 2018, Lee et al., 2014; Sorbring & Lansford, 2019) and each of these biological and school transitions can impact mental health (Lee et al., 2014). Therefore, leading international developmental organizations are increasingly calling for research that investigates shifts in mental health across this transition (at approximately age 10; UNICEF, 2017; Viner at al., 2012). Thus, moving beyond our previous work which only captured how externalizing/internalizing behavior in one year is associated with subsequent behavior in the next year (Coauthor et al., 2018), we now examine unfolding trajectories of internalizing and externalizing behaviors across ages 8–14, to capture changes during the adolescent transition.
The second and third questions regarding parent warmth and behavioral control are also critical to evaluate across the transition to adolescence because our own previous cross-cultural work with the present sample revealed that parent warmth and behavioral control experienced one year only prospectively predicted child externalizing and internalizing behaviors across cultures in preadolescence (i.e., prior to age 10), but not in adolescence (i.e., ages 10–13; Co-Author et al., 2018). These results raise questions about whether parenting “matters” across cultures once the transition to adolescence occurs. However our previous models could not determine whether there were lasting effects of parent warmth or behavioral control that extended beyond the next year. For instance, we could not test whether the effects of parent warmth were associated with growth or decline in externalizing problems experienced at ages 10–14. In the current study, we test these long-lasting effects across cultures by predicting changes in entire trajectories of externalizing and internalizing behavior across ages 8–14.
The Current Study
In sum, the current study builds on our existing work and contributes to existing literature by being the first study to evaluate whether early adolescent (i.e., age 8–14) trajectories of externalizing and internalizing problems vary across cultures. Additionally, our study also contributes to existing literature by addressing why cultural differences in externalizing and internalizing problems persist even after accounting for sociodemographic differences by investigating effects of parental warmth and parental behavioral control on cross-cultural trajectories. In so doing, we make two predictions. First, we hypothesize that parent warmth will protect against externalizing and internalizing problems across most cultures in the sample. Second, we hypothesize that the protective effects of behavioral control will be culturally-specific, and therefore less prevalent across cultures in the current sample.
Method
Participants
Participants included 1,298 children (M = 8.29 years, SD = .66, 51% girls), their mothers (N = 1,275, M = 36.93 years, SD = 6.27), and their fathers (N = 1,032, M = 39.96 years, SD = 6.52) at year 1 (age 8) of 6 annual years (ages 8–14). Families were recruited from 12 distinct ethnic/cultural groups across 9 countries including: Shanghai, China (n = 121); Medellín, Colombia (n = 108); Naples (n = 100) and Rome (n = 103), Italy; Zarqa, Jordan (n = 114); Kisumu, Kenya (n = 100); Manila, Philippines (n = 120); Trollhättan/Vänersborg, Sweden (n = 101); Chiang Mai, Thailand (n = 120); and Durham, NC, United States (n = 111 White, n = 103 Black, n = 97 Latino). Participants were recruited through public and private schools (to increase socioeconomic diversity and representativeness of the sample) in all nine countries. Response rates varied across countries (from 24% to nearly 100%), primarily because of differences in the schools’ roles in recruiting. For example, in China, once the schools agreed to participate, the parents did as well, and interviews were conducted at the schools, leading to participation rates of nearly 100%. In the United States, after schools agreed to help with recruitment, our interview team was allowed to leave letters explaining the study for teachers to send home with students. If parents were willing to have their family participate, they returned a letter to the school indicating their willingness to participate. Our team then contacted them directly to arrange an interview at a time and place that were convenient for the families.
Based on the number of letters we left at schools for teachers to distribute compared to the number of letters returned by parents, we estimated the response rate of 24%. Unfortunately, we are not able to estimate response rates for all sites because in some cases, there is no record of the number of students who were potentially invited to participate versus those who actually agreed to participate due to the differing ways in which schools informed parents about the study (e.g., paper letters, email contact, or verbal announcement). In addition, once families were invited to participate, they were enrolled in the study until we had reached the target sample size (based on our budget support). At that point, families were no longer enrolled, so we do not know how many families would eventually have said yes had we continued to enroll families.
Most parents lived together (82%) and were biological parents (97%); nonresidential and non-biological parents also provided data. Sampling included families from each country’s majority ethnic group, except in Kenya where we sampled Luo (13% of population), and in the U.S., where we sampled equal proportions of White, Black, and Latino families. SES and parental education were sampled in proportions representative of each recruitment area. Data for the present study were from the first six study years. In year six, 79% of the original sample provided data. Attrited participants did not demographically differ from the original sample.
Procedure
Measures were administered in the predominant language of each country, following forward- and back-translation. Interviews lasted 2 hours and were conducted after parent consent and child assent were given in participant-chosen locations. Participants were given the choice of completing the measures in writing or orally. Families were given modest monetary compensation for participating or compensated in other ways deemed appropriate by local IRBs.
Measures
Demographics.
Child gender and number of years of mother and father education at the beginning of the study were included in analyses as covariates.
Parental warmth and behavioral control.
When children were ages 8–10 and 12–13 mothers and fathers completed the Parental Acceptance-Rejection/Control Questionnaire-Short Form, a measure with excellent established reliability and convergent and discriminant validity, that has been used in over 60 cultures worldwide and has been used successfully with the cultural groups in the present study by our own and other research teams (Co-Author et al., 2018; Rohner, 2005). Using the Alignment Method (Asparouhov & Muthén, 2014) we found that both the parent warmth and behavioral control subscales of this measure used in the current study demonstrated measurement invariance across all cultures at all time points with two exceptions: Kenya and China. Specifically, parent warmth at ages 10 and 14 in Kenya and parent behavioral control at ages 8–10 and 14 in Kenya, and at age 8 in China demonstrated non-invariance. Overall, levels of non-invariance for both warmth (2.78%) and behavioral control (6.94%) fell below the 25% threshold indicating acceptable measurement invariance across groups (Muthén & Asparouhov, 2014). Children provided separate ratings about their mothers and fathers at ages 8–10, 12, and 14. Eight items captured parental warmth (e.g., “parents say nice things to child”), and 5 items captured behavioral control (e.g., “parents insist child do exactly as told”). Behavior frequency was rated on a modified 4-point scale (1 = almost never to 4 = every day). Aligning with our prior work (Co-Author et al., 2018), we calculated time-specific family means (i.e., average of all child and parent reports) of parental warmth and behavioral control. This decision was supported by significant correlations among parent and child reports of parental warmth (rs = .21–.70, p < .01) and control (rs = .18–.62, p < .01) at every time point, and by high degrees of internal consistency across reporters (αs = .84–.89) and within each of our 12 cultures (warmth αs = .74–.89; behavioral control αs = .66 – .89 with the exception of Kenya where internal consistency was α = .55; Supplemental Table 1). Given that adolescents with externalizing and internalizing problems provide parent reports that are negatively biased, and parents themselves often report parenting behaviors with a positive bias (Hou et al., 2019), our combined reporter measure attempted to mitigate both of these biases to provide a “middle ground” that captures family-wide perspectives on parenting. Higher scores indicated more warmth/control.
Child externalizing and internalizing problems.
Children completed the Youth Self Report Form of the Child Behavior Checklist (Achenbach & Rescorla, 2001) at ages 8–10, 12, and 14. Children were asked to rate how true each item was during the last six months (0 = not true, 1 = somewhat or sometimes true, 2 = very or often true). The Externalizing Behavior scale summed across 30 items and captured behaviors such as lying, truancy, vandalism, bullying, disobedience and physical violence. The Internalizing Behavior scale summed across 29 items and measured behaviors and emotions such as loneliness, self-consciousness, nervousness, sadness, and anxiety. The Achenbach measures are widely used in international research, with translations in over 100 languages and strong, well-documented psychometric properties (e.g., Achenbach & Rescorla, 2001). Although the Youth Self Report was originally designed to be completed by children ages 11–18 whose reading level is advanced enough to complete the measure alone, the items are comparable to items in parallel parent- and teacher-report versions of the measure appropriate for children as young as 6. Trained interviewers administered the measure orally in the initial years and recorded the children’s responses to avoid the concern about whether children would be able to read the items. Previous research also has demonstrated that children ages 7–10 years are able to make valid reports on the YSR (e.g., Ebesutani, Bernstein, Martinez, Chorpita, & Weisz, 2011). Both the externalizing and internalizing subscales demonstrated strong reliability over time (externalizing α = .79; internalizing α = .78) and across cultures (externalizing α = .70 – .96); internalizing α = .82 – .96; Supplemental Table 1) in the present sample, and have been successfully used in these cultures in prior work by our own and other research groups (e.g., Co-Author et al., 2018; Deater-Deckard et al., 2018; Rescorla et al., 2007). Higher scores indicated greater externalizing/internalizing problems.
Analysis Plan
We estimated a series of latent growth curve models to explore study objectives (Bollen & Curran, 2006; Curran et al., 2010). To begin, we estimated a series of unconditional latent growth curve (LGC) models to examine the nature of age 8–14 trajectories of externalizing and internalizing problems in all cultural groups. We compared four different functional forms of growth to determine which best captured changes in externalizing and internalizing problems over time. These included a) an intercept-only LGC model that allowed adolescents to vary in their externalizing or internalizing problems at age 8 (intercept), but not vary in rate of change in externalizing or internalizing problems over time (slope), b) a linear LGC model where adolescents were allowed to vary in their intercept and slope, and slope was assumed to be constant (linear) over time, c) a quadratic LGC model where adolescents were allowed to vary in their intercept and slope, and a quadratic term was estimated allowing slope to accelerate or decelerate over time, and d) a piecewise linear LGC model with a knot-point at age 10. In this piecewise linear model two different linear slopes were estimated; one capturing rate of change in externalizing or internalizing symptoms before age 10, and one doing so after age 10. We decided a priori to include this piecewise linear model in model comparisons because, as mentioned in the introduction, transitions in schooling, neurobiological development, and parenting that affect adolescent development each emerge at approximately age 10.
Following convention (Bollen & Curran, 2006), we tested fit among nested models with chi-square likelihood ratio tests, and the best fitting model was retained. Fit of quadratic and piecewise linear models were compared using Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC) indices, since these models were not nested (Bollen & Curran, 2006). The model with the lower AIC/BIC values, indicating better fit to the data, was selected. Additionally, the fit of all LGCs was evaluated according to recommended fit index cut-off values that indicate excellent fit (CFI/ TLI > 0.95, SRMR < .08; Kline, 2011).
Once our final culture-specific unconditional LGC models were estimated, we investigated our second and third study objectives by evaluating whether parental warmth and behavioral control predicted externalizing and internalizing trajectories in cultures around the world. We did so by iteratively estimating a series of conditional LGC models. First, we estimated whether demographic covariates (adolescent gender, mother/father years of education at age 8) predicted intercepts and slopes of externalizing and internalizing problems in each of our 12 cultural groups. Covariate effects significant at p < .05 were retained, non-significant effects were trimmed to ensure model parsimony. Then, parental warmth and parental behavioral control were entered into LGC models to determine if either of these parenting predictors altered adolescent trajectories even after controlling for study covariates. For all LGC models, parental warmth and behavioral control at age 8 predicted adolescent externalizing or internalizing behavior at age 8 (i.e., the intercept). For LGC models that included linear or quadratic slopes, average parental warmth and behavioral control across ages 8–14 predicted slopes over age 8–14. For LGC models that included a piecewise slope with an age 10 knot-point, average parental warmth and behavioral control from ages 8–10 were used to predict the 8–10 slope, and average parental warmth and behavioral control from ages 10–14 were used to predict the 10–14 slope.
Results
We first chronicle our efforts to model single culturally-generalizable trajectories of externalizing and internalizing problems. Then, we discuss culture-specific findings. Means/standard deviations of all variables can be found in Table 1.
Table 1.
Descriptive Statistics for Substantive Measures by Cultural Group
| Age | Whole Sample | U.S. White | U.S. Black | U.S. Latino | China | Italy/Naples | Italy/Rome | Kenya | Philippines | Thailand | Sweden | Colombia | Jordan | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | M | SD | M | SD | M | SD | M | SD | M | SD | M | SD | M | SD | M | SD | M | SD | M | SD | |
| Parental Warmth | ||||||||||||||||||||||||||
| 8 | 3.57 | 0.36 | 3.81 | 0.20 | 3.76 | 0.28 | 3.72 | 0.29 | 3.21 | 0.30 | 3.61 | 0.29 | 3.58 | 0.30 | 3.25 | 0.42 | 3.66 | 0.29 | 3.35 | 0.40 | 3.69 | 0.29 | 3.78 | 0.20 | 3.53 | 0.34 |
| 9 | 3.59 | 0.35 | 3.83 | 0.19 | 3.80 | 0.23 | 3.76 | 0.24 | 3.23 | 0.33 | 3.67 | 0.28 | 3.60 | 0.26 | 3.31 | 0.41 | 3.62 | 0.31 | 3.38 | 0.38 | 3.77 | 0.18 | 3.70 | 0.32 | 3.53 | 0.35 |
| 10 | 3.58 | 0.37 | 3.86 | 0.15 | 3.78 | 0.21 | 3.74 | 0.25 | 3.24 | 0.36 | 3.67 | 0.23 | 3.57 | 0.30 | 3.02 | 0.38 | 3.60 | 0.31 | 3.40 | 0.37 | 3.80 | 0.18 | 3.79 | 0.22 | 3.53 | 0.33 |
| 12 | 3.56 | 0.38 | 3.79 | 0.20 | 3.70 | 0.29 | 3.70 | 0.31 | 3.25 | 0.38 | 3.60 | 0.32 | 3.44 | 0.37 | 3.68 | 0.25 | 3.58 | 0.31 | 3.27 | 0.44 | 3.73 | 0.24 | 3.65 | 0.40 | 3.40 | 0.40 |
| 13 | 3.61 | 0.39 | 3.72 | 0.29 | 3.76 | 0.34 | 3.74 | 0.29 | 3.25 | 0.41 | 3.71 | 0.29 | 3.53 | 0.38 | 3.60 | 0.42 | 3.66 | 0.32 | 3.40 | 0.46 | 3.74 | 0.24 | 3.71 | 0.31 | 3.44 | 0.49 |
| 14 | 3.37 | 0.56 | 3.51 | 0.55 | 3.47 | 0.57 | 3.49 | 0.53 | 3.15 | 0.53 | 3.40 | 0.53 | 3.24 | 0.53 | 3.61 | 0.46 | 3.30 | 0.57 | 3.16 | 0.58 | 3.53 | 0.39 | 3.25 | 0.73 | 3.30 | 0.54 |
| Parental Behavioral Control | ||||||||||||||||||||||||||
| 8 | 2.98 | 0.41 | 2.88 | 0.36 | 3.21 | 0.38 | 3.21 | 0.30 | 2.51 | 0.26 | 3.15 | 0.36 | 3.09 | 0.38 | 3.25 | 0.27 | 3.00 | 0.32 | 2.71 | 0.29 | 2.73 | 0.43 | 3.29 | 0.31 | 2.81 | 0.34 |
| 9 | 2.94 | 0.42 | 2.84 | 0.40 | 3.17 | 0.39 | 3.16 | 0.34 | 2.60 | 0.29 | 3.12 | 0.38 | 3.08 | 0.37 | 3.10 | 0.33 | 2.92 | 0.30 | 2.72 | 0.30 | 2.65 | 0.41 | 3.31 | 0.35 | 2.76 | 0.34 |
| 10 | 2.88 | 0.41 | 2.82 | 0.40 | 3.11 | 0.370 | 3.06 | 0.38 | 2.55 | 0.27 | 3.17 | 0.34 | 3.09 | 0.37 | 2.72 | 0.29 | 2.92 | 0.30 | 2.67 | 0.30 | 2.55 | 0.40 | 3.26 | 0.30 | 2.75 | 0.35 |
| 12 | 2.85 | 0.44 | 2.65 | 0.41 | 3.01 | 0.35 | 3.02 | 0.31 | 2.51 | 0.27 | 3.09 | 0.36 | 2.96 | 0.35 | 3.31 | 0.35 | 2.84 | 0.34 | 2.55 | 0.33 | 2.45 | 0.45 | 3.10 | 0.35 | 2.73 | 0.31 |
| 13 | 2.82 | 0.51 | 2.53 | 0.42 | 2.97 | 0.52 | 2.98 | 0.43 | 2.52 | 0.31 | 3.10 | 0.40 | 2.97 | 0.47 | 3.23 | 0.44 | 2.81 | 0.46 | 2.60 | 0.42 | 2.23 | 0.45 | 3.14 | 0.46 | 2.70 | 0.37 |
| 14 | 2.82 | 0.52 | 2.63 | 0.55 | 2.92 | 0.47 | 2.96 | 0.39 | 2.51 | 0.42 | 3.07 | 0.47 | 2.90 | 0.43 | 3.23 | 0.48 | 2.83 | 0.45 | 2.50 | 0.44 | 2.53 | 0.62 | 2.99 | 0.47 | 2.77 | 0.42 |
| Child Externalizing Problems | ||||||||||||||||||||||||||
| 8 | 9.19 | 6.50 | 8.46 | 5.16 | 9.03 | 7.77 | 8.01 | 6.21 | 7.13 | 5.04 | 10.63 | 7.09 | 9.26 | 5.34 | 6.71 | 4.63 | 10.86 | 7.36 | 9.31 | 7.10 | 8.26 | 5.27 | 10.34 | 7.57 | 11.88 | 6.41 |
| 9 | 9.64 | 7.15 | 8.47 | 5.82 | 8.19 | 7.50 | 7.24 | 6.16 | 6.43 | 5.74 | 10.77 | 6.66 | 10.41 | 7.25 | 8.48 | 7.15 | 11.63 | 8.27 | 10.26 | 7.31 | 8.14 | 6.00 | 11.92 | 6.84 | 12.61 | 7.59 |
| 10 | 9.02 | 6.50 | 8.47 | 5.96 | 8.40 | 6.62 | 6.79 | 7.28 | 6.19 | 4.91 | 9.33 | 5.54 | 9.29 | 5.94 | 9.20 | 5.09 | 12.40 | 7.96 | 10.74 | 6.74 | 7.06 | 4.61 | 7.32 | 4.97 | 12.05 | 7.81 |
| 12 | 10.19 | 7.17 | 10.66 | 6.22 | 10.11 | 8.65 | 8.26 | 6.45 | 5.68 | 4.97 | 9.71 | 5.85 | 10.99 | 6.74 | 7.87 | 7.02 | 12.41 | 6.67 | 11.71 | 7.99 | 9.18 | 4.95 | 10.46 | 6.97 | 13.72 | 8.55 |
| 14 | 11.31 | 7.41 | 12.09 | 7.61 | 9.34 | 7.91 | 8.97 | 6.73 | 5.77 | 4.30 | 11.62 | 6.39 | 12.47 | 7.01 | 6.83 | 4.81 | 13.24 | 6.85 | 13.51 | 7.78 | 10.66 | 5.88 | 13.37 | 8.56 | 13.56 | 8.19 |
| Child Internalizing Problems | ||||||||||||||||||||||||||
| 8 | 14.7 | 8.39 | 14.56 | 6.89 | 15.21 | 9.04 | 15.68 | 8.33 | 11.28 | 6.53 | 16.07 | 7.82 | 14.37 | 8.31 | 9.18 | 6.40 | 18.93 | 8.12 | 13.89 | 8.11 | 13.26 | 8.31 | 19.26 | 9.67 | 13.90 | 7.73 |
| 9 | 13.3 | 8.57 | 14.30 | 8.36 | 12.55 | 8.93 | 13.22 | 8.93 | 9.43 | 8.04 | 14.23 | 7.67 | 14.31 | 8.78 | 6.94 | 5.67 | 18.43 | 8.38 | 15.26 | 7.86 | 10.27 | 7.56 | 16.98 | 8.05 | 12.83 | 7.93 |
| 10 | 11.7 | 7.79 | 12.21 | 7.61 | 11.03 | 7.64 | 11.01 | 8.77 | 8.89 | 7.47 | 12.36 | 6.88 | 11.69 | 7.57 | 7.71 | 3.36 | 18.84 | 8.01 | 14.95 | 8.38 | 9.12 | 6.57 | 10.76 | 6.71 | 11.71 | 7.23 |
| 12 | 12.9 | 8.65 | 13.29 | 9.52 | 12.12 | 8.97 | 9.07 | 6.84 | 7.61 | 7.11 | 13.42 | 8.41 | 13.37 | 7.83 | 13.70 | 8.86 | 18.57 | 9.10 | 14.77 | 8.33 | 8.96 | 6.31 | 14.22 | 8.65 | 13.84 | 7.80 |
| 14 | 14.43 | 9.49 | 16.25 | 11.21 | 12.24 | 10.05 | 11.64 | 8.33 | 10.55 | 7.26 | 15.98 | 9.83 | 15.12 | 8.92 | 13.92 | 6.81 | 18.29 | 8.39 | 15.94 | 9.17 | 11.25 | 8.01 | 17.69 | 11.78 | 12.22 | 8.71 |
Note: Bolded and highlighted values differed significantly from the overall sample mean at that particular time point at p<.05. Significantly higher parent warmth and behavioral control, and significantly lower externalizing and internalizing problems compared to the overall sample mean are highlighted in green. Significantly lower parent warmth and behavioral control, and significantly higher externalizing and internalizing problems compared to the sample as a whole are highlighted in red.
Do Generalizable Trajectories of Externalizing and Internalizing Problems Exist?
Initially, we tested whether just one culturally-generalizable externalizing and one culturally-generalizable internalizing trajectory existed. We estimated a single-group, unconditional latent growth curve model to estimate average sample-wide externalizing and internalizing problems trajectories (ignoring cultural membership; Bollen & Curran, 2006). We found that a piecewise linear model with an age 10 knot point best characterized both externalizing and internalizing problems across our entire sample. Next we estimated a multiple group unconditional latent growth curve model to examine whether this piecewise model represented the optimal form of growth for all 12 cultures (Bollen & Curran, 2006). Notifications of model misfit indicated that in at least 1/3rd of the cultures, the piecewise linear model did not represent the optimally-fitting model. Therefore we proceeded to estimate separate cultural models (Bollen & Curran, 2006). These analyses answered our first study question: Neither adolescent externalizing or internalizing behaviors follow the same trajectory across all cultures.
What Do Culture-Specific Externalizing/Internalizing Trajectories Look Like?
We next sought to examine the nature of adolescent externalizing and internalizing problem trajectories in each culture by identifying the optimal functional form of growth that characterized a culture’s average trajectory. Given the large number of findings, we summarize the most important findings here, but depict all trajectories in Figure 1 and present findings in full (intercepts, slopes, parenting predictors, and model fit indices) in Tables 2 and 3. An alternative results section that describes results by culture is included in the Supplemental Materials (Supplemental Results Section) for interested readers. Most models fit the data well according to omnibus measures of model fit; exceptions are noted below.
Figure 1.
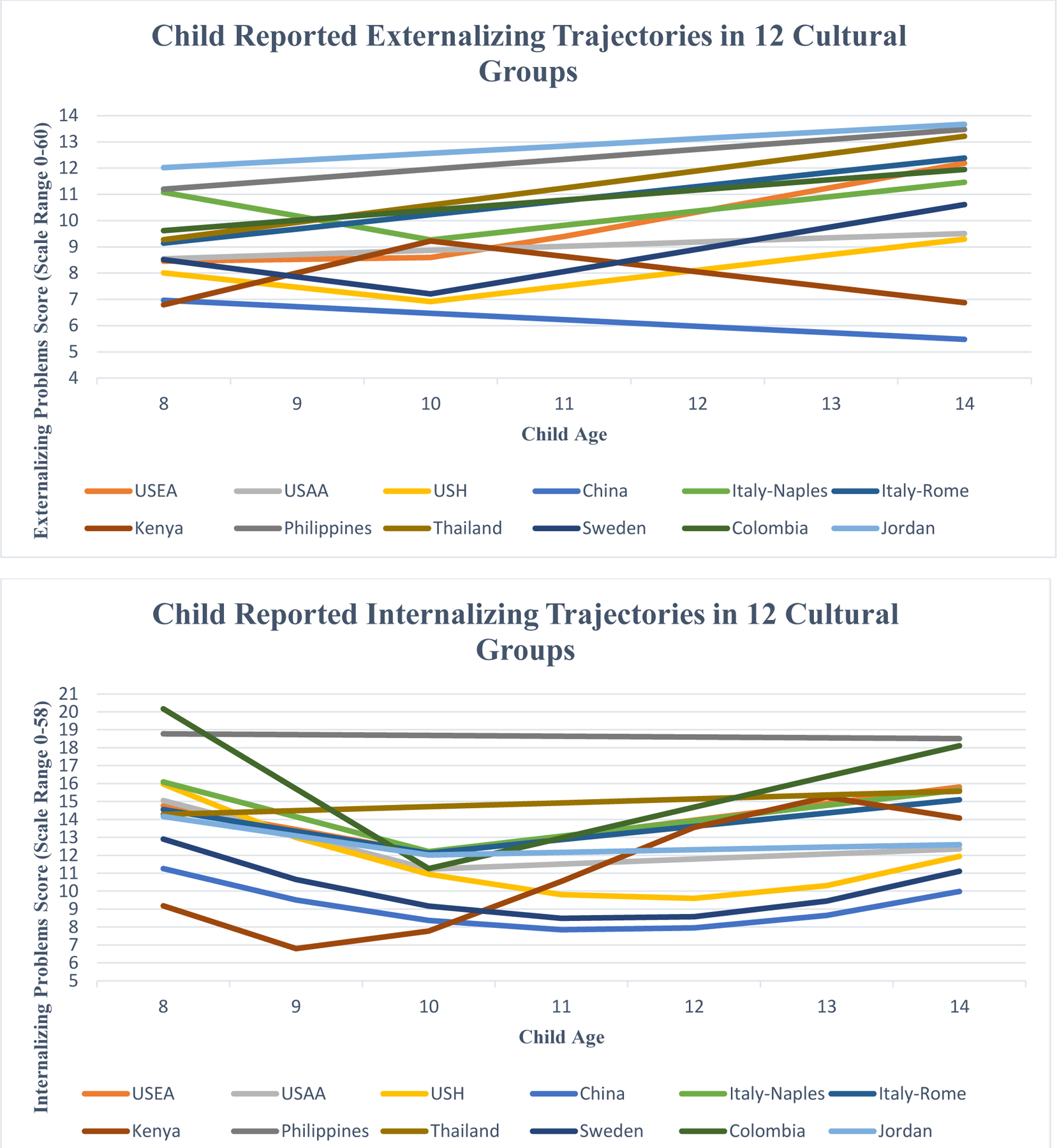
Two depictions of estimated latent growth curve model trajectories of child externalizing (top graph) and internalizing (bottom graph) problems in 12 cultural groups. USEA = U.S. White, USAA = U.S. Black, USH = U.S. Latino
Table 2.
Predicting Latent Growth Curve Trajectories of Child-Reported Externalizing Behavior By Culture
| Cultural Group | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| U.S. White | U.S. Black | U.S. Latino | China | Italy/Naples | Italy/Rome | Kenya | Philippines | Thailand | Sweden | Colombia | Jordan | |||||||||||||
| B | SE | B | SE | B | SE | B | SE | B | SE | B | SE | B | SE | B | SE | B | SE | B | SE | B | SE | B | SE | |
| Intercept | ||||||||||||||||||||||||
| Intercept | 8.46* | 0.49 | 8.55* | 0.70 | 8.01* | 0.61 | 6.97* | 0.43 | 11.08* | 0.67 | 9.14* | 0.49 | 6.79* | 0.45 | 11.20* | 0.67 | 9.28* | 0.53 | 8.52* | 0.51 | N/A | N/A | 12.02* | 0.55 |
| Predictors of Intercept | ||||||||||||||||||||||||
| Parental1 Warmth | 0.22 | 2.34 | −5.30^ | 2.23 | −5.73* | 1.94 | 1.04 | 1.21 | −1.55 | 2.18 | −3.20^ | 1.59 | −0.62 | 1.10 | −6.69* | 2.09 | −1.59 | 1.24 | 1.06 | 1.69 | N/A | N/A | −1.88 | 1.49 |
| Parental Control1 | 1.77 | 1.30 | 0.05 | 1.57 | 3.39 | 1.75 | 1.40 | 1.33 | 1.55 | 1.62 | 1.33 | 1.27 | −2.54 | 1.39 | 0.89 | 1.72 | 5.35* | 1.67 | 0.58 | 1.10 | N/A | N/A | 0.69 | 1.48 |
| Linear Slope | ||||||||||||||||||||||||
| Linear Slope | .075 | 0.26 | 0.16 | 0.16 | −0.555 | 0.40 | −0.24^ | 0.11 | −0.915* | 0.31 | 0.54* | 0.12 | 1.225* | 0.30 | 0.38* | 0.13 | 0.66* | 0.15 | −0.655* | 0.22 | N/A | N/A | 0.28^ | 0.14 |
| Predictors of Linear Slope | ||||||||||||||||||||||||
| Parental Warmth | −0.013 | 1.75 | −2.202* | 0.69 | −0.243 | 1.74 | −0.872^ | 0.40 | 1.063 | 1.32 | −0.882 | 0.46 | 1.153 | 1.16 | −0.312 | 0.48 | −1.062^ | 0.44 | −2.893* | 1.04 | N/A | N/A | −2.132* | 0.43 |
| Parental Control | 0.543 | 0.79 | −0.132 | 0.49 | 1.253 | 1.17 | 0.532 | 0.44 | 0.163 | 0.94 | 0.142 | 0.39 | −1.543 | 1.46 | 0.402 | 0.50 | 0.132 | 0.58 | 1.083^ | 0.56 | N/A | N/A | 1.562* | 0.57 |
| Piecewise Linear Slope | ||||||||||||||||||||||||
| Piecewise Linear Slope | 0.936* | 0.20 | N/A | N/A | 0.606* | 0.22 | N/A | N/A | .556* | .17 | N/A | N/A | −.596* | .18 | N/A | N/A | N/A | N/A | 0.856* | .17 | N/A | N/A | N/A | N/A |
| Predictors of Piecewise Linear Slope | ||||||||||||||||||||||||
| Parental Warmth | −1.724* | 0.70 | N/A | N/A | −0.314 | 0.70 | N/A | N/A | −0.854 | 0.55 | N/A | N/A | −0.814 | 0.52 | N/A | N/A | N/A | N/A | −1.434* | 0.63 | N/A | N/A | N/A | N/A |
| Parental Control | −0.844 | 0.46 | N/A | N/A | 0.004 | 0.61 | N/A | N/A | −0.304 | 0.48 | N/A | N/A | 0.074 | 0.43 | N/A | N/A | N/A | N/A | 0.354 | 0.32 | N/A | N/A | N/A | N/A |
| Omnibus Measures of Model Fit for Growth Curves | ||||||||||||||||||||||||
| CFI | .99 | .95 | 1.0 | .96 | .98 | .93 | .98 | .97 | .94 | .94 | .34 | .97 | ||||||||||||
| TFI | .99 | .95 | 1.0 | .96 | .97 | .93 | .96 | .98 | .95 | .90 | .39 | .98 | ||||||||||||
| SRMR | .06 | .07 | .03 | .07 | .04 | .09 | .05 | .08 | .10 | .11 | .15 | .12 | ||||||||||||
p ≤ .05
p ≤ .01
Age 8 Parenting Behavior
Average Parent Behavior over Ages 8–14
Average Parent Behavior Over Ages 8–10
Average Parent Warmth Over Ages 11–14
Indicates Linear Slope from Ages 8 to 10
Indicates Linear Slope from Ages 10 to 14. CFI = Comparative Fit Index, TLI = Tucker-Lewis Index, SRMR = Standardized Root Mean Square Residual
Table 3.
Predicting Latent Growth Curve Trajectories of Child-Reported Internalizing Behavior By Culture
| Cultural Group | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| U.S. White | U.S. Black | U.S. Latino | China | Italy/Naples | Italy/Rome | Kenya | Philippines | Thailand | Sweden | Colombia | Jordan | |||||||||||||
| B | SE | B | SE | B | SE | B | SE | B | SE | B | SE | B | SE | B | SE | B | SE | B | SE | B | SE | B | SE | |
| Intercept | ||||||||||||||||||||||||
| Intercept | 14.76* | 0.67 | 15.05* | 0.89 | 15.98* | 0.84 | 11.26* | 0.59 | 16.10* | 0.74 | 14.56* | 0.79 | N/A | N/A | 18.77* | 0.69 | 14.28* | 0.61 | 12.90* | 0.79 | 20.17* | 0.92 | 14.17* | 0.70 |
| Predictors of Intercept | ||||||||||||||||||||||||
| Parental1 Warmth | −4.04 | 3.11 | −5.48 | 3.06 | −8.67* | 2.40 | 0.27 | 1.65 | −2.90 | 2.46 | −3.19 | 2.15 | N/A | N/A | −6.78* | 2.09 | −2.50 | 1.49 | 3.57 | 2.16 | −8.78* | 3.36 | −1.61 | 1.54 |
| Parental Control1 | 2.08 | 1.73 | 2.09 | 2.09 | 4.38^ | 2.13 | 1.71 | 1.91 | 1.43 | 1.78 | 1.91 | 1.81 | N/A | N/A | −0.29 | 1.77 | 7.47* | 1.87 | 0.84 | 1.38 | 0.40 | 2.07 | 1.59 | 1.47 |
| Linear Slope | ||||||||||||||||||||||||
| Linear Slope | −1.335* | 0.39 | −1.915* | 0.41 | −3.44* | 0.49 | −2.06* | 0.43 | −1.945* | 0.43 | −1.225* | 0.43 | N/A | N/A | −0.04 | 0.18 | 0.22 | 0.17 | −2.65* | 0.46 | −4.455* | 0.39 | −1.085* | 0.40 |
| Predictors of Linear Slope | ||||||||||||||||||||||||
| Parental Warmth | −1.023 | 2.43 | −0.373 | 2.33 | −0.162 | 2.20 | −3.212^ | 1.56 | −0.163 | 1.74 | −0.213 | 1.67 | N/A | N/A | −0.512 | 0.64 | −1.462* | 0.49 | −6.312* | 2.14 | 3.733* | 1.43 | −0.213 | 1.08 |
| Parental Control | −0.443 | 1.12 | −0.283 | 1.21 | 0.752 | 1.72 | 2.482 | 1.94 | −1.253 | 1.26 | −0.823 | 1.23 | N/A | N/A | 0.172 | 0.67 | −0.452 | 0.64 | 1.312 | 1.02 | 1.113 | 1.18 | 0.553 | 1.06 |
| Piecewise Linear or Quadratic Slope | ||||||||||||||||||||||||
| Piecewise Linear or Quadratic Slope | 0.936* | 0.30 | 0.286 | 0.27 | 0.467* | 0.08 | 0.317* | 0.08 | 0.866* | 0.27 | 0.746* | 0.21 | N/A | N/A | N/A | N/A | N/A | N/A | 0.397* | .07 | 1.716* | 0.33 | 0.156 | 0.26 |
| Predictors of Piecewise or Quadratic Linear Slope | ||||||||||||||||||||||||
| Parental Warmth | −2.954* | 0.86 | −1.844^ | 0.82 | −0.132 | 0.35 | 0.25 | 0.31 | −1.514^ | 0.79 | −1.014 | 0.55 | N/A | N/A | N/A | N/A | N/A | N/A | 0.602 | 0.36 | −1.584^ | 0.70 | −2.164* | 0.52 |
| Parental Control | −2.244* | 0.60 | −0.14 | 0.69 | 0.022 | 0.30 | −0.37 | 0.38 | 0.284 | 0.70 | 0.12 | 0.50 | N/A | N/A | N/A | N/A | N/A | N/A | −0.222 | 0.17 | 0.43 | 0.75 | 1.584^ | 0.68 |
| Omnibus Measures of Model Fit for Growth Curves | ||||||||||||||||||||||||
| CFI | .96 | 1.0 | .94 | 1.0 | 1.0 | .96 | .00 | .99 | .96 | .95 | .96 | .96 | ||||||||||||
| TLI | .94 | 1.0 | .90 | 1.0 | 1.0 | .93 | −5.2 | .99 | .96 | .92 | .94 | .91 | ||||||||||||
| SRMR | .04 | .03 | .08 | .05 | .04 | .08 | .14 | .08 | .07 | .10 | .05 | .08 | ||||||||||||
p ≤ .05
p ≤ .01
Age 8 Parenting Behavior
Average Parent Behavior over Ages 8–14
Average Parent Behavior Over Ages 8–10
Average Parent Warmth Over Ages 11–14
Indicates Linear Slope from Ages 8 to 10
Indicates Linear Slope from Ages 10 to 14
Indicates Quadratic Slope. CFI = Comparative Fit Index, TLI = Tucker-Lewis Index, SRMR = Standardized Root Mean Square Residual
Externalizing trajectories.
Notable variability in starting point (age 8) and rate of change (ages 8–14) in externalizing problems emerged across cultures (Figure 1). Estimated age 8 externalizing problems scores ranged from 6.97 (Kenya) to 12.02 (Jordan) across cultures. Put practically, across cultures, 8-year olds, on average, endorsed experiencing between 7 and 12 externalizing problems at a moderate level, or between 3.5 and 6 externalizing problems at a severe level, or a mix of symptoms at severe and moderate level. There also appears to be pronounced cultural variability in the forms of rates of change over time in adolescent-reported externalizing behaviors. Specifically, externalizing trajectories were characterized by three patterns: stability, linear, and piecewise linear change.
Only the U.S. Black sample showed stability. In this sample, slope terms were non-significant, meaning that U.S. Black adolescent reports of externalizing behavior over ages 8–14 did not significantly change from their initial age 8 levels (where estimated externalizing scores were a “middle-of-the-pack” 8.55).
Five cultures demonstrated linear trajectories (China, Italy/Rome, Jordan, Philippines, and Thailand). In all of these cultures except for China, linear slopes were positive, meaning that externalizing problem scores reported by adolescents increased at a constant rate with each passing year from ages 8–14 (ranging between 0.28–0.54 points/yr across cultures; Table 2). In China, externalizing problems decreased each year (at 0.24 points/yr).
Finally, five cultures demonstrated piecewise linear trajectories (Italy/Naples, Kenya, Sweden, U.S. White, U.S. Latino). In U.S. White and U.S. Latino samples, there was no significant change in scores between ages 8–10, but then externalizing scores increased at a constant rate with each passing year from ages 10–14 (Table 2). In Italy/Naples and Sweden, externalizing scores decreased with each passing year at a constant rate from ages 8–10, before increasing at a constant rate with each passing year from ages 10–14. In Kenya, externalizing scores increased between ages 8–10, before decreasing between ages 10–14 (Table 2).
The Colombian externalizing trajectory never achieved appropriate levels of model fit according to omnibus fit statistics (see Table 2). Therefore, we refrain from interpreting the Colombian externalizing model further. In sum, cultures varied to a wide extent in both externalizing behaviors at age 8, and in the manner in which externalizing behaviors developed over adolescence. However, one notable pattern of similarity emerged across most cultures. Specifically, in 8 of the 11 cultural groups where trajectories could be estimated (all but the China, Kenya, and U.S. Black samples), adolescent-reported externalizing symptoms significantly increased in the early adolescent time period (i.e., ages 10–14).
Internalizing trajectories.
Similar to adolescent externalizing trajectories, variability in starting point (age 8) and rates of change (ages 8–14) in internalizing problems trajectories emerged across cultures (Figure 1). For instance, estimated age 8 internalizing scores ranged from 11.26 (China) to 20.17 (Colombia) across cultures. Practically speaking, 8-year-olds, on average, endorsed experiencing between 11 and 20 internalizing problems at a moderate level or 5.5 and 10 internalizing problems at a severe level across cultures. There was also pronounced cultural variability in the forms of adolescent-reported internalizing trajectories. Trajectories were characterized by three patterns: stability, piecewise linear, and quadratic growth.
Only the Filipino and Thai samples showed stability. In these samples, slope terms were non-significant, meaning that Filipino and Thai adolescent internalizing behaviors over ages 8–14 did not significantly change from their initial age 8 levels (where Filipino estimated internalizing scores were a higher-than-average 18.77 and Thai estimated internalizing scores were a middle-of-the-pack 14.28; Table 3).
Six cultures had piecewise linear trajectories (Colombia, Italy/Naples, Italy/Rome, Jordan, U.S. White, U.S. Black). In all six cultures, adolescent-reported internalizing scores dropped with each passing year from ages 8–10 (Table 3). In two of the six cultures (Jordan and U.S. Black), subsequent slope terms across ages 10–14 were not significant (Table 3), indicating that internalizing scores across ages 10–14 remained stable, and did not differ significantly from their age 10 levels. In the other four cultures (Colombia, Italy/Naples, Italy/Rome, U.S. White) slope terms across ages 10–14 were significant and positive, meaning that adolescent-reported internalizing problems increased at a constant rate with each passing year (Table 3).
Three cultures had quadratic growth trajectories (China, Sweden, and U.S. Latino). In each of these cultures, adolescents’ internalizing scores decreased each year over ages 8–14, but the rate of this decrease was not constant over time. Specifically, in all three cultures, the decrease in adolescents’ internalizing scores slowed over time to the point that, in all three cultures, estimated internalizing scores began to increase again after approximately age 12 (though they never returned to their initial age 8 levels; Table 3).
Additionally, like the Colombian externalizing trajectory, the Kenyan internalizing trajectory never achieved appropriate levels of model fit according to omnibus fit statistics. Therefore, we refrain from interpreting the Kenyan internalizing model further.
To summarize, as with externalizing behaviors, cultures varied widely in both internalizing behaviors at the start of adolescence, and in the manner in which internalizing behaviors unfolded. Yet, one notable pattern of similarities did emerge. In 9 of 11 cultural groups with estimated trajectories, child internalizing symptoms decreased between ages 8–10 (Table 3).
Association of Parent Warmth with Externalizing/Internalizing Trajectories
Next we examined the association of parental warmth and behavioral control with adolescent trajectories of externalizing and internalizing problems. Due to space constraints, and the fact that significant covariate effects were few and not systematic in nature, covariate effects are not reported here but are available upon request. All reported significant warmth and behavioral control effects were found after controlling for significant covariates.
Parent warmth associations with externalizing trajectories.
In four cultures (Italy/Rome, the Philippines, U.S. Black, U.S. Latino) greater parent warmth predicted lower age 8 externalizing scores (Table 2). Additionally, warmth was associated with change in externalizing behavior over time across all three growth patterns observed in our sample (stability, linear, and piecewise linear growth).
In the U.S. Black sample that demonstrated stability in externalizing problems across ages 8 to 14, greater parent warmth from ages 8–14 was associated with fewer adolescent externalizing problems across ages 8–14 (Table 2). Additionally, warmth was a significant predictor of change over time in three of the five cultures that showed linear trajectories of adolescent externalizing problems across ages 8 to 14. Specifically, in China greater parent warmth across ages 8–14 was associated with a more rapid decline in adolescent externalizing problems across ages 8–14, and in Thailand and Jordan, greater parent warmth was associated with less growth in adolescent externalizing problems across ages 8–14 (Table 2).
Finally, warmth significantly predicted change over time in two of five cultures that demonstrated piecewise linear trajectories of adolescent externalizing problems across ages 8 to 14. In the Swedish sample, greater parent warmth from ages 8–10 was associated with a more rapid decline in adolescent externalizing behaviors across ages 8–10, and in both the Swedish and U.S. White sample, greater parent warmth across ages 10–14 was associated with less growth in adolescent externalizing symptoms across ages 10–14. In sum, parent warmth buffered against the emergence of or growth in adolescent externalizing problems at some point between ages 8–14 in 8 of 11 cultures (i.e., all but Italy/Naples, Italy/Rome, and Kenya; Table 2). Additionally, in 6 of 11 cultures (China, Jordan, Sweden, Thailand, U.S. White, U.S. Black), the buffering effects of warmth were maintained through age 14 (Table 2).
Parent warmth associations with internalizing trajectories.
In three cultures (Colombia, Philippines, and U.S. Latino), greater parent warmth predicted lower age 8 internalizing scores (Table 2). Additionally, warmth was associated with change in internalizing behavior over time across all three growth patterns observed in our sample (stability, piecewise linear, and quadratic).
In both the Filipino and Thai samples, which showed stability in internalizing problems across ages 8 to 14, greater parent warmth from ages 8–14 was associated with fewer adolescent internalizing problems across ages 8–14 (Table 3). Additionally, warmth was a significant predictor of change over time in four of the six cultures (Colombia, Italy/Naples, U.S. White, U.S. Black) that showed piecewise linear trajectories of adolescent internalizing problems across ages 8 to 14. Specifically, in all four of these cultures, greater parent warmth from ages 10–14 predicted less growth in adolescent internalizing problems across ages 10–14. Finally, warmth was also a significant predictor of change over time in two of three cultures (China, Sweden) that had quadratic trajectories of adolescent internalizing problems across ages 8 to 14. In these cultures, greater age 8–14 parent warmth predicted greater linear declines in age 8–14 adolescent internalizing symptoms. However, warmth did not significantly predict any changes in the quadratic portion of the slope (so decreases in internalizing problems in these cultures still slowed over time at the same rate with or without warmth included in the model).
Taken together, these results indicate that parent warmth protected against the emergence of or growth in adolescent internalizing problems at some point between ages 8–14 in 10 of 11 cultures (i.e., all but Italy/Rome; Table 3). Additionally, in 9 of 11 cultures (all but Italy/Rome and Philippines), the buffering effects of warmth were maintained through age 14 (Table 3).
Association of Parent Behavioral Control with Externalizing/Internalizing Trajectories
Parent behavioral control associations with externalizing trajectories.
Greater parent behavioral control predicted higher age 8 externalizing problems in only one culture (Thailand). Additionally, behavioral control was associated with change in externalizing problems over time in only two cultures (Table 2). In Sweden, greater behavioral control was associated with less decline in adolescent externalizing problems from ages 8–10. In Jordan, greater behavioral control was associated with larger growth in adolescent externalizing problems across ages 8–14.
Parent behavioral control associations with internalizing trajectories.
Greater parent behavioral control only predicted higher age 8 internalizing problems in two cultures (Thailand and U.S. Latino). Additionally, behavioral control was associated with change in internalizing behavior over time in only two cultures. In the U.S. White sample, greater behavioral control was associated with less growth in adolescent internalizing behavior from ages 10–14 (Table 3). In Jordan, greater behavioral control was associated with greater growth across ages 10–14.
Discussion
Similarity in Adolescent Externalizing/Internalizing Trajectories Across Cultures
We examined whether trajectories of externalizing and internalizing behavior were similar across 12 cultural groups. Our findings resolve discrepancies in existing literature by identifying that small but significant cross-cultural differences in adolescent externalizing and internalizing behaviors observed in cross-sectional literature appear to persist long enough over development that investigating culture-specific trajectories of externalizing and internalizing behavior is appropriate. Specifically, our findings do not support the notion that single universal trajectories define adolescent externalizing or internalizing problems. Some similarities in the development of adolescent externalizing and internalizing problems emerged across cultures, but so did numerous cross-cultural differences in patterns of growth.
Similarities and Differences in Adolescent Externalizing Trajectories Across Cultures
One major similarity in adolescent externalizing problem trajectories emerged across most cultures in our sample. Specifically, in 8 of 11 cultures that we investigated (all except China, Kenya, and U.S. Black), adolescent externalizing problems significantly increased each year from ages 10–14. Existing longitudinal literature demonstrates this phenomenon in Western cultural samples (Collishaw, 2015), and our findings support the notion that this effect generalizes when examining trajectories in other cultural groups. The cross-cultural nature of this phenomenon may arise because adolescents in many different cultures become more prone to take risks, which is associated with increased externalizing behaviors in many cultures (Steinberg et al., 2018). However, this single similarity in trajectories across cultures was complemented by numerous differences in externalizing trajectories across cultures.
First, in three cultures (China, Kenya, and U.S. Black) adolescent externalizing problems either remained stable or actually decreased by age 14. Several culture-specific contexts may account for why each of these cultures experienced no increase in externalizing problems through age 14. Fascinatingly, just as Kenyan adolescents in our sample turned age 10, Kenya passed a law outlawing parental corporal punishment. It may be that this law change spurred Kenyan parents to abandon corporal punishment and adopt more adaptive parenting behaviors (such as parent warmth) that prevented an increase in externalizing behaviors over ages 10–14 in Kenyan adolescents. Evidence for this effect emerges in Table 1, which indicates that Kenyan parents’ warmth was significantly higher than the overall sample average at ages 12 and 14, and Kenyan adolescents’ externalizing behaviors were also significantly below the sample average at these ages. A similar effect of warmth may have emerged in the U.S. Black sample, but due to cultural normativeness instead of a law change. Parents in our U.S. Black sample exhibited significantly above-average sample warmth at all ages (8–14; Table 1), and this warmth was associated with U.S. Black adolescents experiencing significantly fewer externalizing problems across ages 8–14 (Table 2). Thus, U.S. Black adolescents may not have shown increases in adolescent externalizing symptoms through age 14 because warmth served as a protective factor against these problems in this sample, and because U.S. Black parents provide this protective warmth much more frequently than average. Interestingly, the Chinese sample was below the sample average in both warmth and behavioral control (Table 3), so greater prevalence of such behaviors probably does not account for decreases in externalizing problems seen in China. However, Chinese culture does emphasize harmony with others, and aggressive acts in violation of these norms are perceived as extremely dishonorable (Dwairy & Achoui, 2010). Therefore, in China, externalizing symptoms may decrease over time as adolescents become increasingly aware of behavioral cultural norms, and regulate their behavior to avoid dishonor.
Second, in the eight cultures that do demonstrate significant increases in externalizing behavior through age 14, these increases appear to happen at different times. In four cultures (Italy/Rome, Jordan, Philippines, and Thailand), we found a constant increase in externalizing symptoms from ages 8–14, whereas in four other cultures (Italy/Naples, Sweden, U.S. White, and U.S. Latino), increases in externalizing behaviors began around age 10. Moreover, as can be seen in Tables 1–3, no discernable patterns concerning the effects of warmth or control appear to emerge in one of these sets of cultures compared to the other, so variability in parenting effects alone does not account for these differences. However, each of the cultural groups where externalizing symptoms increase starting after age 10 participated in Western educational systems, where the transition to middle school between ages 10–12 is especially drastic as adolescents change school settings, associate with new peers, and form new social networks (Sorbring & Lansford, 2019). Therefore, perhaps externalizing symptoms are especially likely to increase after age 10 because of the difficulty of the school transition itself and the increased likelihood of disruptions in peer relationships related to externalizing behaviors (Sheppard, Giletta, & Prinstein, 2019). This finding is speculative, however, and requires further study.
Similarities and Differences in Adolescent Internalizing Trajectories Across Cultures
One major similarity in adolescent internalizing problem trajectories emerged across most cultures in our sample. In 9 of 11 cultural groups (all except for Thailand and the Philippines), child self-reported internalizing symptoms decreased in the preadolescent period (ages 8–10). Internalizing trajectories within this developmental period are rarely studied, but some studies have found this decreasing effect (Wetter & El-Sheikh, 2012). Child social competence and emotional regulation begin to mature rapidly over ages 8–10 (Rooney et al., 2013). Adaptive maturation of these systems consistently protects against the emergence of internalizing problems. Moreover, at age 8–10, the adolescent school demands and peer stressors that lead to greater adolescent risk for internalizing symptoms might not be as prevalent (Rooney et al., 2013). Therefore, ages 8–10 may represent a “window” within which adaptive systems that protect against internalizing symptoms strengthen, while risk factors that precipitate internalizing symptoms generally do not increase, leading to decreases in average trajectories of internalizing symptoms. Yet, this cross-cultural similarity was complemented by numerous cultural differences in internalizing trajectories.
First, in two cultures (Thailand and Philippines), adolescent internalizing behaviors remained higher than average for the sample and stable across ages 8–14. In Thailand, these high stable internalizing symptoms may be best explained by the relatively fewer opportunities adolescents in this sample have to experience warmth. Specifically, we discovered that Thai parents expressed warmth towards their children less often compared to the overall sample mean at every time point from ages 8–14 (Table 1), perhaps because verbal expressions of warmth such as those captured by our warmth measure are less common-place in Thai culture than are other ways of expressing warmth, such as by preparing special foods for the child (Punyanunt-Carter, 2016). Consequently, it may be that Thai adolescents in our sample simply experience fewer of the verbal expressions of warmth that protect against internalizing problems than adolescents in other cultures, and therefore their internalizing behaviors are relatively high. In contrast, Filipino adolescents in our sample experience average levels of parent warmth and control (Table 3), but uncertainties and stress related to neighborhood contexts and low socioeconomic status may have led to increases in anxiety, sadness, and other internalizing behaviors (Alampay & Garcia, 2019).
In five other cultures, adolescents’ internalizing problems decreased between ages 8–10 and then remained stable (Jordan and U.S. Black samples; Figure 1; Table 3) or decreased over time before slightly increasing between ages 12–14 (but not returning to age 8 levels; China, Sweden, U.S. Latino). Interestingly, these five cultures were not distinguished by distinct parenting behavior profiles that all cultures shared, so it appears that contextual variables beyond parenting may account for these cultural trajectories. One such contextual variable may be the intersectionality between behavioral control and family obligations (i.e., the expectation that adolescents need to respect parental authority and be present with their family on a daily basis; COAUTHOR ET AL., 2016). The cultures evaluated here were either among the five highest (Jordan, U.S. Black, U.S. Latino) or three lowest (China and Sweden) in levels of adolescent self-reported family obligations in the present sample (COAUTHOR ET AL., 2016). Two of the cultures that were highest in family obligations also had significantly above-average levels of behavioral control (U.S. Black and U.S. Latino; Table 1), whereas both of the cultures that had the lowest levels of family obligations also had significantly below-average levels of parent behavioral control (China and Sweden; Table 1). Therefore, perhaps in cultures where adolescents are granted greater autonomy (because both family obligations and behavioral control are low, like in Sweden), fewer internalizing problems emerge over adolescence because parent-adolescent conflict about autonomy is lessened. Similarly, perhaps in cultures where family closeness is especially prized (because family obligations and behavioral control are both high, as in U.S. Black and U.S. Latino youth) fewer internalizing problems emerge because, once again, parent-adolescent conflict about autonomy is lessened, but for different reasons than in “high autonomy” cultures. Future studies are needed to evaluate this hypothesis.
Why Studying Culture-Specific Variability in Trajectories Is Important
Collectively, our results highlight the importance of investigating cultural variability in adolescent externalizing and internalizing behaviors. Assuming universal trajectories of externalizing and internalizing problems across adolescence is perhaps most problematic because doing so prevents the identification of specific periods of growth or desistance in problems in each culture that provide insight into why a particular culture might be faring better in preventing adolescent problems. In the above discussion, we identify myriad factors at multiple levels of analysis that vary over culture, including legislative changes, educational transitions, and cultural norms around parent warmth, control, family obligations, and aggressive behaviors that may account for specific cultural variation in adolescent externalizing and internalizing trajectories. Only some of these hypotheses may be supported in the future, but all are testable, and all were made possible because we assumed cultural variability, instead of cultural uniformity, in adolescent externalizing and internalizing trajectories (Bornstein et al., 2017).
Cross-Cultural Effects of Parenting on Adolescent Externalizing/Internalizing Trajectories
We also examined the extent to which parent warmth and parent behavioral control were associated with trajectories of externalizing and internalizing behavior across cultures over time by utilizing the specificity principle (Bornstein, 2017) and IPART Theory (Rohner &AUTHOR, 2017). We made two predictions. First, based on IPART theory, we expected parent warmth to be near-universally associated with decreases in adolescent externalizing and internalizing problems over time across culture. Second, based on the specificity principle and the theoretical conceptualization that normative levels of behavioral control are more variable depending on cultural norms around family obligation and adolescent autonomy granting (Lansford, Godwin, et al., 2017; Dwairy & Achoui, 2010), we expected the prevalence of effects of behavioral control to vary to a much greater extent over cultures. Both hypotheses were largely supported. Support for these hypotheses begins to address why cross-cultural discrepancies in externalizing and internalizing behaviors persist even after controlling for a host of sociodemographic factors (Atilol et al., 2013; Rescorla et al., 2007a). It appears that cross-cultural differences in parent warmth and control can partially account for these discrepancies.
The Cross-Cultural Effects of Warmth
In 8 of 11 cultures (all except for Naples, Italy; Rome, Italy; and Kenya) parent warmth was associated with decreased externalizing problems at some point in development, and in 6 of 11 cultures, these associations continued or emerged in early adolescence from ages 10–14. Similarly, in 10 of 11 cultures (all except Rome, Italy) parent warmth protected against the emergence of internalizing problems at some point in development, and in 9 of 11 cultures, these effects continued or emerged in early adolescence from ages 10–14. Taken together, these results build on IPART’s hypothesis that children around the world have a need for warmth from their caregivers (Rohner & Co-Author, 2017) in two ways. First, our study demonstrates that parent warmth is associated with adaptive changes in externalizing and internalizing problems (which had not been previously measured in IPART literature). Second, our study demonstrates that these changes endure over the entirety of adolescence in many cultures (previous IPART studies were based on examining year-to-year change). Additionally, these current findings align with our previous work that demonstrated higher parent warmth was associated with lower internalizing and externalizing symptoms across cultures before, but not after, age 10 (Co-Author et al., 2018). However, our current work expands upon this previous work by moving beyond the study of year-over-year effects to investigate lasting effects of warmth on developmental trajectories of externalizing and internalizing problems over the entirety of adolescence. This shift was vital because it allowed us to identify that effects of warmth were not just limited to before age 10, but actually had downstream adaptive associations with externalizing and internalizing behavior into mid-adolescence (i.e., through age 14) in six of our eleven cultures.
The Culture-Specific Effects of Behavioral Control
Our specificity-principle-based hypothesis regarding high variability in prevalence of parent behavioral control across cultures was also supported. Parent behavioral control was associated with the emergence of externalizing problems in 3 of 11 cultures (Jordan, Sweden, and Thailand) and persisted past the age of 8 in Jordan and Sweden. Parent behavioral control was associated with emergence of internalizing problems in 4 of 11 cultures (Jordan, Thailand, U.S. White, U.S. Latino), and persisted to age 14 in the Jordan and U.S. White samples. Moreover, the direction of effects varied across cultures. For the U.S. White sample, higher parent behavioral control predicted decreases in internalizing problems across ages 10 to 14. Additionally, aligning with prior literature, for the U.S. White sample, higher levels of parent behavioral control across ages 10–14 were associated with less growth in externalizing symptoms across ages 10–14 at a marginally significant level (B = −.84, p = .067; Table 2). However, for all other cultures where behavioral control was significant, higher control predicted higher externalizing/internalizing problems. Notably, there was one cultural group (Jordan) where behavioral control was persistently and positively associated with both adolescent externalizing and internalizing symptoms.
We believe the lack of consistency in significance or direction in cross-cultural behavioral control effects emerges because cultural expectations vary greatly in how parents are expected to utilize behavioral control across the transition to adolescence (Co-Author et al., 2018). In some groups, parents are expected to give up behavioral control as their children transition to adolescence, whereas in others, parents are expected to maintain or increase their behavioral control, and even within groups the extent to which behavioral control is utilized by different families varies widely. Indeed, in prior analyses in our sample, 70% – 90% of variability in parent behavioral control existed within, as opposed to between, cultures (CoAuthor, 2018).
The present results build on our prior work with the present sample (i.e., Co-Author et al., 2018) in two ways. First, in contrast to our prior work, which examined change from one year to the next and found no culture-specific effects of behavioral control, the current study examined adolescent trajectories and did identify that behavioral control had some culture-specific effects over time. It is notable that in two cultures (Jordan and Sweden) where behavioral control was less normative than in the sample as a whole, greater behavioral control was associated with growth in externalizing (in the case of Sweden and Jordan) or internalizing (in the case of Jordan) trajectories. It may be that in some cultures where behavioral control is less normative, high parental behavioral control is deleterious as children age because the discrepancy between the normative levels of control that adolescents perceive in their culture, and the high levels of control they experience in their own family exacerbates parent-adolescent conflict around autonomy (Dwairy & Achoui, 2010).
Second, the current study builds on our past work by replicating our previous finding that there are relatively few universal effects of behavioral control on child development (Co-Author et al., 2018) and adds to this work by demonstrating effect replication when examining changing adolescent behavior over time. Given the lack of universal effects found across both of our studies, it may be that the effects of behavioral control on child externalizing and internalizing problems is a process that is best examined emically, from within each cultural group, and is less generalizable etically, or across cultures. Emphasizing this point, in our study higher parent behavioral control was a risk factor for externalizing and internalizing symptoms when it was significant in several cultures outside of the United States (e.g., Jordan, Sweden, Thailand). However, most meta-analyses utilizing primarily North American/European samples identify behavioral control as a protective factor. Without examining behavioral control effects across multiple cultures over time, universality of such protective effects could be erroneously assumed.
Strengths and Limitations
Our study has notable strengths, including its cross-cultural, longitudinal focus, emphasis on estimating trajectories of change in externalizing and internalizing behavior over time, and use of cross-culturally validated measures. However, our study also has limitations. First, our cultural groups are only generalizable to the cities, but not to the countries, in which they were collected. Second, data were available only from ages 8–14, and therefore we cannot speak to how the externalizing and internalizing trajectories we estimated extend earlier or later in development. Third, this study examined differences in level and slope of externalizing and internalizing behaviors, but did not examine the specific nature of internalizing and externalizing symptoms cross-culturally. So, for instance, although parents from two different cultures might rate an adolescent the same on being “too fearful/anxious,” the manifestations of behaviors that parents observe may vary across cultures. Future qualitative work can uncover cross-cultural differences in the specific nature of externalizing/internalizing problems.
Fourth, we only detected deleterious effects of parent behavioral over-control, as opposed to deleterious effects of both over-control and under-control. We suspect this may be because our behavioral control questionnaire items were more likely to pick up effects of behavioral over-control, such as higher parental strictness and punishment after rule-breaking. For instance “parents insist children do exactly as they are told” and “parents want to control whatever I do,” were items on our questionnaire that indicated over-control if scored higher. Consequently, future investigations should utilize other measures of behavioral control to identify whether effects of behavioral under-control can also be identified across cultures. Fifth, though prior investigations have demonstrated that cultural differences in externalizing and internalizing problems persist even when other sociodemographic factors are controlled, these sociodemographic factors (e.g., socioeconomic status, education) might moderate the effect of parenting on externalizing and internalizing trajectories in different cultures. These moderating effects should be studied in future investigations. Sixth, our parenting measures demonstrated impressive measurement invariance across most cultures, but warmth (in Kenya) and behavioral control (in Kenya and China) demonstrated non-invariance at some time points. Consequently, we refrained from making any culture-specific inferences about the effects of parenting behaviors in Kenya or China. Seventh and finally, we examined changes in trajectories before and after age 10 in the current study, because age 10 marked the average age of many school, peer, and neurobiological changes endured in adolescence. However, this is an imprecise measure; an even more precise measure of “pre-” and “post-” adolescence would be examining differences in trajectories before and after puberty onset. Future analyses can take this approach.
Conclusion
Internalizing and externalizing problems impair functioning at one point or another in most adolescents (Achenbach et al., 2008). Yet, existing cross-cultural studies of adolescent externalizing and internalizing behaviors are largely cross-sectional in nature and unable to identify why cultural differences may persist across cultures that vary widely in geographic region, ethnicity, religion, size, population and economic/political system. Addressing these gaps, ours is the first investigation to compare the continuous developmental course of externalizing and internalizing problems in early to mid-adolescence in many different cultures and to investigate one explanation for persistent cross-cultural differences: parenting behaviors. Across 12 cultural groups, we did not find universal trajectories of adolescent externalizing or internalizing problems and instead found significant cultural heterogeneity in starting points and rates of change in both externalizing and internalizing symptoms. Some similarities did emerge. In many of our cultural groups, internalizing symptoms decreased from ages 8–10, and externalizing symptoms increased from ages 10–14. Moreover, parental warmth appeared to function similarly in many cultures as a protective factor that prevented the onset and growth of externalizing and internalizing symptoms in adolescence. Finally, effects of behavioral control on externalizing and internalizing symptoms were less prevalent in significance and consistent in direction across cultures, and need further study in emic cultural models.
Supplementary Material
Acknowledgements
This research has been funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development grant RO1-HD054805 and Fogarty International Center grant RO3-TW008141. This research also was supported by the Intramural Research Program of the NIH/NICHD, USA, and an International Research Fellowship in collaboration with the Centre for the Evaluation of Development Policies (EDePO) at the Institute for Fiscal Studies (IFS), London, UK, funded by the European Research Council (ERC) under the Horizon 2020 research and innovation programme (grant agreement No 695300-HKADeC-ERC-2015-AdG). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH or NICHD.
Contributor Information
W. Andrew Rothenberg, Duke University, Durham, NC, USA.
Jennifer E. Lansford, Duke University, Durham, NC, USA
Marc H. Bornstein, Institute for Fiscal Studies, London, UK, and Eunice Kennedy Shriver National Institute of Child Health and Human Development, Bethesda, MD, USA
Lei Chang, University of Macau, China.
Kirby Deater-Deckard, University of Massachusetts, Amherst, MA, USA.
Laura Di Giunta, Università di Roma “La Sapienza,” Rome, Italy.
Kenneth A. Dodge, Duke University, Durham, NC, USA
Patrick S. Malone, Duke University, Durham, NC, USA
Paul Oburu, Maseno University, Maseno, Kenya.
Concetta Pastorelli, Università di Roma “La Sapienza,” Rome, Italy.
Ann T. Skinner, Duke University, Durham, NC, USA
Emma Sorbring, University West, Trollhättan, Sweden.
Laurence Steinberg, Temple University, Philadelphia, PA, USA.
Sombat Tapanya, Chiang Mai University, Chiang Mai, Thailand.
Liliana Maria Uribe Tirado, Universidad San Buenaventura, Medellín, Colombia.
Saengduean Yotanyamaneewong, Chiang Mai University, Chiang Mai, Thailand.
Liane Peña Alampay, Ateneo de Manila University, Quezon City, Philippines.
Suha M. Al-Hassan, Hashemite University, Zarqa, Jordan, and Emirates College for Advanced Education, Abu Dhabi, UAE
Dario Bacchini, University of Naples “Federico II,” Naples, Italy.
References
- Achenbach TM, & Rescorla LA (2001). Manual for the ASEBA School-Age Forms & Profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, & Families. [Google Scholar]
- Alampay LP, & Garcia AS (2019). Education and parenting in the Philippines. In Sorbring E & Lansford JE (Eds.), School systems, parent behavior, and academic achievement: An international perspective (pp. 79–94). Cham, Switzerland: Springer. [Google Scholar]
- Asparouhov T, & Muthén B (2014). Multiple-group factor analysis alignment. Structural Equation Modeling, 21(4), 495–508. [Google Scholar]
- Atilola O, Balhara YPS, Stevanovic D, Avicenna M, & Kandemir H (2013). Self-reported mental health problems among adolescents in developing countries: Results from an international pilot sample. Journal of Developmental and Behavioral Pediatrics, 34(2), 129–137. [DOI] [PubMed] [Google Scholar]
- Bollen KA, & Curran PJ (2006). Latent curve models: A structural equation approach. Wiley Series on Probability and Mathematical Statistics. Hoboken, NY: Wiley. [Google Scholar]
- Bornstein MH (2017). The specificity principle in acculturation science. Perspectives on Psychological Science, 12(1), 3–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Collishaw S (2015). Annual research review: Secular trends in child and adolescent mental health. Journal of Child Psychology and Psychiatry, 56(3), 370–393. [DOI] [PubMed] [Google Scholar]
- Curran PJ, Obeidat K, & Losardo D (2010). Twelve frequently asked questions about growth curve modeling. Journal of Cognition and Development, 11, 121–136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deater-Deckard K, Godwin J, Co-Author JE, Bacchini D, Bombi AS, Bornstein MH, … Al-Hassan SM (2018). Within- and between-person and group variance in behavior and beliefs in cross-cultural longitudinal data. Journal of Adolescence, 62, 207–217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ebesutani C, Bernstein A, Martinez JI, Chorpita BF, & Weisz JR (2011). The Youth Self Report: Applicability and validity across younger and older youths. Journal of Clinical Child & Adolescent Psychology, 40, 338–346. [DOI] [PubMed] [Google Scholar]
- Kieling C, Baker-Henningham H, Belfer M, Conti G, Ertem I, Omigbodun O, … Rahman A (2011). Child and adolescent mental health worldwide: Evidence for action. The Lancet, 378(9801), 1515–1525. [DOI] [PubMed] [Google Scholar]
- Khaleque A, & Rohner RP (2012). Pancultural associations between perceived parental acceptance and psychological adjustment of children and adults: A meta-analytic review of worldwide research. Journal of Cross-Cultural Psychology, 43(5), 784–800. [Google Scholar]
- Kline RB (2011). Principles and practices of structural equation modeling (3rd ed.). New York, NY: Guilford Press. [Google Scholar]
- Lancet The. (2017). Better understanding of youth mental health. The Lancet, 389(10080), 1670. [DOI] [PubMed] [Google Scholar]
- McKee L, Colletti C, Rakow A, Jones DJ, & Forehand R (2008). Parenting and child externalizing behaviors: Are the associations specific or diffuse? Aggression and Violent Behavior, 13(3), 201–215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén B, & Asparouhov T (2014). IRT studies of many groups: The alignment method. Frontiers in Psychology, 5, 978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pinquart M (2017b). Associations of parenting dimensions and styles with externalizing problems of children and adolescents: An updated meta-analysis. Developmental Psychology, 53(5), 873–932. [DOI] [PubMed] [Google Scholar]
- Pinquart M (2017a). Associations of parenting dimensions and styles with internalizing symptoms in children and adolescents: A meta-analysis. Marriage & Family Review, 53(7), 613–640. [Google Scholar]
- Punyanunt-Carter NM (2016). An examination of communication motives and relationship maintenance behaviors in Thai and US father-daughter relationships. Asian Communication Research 13(1), 157–179. [Google Scholar]
- Rescorla L, Achenbach T, Ivanova MY, Dumenci L, Almqvist F, Bilenberg N, … Verhulst F (2007a). Behavioral and emotional problems reported by parents of children ages 6 to 16 in 31 societies. Journal of Emotional and Behavioral Disorders, 15(3), 130–142. [Google Scholar]
- Rescorla L, Achenbach TM, Ivanova MY, Dumenci L, Almqvist F, Bilenberg N, … Verhulst F (2007b). Epidemiological comparisons of problems and positive qualities reported by adolescents in 24 countries. Journal of Consulting and Clinical Psychology, 75(2), 351–358. [DOI] [PubMed] [Google Scholar]
- Rescorla L, Ivanova MY, Achenbach TM, Begovac I, Chahed M, Drugli MB,… Zhang EY (2012). International epidemiology of child and adolescent psychopathology II: Integration and applications of dimensional findings from 44 societies. Journal of the American Academy of Child & Adolescent Psychiatry, 51(12), 1273–1283. [DOI] [PubMed] [Google Scholar]
- Rohner RP (2005). Parental Acceptance-Rejection Questionnaire (PARQ): Test manual. In Rohner RP & Khaleque A (Eds.), Handbook for the study of parental acceptance and rejection (4th ed., pp. 43–106). Storrs, CT: Center for the Study of Parental Acceptance and Rejection, University of Connecticut. [Google Scholar]
- Rohner RP, & Co-Author JE (2017). Deep structure of the human affectional system: Introduction to interpersonal acceptance–rejection theory. Journal of Family Theory & Review, 9(4), 426–440. [Google Scholar]
- Rooney RM, Morrison D, Hassan S, Kane R, Roberts C, & Mancini V (2013). Prevention of internalizing disorders in 9–10 year old children: Efficacy of The Aussie Optimism Positive Thinking Skills Program at 30-month follow-up. Frontiers in Psychology, 4, 988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sheppard CS, Giletta M, & Prinstein MJ (2019). Peer victimization trajectories at the adolescent transition: Associations among chronic victimization, peer-reported status, and adjustment. Journal of Clinical Child & Adolescent Psychology, 48, 218–227. [DOI] [PubMed] [Google Scholar]
- Sorbring E, & Lansford JE (Eds.). (2019). School systems, parent behavior, and academic achievement: An international perspective. Cham, Switzerland: Springer. [Google Scholar]
- Steinberg L, Icenogle G, Shulman EP, Breiner K, Chein J, Bacchini D, … Takash HMS (2018). Around the world, adolescence is a time of heightened sensation seeking and immature self-regulation. Developmental Science, 21(2), 1–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Verhulst FC, Achenbach TM, van der Ende J, Erol N, Lambert MC, Leung PWL, Silva MA,…& Zubrick SR (2003). Comparisons of problems reported by youths from seven countries. The American Journal of Psychiatry, 160(8), 1479–1485. [DOI] [PubMed] [Google Scholar]
- Wetter EK, & El-Sheikh SM (2012). Trajectories of children’s internalizing symptoms: The role of maternal internalizing symptoms, respiratory sinus arrhythmia and child sex. Journal of Child Psychology and Psychiatry, 53(2), 168–177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- UNICEF. (2017). Standards for ECD parenting programmes in low and middle income countries. New York, NY: UNICEF. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.