

Abstract
Background
Drug users (including both injection drug users and crack cocaine users), are at high levels of risk for contracting HIV. Therefore it is important to reduce the injection and/or sexual risk behaviours of these groups both for the benefit of themselves and for society as a whole.
Objectives
To assess the efficacy of multi‐session psychosocial interventions in comparison with standard education and minimal intervention controls for the reduction of injection and sexual risk behaviour.
Search methods
Electronic searches were conducted of a number of bibliographic databases (including Cochrane Library, CINAHL, MEDLINE, PsycINFO). In addition, other methods of locating papers were employed including contacting various authors working in the field of HIV risk reduction and examining reference lists of applicable papers identified in the electronic search.
Selection criteria
The inclusion criteria consisted of randomised and quazi‐randomised trials assessing the efficacy of psychosocial interventions in the reduction of injection and sexual risk behaviour for people who misused opiates, cocaine, or a combination of these drugs.
Data collection and analysis
Two authors independently assessed the eligibility of studies identified by the search strategy, quality assessed these studies and extracted the data. A total of 35 trials met the eligibility criteria of the review providing data on 11,867 participants.
Main results
There were minimal differences identified between multi‐session psychosocial interventions and standard educational interventions for both injection and sexual risk behaviour. Although it should be noted there were large pre‐post changes for both groups suggesting both were effective in reducing risk behaviours. In addition, there was some evidence of benefit for multi‐session psychosocial interventions when compared with minimal controls. Subgroup analyses suggest that people in formal treatment are likely to respond to multi‐session psychosocial interventions. It also appears single‐gender groups may be associated with greater benefit.
Authors' conclusions
There is limited support for the widespread use of formal multi‐session psychosocial interventions for reducing injection and sexual risk behaviour. Brief standard education interventions appear to be a more cost‐effective option. Further research is required to assess if there are particular groups of drug users more likely to respond to such interventions.
Plain language summary
Psychosocial interventions for the reduction of injection and sexual risk behaviour for preventing HIV in drug users
People who misuse drugs are at greater risk of developing HIV. Interventions designed to reduce this risk have been developed. There were 35 trials on 11,867 participants that examined whether these interventions are effective in reducing sexual and injection behaviour associated with greater risk of developing HIV. There are not large differences in effectiveness between multi‐session psychosocial interventions and briefer interventions. This suggests brief educational interventions are more likely to be cost‐effective and may be more readily implemented in a variety of different contexts.
Background
It is widely accepted that injecting drug users are at greater risk of developing blood borne viruses (such as HIV) than the general population. A recent prospective cohort study of new injecting drug users in the UK found high levels of injecting risk behaviour (Judd 2005). A total of 24% reported having injected in the last 4 weeks with needles and syringes used by someone else and 53% having shared injecting paraphernalia. The baseline prevalence of antibodies to hepatitis C virus was 44% and of antibodies to HIV 4%. It would appear that injecting drug users have an incidence of HIV comparable to that among men who have sex with men attending clinics for sexually transmitted infections (Judd 2005). However, IDUs present as a risk of contracting HIV not only in terms of their injecting but also their sexual risk behaviour. The diverse nature of such risk behaviour presents a formidable challenge for interventions designed to prevent or reduce risk for infection in this population (Copenhaver 2006). In addition, HIV risk behaviours are not only prevalent among IDUs but also in other groups of drug users. For example, people who misuse crack cocaine also appear to engage in high levels of sexual risk behaviour (for example, Malow 1994).
Reducing injecting and sexual risk behaviours of illicit drug users has important public health implications throughout the world. During most of the twentieth century, illicit narcotic use was sufficiently concentrated in the United States that heroin addiction was known as "the American Disease" (Musto 1993). Heroin use then expanded greatly and became well established in Western Europe (EMCCDA2007). With the globalisation of international trade, however, heroin use and illicit drug injection has become a significant problem in developing and transitional countries.
Recent estimates suggests there are approximately 13‐16 million injecting drug users worldwide (Aceijas 2004; Mathers 2008). Approximately 77% of the total injecting drug users were located in developing and transitional countries (Aceijas 2004). One important consequence of this is the need for interventions that not only are effective in reducing risk behavior and HIV transmission among IDUs, but that require only modest amounts of resources in terms of both monies and highly trained personnel.
One of the central public health interventions to reduce injection drug use has been through the establishment of needle and syringe exchange programmes. A number of studies have assessed the efficacy of needle and syringe exchange (NSE) programmes. The results have been summarised in several recent systematic reviews (for example, Gibson 2001; Ksobiech 2003;Wodak 2005) and therefore will not be specifically considered here.
The focus of this review will be on multi‐session psychosocial interventions designed to reduce injection and sexual behaviours associated with greater risk of contracting HIV.This is important for a number of reasons: firstly this will help to inform NSE and drug treatment programmes on whether the provision of psychosocial interventions (and at what intensity) is likely to prevent HIV risk behaviours which should have important implications for resource use in these settings. Secondly, while the focus of NSE programmes is on reducing injection risk behaviour, for non‐injecting drug users and injection drug users who engage in sexual risk behaviour, psychosocial interventions are particularly likely to have potential for reducing HIV risk behaviours in these groups.
There have been few systematic reviews of HIV risk reduction in drug users. A recent systematic review concluded that multi‐session psychosocial interventions were effective in reducing risk behaviour (Copenhaver 2006). However, there were some questions with how the meta‐analysis was conducted. For example, it appeared that in trials with more than one treatment arm data was included in the analysis of both treatments which is likely to introduce bias in the analysis. In addition, interventions were compared with control groups of varying intensity therefore it is difficult to interpret the effect estimates.
Objectives
1) To locate and describe randomised and quazi‐randomised controlled trials on multi‐session psychosocial interventions in comparison with standard education and minimal interventions to reduce injection and sexual behaviours in people who misuse cocaine, opiates, or a combination of cocaine and opiates associated with greater risk of HIV infection.
2) To conduct meta‐analysis, where possible and appropriate, to assess the efficacy of the included interventions for reducing injection and sexual risk behaviours.
3) To make practical recommendations on the use of multi‐session psychosocial interventions in drug treatment and other services to reduce risk behaviours.
4) To provide suggestions for further research.
Methods
Criteria for considering studies for this review
Types of studies
Randomised and quasi‐randomised controlled trials.
Types of participants
People who misuse opiates, cocaine or a combination of opiates and cocaine. This includes both people in contact with drug treatment services and those who are not. People who primarily misuse alcohol or other drugs such as methamphetamine were excluded from this review.
Types of interventions
Multi‐session psychosocial interventions designed specifically to reduce injection and/or sexual risk behaviour among people who misuse drugs. Multi‐session psychosocial interventions were defined as a programme designed for individuals or groups of people who misuse drugs that consist of a minimum of three sessions combining education about HIV with skills training to improve communication skills, assertiveness, and safe sexual and injection risk behaviour. It also provides people who misuse drugs with an opportunity to ask questions and receive relevant feedback. These interventions are provided in a variety of settings such as methadone maintenance clinics, needle and syringe exchanges, and outreach programmes.
Standard education interventions designed for individuals or groups of people who misuse drugs and consisting of one to two sessions. The content is often similar to multi‐session interventions including HIV testing, counselling and some skills training.
Minimal intervention was defined as receiving minimal or no psychosocial intervention and often involved the provision of a self help booklet.
Types of outcome measures
Intervention studies should contain at least one outcome measure of injection risk behaviour, sexual risk behaviour, or HIV seroconversion.
Search methods for identification of studies
a) Electronic searching
We searched the Cochrane Library, CINAHL, MEDLINE, and PsycINFO databases in November 2006, using the following search strategy, from inception to 2006:
Drugs filter 1) Cocaine‐related disorders/or Substance withdrawal syndrome/ or exp Opioid‐related disorders/ or Substance abuse, intravenous/ or Substance‐related disorders/
2) Analgesic agent abuse/ or Cocaine dependence/ or Drug abuse/ or Drug abuse pattern/ or Drug dependence/ or Drug misuse/ or Intravenous drug abuse/ or Multiple drug abuse/ or exp Narcotic dependence/ or Opiate addiction/or Substance abuse/ or "Substance use disorders"/ or Substance abuse/ or Substance abuse, intravenous/ or Substance abuse, perinatal/ or Substance dependence/ or Substance withdrawal syndrome/
3)Drug abuse/ or Drug Dependency/ or Polydrug abuse/ or Drug addiction/ or Drug dependency/ or Heroin addiction/ or Drug overdoses/ 5(((stimulant$ or polydrug$ or drug$1 or substance) adj3 (abstain$ or abstinen$ or abus$ or addict$ or (excessive adj use$) or dependen$ or disorder$ or intoxicat$ or misuse$ or over dos$ or overdos$ or (use$ adj (disorder$ or illicit)) or withdraw$)) or (drug$1 adj user$)).tw.
4) or/1‐3
5) (abstain$ or abstinen$ or abus$ or addict$ or (drug adj use$) or (excessive adj use$) or dependen$ or intoxicat$ or misus$ or over dos$ or overdos$ or (use$ adj (disorder$ or illicit)) or withdraw$).ti,ab.
6) Diamorphine/ or exp Heroin/ 9(heroin or diacetylmorphine or diamorphine or morphin$ or morfin$).ab,ti.
7) exp Narcotic agent/ or exp Narcotics/
8) opioid$.ab,ti.
9)opiate$.mp.
10) exp Methadone/
11) methadone.ab,ti.
12)exp Opiate/ or exp Opiates/ or exp Opium/
13)opium.ab,ti.
14) exp Amphetamines/
15) (amphetamine$ or amphetamine$ or crank or methamphetamine$ or dextroamphetamine$ or speed).ti,ab.
16) exp Cocaine/
17) (cocaine or crack).ab,ti.
18)Central nervous system stimulants/ or Central nervous system stimulating drugs/ or Central Stimulant Agent/
19)(analeptic$ or psychostimulant$ or stimulant$).ab,ti.
20)(diethylpropion or ephedrine or fenfluramine or methylphenidate or pemoline or phenmetrazine or phendimetrazine or phenylpropanolamine).mp.
21) or/4‐20
Psychosocial Interventions filter 22) adaptation,psychological/
23) exp aversive stimulation/ or exp electrical stimulation/
24) exp behavior therapy/
25) "biofeedback (psychology)"/ or "biofeedback (IOWA NIC)"/ or biofeedback/ or feedback system/
26) exp case management/
27)exp cognitive therapy/
28) exp community mental health/ or exp community mental health services/
29)exp community networks/
30) exp coping behavior/
31) exp counseling/ or exp family counseling/ or exp patient counseling/
32) (day care$ or partial hospitalization).sh.
33) education program/
34) exp family therapy/
35) exp "imagery (psychotherapy)"/
36)interpersonal psychotherapy/
37) exp marriage counseling/ or exp marital therapy/
38) exp motivation/
39)patient education/ or client education/
40) psychoeducation/
41) exp psychodynamics/
42) exp psychotherapy/ or psychotherapy,brief/ or exp brief psychotherapy/ or psychotherapy,group/ or psychotherapy,multiple/ or exp supportive psychotherapy/ or exp interpersonal psychotherapy/ or exp expressive psychotherapy/ or exp group psychotherapy/ or exp individual psychotherapy/
43) exp reinforcement/ or exp reinforcement schedules/ or exp reinforcement,social/
44) exp relaxation/ or exp relaxation techniques/
45)residen$.mp. and (rehab$.mp. or exp drug abuse/rh or exp substance abuse/rh or exp substance related disorders/rh)
46)exp self help groups/ or exp self help/
47)social adaption/ or exp social adjustment/
48)exp social skills training/
49)exp social support/
50) exp socialization/
60) exp teaching/
61) exp therapeutic community/
62) biofeedback.tw.
63) ((case or care) and management) or CPA or care programme approach or assertive community treatment or PACT or TCL or (training adj2 community living) or (madison adj5 model)).mp.
64) ((behavio?r$ or cogniti$) and (educat$ or intervent$ or manage$ or program$ or rehab$ or technique$ or therap$ or train$ or treat$)) or cbt).tw.
65) (communicat$ adj5 (educat$ or intervent$ or manage$ or program$ or rehab$ or technique$ or therap$ or train$ or treat$)).tw.
66) (confrontational adj5 (educat$ or intervent$ or manage$ or program$ or rehab$ or technique$ or therap$ or train$ or treat$)).tw.
67) (contingency adj5 (educat$ or intervent$ or manage$ or program$ or rehab$ or technique$ or therap$ or train$ or treat$)).tw.
68) ((cope or coping) adj5 (educat$ or interven$ or manage$ or program$ or technique$ or therap$ or train$ or treat$)).tw.
69) (counsel?ing or counsel?or$).mp. or ((clientcentred or client centred) adj5 (communicat$ or educat$ or intervention$ or management$ or treatment$ or program$ or relation$ or support$ or therap$ or train$)).tw.
70) covert sensitisation.tw.
71) (day adj (care$ or center$ or centre$ or facilit$ or hospital$ or program$)) or daycare$).tw.
72) (educat$ adj5 (film$ or intervention$ or lecture$ or program$ or therap$ or treat$)).tw.
73) (family adj (based or cent$ or focused or focused)) or (family adj3 (communicat$ or educat$ or intervention$ or manage$ or treat$ or program$ or relation$ or support$ or therap$ or train$)) or (conjoint adj therap$) or (parent and (child$ adj3 treatment$)) or ((father or mother or parent) and (child adj3 (intervention$ or therap$ or treatment$))) or (family‐based or family‐responsive or family‐relation$)).tw.
74) ((inter personal or interpersonal) adj5 (educat$ or intervent$ or manage$ or program$ or technique$ or therap$ or train$ or treat$)).tw.
75) ((marital or marriage) adj (based or cent$ or focused)) or ((marital or marriage) adj5 (educat$ or intervent$ or manage$ or program$ or rehab$ or technique$ or therap$ or train$ or treat$))).tw.
76) (matrix or minnesota) and model).mp.
77) ((milieu or situational or socio?environmental or socio environmental) adj5 (educat$ or intervent$ or manage$ or program$ or rehab$ or technique$ or therap$ or train$ or treat$)) or (therapeutic adj communit$)).tw.
78) (motivation$ adj5 (educat$ or enhance$ or interview$ or manage$ or program$ or intervention$ or technique$ or therap$ or train$ or treat$)).tw. 80((neurobehavio$ or neuro behav$) adj5 (educat$ or intervent$ or manage$ or program$ or rehab$ or technique$ or therap$ or train$ or treat$)).tw. 81(psycho$ adj (communicat$ or educat$ or intervention$ or manage$ or treatment$ or program$ or rehab$ or relation$ or support$ or technique$ or therap$ or train$)).mp.
80) (psycho analy$ or psychoanaly$).mp.
81) (psycho dynamic$ or psychodynamic$).mp.
82) (psycho educat$ or psychoeducat$).mp.
83) (psychological adj5 (educat$ or intervent$ or manage$ or program$ or rehab$ or technique$ or therap$ or train$ or treat$)).tw. 86(psycho‐social$ or psychosocial$).mp.
87) psychotherap$.mp.
88) (reinforcer$ or reinforcement).tw.
89) relapse prevent$.tw.
90) relax$.mp. or controlled breathing.tw.
91) (self control and (educat$ or intervent$ or manage$ or program$ or technique$ or therap$ or treat$)).tw.
92) ((selfhelp or self help$ or self control) adj (based or cent$ or focused or focused)) or ((selfhelp or self help$ or self control) adj3 (communicat$ or educat$ or intervention$ or management$ or technique$ or treatment$ or program$ or relation$ or support$ or therap$ or train$))).tw.
93) (skill$ adj3 train$).tw.
94) (social adj2 (adapt$ or adjust$)).mp.
95) (social skill$ adj5 (educat$ or intervent$ or manage$ or program$ or technique$ or therap$ or train$ or treat$)).tw.
96) (stress adj5 (educat$ or intervent$ or manage$ or program$ or technique$ or therap$ or train$ or treat$)) or ((anger or parent$) adj3 manage$)).tw.
97) (supportive adj5 expressive).tw.
98) "12 step$1".tw.
99) ((psych$ or social$) adj5 (educat$ or intervent$ or manage$ or program$ or technique$ or therap$ or train$ or treat$)).tw.
100) or/22‐99
RCT filter 101) exp clinical trials/ or exp clinical trial/ or exp controlled clinical trials/
102) exp crossover procedure/ or exp cross over studies/ or exp crossover design/
103) exp double blind procedure/ or exp double blind method/ or exp double blind studies/ or exp single blind procedure/ or exp single blind method/ or exp single blind studies/
104) exp random allocation/ or exp randomization/ or exp random assignment/ or exp random sample/ or exp random sampling/
105) exp randomized controlled trials/ or exp randomized controlled trial/
106) (clinical adj2 trial$).tw.
107) (crossover or cross over).tw.
108) ((single$ or doubl$ or trebl$ or tripl$) adj5 (blind$ or mask$ or dummy)) or (singleblind$ or doubleblind$ or trebleblind$)).tw.
109) (placebo$ or random$).mp.
110) (clinical trial$ or random$).pt. or (random$ or clinical control trial).sd.
111) or/101‐110
112) and/21,100,111
b) Reference lists Reference lists of all the studies which went into the pool of retrieved studies, including those of other reviews, were examined in order to identify any further studies.
c) Personal contact We attempted to contact authors and experts in the field to identify further relevant studies.
Data collection and analysis
1. Selection of studies
NM and RL independently applied the inclusion criteria and differences were resolved by a third author (SP). Studies were reviewed for relevance on the basis of study design, population, intervention, and outcome as set out above.
2. Data extraction
Data was entered into a database designed specifically for data extraction which has been piloted on several previous systematic reviews by the authors providing a standardised overview of all included studies and the reasons for exclusion of excluded studies.
3. Quality assessment
The SIGN checklist for randomised controlled trials (for further details see NICE 2005) was used to assess the quality of all included trials. NM and RL applied the quality criteria independently and any differences were resolved by a third reviewer SP.
4. Data synthesis
Meta‐analysis, where possible and appropriate, was conducted.
Sub‐group analyses were undertaken on setting, gender‐specific interventions, and HIV testing.
Results
Description of studies
A total of 35 trials met the eligibility criteria of the review providing data on 11,867 participants and 24 trials were excluded.
Of the included trials, 28 contained comparisons of multi‐session psychosocial interventions with standard education, five comparisons of multi‐session psychosocial interventions with the provision of a self‐help booklet, six comparisons of standard education with a self‐help booklet (the total number of comparisons was greater than the total number of trials as some included more than one treatment or control arm). Multi‐session psychosocial interventions ranged from 3‐16 sessions, whilst standard education and self‐help interventions consisted of one to two sessions. In addition, 4 of these included trials conducted a sub‐analysis on participants who were considered to be at a high risk of contracting blood‐borne viruses. No unpublished or foreign language studies were identified by the search methods.
In terms of setting in which the multi‐session psychosocial intervention was delivered, 12 trials were of people in formal drug treatment and 23 trials were of participants not in formal drug treatment.
Risk of bias in included studies
Most studies did not report methods of allocation concealment, information was available from only two studies (SORENSEN1994: Detox; SORENSEN1994: MMT;TUCKER2004) both used sealed envelopes.
In terms of randomisation, 13 trials were quasi‐randomised all forming part of the NADR study (COLON1993; KOTRANSKI1998; SIEGAL1995; NADR: Site 1; NADR: Site 10; NADR: Site 14; NADR: Site 16; NADR: Site 17; NADR: Site 18; NADR: Site 19; NADR: Site 20; NADR: Site 4) all other included studies were randomised.
In terms of blinding, seven trials reported not using blinding, 24 trials blinding was not reported and four studies were single blinded.
Attrition, as commonly found in studies of people who misuse drugs, was high.
Effects of interventions
All results of the meta‐analyses are provided in the data and analyses section. Separate meta‐analyses compared multi‐session psychosocial interventions with standard education, standard education with minimal controls and multi‐session psychosocial interventions with minimal controls.
In addition, planned sub‐group analyses were conducted comparing the effectiveness of interventions for formal and informal settings, single‐gender and mixed gender groups, and in studies that included HIV testing in both groups. These sub‐group analyses were examined using combined injection and sexual risk behaviour in order to increase the power of detecting differences between sub‐groups.
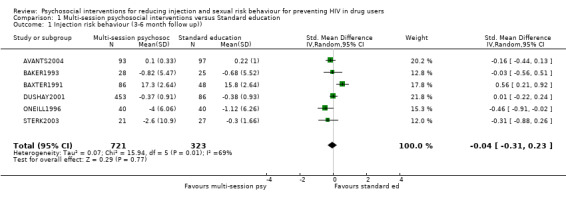
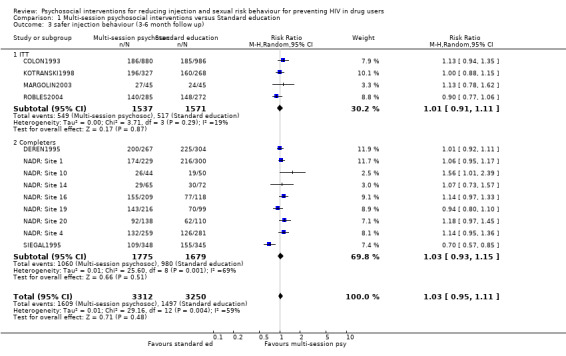
Multi‐session psychosocial interventions versus Standard education (see section 1: Data and analyses) There was little evidence of benefit for multi‐session psychosocial interventions in comparison with standard education. In terms of injection risk behaviour, no differences were found in the dichotomous outcome of engaging in safer injecting behaviours (RR = 1.03, 95% CI 0.95, 1.11) nor for the continuous outcome of reducing risk behaviour at endpoint (SMD = ‐0.04, 95% CI ‐0.31, 0.23). For both outcomes there was high heterogeneity with I2 values of 59% and 69% respectively. However, at longer term follow up there was some evidence of benefit (SMD = ‐0.81, 95% CI ‐1.29, ‐0.33) but data was only available for one trial.
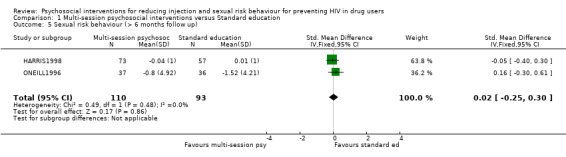
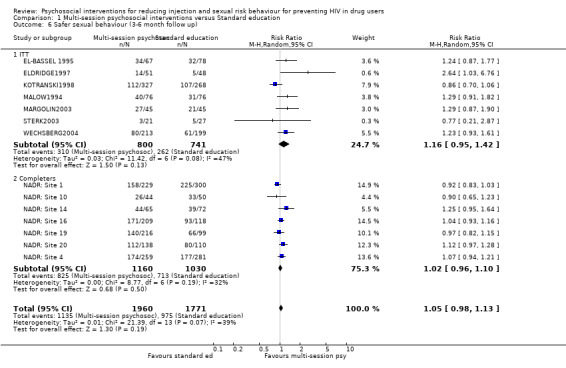
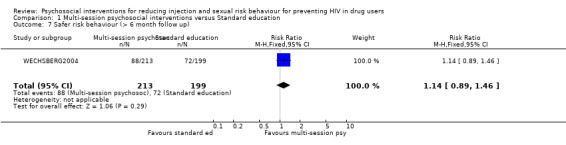
There was similar results with regard to sexual risk behaviour. Little difference was found between multi‐session psychosocial interventions and standard education in engaging in safer sexual risk behaviour (RR = 1.05, 95% CI 0.98, 1.13) and reducing sexual risk behaviour (SMD = ‐0.12, 95% CI ‐0.33, 0.08). There was also high heterogeneity (I2 = 49% and 39% respectively).
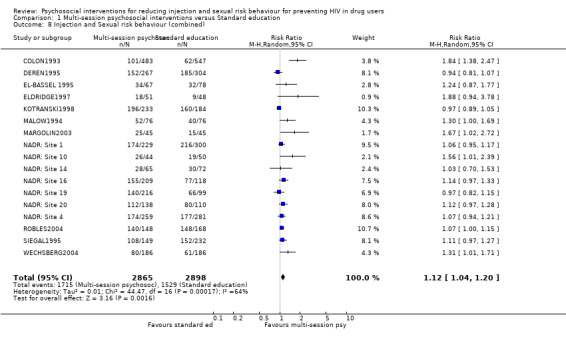
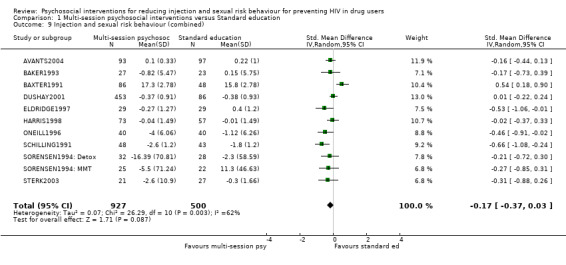
Combining data on injection and sexual risk behaviour there was some evidence for a small increase in safer behaviour (RR = 1.12, 95% CI 1.04, 1.20), however, there was a high level of heterogeneity (I2 = 81.1%). Similarly, there was a small, but not statistically significant, reduction in risk behaviour (SMD = ‐0.17, 95% CI ‐0.37, 0.03) and evidence of high heterogeneity (I2 = 62.0%).
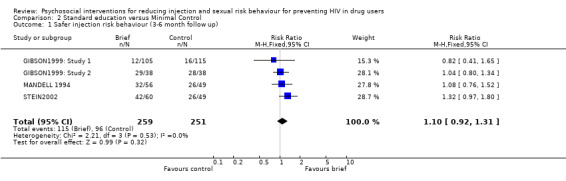
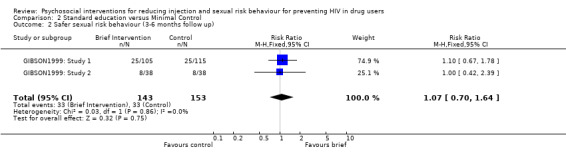
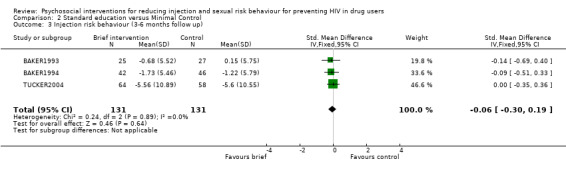
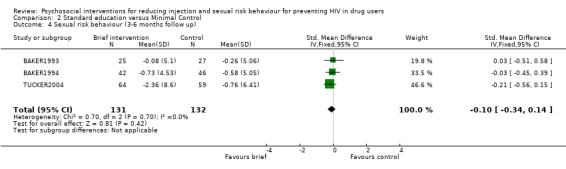
Standard education versus Minimal Control (see section 2:Data and analyses) There was no evidence of difference between standard interventions and minimal interventions for both injection risk behaviour (engaging in risk behaviour: RR = 1.10 95% CI 0.92, 1.31; reducing risk behaviour: SMD = ‐0.06; 95% CI ‐0.30, 0.19) and sexual risk behaviour (engaging in risk behaviour: RR = 1.07, 95% CI 0.70, 1.64; reducing risk behaviour: SMD = ‐0.10, 95% CI ‐0.34, 0.14).
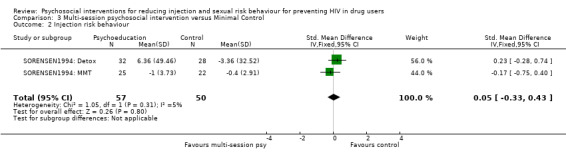
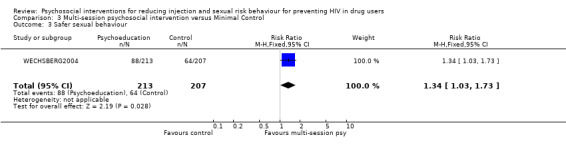
Multi‐session psychosocial interventions versus Minimal Control (see section 3: Data and analyses) There was no evidence of difference between multi‐session psychosocial interventions and minimal interventions for injection risk behaviour (SMD = 0.05, 95% CI ‐0.33, 0.43). However, there was some evidence of benefit for multi‐session psychosocial interventions for sexual risk behaviour in terms of dichotomous measures (although only consisting of one study) of engaging in safer sexual behaviour (RR = 1.34, 95% CI 1.03, 1.73) and in terms of continuous measures of reducing sexual risk behaviour (SMD = ‐0.31; 95% CI ‐0.56, ‐0.06).
Sub‐group analyses (see sections 4, 5 and 6: Data and analyses)
Sub‐group analyses were conducted on a priori determined groups of trials on the basis of setting (receiving formal drug treatment or not), gender (mixed or single gender group interventions) and the use of HIV testing.
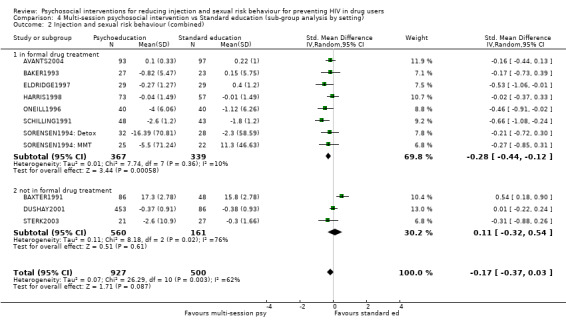
Setting appeared to have some impact on the effectiveness of the intervention. Although there was some overlap in confidence intervals between the two sub‐groups there appeared to be a small benefit for people engaged in treatment (RR = 1.42, 95% CI 1.14, 1.77; SMD = ‐0.28, 95% CI ‐0.44, ‐0.12) but less evidence of effectiveness for those not engaged in treatment (RR = 1.10, 95% CI 1.02, 1.18; SMD = 0.11, 95% CI ‐0.32, 0.54).
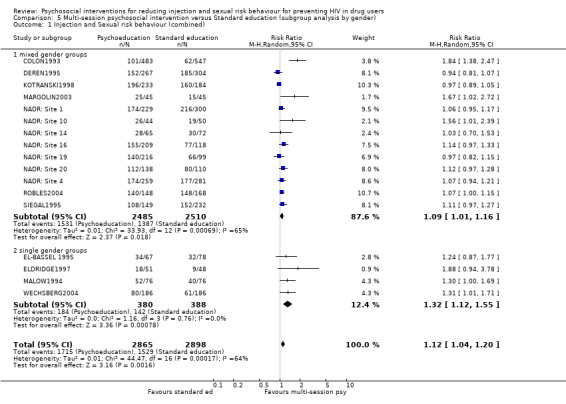
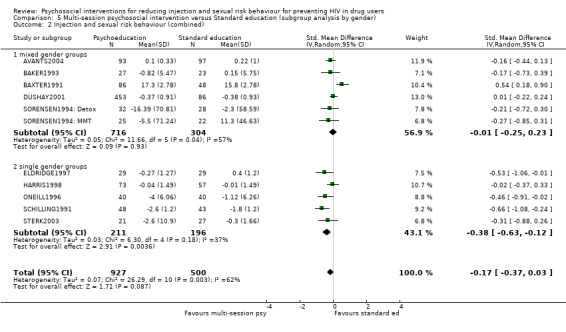
Trials conducted on specific gender groups (mainly females) appeared to be slightly more effective (RR = 1.32, 95% CI 1.12, 1.55; SMD = ‐0.38, 95% CI ‐0.63, ‐0.12) compared with mixed gender groups (RR = 1.09, 95% CI 1.01, 1.16; SMD = ‐0.01, 95% CI ‐0.25, 0.23) but there was overlap between confidence intervals.
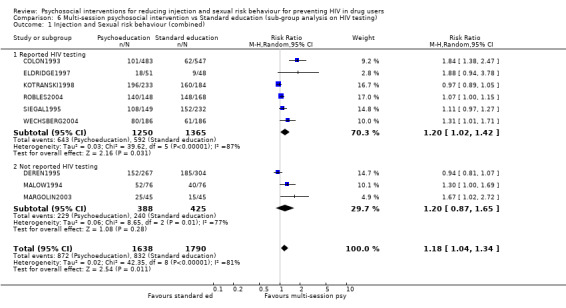
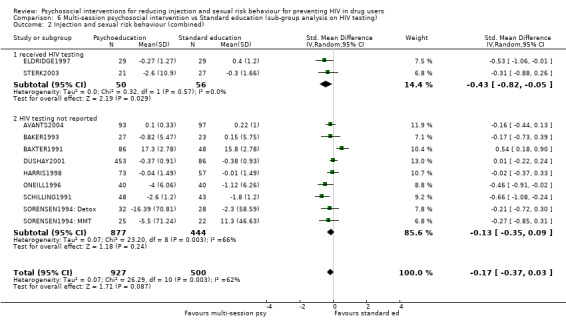
The effects of the provision of HIV testing did not appear to have an impact on results. There was wide overlap between confidence intervals in those studies that reported the use of HIV testing for all participants.
Sensitivity analysis (see section 7: Data and analyses)
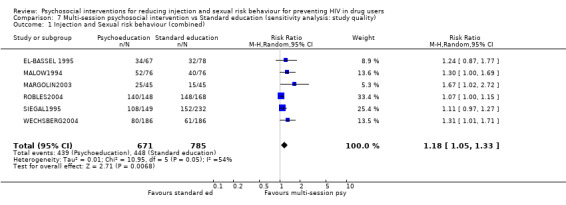
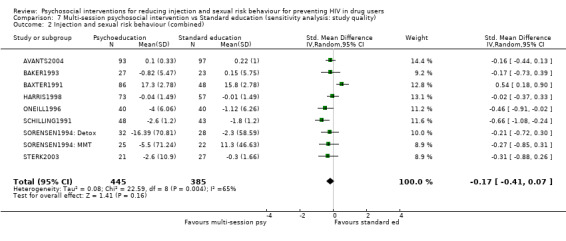
Study design did not appear to have a strong impact on results, the inclusion of only randomised controlled trials made little difference to the conclusions on estimate of effect.
Discussion
It appears that formal multi‐session psychosocial interventions are not more effective than briefer standard education. Therefore there is insufficient evidence to recommend the widespread use of formal multi‐session psychosocial interventions to reduce the injection and sexual risk behaviours of drug users. However, this suggests the possible benefit of using brief educational interventions (in terms of cost‐effectiveness and ease of implementation).
The very modest effect size we observed requires some comment. First, the effect is based on the comparison of the intervention with a comparison condition that usually involved HIV counselling and testing and some form of HIV education. Ethical considerations relating to providing information needed to avoid a potentially fatal disease, and research considerations obtaining HIV prevalence data, typically required that subjects in the comparison condition receive these services. Inspection of the pre vs. post data in the studies generally showed substantial reported behavior change in both the intervention and comparison groups. Thus, the findings in this review should not be interpreted as indicating that the interventions were not effective, but rather that the interventions were not substantially more effective than the services provided to the comparison subjects.
A second consideration is based on the social nature of much injecting drug use. Many drug users frequently share information about sources of drugs, cooperate to obtain drugs, and use drugs together. Thus, they are also likely to share new information about AIDS, and these group discussions may promote risk reduction among members of both intervention and comparison groups (Des Jarlais 1995).
Finally, most of the studies did not conduct (or at least did not report conducting) needs assessments before conducting the intervention studies. It is possible that needs assessments would have led to modest differences in the interventions that might have produced much larger differences between the intervention and the comparison groups. Conducting such needs assessments before implementing the intervention studies, however, illustrates the ethical issues involved in HIV prevention research. If the needs assessment showed that the potential subjects had specific requirements for reducing their risk of acquiring HIV, then the researchers would have a very strong ethical imperative to provide the needed services to both intervention and control subjects.
The results of this systematic review are generally consistent with previous reviews (for example, Copenhaver 2006; Semaan 2002) suggesting minimal differences between more intensive multi‐session psychosocial and standard educational interventions. Although Copenhaver 2006 suggested their meta‐analysis indicated the efficacy of multi‐session psychosocial (or behavioural interventions) their conclusions may have relied more on statistical significance than clinical significance. Additionally, inclusion of both minimal controls and brief educational comparators in the same analysis may have inflated the effect slightly. Similarly, Semaan 2002 found a relatively small effect size when comparing multi‐session psychosocial interventions with other interventions and also found some benefit for multi‐session psychosocial interventions compared with minimal interventions for sexual risk reduction.
There are several limitations to this review. All studies relied on self‐report measures and so didn't include objective indicators such as HIV seroconversion rates. Secondly, most studies did not report intention‐to‐treat data which may have added bias to the results. Thirdly, most studies were conducted in North America therefore it may be questioned whether these findings can be extrapolated to other populations, such as developing countries, where the vast majority of injecting drug users reside. Finally, it could be argued, the inclusion of quasi‐randomised studies may have introduced bias into the meta‐analysis. However, a sensitivity analysis including only randomised trials found largely similar results.
Authors' conclusions
Implications for practice.
There is insufficient evidence to recommend the widespread use of formal multi‐session psychosocial interventions to reduce the injection and sexual risk behaviours of drug users. In addition, subgroup analyses suggest that those in formal drug treatment appear to be slightly more likely to reduce their risk behaviour but this still requires substantiating in randomised trials.
However, we would not want readers of this review to conclude that interventions to reduce risk behavior among IDUs are ineffective. Both standard education and formal multi‐session psychosocial interventions were associated with reductions in risk behaviour. This is an important finding, both for people in developing and developed countries, as it suggests standard education interventions are likely to be a more cost‐effective option for reducing HIV risk behaviour. This suggests brief standard education interventions should be a treatment option alongside other effective interventions. There is a general consensus that community outreach programs, programs to provide access to sterile injection equipment, and drug abuse treatment (particularly methadone maintenance treatment for heroin addiction) are effective in reducing risk behavior and HIV transmission among IDUs (National Institute for Health 1997; Institute of Medicine 2006). We would note that the greatest effects are likely to occur with "structural" interventions that are applied at the community level, with diffusion of information and materials for safer behavior (sterile injection equipment and condoms) throughout the local IDU population and the development of new social norms promoting safer behavior (Des Jarlais2000).
Implications for research.
The emphasis on formal multi‐session psychosocial interventions in the HIV risk reduction literature has resulted in a considerable evidence base on the efficacy of such approaches. However, the possible benefits of brief educational interventions have not received as much attention. The results of this systematic review suggest the importance of further research investigating the cost‐effectiveness of brief standard education interventions and their implementation in developing world contexts.
However, brief standard education interventions may not be appropriate for all people so further research should also seek to identify if there are sub‐groups of drug users (for example, people in formal drug treatment) likely to benefit from more intensive multi‐session psychosocial interventions.
As discussed above, there are a number of limitations to the literature in this field. Firstly, there is a lack of research on reducing HIV risk behaviours in drug users in developing countries. Secondly, a particularly important limitation of the interventions that we reviewed is that the great majority are focused on the individual, and thus make no provisions for social reinforcement of new behaviors over time. Interventions focusing on change with social networks have found promising results (for example, Latkin 2003). Developing mechanisms for long‐term social reinforement of behavior change is an area that deserves more attention in HIV behavior change research. A further limitation of the current literature concerns outcome assessment, our review of the literature suggests future studies require more objective measures of sexual and injection risk behaviour with longer follow up.
History
Protocol first published: Issue 2, 2008 Review first published: Issue 1, 2010
| Date | Event | Description |
|---|---|---|
| 26 February 2009 | Amended | Converted to new review format. |
Data and analyses
Comparison 1. Multi‐session psychosocial interventions versus Standard education.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Injection risk behaviour (3‐6 month follow up)) | 6 | 1044 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.04 [‐0.31, 0.23] |
| 2 Injection risk behaviour (follow up > 6months) | 1 | 73 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.81 [‐1.29, ‐0.33] |
| 3 safer injection behaviour (3‐6 month follow up) | 13 | 6562 | Risk Ratio (M‐H, Random, 95% CI) | 1.03 [0.95, 1.11] |
| 3.1 ITT | 4 | 3108 | Risk Ratio (M‐H, Random, 95% CI) | 1.01 [0.91, 1.11] |
| 3.2 Completers | 9 | 3454 | Risk Ratio (M‐H, Random, 95% CI) | 1.03 [0.93, 1.15] |
| 4 Sexual risk behaviour (3‐6 month follow up) | 6 | 1050 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.12 [‐0.33, 0.08] |
| 5 Sexual risk behaviour (> 6 months follow up) | 2 | 203 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.02 [‐0.25, 0.30] |
| 6 Safer sexual behaviour (3‐6 month follow up) | 14 | 3731 | Risk Ratio (M‐H, Random, 95% CI) | 1.05 [0.98, 1.13] |
| 6.1 ITT | 7 | 1541 | Risk Ratio (M‐H, Random, 95% CI) | 1.16 [0.95, 1.42] |
| 6.2 Completers | 7 | 2190 | Risk Ratio (M‐H, Random, 95% CI) | 1.02 [0.96, 1.10] |
| 7 Safer risk behaviour (> 6 month follow up) | 1 | 412 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.14 [0.89, 1.46] |
| 8 Injection and Sexual risk behaviour (combined) | 17 | 5763 | Risk Ratio (M‐H, Random, 95% CI) | 1.12 [1.04, 1.20] |
| 9 Injection and sexual risk behaviour (combined) | 11 | 1427 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.17 [‐0.37, 0.03] |
1.1. Analysis.
Comparison 1 Multi‐session psychosocial interventions versus Standard education, Outcome 1 Injection risk behaviour (3‐6 month follow up)).
1.2. Analysis.

Comparison 1 Multi‐session psychosocial interventions versus Standard education, Outcome 2 Injection risk behaviour (follow up > 6months).
1.3. Analysis.
Comparison 1 Multi‐session psychosocial interventions versus Standard education, Outcome 3 safer injection behaviour (3‐6 month follow up).
1.4. Analysis.

Comparison 1 Multi‐session psychosocial interventions versus Standard education, Outcome 4 Sexual risk behaviour (3‐6 month follow up).
1.5. Analysis.
Comparison 1 Multi‐session psychosocial interventions versus Standard education, Outcome 5 Sexual risk behaviour (> 6 months follow up).
1.6. Analysis.
Comparison 1 Multi‐session psychosocial interventions versus Standard education, Outcome 6 Safer sexual behaviour (3‐6 month follow up).
1.7. Analysis.
Comparison 1 Multi‐session psychosocial interventions versus Standard education, Outcome 7 Safer risk behaviour (> 6 month follow up).
1.8. Analysis.
Comparison 1 Multi‐session psychosocial interventions versus Standard education, Outcome 8 Injection and Sexual risk behaviour (combined).
1.9. Analysis.
Comparison 1 Multi‐session psychosocial interventions versus Standard education, Outcome 9 Injection and sexual risk behaviour (combined).
Comparison 2. Standard education versus Minimal Control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Safer injection risk behaviour (3‐6 month follow up) | 4 | 510 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.10 [0.92, 1.31] |
| 2 Safer sexual risk behaviour (3‐6 months follow up) | 2 | 296 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.07 [0.70, 1.64] |
| 3 Injection risk behaviour (3‐6 months follow up) | 3 | 262 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.06 [‐0.30, 0.19] |
| 4 Sexual risk behaviour (3‐6 months follow up) | 3 | 263 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.10 [‐0.34, 0.14] |
2.1. Analysis.
Comparison 2 Standard education versus Minimal Control, Outcome 1 Safer injection risk behaviour (3‐6 month follow up).
2.2. Analysis.
Comparison 2 Standard education versus Minimal Control, Outcome 2 Safer sexual risk behaviour (3‐6 months follow up).
2.3. Analysis.
Comparison 2 Standard education versus Minimal Control, Outcome 3 Injection risk behaviour (3‐6 months follow up).
2.4. Analysis.
Comparison 2 Standard education versus Minimal Control, Outcome 4 Sexual risk behaviour (3‐6 months follow up).
Comparison 3. Multi‐session psychosocial intervention versus Minimal Control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Sexual risk behaviour | 4 | 253 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.31 [‐0.56, ‐0.06] |
| 2 Injection risk behaviour | 2 | 107 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.05 [‐0.33, 0.43] |
| 3 Safer sexual behaviour | 1 | 420 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.34 [1.03, 1.73] |
3.1. Analysis.

Comparison 3 Multi‐session psychosocial intervention versus Minimal Control, Outcome 1 Sexual risk behaviour.
3.2. Analysis.
Comparison 3 Multi‐session psychosocial intervention versus Minimal Control, Outcome 2 Injection risk behaviour.
3.3. Analysis.
Comparison 3 Multi‐session psychosocial intervention versus Minimal Control, Outcome 3 Safer sexual behaviour.
Comparison 4. Multi‐session psychosocial intervention vs Standard education (sub‐group analysis by setting).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Injection and Sexual risk behaviour (combined) | 16 | 5618 | Risk Ratio (M‐H, Random, 95% CI) | 1.13 [1.05, 1.22] |
| 1.1 in formal drug treatment | 3 | 341 | Risk Ratio (M‐H, Random, 95% CI) | 1.42 [1.14, 1.77] |
| 1.2 not in formal drug treatment | 13 | 5277 | Risk Ratio (M‐H, Random, 95% CI) | 1.10 [1.02, 1.18] |
| 2 Injection and sexual risk behaviour (combined) | 11 | 1427 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.17 [‐0.37, 0.03] |
| 2.1 in formal drug treatment | 8 | 706 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.28 [‐0.44, ‐0.12] |
| 2.2 not in formal drug treatment | 3 | 721 | Std. Mean Difference (IV, Random, 95% CI) | 0.11 [‐0.32, 0.54] |
4.1. Analysis.

Comparison 4 Multi‐session psychosocial intervention vs Standard education (sub‐group analysis by setting), Outcome 1 Injection and Sexual risk behaviour (combined).
4.2. Analysis.
Comparison 4 Multi‐session psychosocial intervention vs Standard education (sub‐group analysis by setting), Outcome 2 Injection and sexual risk behaviour (combined).
Comparison 5. Multi‐session psychosocial intervention versus Standard education (subgroup analysis by gender).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Injection and Sexual risk behaviour (combined) | 17 | 5763 | Risk Ratio (M‐H, Random, 95% CI) | 1.12 [1.04, 1.20] |
| 1.1 mixed gender groups | 13 | 4995 | Risk Ratio (M‐H, Random, 95% CI) | 1.09 [1.01, 1.16] |
| 1.2 single gender groups | 4 | 768 | Risk Ratio (M‐H, Random, 95% CI) | 1.32 [1.12, 1.55] |
| 2 Injection and sexual risk behaviour (combined) | 11 | 1427 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.17 [‐0.37, 0.03] |
| 2.1 mixed gender groups | 6 | 1020 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.01 [‐0.25, 0.23] |
| 2.2 single gender groups | 5 | 407 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.38 [‐0.63, ‐0.12] |
5.1. Analysis.
Comparison 5 Multi‐session psychosocial intervention versus Standard education (subgroup analysis by gender), Outcome 1 Injection and Sexual risk behaviour (combined).
5.2. Analysis.
Comparison 5 Multi‐session psychosocial intervention versus Standard education (subgroup analysis by gender), Outcome 2 Injection and sexual risk behaviour (combined).
Comparison 6. Multi‐session psychosocial intervention vs Standard education (sub‐group analysis on HIV testing).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Injection and Sexual risk behaviour (combined) | 9 | 3428 | Risk Ratio (M‐H, Random, 95% CI) | 1.18 [1.04, 1.34] |
| 1.1 Reported HIV testing | 6 | 2615 | Risk Ratio (M‐H, Random, 95% CI) | 1.20 [1.02, 1.42] |
| 1.2 Not reported HIV testing | 3 | 813 | Risk Ratio (M‐H, Random, 95% CI) | 1.20 [0.87, 1.65] |
| 2 Injection and sexual risk behaviour (combined) | 11 | 1427 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.17 [‐0.37, 0.03] |
| 2.1 received HIV testing | 2 | 106 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.43 [‐0.82, ‐0.05] |
| 2.2 HIV testing not reported | 9 | 1321 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.13 [‐0.35, 0.09] |
6.1. Analysis.
Comparison 6 Multi‐session psychosocial intervention vs Standard education (sub‐group analysis on HIV testing), Outcome 1 Injection and Sexual risk behaviour (combined).
6.2. Analysis.
Comparison 6 Multi‐session psychosocial intervention vs Standard education (sub‐group analysis on HIV testing), Outcome 2 Injection and sexual risk behaviour (combined).
Comparison 7. Multi‐session psychosocial intervention vs Standard education (sensitivity analysis: study quality).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Injection and Sexual risk behaviour (combined) | 6 | 1456 | Risk Ratio (M‐H, Random, 95% CI) | 1.18 [1.05, 1.33] |
| 2 Injection and sexual risk behaviour (combined) | 9 | 830 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.17 [‐0.41, 0.07] |
7.1. Analysis.
Comparison 7 Multi‐session psychosocial intervention vs Standard education (sensitivity analysis: study quality), Outcome 1 Injection and Sexual risk behaviour (combined).
7.2. Analysis.
Comparison 7 Multi‐session psychosocial intervention vs Standard education (sensitivity analysis: study quality), Outcome 2 Injection and sexual risk behaviour (combined).
Characteristics of studies
Characteristics of included studies [ordered by study ID]
AVANTS2004.
| Methods | Random assignment of individuals | |
| Participants | 220 participants receiving MMT in USA (46% were also cocaine dependent) Mean Age: 37 years Sex: 151 Males and 68 Females |
|
| Interventions | 1. Psychoeducation:12 sessions of 90 min duration. Focused on information, motivation and behavioural skills 2. MI + Standard care: 1 session of MI followed by 2 hours counselling and case management per month |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | no blinding | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
BAKER1993.
| Methods | Random assignment of individuals | |
| Participants | 95 participants who were IDUs receiving MMT in Australia Mean age: 31 years Sex: 44 males, 51 females 6 participants were HIV positive |
|
| Interventions | 1. Psychoeducation: 6 sessions including MI and behavioural skills training 2. MI: 1 session of 60‐90 min duration 3. Standard care: standard advice and self‐help booklet |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | single blinded | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
BAKER1994.
| Methods | Random assignment of individuals | |
| Participants | 200 participants who were IDUs and attended a general medical centre in Australia Age: 29 years Sex: 159 males, 41 females |
|
| Interventions | 1. MI: 1 session for 30 mins 2. Standard care |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | single blinded received HIV testing |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
BAXTER1991.
| Methods | Random assignment of individuals | |
| Participants | 134 IDU participants in a US prison | |
| Interventions | 1. Psychoeducation: 6 sessions on injection and sexual risk reduction 2. Control |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | No information on blinding | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
COLON1993.
| Methods | Quasi‐randomised assignment of individuals (based on day of admission) | |
| Participants | 1866 participants from 4 communities in Puerto Rico Mean Age: 33 years Sex: 1478 males, 378 females |
|
| Interventions | 1. Psychoeducation: 3 sessions including street outreach and behavioural skills training 2. Control |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | no blinding received HIV testing |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
DEREN1995.
| Methods | Random assignment of individuals | |
| Participants | 1770 IDUs or their sex partners in USA Mean age: 35 years Sex: 71% males |
|
| Interventions | 1. Psychoeducation: 3 sessions 2. Standard education: 1 session |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | 994/1770 followed up No mention of blinding |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
DUSHAY2001.
| Methods | Quasi‐randomised assignment of individuals (every fifth [later third] African‐american or Puerto‐rican were assigned to standard) | |
| Participants | 539 Puerto‐Rican or African American participants | |
| Interventions | 1. Psychoeducation: 3 sessions adjusted to be culturally appropriate for either Puerto‐ricans or African Americans 2. Standard education: 2 sessions education on injection and sexual risk |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | No information on blinding | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
EL‐BASSEL 1995.
| Methods | Random assignment of individuals | |
| Participants | 145 incarcerated women in USA Mean age: 33 years |
|
| Interventions | 1. Psychoeducation:16 sessions of skill building 2. Standard education: 2 HIV/AIDS Information group sessions |
|
| Outcomes | Sexual risk behaviour | |
| Notes | No information on blinding | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
ELDRIDGE1997.
| Methods | Quasi‐randomised assignment of individuals (based on day of admission) | |
| Participants | 104 participants receiving treatment in the criminal justice system in the USA Mean age: 34 years Sex: all female |
|
| Interventions | 1. Psychoeducation: 6 sessions of behavioural skills training, education, 2. Standard education: 2 sessions |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | no information on blinding received HIV testing |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
GIBSON1999: Study 1.
| Methods | Random assignment of individuals | |
| Participants | 220 participants who had just completed opioid detoxification in USA Age range: 20‐49 Sex: 204 males, 91 females |
|
| Interventions | 1. Standard education: 1 session (50 mins) of education and problem solving 2. Self help booklet |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | no blinding HIV testing |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
GIBSON1999: Study 2.
| Methods | Random assignment of individuals | |
| Participants | 76 participants who had just completed opioid detoxification in USA Age range: 20‐49 years Sex: 44 males 22 females |
|
| Interventions | 1. Standard education: 1 session (50 mins) of education and problem solving 2. Control: short interview (15 mins) |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | No mention of blinding HIV testing |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
HARRIS1998.
| Methods | Random assignment of individuals | |
| Participants | 204 participants who received MMT in USA Mean age: 36 years Sex: all females |
|
| Interventions | 1. Psychoeducation: 16 sessions behavioural skills intervention specifically designed for women 2. Standard care: standard services within MMT |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | No blinding | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
KOTRANSKI1998.
| Methods | Quasi‐randomised assignment of individuals | |
| Participants | 417 IDU participants from USA Mean age: 39 years Sex: 265 males, 152 females |
|
| Interventions | 1. Psychoeducation: 3 sessions behavioural skills 2. Standard education: 2 sessions |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | No mention of blinding received HIV testing |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
MALOW1994.
| Methods | Random assignment of individuals | |
| Participants | 152 participants from USA who were dependent on crack cocaine Mean age: 35 years Sex: all males |
|
| Interventions | 1. Psychoeducation: 3 sessions on behavioural skills, stress reduction 2. Control: same content but minimal participant‐therapist interaction |
|
| Outcomes | Sexual risk behaviour | |
| Notes | No mention of blinding | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
MANDELL 1994.
| Methods | Random assignment of individuals | |
| Participants | 105 participants from USA not in formal drug treatment Mean age: 34 years Sex: 90 Males, 15 females |
|
| Interventions | 1. Brief intervention: 1 hour session 2. Minimal intervention: 15 mins information |
|
| Outcomes | Injection risk behaviour | |
| Notes | No mention of blinding received HIV testing |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
MARGOLIN2003.
| Methods | Random assignment of individuals | |
| Participants | 90 participants receiving MMT in USA Mean age: 41 years Sex: 63 males, 27 females |
|
| Interventions | 1. Psychoeducation: 6 sessions behavioural skills and MI 2. Standard care: group counselling |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | No mention of blinding | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
NADR: Site 1.
| Methods | Quasi‐randomised assignment of individuals | |
| Participants | 531 participants not in drug treatment in USA Mean age: 35 years Sex: 361 males, 170 females |
|
| Interventions | 1. Psychoeducation 2. Standard education |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | No mention of blinding | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
NADR: Site 10.
| Methods | Quasi‐randomised assignment of individuals | |
| Participants | 131 participants not in drug treatment in USA Mean age: 34 years Sex: 96 males, 35 females |
|
| Interventions | 1. Psychoeducation 2. Standard education |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | No mention of blinding | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
NADR: Site 14.
| Methods | Quasi‐randomised assignment of individuals | |
| Participants | 143 participants not in drug treatment in USA Mean age: 35 years Sex: 120 males, 23 females |
|
| Interventions | 1. Psychoeducation 2. Standard education |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | No mention of blinding | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
NADR: Site 16.
| Methods | Quasi‐randomised assignment of individuals | |
| Participants | 343 participants not in drug treatment in the USA Mean age: 35 years Sex: 244 males, 99 females |
|
| Interventions | 1. Psychoeducation 2. Standard education |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | No mention of blinding | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
NADR: Site 17.
| Methods | Quasi‐randomised assignment of individuals | |
| Participants | 884 participants not in drug treatment in the USA Mean age: 34 years Sex: 628 males, 256 females |
|
| Interventions | 1. Psychoeducation 2. Standard education |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | No mention of blinding Very high attrition: 76% therefore not included in meta‐analysis |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
NADR: Site 18.
| Methods | Quasi‐randomised assignment of individuals | |
| Participants | 177 participants not in drug treatment in the USA Mean age: 38 years Sex: 124 males, 53 females |
|
| Interventions | 1. Psychoeducation 2. Standard education |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | No mention of blinding Very high attrition: 93% therefore not included in the meta‐analysis |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
NADR: Site 19.
| Methods | Quasi‐randomised assignment of individuals | |
| Participants | 317 participants not in drug treatment in the USA Mean age: 34 years Sex: 225 males, 92 females |
|
| Interventions | 1. Psychoeducation 2. Standard education |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | No mention of blinding | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
NADR: Site 20.
| Methods | Quasi‐randomised assignment of individuals | |
| Participants | 276 participants not in drug treatment in the USA Mean age: 33 years Sex: 182 males, 94 females |
|
| Interventions | 1. Psychoeducation 2. Standard education |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | No mention of blinding | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
NADR: Site 4.
| Methods | Quasi‐randomised assignment of individuals | |
| Participants | 540 participants not in drug treatment in the USA Mean age: 37 years Sex: 357 males, 183 females |
|
| Interventions | 1. Psychoeducation 2. Standard education |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | No mention of blinding | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
ONEILL1996.
| Methods | Random assignment of individuals | |
| Participants | 92 participants who were IDUs and receiving MMT in Australia Mean age: 26 years Sex: all females |
|
| Interventions | 1. Psychoeducation: MI (1 session) and behavioural skills training (5 sessions 2. Standard care |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | Single blinding | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
ROBLES2004.
| Methods | Random assignment of individuals | |
| Participants | 557 participants who were IDUs and over 18 years old living in Puerto Rico. Mean age: 34.4% under 25 years, 36.6% 25‐34 years, 29.0% over 35 years Sex: 498 males, 59 females |
|
| Interventions | 1. Psychoeducation: 6 sessions, including MI and behavioural skills training. Each session was followed by case management . 2. Standard education: 2 sessions of education/discussion on HIV/AIDS as a disease, discussion of safe needle and safe sex skills, offer of HIV test |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | No mention of blinding HIV testing |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
SCHILLING1991.
| Methods | Random assignment of individuals | |
| Participants | 91 participants receiving MMT in USA Age range: 21‐42 years Sex: all females |
|
| Interventions | 1. Psychoeducation: 5 sessions on education and behavioural skills 2. Standard education: standard information provided at clinic |
|
| Outcomes | Sexual risk behaviour | |
| Notes | No mention of blinding | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
SIEGAL1995.
| Methods | Random assignment of individuals | |
| Participants | 381 participants recruited in a needle exchange programme in USA Mean age: 37 years Sex: 282 males, 99 females |
|
| Interventions | 1. Psychoeducation: 4 sessions on education and behavioural skills 2. Enhanced Standard care: 1 session education and behavioural skills training |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | No mention of blinding HIV testing |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
SORENSEN1994: Detox.
| Methods | Random assignment of individuals | |
| Participants | 60 participants receiving opiate detoxification in USA | |
| Interventions | 1. Psychoeducation: 2 sessions (first for4 hours and last for 2hours) education and behavioural skills training 2. Control |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | No mention of blinding | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Low risk | A ‐ Adequate (used sealed envelopes) |
SORENSEN1994: MMT.
| Methods | Random assignment of individuals | |
| Participants | 50 participants receiving MTT in USA Mean age: 40 years Sex: 33 males and 17 females |
|
| Interventions | 1. Psychoeducation: 3 sessions education and behavioural skills training 2. Control |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | No mention of blinding | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Low risk | A ‐ Adequate (used sealed envelopes) |
STEIN2002.
| Methods | Random assignment of individuals | |
| Participants | 109 participants from USA who were IDUs and also exhibited hazardous or harmful alcohol use Mean age: 36 years Sex: 68 males 41 females |
|
| Interventions | 1. Brief intervention: 2 sessions of motivational interviewing 2. Control |
|
| Outcomes | Injection risk behaviour | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | B ‐ Unclear |
STERK2003.
| Methods | Random assignment of individuals | |
| Participants | 68 participants who were IDUs in USA Mean age: 41 years Sex: all females |
|
| Interventions | 1. Psychoeducation (motivation‐focused): 4 sessions on education and reducing ambivalence 2. Psychoeducation(behavioural focused): 4 sessions on education and behavioural skills training 3. Standard education |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | No blinding HIV testing |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
TUCKER2004.
| Methods | Random assignment of individuals | |
| Participants | 145 participants who were IDUs in Australia Mean age:31 years Sex: 84 males, 21 females |
|
| Interventions | 1. MI: 1 session 2. self help booklet | |
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | Single blinding | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Low risk | A ‐ Adequate (used sealed envelopes) |
WECHSBERG2004.
| Methods | Random assignment of individuals | |
| Participants | 620 African‐American women participants who
were crack cocaine dependent Mean age: 37 years Sex: all females |
|
| Interventions | 1. Psychoeducation: 4 sessions on education and behavioural skills training 2. Standard education 3. Waitlist |
|
| Outcomes | Injection risk behaviour Sexual risk behaviour |
|
| Notes | No mention of blinding HIV testing |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | D ‐ Not used |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Boatler 1994 | pre‐post analysis with inadequate controls |
| Booth 1996 | aim of intervention not focused on HIV risk prevention |
| Booth 2004 | no extractable data |
| CDC 1999 | intervention conducted at the community level |
| Choopanya 2003 | pre‐post analysis with inadequate controls |
| Compton 1998 | not relevant comparison |
| Compton 2000 | not relevant comparison |
| Conrad 1998 | primarily addressing alcohol misuse |
| El‐Bassel 2005 | no adequate controls |
| Epstein2003 | not primarily aimed at reducing HIV risk behaviours |
| Heil 2005 | no behavioural outcomes |
| Hershberger 2003 | not RCT |
| Kwiatkowski 1999 | not analysed by original groups |
| Latkin 1996 | structural interventions |
| Latkin 2003 | structural interventions |
| Linderberg 2002 | not primarily addressing people who misuse drugs |
| Malow 1992 | did not directly assess behavioural outcomes |
| Martin 2001 | did not assess required behavioural outcomes |
| McCoy 1996 | no extractable data |
| McCusker 1992 | no extractable data |
| Rhodes 1994 | no clear information on group assignment |
| Sherman 2006 | no control group |
| Simpson 1994 | no extractable data for intervention vs control |
| St Lawrence 1997 | no behavioural outcomes |
| Sterk 2003 | no extractable data |
Contributions of authors
NM: contributed to design of review, assessed studies for inclusion, quality appraisal of studies, extracted data and conducted analysis, wrote first draft
RL: contributed to design of review, assessed studies for inclusion, quality appraisal of studies, extracted data, commented on draft
DDJ: contributed to design of review, added additional content to the draft and commented on analysis
SP: contributed to design of review, resolved differences in interpretation between NM and RL in applying the inclusion criteria, commented on draft
Sources of support
Internal sources
National Institute of Health and Clinical Excellence, UK.
External sources
No sources of support supplied
Declarations of interest
None known
New
References
References to studies included in this review
AVANTS2004 {published data only}
- Avants, K, Margolin, A, Usubiaga, M.H, Doebrick. C. Targeting HIV‐related outcomes with intravenous drug users maintained on methadone: a randomized clinical trial of a harm reduction group therapy.. Journal of Substance Abuse Treatment 2004;26:67‐78. [DOI] [PubMed] [Google Scholar]
BAKER1993 {published data only}
- Baker, A, Heather, N, Wodak, A, Dixon, J, & Holt, P. Evaluation of a cognitive‐behavioural intervention for HIV prevention among injecting drug users.. AIDS 1993;7:247‐256. [DOI] [PubMed] [Google Scholar]
BAKER1994 {published data only}
- Baker, A, Kochan, N, Dixon, J, Heather, N, & Wodak, A. Controlled evaluation of a brief intervention for HIV prevention among injecting drug users not in treatment.. AIDS Care 1994;6:559‐570. [DOI] [PubMed] [Google Scholar]
BAXTER1991 {published data only}
- Baxter S. AIDS education in the jail setting. Crime and Delinquency 1991;37:48‐63. [Google Scholar]
COLON1993 {published data only}
- Colon M, Robles R, Freeman D, Matos T. Effects of a HIV risk reduction education program among injection drug users in Puerto Rico.. Puerto Rico Health Sciences Journal 1993;12:27‐34. [PubMed] [Google Scholar]
DEREN1995 {published data only}
- Deren S, Rees Davis W, Beadsley M, et al. Outcomes of a risk‐reduction intervention with high risk populations: the Harlem AIDS project. AIDS Education & Prevention 1995;7:379‐390. [PubMed] [Google Scholar]
DUSHAY2001 {published data only}
- Dushay RA, Singer M, Weeks MR, et al. Lowering HIV risk among ethnic minority drug users: comparing culturally targetted intervention to a standard intervention. American Journal of Drug and Alcohol Abuse 2001;27:501‐524. [DOI] [PubMed] [Google Scholar]
EL‐BASSEL 1995 {published data only}
- Bassell N, Ivanoff A, Schilling RF, et al. Preventing HIV/AIDS in drug abusing incarcerated women through skill building and social support enhancement: preliminary outcomes. Social Work Research 1995;19:131‐141. [PubMed] [Google Scholar]
ELDRIDGE1997 {published data only}
- Eldridge, G.D, check reference. Evaluation of the HIV risk reduction intervention for women entering inpatient substance abuse treatment. AIDS Education & Prevention 1997;9:62‐76. [PubMed] [Google Scholar]
GIBSON1999: Study 1 {published data only}
- Gibson, R, Lovelle‐Drache, J, Young, M, Hudes, E.S, Sorensen. J.L. Effectiveness of brief counseling in reducing HIV risk behavior in injecting drug users: Final results of randomized trials of counseling with and without HIV testing. AIDS and Behavior 1999;3:3‐12. [Google Scholar]
GIBSON1999: Study 2 {published data only}
- Gibson, R, Lovelle‐Drache, J, Young, M, Hudes, E.S, Sorensen. J.L. Effectiveness of brief counseling in reducing HIV risk behavior in injecting drug users: Final results of randomized trials of counseling with and without HIV testing. AIDS and Behavior 1999;3:3‐12. [Google Scholar]
HARRIS1998 {published data only}
- Harris, R.M, Bausell, R.B, Scott, D.E, Hetherington, S.E, & Kavanagh, K.H. An intervention for changing high‐risk HIV behaviors of African American drug‐dependent women. Research in Nursing & Health 1998;21:239‐250. [DOI] [PubMed] [Google Scholar]
KOTRANSKI1998 {published data only}
- Kotranski, L, Semaan, S, Collier, K, Lauby, J, Halbert, J, & Feighan, K. Effectiveness of an HIV risk reduction counseling intervention for out‐of‐treatment drug users. AIDS Education & Prevention 1998;10:19‐33. [PubMed] [Google Scholar]
MALOW1994 {published data only}
- Malow, R. M, West, J. A, Corrigan, S. A, Pena, J. M, & Cunningham, S. C. Outcome of psychoeducation for HIV risk reduction.. AIDS Education and Prevention 1994;6:113‐125. [PubMed] [Google Scholar]
MANDELL 1994 {published data only}
- Mandell W, Vlahor D, Latkin CA, et al. Changes in HIV risk behaviors among counseled injecting drug users. Journal of Drug Issues 1994;24:555‐567. [Google Scholar]
MARGOLIN2003 {published data only}
- Margolin, A, Avants, S. K, Warburton, L. A, Hawkins, K. A, Shi. J. A randomized clinical trial of a manual‐guided risk reduction intervention for HIV‐positive injection drug users. Health Psychology 2003;22:223‐228. [PubMed] [Google Scholar]
NADR: Site 1 {published data only}
- Stephens RC, Simpson DD, Coyle SL, et al. Comparative effectiveness of NADR interventions. In: Brown BS, Meschner GM editor(s). Handbook on risk of AIDS: injection drug users and their sexual partners. Westport: CT: Greenwood Press, 1993. [Google Scholar]
NADR: Site 10 {published data only}
- Stephens RC, Simpson DD, Coyle SL, et al. Comparative effectiveness of NADR interventions. In: Brown BS, Meschner GM editor(s). Handbook on risk of AIDS: injection drug users and their sexual partners. Westport: CT: Greenwood Press, 1993. [Google Scholar]
NADR: Site 14 {published data only}
- Stephens RC, Simpson DD, Coyle SL, et al. Comparative effectiveness of NADR interventions. In: Brown BS, Meschner GM editor(s). Handbook on risk of AIDS: Injection drug users and their sexual partners. Westport, CT: Greenwood Press, 1993. [Google Scholar]
NADR: Site 16 {published data only}
- Stephens RC, Simpson DD, Coyle SL, et al. Comparative effectiveness of NADR interventions. In: Brown BS, Meschner GM editor(s). Handbook on risk of AIDS: Injection drug users and their sexual partners. Westport, CT: Greenwood Press, 1993. [Google Scholar]
NADR: Site 17 {published data only}
- Stephens RC, Simpson DD, Coyle SL, et al. Comparative effectiveness of NADR interventions. In: Brown BS, Meschner GM editor(s). Handbook on risk of AIDS: Injection drug users and their sexual partners. Westport, CT: Greenwood Press, 1993. [Google Scholar]
NADR: Site 18 {published data only}
- Stephens RC, Simpson DD, Coyle SL, et al. Comparative effectiveness of NADR interventions. In: Brown BS, Meschner GM editor(s). Handbook on risk of AIDS: Injection drug users and their sexual partners. Westport, CT: Greenwood Press, 1993. [Google Scholar]
NADR: Site 19 {published data only}
- Stephens RC, Simpson DD, Coyle SL, et al. Comparative effectiveness of NADR interventions. In: Brown BS, Meschner GM editor(s). Handbook on risk of AIDS: Injection drug users and their sexual partners. Westport, CT: Greenwood Press, 1993. [Google Scholar]
NADR: Site 20 {published data only}
- Stephens RC, Simpson DD, Coyle SL, et al. Comparative effectiveness of NADR interventions. In: Brown BS, Meschner GM editor(s). Handbook on risk of AIDS: Injection drug users and their sexual partners. Westport, CT: Greenwood Press, 1993. [Google Scholar]
NADR: Site 4 {published data only}
- Stephens RC, Simpson DD, Coyle SL, et al. Comparative effectiveness of NADR interventions. In: Brown BS, Meschner GM editor(s). Handbook on risk of AIDS: Injection drug users and their sexual partners. Westport, CT: Greenwood Press, 1993. [Google Scholar]
ONEILL1996 {published data only}
- O'Neill, K, Baker, A, Cooke, M, Collins, E, Heather, N, & Wodak, A. Evaluation of a cognitive‐behavioural intervention for pregnant injecting drug users at risk of HIV infection. Addiction 1996;91:1115‐1125. [DOI] [PubMed] [Google Scholar]
ROBLES2004 {published data only}
- Robles RR, Reyes JC, Colon HM, et al. Effects of combined counseling and case management to reduce HIV risk behaviors among Hispanic drug injectors in Puerto Rico: a randomized controlled study. Journal of Substance Abuse Treatment 2004;27:145‐152. [DOI] [PubMed] [Google Scholar]
SCHILLING1991 {published data only}
- Schilling, R. F, El‐Bassel, N, Schinke, S. P, Gordon, K, & Nichols, S. Building skills of recovering women drug users to reduce heterosexual AIDS transmission. Public Health Reports 1991;106:297‐304. [PMC free article] [PubMed] [Google Scholar]
SIEGAL1995 {published data only}
- Siegal, H. A, Falck, R. S, Carlson, R. G, & Wang, J. Reducing HIV needle risk behaviors among injection‐drug users in the Midwest: an evaluation of the efficacy of standard and enhanced interventions. AIDS Education & Prevention 1995;7:308‐319. [PubMed] [Google Scholar]
SORENSEN1994: Detox {published data only}
- Sorensen JL, London J, Heitzmann C, Gibson DR, Morales ES, Dumontet R, et al. Psychoeducation group approach: HIV risk reduction in drug users. AIDS Education & Prevention 1994;6:95‐112. [PubMed] [Google Scholar]
SORENSEN1994: MMT {published data only}
- Sorensen, J. L, London, J, Heitzmann, C, Gibson, D. R. Morales, E. S, Dumontet, R, et al. Psychoeducational group approach: HIV risk reduction in drug users. AIDS Education & Prevention 1994;6:95‐112. [PubMed] [Google Scholar]
STEIN2002 {published data only}
- Stein MD, Anderson B, Charuvastra A, Maksad J, Friedmann PD. A brief intervention for hazardous drinkers in a needle exchange program. Journal of Substance Abuse Treatment 2002;22(1):23‐31. [DOI] [PubMed] [Google Scholar]
STERK2003 {published data only}
- Sterk, C. E, Theall, K. P, Elifson, K. W, Kidder. D. HIV risk reduction among African‐American women who inject drugs: a randomized controlled trial. AIDS & Behavior 2003;7:73‐86. [DOI] [PubMed] [Google Scholar]
TUCKER2004 {published data only}
- Tucker, T, Fry, C. L, Lintzeris, N, Baldwin, S, Ritter, A, Donath, S, et al. Randomized controlled trial of a brief behavioural intervention for reducing hepatitis C virus risk practices among injecting drug users. Addiction 2004;99:1157‐1166. [DOI] [PubMed] [Google Scholar]
WECHSBERG2004 {published data only}
- Wechsberg, W. M, Lam, W. K, Zule, W. A, & Bobashev, G. Efficacy of a woman‐focused intervention to reduce HIV risk and increase self‐sufficiency among African American crack abusers. American Journal of Public Health 2004;94:1165‐1173. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies excluded from this review
Boatler 1994 {published data only}
- Boatler JF, Knight K, Simpson DD. Assessment of an AIDS intervention program during drug abuse treatment. Journal of Substance Abuse Treatment 1994;11(4):367‐372. [DOI] [PubMed] [Google Scholar]
Booth 1996 {published data only}
- Booth RE, Crowley TJ, Zhang Y. Substance abuse treatment entry, retention and effectiveness: out‐of‐treatment opiate injection drug users. Drug & Alcohol Dependence 1996;42(1):11‐20. [DOI] [PubMed] [Google Scholar]
Booth 2004 {published data only}
- Booth RE, Corsi KF, Mikulich‐Gilbertson SK. Factors associated with methadone maintenance treatment retention among street‐recruited injection drug users. Drug Alcohol Depend 2004;74(2):177‐185. [DOI] [PubMed] [Google Scholar]
CDC 1999 {published data only}
- Centre of Disease Control. Community‐Level HIV intervention in 5 cities: final outcome data from CDC AIDS community demonstration projects. American Journal of Public Health 1999;89:336‐345. [DOI] [PMC free article] [PubMed] [Google Scholar]
Choopanya 2003 {published data only}
- Choopanya K, Des J, Vanichseni S, Mock PA, Kitayaporn D, Sangkhum U, Prasithiphol B, Hiranrus K, van GF, Tappero JW, Mastro TD. HIV risk reduction in a cohort of injecting drug users in Bangkok, Thailand. Journal of Acquired Immune Deficiency Syndromes: JAIDS 2003;33(1):88‐95. [DOI] [PubMed] [Google Scholar]
Compton 1998 {published data only}
- Compton WM, Cottler LB, Spitznagel EL, Abdallah AB, Gallagher T. Cocaine users with antisocial personality improve HIV risk behaviors as much as those without antisocial personality. Drug & Alcohol Dependence 1998;49(3):239‐247. [DOI] [PubMed] [Google Scholar]
Compton 2000 {published data only}
- Compton WM, Cottler LB, Ben‐Abdallah A, Cunningham‐Williams R, Spitznagel EL. The effects of psychiatric comorbidity on response to an HIV prevention intervention. Drug & Alcohol Dependence 2000;58(3):247‐257. [PubMed] [Google Scholar]
Conrad 1998 {published data only}
- Conrad KJ, Hultman CI, Pope AR, Lyons JS, Baxter WC, Daghestani AN, Lisiecki JPJ, Elbaum PL, McCarthy MJ, Manheim LM. Case managed residential care for homeless addicted veterans. Results of a true experiment. Medical Care 1998;36(1):40‐53. [DOI] [PubMed] [Google Scholar]
El‐Bassel 2005 {published data only}
- El‐Bassel N, Gilbert L, Wu E, Go H, Hill J. HIV and intimate partner violence among methadone‐maintained women in New York City. Social Science & Medicine 2005;61(1):171‐183. [DOI] [PubMed] [Google Scholar]
Epstein2003 {published data only}
- Epstein, D.H, Hawkins, W.E, Covi, L, Umbricht, A, & Preston, K.L. Cognitive‐behavioral therapy plus contingency management for cocaine use: findings during treatment and across 12‐month follow‐up. Psychology of Addictive Behaviors 2003;17:73‐82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gibson, R, Lovelle‐Drache, J, Young, M, Hudes, E.S, Sorensen. J.L. Effectiveness of brief counseling in reducing HIV risk behavior in injecting drug users: Final results of randomized trials of counseling with and without HIV testing. AIDS and Behavior 1999;3. [Google Scholar]
Heil 2005 {published data only}
- Heil SH, Sigmon SC, Mongeon JA, Higgins ST. Characterizing and improving HIV/AIDS knowledge among cocaine‐dependent outpatients. Experimental & Clinical Psychopharmacology 2005;13(3):238‐243. [DOI] [PubMed] [Google Scholar]
Hershberger 2003 {published data only}
- Hershberger SL, Wood MM, Fisher DG. A cognitive‐behavioral intervention to reduce HIV risk behaviors in crack and injection drug users. AIDS & Behavior 2003;7(3):229‐243. [DOI] [PubMed] [Google Scholar]
Kwiatkowski 1999 {published data only}
- Kwiatkowski CF, Stober DR, Booth RE, Zhang Y. Predictors of increased condom use following HIV intervention with heterosexually active drug users. Drug & Alcohol Dependence 1999;54(1):57‐62. [DOI] [PubMed] [Google Scholar]
Latkin 1996 {published data only}
- Latkin CA, Mandell W, Vlahov D, et al. The long‐term outcome of a personal network‐oriented HIV prevention intervention for injection drug users: the SAFE study. American Journal of Community Psychology 1996;24:341‐364. [DOI] [PubMed] [Google Scholar]
Latkin 2003 {published data only}
- Latkin CA, Sherman S, Knowlton A. HIV prevention among drug users: outcome of a network‐oriented peer outreach intervention. Health Psychology 2003;23:332‐339. [DOI] [PubMed] [Google Scholar]
Linderberg 2002 {published data only}
- Linderberg CS, Solorzano RM, Bear D, Strickland O, Galvis C, Pittman K. Reducing substance use and risky sexual behavior among young, low‐income, Mexican‐American women: comparison of two interventions. Applied Nursing Research 2002;15(3):137‐148. [DOI] [PubMed] [Google Scholar]
Malow 1992 {published data only}
- Malow RM, Corrigan SA, Pena JM, Calkins AM, Bannister TM. Effectiveness of a psychoeducational approach to HIV risk behavior reduction. Psychology of Addictive Behaviors 1992;6(2):120‐125. [Google Scholar]
Martin 2001 {published data only}
- Martin J, Sabugal GM, Rubio R, Sainz‐Maza M, Blanco JM, Alonso JL, Dominguez J. Outcomes of a health education intervention in a sample of patients infected by HIV, most of them injection drug users: possibilities and limitations. AIDS Care 2001;13(4):467‐473. [DOI] [PubMed] [Google Scholar]
McCoy 1996 {published data only}
- McCoy CB, Wetherby NL, Metsch LR, et al. Effectiveness of HIV interventions among crack users. Drugs and Society 1996;9:137‐154. [Google Scholar]
McCusker 1992 {published data only}
- McCusker J, Stoddard AM, Zapka JG, Morrison CS, Zorn M, Lewis BF. AIDS education for drug abusers: evaluation of short‐term effectiveness. American Journal of Public Health 1992;82(4):533‐540. [DOI] [PMC free article] [PubMed] [Google Scholar]
Rhodes 1994 {published data only}
- Rhodes F, Malotte CK. HIV risk intervention for active drug users: experience and prospects. In: Oskamp S, Thompson SE editor(s). Understanding and preventing HIV risk behavior, safer sex and drug use. Thousand Oaks, California: Sage, 1996. [Google Scholar]
Sherman 2006 {published data only}
- Sherman SG, German D, Cheng Y, Marks M, Bailey‐Kloche M. The evaluation of the JEWEL project: An innovative economic enhancement and HIV prevention intervention study targeting drug using women involved in prostitution. AIDS Care 2006;18(1):01. [DOI] [PubMed] [Google Scholar]
Simpson 1994 {published data only}
- Simpson DD, Camacho LM, Vogtsberger KN, Williams ML, Stephens RC, Jones A, Watson DD. Reducing AIDS risks through community outreach interventions for drug injectors. Psychology of Addictive Behaviors 1994;8(2):86‐101. [Google Scholar]
St Lawrence 1997 {published data only}
- Lawrence JS, Eldridge GD, Shelby MC, et al. HIV risk reduction for incarcerated women: A comparison of brief interventions based on two theoretical models. Journal of Consulting and Clinical Psychology 1997;65:504‐509. [DOI] [PubMed] [Google Scholar]
Sterk 2003 {published data only}
- Sterk CE, Theall KP, Elifson KW. Who's getting the message? Intervention response rates among women who inject drugs and/or smoke crack cocaine. Preventive Medicine 2003;37(2):119‐128. [DOI] [PubMed] [Google Scholar]
Additional references
Aceijas 2004
- Aceijas C, Stimson GV, Hickman M, Rhodes T. Global overview of injecting drug use and HIV infection among injecting drug users.. AIDS 2004;18:2295‐2303. [DOI] [PubMed] [Google Scholar]
Copenhaver 2006
- Copenhaver M, Johnson BT, Ching‐Lee I, et al. Behavioral HIV risk reduction among people who inject drugs: meta‐analytic evidence of efficacy.. Journal of Substance Abuse Treatment 2006;31:163‐171. [DOI] [PMC free article] [PubMed] [Google Scholar]
Des Jarlais 1995
- Jarlais DC, Friedman SR, Friedmann P, Wenston J, Sotheran JL, Choopanya K, Vanichseni S, Raktham S, Goldberg D, Frischer M. HIV/AIDS‐related behavior change among injecting drug users in different national settings. AIDS 1995;9:611‐617. [DOI] [PubMed] [Google Scholar]
Des Jarlais2000
- Jarlais D. Structural interventions to reduce HIV transmission among injecting drug users. AIDS 2000;14(Supplement 1):S41‐S46. [DOI] [PubMed] [Google Scholar]
EMCCDA2007
- EMCCDA. Annual report 2007: The state of the drug problem in Europe. Luxembourg: Office for the official publication of the European Communities, 2007. [Google Scholar]
Gibson 2001
- Gibson DR, Flynn NM, Perales D. Effectiveness of syringe exchange programs in reducing HIV risk behavior and HIV seroconversion among injecting drug users.. AIDS 2001;15:1329‐1341. [DOI] [PubMed] [Google Scholar]
Institute of Medicine 2006
- Institute of Medicine. Preventing HIV Infection among Injecting Drug Users in High Risk Countries: An Assessment of the Evidence Prevention of HIV infection among injecting drug users in high risk countries: An assessment of the evidence. Washington DC: Institute of Medicine, 2006. [Google Scholar]
Judd 2005
- Judd A, Hickman M, Jones S, et al. Incidence of hepatitis C virus and HIV among new injecting drug users in London: prospective cohort study.. BMJ 2005;330:24‐25. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ksobiech 2003
- Ksobiech K. A meta‐analysis of needle sharing, lending, and borrowing behaviors of needle exchange attendees. AIDS Education and Prevention 2003;15:257‐268. [DOI] [PubMed] [Google Scholar]
Malow 1994
- Malow, R. M, West, J. A, Corrigan, S. A, Pena, J. M, & Cunningham, S. C. Outcome of psychoeducation for HIV risk reduction.. AIDS Education and Prevention 1994;6:113‐125. [PubMed] [Google Scholar]
Mathers 2008
- Mathers BM, Degenhardt L, Phillips B, et al. Global epidemiology of injecting drug use and HIV among people who inject drugs: a systematic review. Lancet 2008;372:1733‐1745. [DOI] [PubMed] [Google Scholar]
Musto 1993
- Musto D. The American Disease: Origins of narcotic control. New Haven: Yale University Press, 1973. [Google Scholar]
National Institute for Health 1997
- National Institute for Health. Interventions to prevent HIV risk behaviors. NIH Consensus Development Statement 1997;15:1‐41. [PubMed] [Google Scholar]
NICE 2005
- NICE. Guideline development methods: information for national collaborating centres and guideline developers.. London: NICE, 2005. [Google Scholar]
Semaan 2002
- Semaan S, Jarlais DC, Sogolow E, et al. A meta‐analysis of the effect of HIV prevention interventions on the sex behaviors of drug users in the United States. Journal of Acquired Immune Deficiency Syndromes & Human Retrovirology 2002;30(Supplement 1):S73‐93. [PubMed] [Google Scholar]
Wodak 2005
- Wodak A, Cooney A. Effectivenesss of sterile needle and syringe exchange programmes. International Journal of Drug Policy 2005;16S:S31‐S44. [Google Scholar]