

In his Nobel laureate address, Joseph Goldstein referred to cholesterol as the most decorated molecule in history,1 and certainly there is a lot of evidence relating the levels of total and low-density lipoprotein (LDL) cholesterol to the risk of vascular disease. But does that mean that they will remain tomorrow in the central position that they occupy today? We believe that the answer may well be No, because plasma apolipoprotein B (apo B) appears to be a better marker of the risk due to the atherogenic lipoproteins, namely, very low-density lipoprotein (VLDL) and LDL.
The latest critical piece of evidence comes from the AFCAPS/TexCAPS study, which tested whether treatment with lovastatin would reduce the frequency of coronary events in a large asymptomatic group of individuals who did not have marked hypercholesterolemia, many of whom also had low levels of high-density lipoprotein (HDL) cholesterol.2 Several of these researchers subsequently considered which lipid variables predicted clinical benefit before and during therapy.3 LDL cholesterol was not the most informative parameter. Rather, the most valuable turned out to be apo B. The authors write, “Apo B was in fact the single most significant and consistent lipid measurement to predict risk at both baseline and on-treatment.” Because apo B is neither generally measured nor familiar to most Canadian practitioners, we believe that their findings, taken with the other evidence that is available, merit serious attention.
Within a population, as the levels of cholesterol rise, so does the risk of coronary disease and, unquestionably, individuals with very high levels of cholesterol are at very high risk. However, only a small portion of the population have very high levels of cholesterol. It is not generally appreciated that a major finding of the Framingham study is that most cases of premature vascular disease occurred in individuals with levels of total and LDL cholesterol that were indistinguishable from those of individuals who did not develop premature disease.4 Moreover, except for those individuals with extremely high values, only a minority at any level will develop premature disease.5 Thus, cholesterol is a good marker of risk within a large group but, for the most part, is a relatively poor marker of risk for its individual members.
One result of this paradox has been a successive lowering of the definition of “high” cholesterol, with the desirable level now being designated as a less than 5.2 mmol/L of total cholesterol and less than 3.4 mmol/L of LDL cholesterol. The drawback to this approach is that about 50% of our population will automatically be designated “hypercholesterolemic.”6 Even so, 40% of individuals with premature vascular disease will have levels of total and LDL cholesterol below those of the 50th percentile of the population.7 Measurement of HDL cholesterol and triglycerides does improve the recognition of risk, with lower levels of the former and higher levels of the latter being associated with an increased likelihood of disease. But the questions remain: Can we do better to recognize those at risk and — equally important — can we make clinical practice simpler?
The liver secretes a triglyceride-rich lipoprotein, VLDL, which by the removal of most of its triglyceride is converted to a smaller cholesterol-rich lipoprotein, LDL. The biologic half-life of an LDL particle is at least 9 times longer than that of a VLDL particle and, therefore, there are always 9 times more LDL particles than VLDL particles (Fig. 1). Because each VLDL and LDL particle contains one molecule of apo B, measuring plasma apo B measures exactly the total number of VLDL and LDL particles, 90% of which are LDL.8 In contrast, because LDL particles differ substantially from one another in the amount of cholesterol they contain, total and LDL cholesterol are imprecise measures of the number of apo B particles. Measuring apo B, therefore, provides a direct estimate of the total number of atherogenic particles. The measurement of plasma apo B is standardized, automated and inexpensive.9 It can be performed on nonfasting samples, and population reference values are now available.10,11
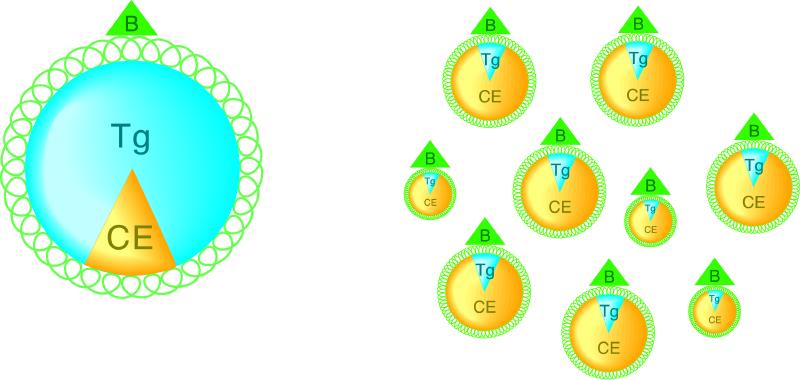
Fig. 1: The normal ratio of VLDL to LDL particles in plasma (above). The VLDL particles are larger (left) because they are enriched with triglyceride, whereas the LDL particles (right) are smaller and enriched with cholesterol. Each particle contains one molecule of apo B. LDL particles differ in size, with most being larger because they contain more cholesterol. Hypertriglyceridemic hyperapo B (below). This is the most common atherogenic dyslipoproteinemia and is characterized by increased numbers of VLDL particles (left) and increased numbers of smaller, denser LDL particles (right). VLDL = very low-density lipoprotein, LDL = low-density lipoprotein, apo B and B = apolipoprotein B, Tg = triglyceride, CE = cholesterol ester.
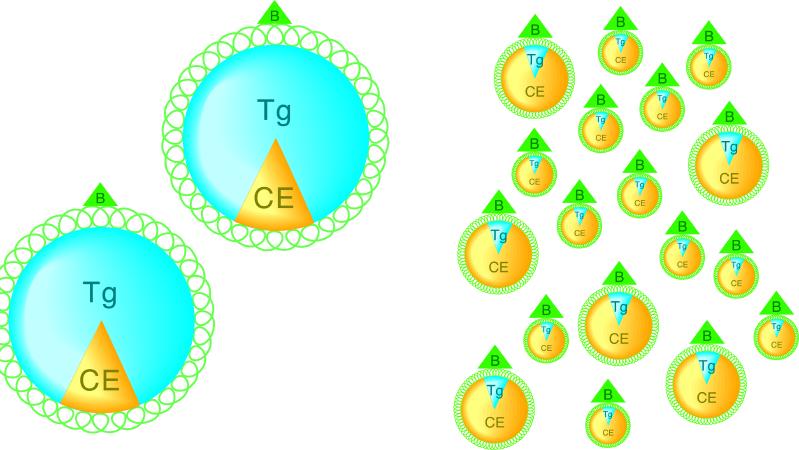
Figure 1. Continued.
The most common atherogenic dyslipoproteinemia consists of mild to moderate hypertriglyceridemia, low HDL cholesterol and increased numbers of small dense LDL particles (Fig. 1).12,13 These are the consequence of increased secretion of VLDL particles by the liver. This, in addition to increased “core lipid exchange,” results in the formation of increased numbers of small dense LDL particles and low HDL cholesterol.14 It should be noted that because the cholesterol content is reduced in small dense LDL, the LDL and total cholesterol levels may be normal even when the number of LDL particles is elevated.
A series of basic studies have shown that, particle for particle, small dense LDL particles are more atherogenic than the larger, more cholesterol-rich LDL particles.15,16,17,18,19,20,21,22,23,24,25,26,27,28,29 These are critical findings but they form only part of the evidence. Data from a series of prospective double-blind trials that tested the effect of various LDL-lowering regimens on the rate of progression or regression, or both, of angiographically evident coronary disease showed that a benefit was associated with the reduction in levels of small dense LDL.30,31,32,33 There have also been several prospective epidemiologic studies that showed that small dense LDL particles were associated with a greater risk of vascular disease.34,35,36
Most of these studies were relatively small, and their findings have had little impact. However, a major recent Canadian study has changed the epidemiologic landscape. The Quebec Cardiovascular Study is the most up-to-date, prospective, epidemiologic investigation of the risk factors responsible for coronary artery disease. It is also the first study in which apo B was measured in all subjects, and it is worth noting that apo B was found to be the single most important lipid parameter for influencing outcome.37
More significantly, for the first time, this study allowed the respective roles of the number of LDL particles and LDL composition to be disentangled. Thus, when the number of LDL particles was increased, that is, if plasma apo B was greater than or equal to 1.20 g/L and LDL composition was normal, risk was increased 2-fold. However, when the number of LDL particles was increased and small dense LDL particles were present, risk was increased more than 6-fold.38 On the other hand, when small dense LDL particles were present but the number of LDL particles was normal (apo B less than 1.20 g/L), risk was not increased.38 Thus, increased numbers of small dense LDL particles constitute a particularly deadly duo. There are no practical ways to measure the size of LDL particles in clinical laboratories, but this is, in any case, unnecessary because of their predictable relation to plasma triglyceride. Thus, if fasting plasma triglycerides are greater than 1.5 mmol/L, small dense LDL particles are very likely to be present.12
The data from AFCAPS/TexCAPS demonstrate that prior to therapy, levels of LDL cholesterol, HDL cholesterol and apo B predict cardiac outcome. However, during therapy, lipid levels and their ratios did not predict outcome, whereas apo B and the ratio of apo B to apolipoprotein A-I (apo A-I) did. It is important to point out that all the analyses were prespecified and, therefore, this does not represent a post hoc analysis. These findings fit with the observational data reported by Moss and colleagues,39 who followed 1045 postinfarction patients and also found that lipid levels did not predict outcome, whereas levels of apo B, apo A-I and the d-dimer of fibrin, which is a degradation product of fibrin, did.
If apo B remains predictive during therapy, it becomes critical to have a target value. This can be taken with some confidence from the POSTCABG study, which is the only clinical trial that has tested whether more intensive LDL lowering with a statin is more effective than less intensive therapy. Alaupovic and colleagues demonstrated that more intensive lowering of the LDL level was superior in terms of angiographic outcome, and that this was associated with a mean apo B level of less than 0.90 g/L,40 a target level that has been accepted by the Canadian Cardiovascular Society.41
Current clinical practice in the diagnosis and treatment of lipids is undeniably complex and confusing. Five parameters — total cholesterol, plasma triglycerides, HDL cholesterol, LDL cholesterol and the total cholesterol–HDL ratio — are reported. All 5 must be interpreted by the physician and understood by the patient, and the complexity inherent in such a system may explain, to some degree at least, why only a minority of patients who begin pharmacologic lipid-lowering therapy reach target levels and stay on therapy.42
Given that the present system is far from ideal, should we not consider modifying it? Why should we not measure apo B in routine practice if it improves the prediction of risk and outcome? Moreover, if statin therapy is chosen, the evidence described here suggests that only apo B need be measured in follow-up. If so, care would be simpler for the patient, in that fasting is not necessary, and simpler for the physician in that only one result, and not 5, needs to be considered and acted on. Simpler care should translate into more cost-effective care and therefore the payer, that is, the government or, rather, ourselves, should benefit as well.
We would emphasize that we are proposing modification, not abolition, of the present system. Apo B should not be the only parameter measured in the initial assessment of the risk of disease due to lipids. Marked hypertriglyceridemia certainly increases the risk of pancreatitis, and the plasma triglyceride level cannot be predicted from apo B. Similarly, a low level of HDL cholesterol increases the risk of vascular disease, and the level of HDL cholesterol cannot be predicted from plasma apo B. The converse, however, is also true: low HDL cholesterol and otherwise normal plasma lipids can coexist with an elevated level of apo B.43
Even if it is granted that such a shift in practice is acceptable from a medical perspective, careful preparation will be essential and considerable education will be required. Given the importance that has been assigned to cholesterol, change will not be easy. But change is the price of progress. Whether we accept this particular change, and how long it takes to do so, will reveal just how much our policy decisions are evidence based and can evolve, or how much they are determined by choices made in the past and are static. Given the potential for benefit for our patients and our society, we hope the former and not the latter will prove to be the case.
Footnotes
This article has been peer reviewed.
Competing interests: None declared for Dr. Bergeron. Dr. Sniderman is a consultant for Merck Frosst Canada Inc. and for Servier Canada; he has received speaker fees from Merck Frosst Canada Inc. and Pfizer Canada Inc. within the past 2 years. Dr. Frolich has served as a consultant to all companies dealing with lipid-lowering agents and has occasionally accepted compensation for himself or for his department's trust fund.
Correspondence to: Dr. Allan D. Sniderman, Mike Rosenbloom Laboratory for Cardiovascular Research, McGill University Health Centre, Royal Victoria Hospital, 687 Pine Ave. W, Montreal QC H3A 1A1; fax 514 982-0686; allan.sniderman@muhc.mcgill.ca
References
- 1.Brown MS, Goldstein JL. A receptor-mediated pathway for cholesterol homeostasis. Science 1986;232:34-47. [DOI] [PubMed]
- 2.Downs JR, Clearfield M, Weis S, Whitney E, Shapiro DR, Beere PA, et al. Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels. JAMA 1998;279:1615-22. [DOI] [PubMed]
- 3.Gotto AM Jr, Whitney E, Stein EA, Shapiro DR, Clearfield M, Weis S, et al. Relation between baseline and on-treatment lipid parameters and first acute major coronary events in the Air Force/Texas Coronary Atherosclerosis Prevention Study (AFCAPS/TexCAPS). Circulation 2000;101:477-84. [DOI] [PubMed]
- 4.Kannel WB, Castelli WP, Gordon T. Cholesterol in the prediction of atherosclerotic disease. New perspectives based on the Framingham study. Ann Intern Med 1979;90:85-91. [DOI] [PubMed]
- 5.Toronto Working Group on Cholesterol Policy: Naylor CD, Basinski A, Frank JW, Rachlis MM. Asymptomatic hypercholesterolemia: a clinical policy review. J Clin Epidemiol 1990;43:1028-1121. [PubMed]
- 6.MacLean DR, Petrasovits A, Connelly PW, Joffres M, O'Connor B, Little JA. Plasma lipids and lipoprotein reference values, and the prevalence of dyslipoproteinemia in Canadian adults. Canadian Heart Health Surveys Research Group. Can J Cardiol 1999;15:434-44. [PubMed]
- 7.Genest J Jr, McNamara JR, Ordovas JM, Jenner JL, Silberman SR, Anderson KM, et al. Lipoprotein cholesterol, apolipoprotein A-I and B and lipoprotein (a) abnormalities in men with premature coronary artery disease. J Am Coll Cardiol 1992;19:792-802. [DOI] [PubMed]
- 8.Sniderman AD, Vu H, Cianflone K. The effect of moderate hypertriglyceridemia on the relation of plasma total and LDL apoB levels. Atherosclerosis 1991;89:109-16. [DOI] [PubMed]
- 9.Marcovina SM, Albers JJ, Kennedy H, Mei JV, Henderson LO, Hannon WH. International Federation of Clinical Chemistry standardization project for measurements of apolipoproteins A-I and B. IV. Comparability of apolipoprotein B values by use of International Reference Material. Clin Chem 1994;40:586-92. [PubMed]
- 10.Connelly PW, Poapst M, Davignon J, Lussier-Cacan S, Reeder B, Lessard R, et al. Reference values of plasma apolipoproteins A-I and B, and association with nonlipid risk factors in the populations of two Canadian provinces: Quebec and Saskatchewan. Canadian Heart Health Surveys Research Group. Can J Cardiol 1999;15:409-18. [PubMed]
- 11.Contois JH, McNamara JR, Lammi-Keefe CJ, Wilson PW, Massov T, Schaefer EJ. Reference intervals for plasma apolipoprotein B determined with a standardized commercial immunoturbidimetric assay: results from the Framingham Offspring Study. Clin Chem 1996;42:515-23. [PubMed]
- 12.Griffin BA, Freeman DJ, Tait GW, Thomson J, Caslake MJ, Packard CJ, et al. Role of plasma triglyceride in the regulation of plasma low density lipoprotein (LDL) subfractions: relative contribution of small, dense LDL to coronary heart disease risk. Atherosclerosis 1994;106:241-53. [DOI] [PubMed]
- 13.Lamarche B, Despres JP, Moorjani S, Cantin B, Dagenais GR, Lupien PJ. Prevalence of dyslipidemic phenotypes in ischemic heart disease (prospective results from the Quebec Cardiovascular Study). Am J Cardiol 1995;75:1189-95. [DOI] [PubMed]
- 14.Sniderman AD, Cianflone K, Arner P, Summers L, Frayn K. The adipocyte, fatty acid trapping, and atherogenesis. Arterioscler Thromb Vasc Biol 1998; 18:147-51. [DOI] [PubMed]
- 15.Nordestgaard BG, Zilversmit DB. Comparison of arterial intimal clearances of LDL from diabetic and nondiabetic cholesterol-fed rabbits. Differences in intimal clearance explained by size differences. Arteriosclerosis 1989;9:176-83. [DOI] [PubMed]
- 16.Bjornheden T, Babyi A, Bondjers G, Wiklund O. Accumulation of lipoprotein fractions and subfractions in the arterial wall, determined in an in vitro perfusion system. Atherosclerosis 1996;123:43-56. [DOI] [PubMed]
- 17.Sattar N, Petrie JR, Jaap AJ. The atherogenic lipoprotein phenotype and vascular endothelial dysfunction. Atherosclerosis 1998;138:229-35. [DOI] [PubMed]
- 18.Festa A, D'Agostino R Jr, Mykkanen L, Tracy R, Howard BV, Haffner SM. Low-density lipoprotein particle size is inversely related to plasminogen activator inhibitor-1 levels. The Insulin Resistance Atherosclerosis Study. Arterioscler Thromb Vasc Biol 1999;19:605-10. [DOI] [PubMed]
- 19.Vaisanen S, Baumstark MW, Penttila I, Bouchard C, Halonen P, Rankinen T, et al. Small, dense LDL particle concentration correlates with plasminogen activator inhibitor type-1 (PAI-1) activity. Thromb Haemost 1997;78: 1495-9. [PubMed]
- 20.O'Brien SF, Watts GF, Playford DA, Burke V, O'Neal DN, Best JD. Low-density lipoprotein size, high-density lipoprotein concentration, and endothelial dysfunction in non-insulin-dependent diabetes. Diabet Med 1997;14: 974-8. [DOI] [PubMed]
- 21.Weisser B, Locher R, de Graaf J, Moser R, Sachinidis A, Vetter W. Low density lipoprotein subfractions increase thromboxane formation in endothelial cells. Biochem Biophys Res Commun 1993;192:1245-50. [DOI] [PubMed]
- 22.De Graaf J, Hak-Lemmers HL, Hectors MP, Demacker PN, Hendriks JC, Stalenhoef AF. Enhanced susceptibility to in vitro oxidation of the dense low density lipoprotein subfraction in healthy subjects. Arterioscler Thromb 1991;11:298-306. [DOI] [PubMed]
- 23.Dejager S, Bruckert E, Chapman MJ. Dense low density lipoprotein subspecies with diminished oxidative resistance predominate in combined hyperlipidemia. J Lipid Res 1993;34:295-308. [PubMed]
- 24.Hurt-Camejo E, Camejo G, Rosengren B, Lopez F, Wiklund O, Bondjers G. Differential uptake of proteoglycan-selected subfractions of low density lipoprotein by human macrophages. J Lipid Res 1990;31:1387-98. [PubMed]
- 25.Anber V, Griffin BA, McConnell M, Packard CJ, Shepherd J. Influence of plasma lipid and LDL-subfraction profile on the interaction between low density lipoprotein with human arterial wall proteoglycans. Atherosclerosis 1996;124:261-71. [DOI] [PubMed]
- 26.Weisser B, Locher R, De Graaf J, Vetter W. Low density lipoprotein subfractions and [Ca2+]i in vascular smooth muscle cells. Circ Res 1993;73:118-24. [DOI] [PubMed]
- 27.Teng B, Sniderman AD, Krauss RM, Kwiterovich PO Jr, Milne RW, Marcel YL. Modulation of apolipoprotein B antigenic determinants in human low-density lipoprotein subclasses. J Biol Chem 1985;260:5067-72. [PubMed]
- 28.Galeano NF, Milne R, Marcel YL, Walsh MT, Levy E, Ngu'yen TD, et al. Apoprotein B structure and receptor recognition of triglyceride-rich low density lipoprotein (LDL) is modified in small LDL but not in triglyceride-rich LDL of normal size. J Biol Chem 1994;269:511-9. [PubMed]
- 29.Chen GC, Liu W, Duchateau P, Allaart J, Hamilton RL, Mendel CM, et al. Conformational differences in human apolipoprotein B-100 among subspecies of low density lipoproteins (LDL). Association of altered proteolytic accessibility with decreased receptor binding of LDL subspecies from hypertriglyceridemic subjects. J Biol Chem 1994;269:29121-8. [PubMed]
- 30.Krauss RM, Lindgren FT, Williams PT, Kelsey SF, Brensike J, Vranizan K, et al. Intermediate-density lipoproteins and progression of coronary artery disease in hypercholesterolaemic men. Lancet 1987;2(8550):62-6. [DOI] [PubMed]
- 31.Watts GF, Mandalia S, Brunt JN, Slavin BM, Coltart DJ, Lewis B. Independent associations between plasma lipoprotein subfraction levels and the course of coronary artery disease in the St. Thomas' Atherosclerosis Regression Study (STARS). Metabolism 1993;42:1461-7. [DOI] [PubMed]
- 32.Miller BD, Alderman EL, Haskell WL, Fair JM, Krauss RM. Predominance of dense low-density lipoprotein particles predicts angiographic benefit of therapy in the Stanford Coronary Risk Intervention Project. Circulation 1996;94:2146-53. [DOI] [PubMed]
- 33.Zambon A, Hokanson JE, Brown BG, Brunzell JD. Evidence for a new pathophysiological mechanism for coronary artery disease regression: hepatic lipase-mediated changes in LDL density. Circulation 1999;99:1959-64. [DOI] [PubMed]
- 34.Gardner CD, Fortmann SP, Krauss RM. Association of small low-density lipoprotein particles with the incidence of coronary artery disease in men and women. JAMA 1996;276:875-81. [PubMed]
- 35.Stampfer MJ, Krauss RM, Ma J, Blanche PJ, Holl LG, Sacks FM, et al. A prospective study of triglyceride level, low-density lipoprotein particle diameter, and risk of myocardial infarction. JAMA 1996;276:882-8. [PubMed]
- 36.Mykkanen L, Kuusisto J, Haffner SM, Laakso M, Austin MA. LDL size and risk of coronary heart disease in elderly men and women. Arterioscler Thromb Vasc Biol 1999;19:2742-8. [DOI] [PubMed]
- 37.Lamarche B, Moorjani S, Lupien PJ, Cantin B, Bernard PM, Dagenais GR, et al. Apolipoprotein A-1 and B levels and the risk of ischemic heart disease during a five-year follow-up of men in the Quebec cardiovascular study. Circulation 1996;94:273-8. [DOI] [PubMed]
- 38.Lamarche B, Tchernof A, Moorjani S, Cantin B, Dagenais GR, Lupien PJ, et al. Small, dense low-density lipoprotein particles as a predictor of the risk of ischemic heart disease in men. Prospective results from the Quebec Cardiovascular Study. Circulation 1997;95:69-75. [DOI] [PubMed]
- 39.Moss AJ, Goldstein RE, Marder VJ, Sparks CE, Oakes D, Greenberg H, et al. Thrombogenic factors and recurrent coronary events. Circulation 1999; 99:2517-22. [DOI] [PubMed]
- 40.Alaupovic P, Fesmire JD, Hunnighake D, Domanski M, Forman S, Knatterud GL, et al. The effect of aggressive and moderate lowering of LDL-cholesterol and low dose anticoagulation on plasma lipids, apolipoproteins and lipoprotein families in post coronary artery bypass graft trial. Atherosclerosis 1999;146:369-79. [DOI] [PubMed]
- 41.Collins-Nakai RL, Dagenais GR. The role of the cardiovascular specialist in the prevention of cardiovascular diseases — executive summary. Can J Cardiol 1999;15:7G-10G. [PubMed]
- 42.Avorn J, Monette J, Lacour A, Bohn RL, Monane M, Mogun H, et al. Persistence of use of lipid-lowering medications: a cross-national study. JAMA 1998;279:1458-62. [DOI] [PubMed]
- 43.Genest J Jr, Bard JM, Fruchart JC, Ordovas JM, Schaefer EJ. Familial hypoalphalipoproteinemia in premature coronary artery disease. Arterioscler Thromb 1993;13:1728-37. [DOI] [PubMed]