

Abstract
IN THIS ARTICLE THE ACTUAL AND RELATIVE COSTS OF TUITION AT 3 Ontario medical schools are traced over the past 150 years. In addition, the factors that led to Ontario's nearly 4-decade experiment in private medical education (and to its eventual demise) are presented. In relative terms, tuition was stable for over a century, then declined (after 1960) as government support rose. Access to medical training for students from middle-income families may also have improved steadily until the late 1980s. Because there is no shortage of people wanting to become doctors, there seems to be no limit to the price that could be set for a medical education. The recent hikes in tuition have outstripped inflation and may be reducing accessibility to restrictive levels, similar to those that prevailed in the 19th century. The author invites readers to question current trends.
A report in CMAJ characterized the 1997 deregulation of medical tuition in Ontario as "a nightmare for many medical students," and the dean of one medical school predicted that "the higher fees will create barriers."1 When my students asked if the tuition hikes were unprecedented, I was surprised to discover that medical historians and educators have ignored this question, and that few have asked how tuition influences who becomes a doctor.
In this paper I review the actual and relative costs of medical tuition at 3 Ontario schools over the past 150 years, relating them to government funding and public access. My questions included the following: Has the worst-case scenario (no public funding) happened before? Has tuition always risen over time? Have students in the past ever paid as much as today's students do? Has high medical tuition been a barrier to students? And if we do not know the answer to that question, why not?
A precedent for the worst-case scenario
Recent increases in tuition have stemmed from declining public funding of higher education. For example, the Ontario government has just announced its intention to give degree-granting privileges to private universities.2 If public support for medical training were to fall to zero, how much would students have to pay to cover all costs? Would schools be forced to close or to privatize?
Readers may be surprised to learn that Ontario has already conducted a nearly 4-decade experiment along these lines, and it was judged a failure. In April 1853, a federal legislative act closed the faculties of law and medicine at the University of Toronto (U of T).3 The institution could examine students for their degrees, but no tax money was to be spent on teaching or facilities. Medical education was not abolished; rather, it was "privatized" into corporate schools, where tuition covered costs. Enormous public savings were promised, and access was expected to improve. In the House of Commons Francis Hincks, who introduced the bill, said, "It is not desirable that teachers of any of the professions . . . of a lucrative nature should be paid by the government."4
Members on both sides of the House agreed.5 The changes would raise standards in the "overcrowded" professions by excluding those who were "better qualified for inferior pursuits."6 Only 2 members were opposed: George Brown, the editor of the Globe, and his fellow journalist- politician, Joseph-Edouard Cauchon of Quebec City.7
Some witnesses plausibly suggested that the faculty closure had been engineered by John Rolph.8,9 A remarkable character — physician, lawyer and politician — Rolph has fascinated historians for his rebel role in the Rebellion of 1837.10,11,12 From 1843 he ran a private medical school in Toronto. His main rival was the King's College medical school, which, by 1850, had become the medical faculty at U of T.13,14 The conservative professors at the King's College school disapproved of Rolph's political views and favoured their own students in the degree and licensing examinations, which they controlled. Provoked by this competition, Rolph secured a seat in the federal legislature and a place in Cabinet. In supporting the Hincks bill, he decried the fiscal irresponsibility of the professors who let "revenues [be] trifled away;" he chastised these "sons of nobility and gentry" for "sponging" off the labour of "honest men;" and he exclaimed, "Free taught doctors, lawyers, divines, or editors or bankers or butchers or bakers, everyone must repudiate!"15 Even Rolph's journalistic enemies joined him in praise of the bill.16,17
In support of Rolph's presumed influence and belying the high language against public funding for professions, government money continued to flow to new and existing medical schools, including Queen's University, in Kingston, which opened in 1854.18 But medicine at U of T was finished, at least for the next 34 years, a period when the training of doctors in Toronto was left to private, "proprietary" schools — at least 2 of which operated at any given time.14,19,20,21,22,23
History of Ontario medical tuition: sources and methods
Few historians have examined medical tuition.24,25 Some policy analysts have used historical data to ask at what level fees and loans should be set.26,27 To explore this topic, I consulted announcements (or calendars) from the medical faculties of Queen's University,28 which opened in 1854, the University of Western Ontario (UWO), London,29 which opened in 1882, and U of T,30 which reopened in 1887, to establish the average fee for 1 year of undergraduate medical training since the 1850s. I also sought to relate fees to government support through the same period.
Some methodological problems arose. First, none of the calendar collections was complete. Second, until 1895, students were charged on a course-by-course basis, so the average annual fees had to be calculated. Third, I found that students were subject to charges for other activities intended to enhance scientific and social life. Of these extra charges, I included only hospital fees in my calculations. Finally, the duration of medical training has changed over time: from 4, to 5, to 6 and back to 4 years. When fees for "premedical" and "postmedical" years were different from the fees for "medical" years, only the latter were included.
Results in actual dollars
In 1861 the average annual fee for a student at Queen's (the only school for which data are available from that period) was $55. Tuition rose slowly in uneven increments, reaching $80 by 1900. This stepwise rise, which also characterized trends in fees at UWO and U of T (after the faculty was reopened in 1887), continued over the next 80 years (Figs. 1-3). Similarities and minor differences between the 3 schools are apparent. U of T charged the most until the 1950s, when UWO took the lead. Tuition at Queen's was usually the lowest. Tuition doubled twice over 2 consecutive 40-year periods, then it doubled over 15 years, then the rate of increase slowed, and the next doubling took 25 years. For all 3 schools, the rise in tuition over the past 3 years (1997-1999) represents the steepest slope in 150 years.
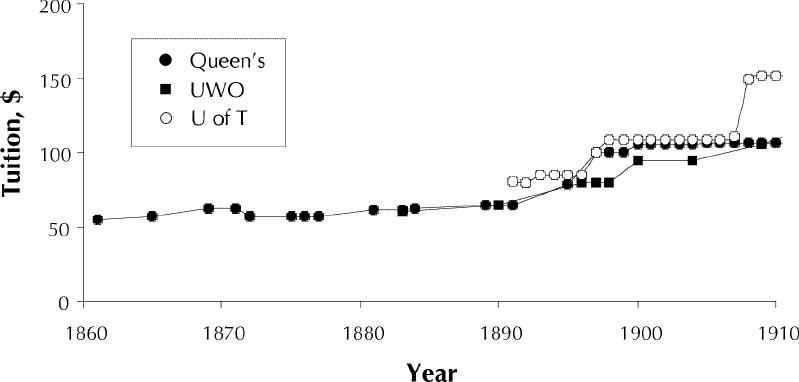
Fig. 1: Average annual tuition at 3 Ontario medical schools, 1860-1910.28,29,30 Queen's = Queen's University, Kingston; UWO = University of Western Ontario, London; U of T = University of Toronto.
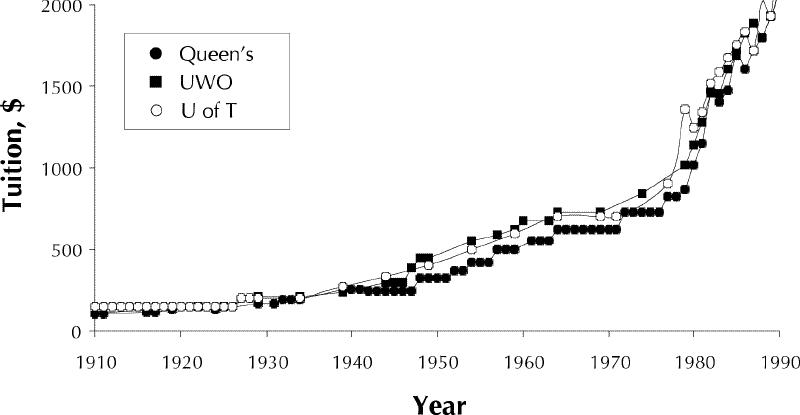
Fig. 2: Average annual tuition at 3 Ontario medical schools, 1910-1990.28,29,30
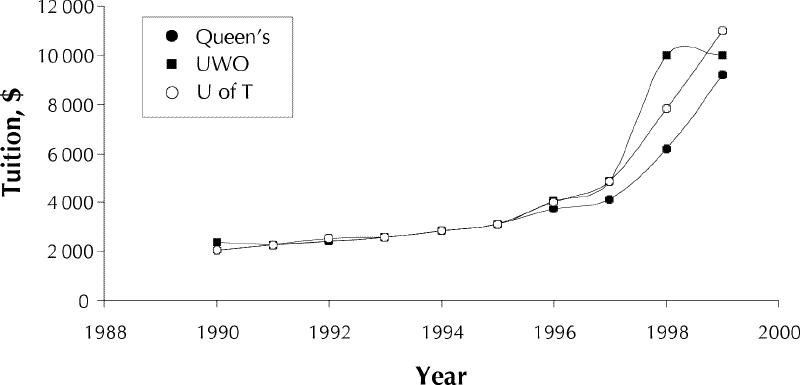
Fig. 3: Average annual tuition at 3 Ontario medical schools, 1990-1999.28,29,30
Slight differences in fees may not have seemed slight to prospective students, and competition for candidates dictated calendar copy. From 1894 until 1900, U of T assured prospective students that "The Faculty ... has spared no expense in making the arrangements for medical instruction perfect."31 The emphasis on science at U of T justified hikes in tuition, and laboratories were featured in words, maps and even pictures. Queen's announcements described Kingston as "a pleasant city, free from the attractive amusements that interfere with study."32
Increases in tuition have been more frequent than decreases, especially since the 1980s. At Queen's, for example, tuition was raised by more than 25% in 1897, 1927, 1929, 1939, 1948 and 1982; the largest increase was 32.5% in 1948. On rare occasions, Queen's tuition fell, the greatest decline being 10% in 1872, and the most recent, 4% in 1983. Like other commodity prices, tuition has responded to important economic events: the Great Depression, world conflict and inflation.
Results in 1999 dollars
Clearly, $55 was worth a lot more in 1861 than in 2001, but does the steady rise in tuition persist when the raw amounts are converted to constant dollars? Tracing dollar values back many decades is fraught with difficulty.33 Two tools were used for this exercise: the gross domestic product deflation index and the consumer price index.
Despite the relentless climb in actual dollars, I found that when expressed in 1999 dollars, tuition was relatively stable until the 1980s and 1990s (Fig. 4), hovering around the equivalent of $2000. Sometimes, tuition rose or fell in 1999 dollars when it appeared unchanged in actual dollars. Relative declines in tuition were more frequent than declines in actual dollars, but the increases continue to outpace any decreases. The 50% hikes of 1998 and 1999 remained the maximum. The stability of tuition and then its slow rise in actual dollars from the late 1960s to the 1980s corresponded to a steady relative decline in 1999 dollars. These trends indicate the financial privilege enjoyed by physicians trained in the late 1960s and 1970s who have become the academics presiding over current fee increases.
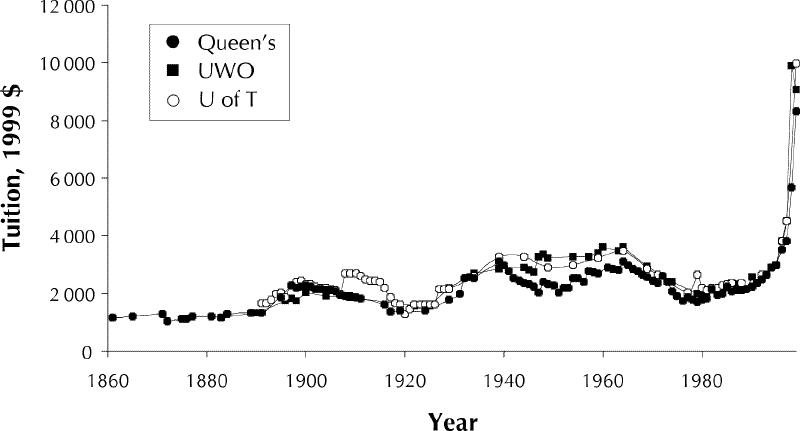
Fig. 4: Average annual tuition at 3 Ontario medical schools, 1860-1999,28,29,30 expressed in constant (1999) dollars, as determined from gross domestic product deflator and consumer price index.
Tuition and government support
Medical faculties have been supported to a variable extent by government grants over the past 150 years. Because transfers have been made on variable scales and through a variety of "envelopes" from the central university administration, precise amounts are difficult to determine. I used the financial summaries in the annual reports of the principal of Queen's University to calculate the percentages of revenue for the entire institution deriving from government support and tuition (Fig. 5).34 Governments — mostly provincial — were fairly equal partners with students in university funding from about the turn of the century until the 1960s. Then, the percentage of funding from government revenue began to rise as support from tuition declined. Recent changes show a reversal of the pattern and a trend toward more equal sharing.
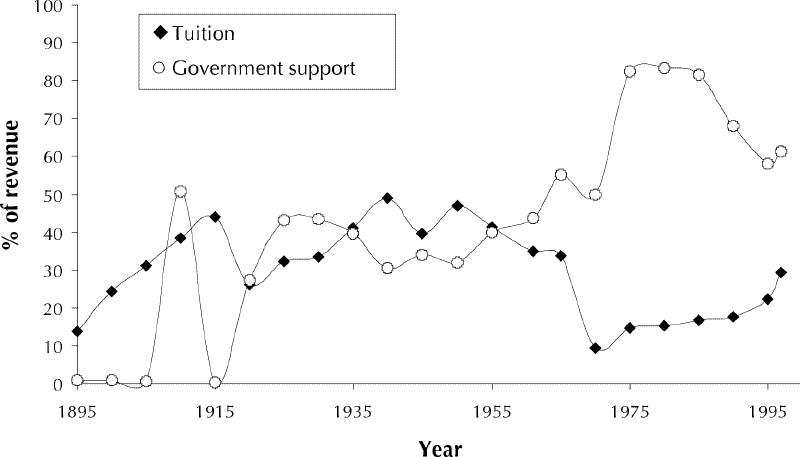
Fig. 5: Percentage of university revenue obtained from tuition and from government support at Queen's University, Kingston, Ont., 1895-1999.34
Carpenter caper
A discussion of tuition is meaningless without consideration of accessibility. Do fees have an impact on who can become a doctor? Instinctively, we might say Yes, but academic and government bureaucrats typically respond with a reassuring No, pointing to the availability of scholarships and loans. I wondered if the costs of a medical education could be compared to the income of a middle-class family. Since "minimum wage" is a 20th-century concept, I had to identify a trade that was still practised in the year 2000 and for which salaries could be traced reliably back to 1860.
The venerable trade of carpentry flourished as a waged industry from the time of the French Regime in Canada,35 and it is still important today. In addition, reliable figures on carpenters' wages are available.36,37,38 The hourly wages of a carpenter through time do not correlate with weekly or annual earnings. Twelve-hour days were common until the 1870s, a 60-hour work week then prevailed until about 1900, and the 40-hour work week was introduced after World War II.39 But an hour of work for a carpenter is still an hour of work.
Carpenters' hourly wages rose steadily from a low of about $0.09 in 1871 to more than $20 in the late 1990s. To explore the question of how this increase compared with changes in medical tuition, I expressed tuition in terms of hours of carpenter labour and found a strikingly different pattern from the trend expressed in dollars (Fig. 6). Current fees no longer appear as the highest. In 1999 they were moving upward but still fell below the nearly 700 hours of carpenter labour required to support 1 year of medical education in the 1870s. Again, instances of decline and rise are visible, and a falling trend predominated until the 1980s. A halcyon low point came in the late 1970s, when a carpenter needed to work only about 83 hours to fund a year of his daughter's medical education.
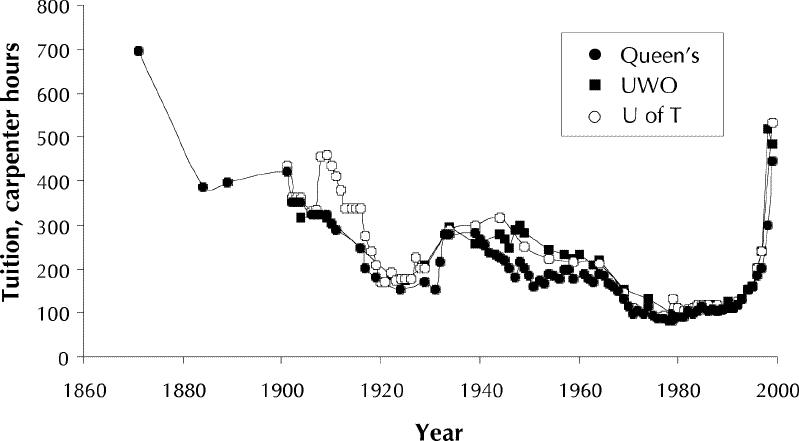
Fig. 6: Average annual tuition at 3 Ontario medical schools, 1860-1999, in terms of "carpenter hours."28,29,30,36,37,38
Medical education may have been less accessible for carpenters in the past than it is now. But the relatively lower level of current fees that is apparent when tuition is expressed this way does not imply that we should stop worrying. On the contrary, at current rates of increase, the carpenter will soon be right back where he started. Social policy initiatives undertaken over a century and a half — a period that saw Confederation, the rise of the welfare state and the development of a Canadian identity with its emphasis on literacy and learning — are about to be erased. Perhaps public access to education — a characteristic of our national identity and an emblem of our high quality of life — is becoming a thing of the past.
Why care? Tuition and access to medical education
The relation between tuition and the question of who becomes a doctor is unknown. Just as fees have not been studied historically, they have scarcely been studied sociologically or demographically. US historians have examined discrimination in medical education on the basis of race, sex and religion, but we do not know whether discrimination is also based on financial barriers.
Historical research in the United States suggests that we should care about this matter for at least 2 reasons. First, government support has helped to improve the quality of education, in particular by covering the increases in costs as laboratory science has evolved (during the bacteriology boom of the 1880s and after the 1910 Flexner Report24,40). When government support declines, so too do intellectual standards and the physical plant.24,25
The second reason is the ability of medicine to address the social determinants of health, rather than simply paying them pedagogic lip service. Do doctors have difficulty conceiving of socially determined health problems because of their own social class? Without representatives from all social groups, how can the profession understand, research and solve major health issues?
Studies in Canada and the rest of the developed world have repeatedly shown that doctors come from privileged backgrounds.41,42,43,44,45,46,47 US work from the 1960s and 1970s has suggested that perhaps tuition plays a role in their selection. In a 1965 report, Rosinski48 showed that the numbers of medical students from the lower income classes were small; however, their highest representation was in schools with the lowest tuition. Another study found that students from lower social classes performed just as well on national board examinations as their more fortunate peers.49 In the United States this socioeconomic question is bound up with issues of race and ethnicity. Affirmative action programs, designed to address the exclusiveness of medical training, have encountered furious opposition, each side accusing the other of racism.46,47,50,51,52
In 1981 Sandson53 described the "crisis" caused by a rise in US medical school tuition to a rough average of $10 000 a year. Claiming that minority access to medical education was declining, he argued for enhanced financial assistance. His essay has been cited in pleas for better loans, but his observations about declining minority presence have been ignored.
Why is there so little information on the question of the impact of tuition on physician identity? First, the monetary barrier is difficult to perceive. Applicants to medical school are not in short supply: if money is a barrier for one candidate, another who is more affluent will fill the vacancy. Second, the barrier operates not only at the time of application but also before students become eligible for medical school — something that has been addressed by initiatives in the United States.54,55 Now that at least one postsecondary degree is needed for admission, potential applicants who cannot afford any postsecondary education are automatically eliminated. A recently reported survey showed that lower-income parents of 7th- and 8th-grade children in the Maritimes considered university beyond their reach.56 In 1999 lower tuition was part of the successful NDP platform in Manitoba. The new premier has admitted that evidence is lacking for barriers created by high tuition; however, from conversations with high school students, his team had "a gut feeling" about barriers.57 Thus, tuition is part of a broader question of accessibility and quality.
Finally, we do not have the information because we may avoid the research for egocentric reasons. Doctors sometimes conduct surveys to determine the demographic characteristics of our profession and of our students, but rarely do we ask who should be here instead. Several groups have studied applicants who were later admitted to other schools (i.e., "wrongly" rejected applicants), but I found only one study addressing the identity of rejected applicants: back in 1971, being female and having a public, not a private, education were correlated with rejection.58
Perhaps a sense of entitlement hampers the investigation. It takes courage to ask if your own admission to the profession has come at someone else's expense, someone who might be more deserving intellectually and more useful socially, someone who was not even in the applicant pool. Without asking that question, we lack the moral evidence to bolster claims that the tuition hikes should be stayed. So, ask it we must.
Some surveys on present students and medical school applicants are underway (e.g., as described by Sibbald1 and undertaken by D.A. Sim ["Report of the 1999 survey of medical students at U.W.O.," unpublished report]), but their focus must be expanded. Questions should be asked about parental employment, health and income and about whether the student comes from a single-parent family or is disabled, a refugee, or from an economically depressed region of Canada or another country. Because Canada favours immigration on the basis of wealth, the last of these factors must be correlated with parental income. We should also ask if the student considers himself or herself to be from a minority. This work should be done on a national scale and should extend to all undergraduates and postgraduates, a group that will allow analysis of demographic trends over the past 9 years, right through the staggering tuition hikes. We must find out who is missing from our ranks.
The failure of privatization: U of T reopens its medical faculty
When the U of T faculty was closed in 1853, the government claimed that taxpayers should not support training for a lucrative profession. But the faculty did reopen. What caused the reversal? How did Ontarians come to believe, once again, that money should be spent on medical education? The answer to this question should be important now, with privatization looming again and with that unproven "gut feeling" that future doctors may not always reflect the best, the brightest and the fullest extent of our national diversity.
Within a short time after the faculty closure, the fired professors lobbied the government to reopen the faculty or provide pensions.59,60 Meanwhile, the private medical schools in Toronto continued to operate, supported entirely by fees.61,62,63 But partisan politics had spilled over into all aspects of medical education. Collaborative efforts for change foundered in endless squabbling between schools over professional organization,64 licensing65 and hospitals, which were deplored for biased teaching, notorious filth and the alcoholic indiscretions of staff.66,67,68,69,70 Closing the medical faculty had not helped, yet as late as 1877 provincial legislation cited the 1853 federal legislation to justify its continued closure.71 The early 1880s triumph of germ theory and the promise of science also played a role.
Finally, in 1887, 34 years after the closure, a new Ontario statute recreated the Faculty of Medicine at U of T.72 A handful of doctors protested, attempting to save their private schools on the basis of the old arguments,73 but their pleas were denigrated.74,75
In a rousing speech, the Liberal minister of education, G.W. Ross, explained his new bill.76 Having just revamped and replenished elementary and secondary education, he derided the folly of withholding funds from the very culmination of the educational pyramid. The costs of running laboratories were crippling private schools. Scientific standards were slipping, and students were leaving for study elsewhere. The university already had the essential laboratories, and the instructors in those laboratories wanted access to clinical material to enhance research and learning. "Ample precedents [show]," Ross said, that "the State must attend . . . to superior education ... [for] every young man and he was happy to say every young woman." He continued, "Education in the university would be free."76 The people of the province would be the beneficiaries of scientifically trained doctors; it made perfect sense that the people of the province should pay to educate those doctors.
Amazingly enough, both sides of the House agreed.77,78 The bill passed in April 1887, and U of T's Faculty of Medicine reopened 6 months later. Instructors of the proprietary schools were invited to become the professors.61
And what of that "free tuition," written into law in late April 1887? It did not last long. On May 23, the new teachers set out the terms under which they would join the university. To protect them from financial loss, it was argued that tuition should continue at least at the same rate as in the private schools, because it had always managed to "yield a profit to the school."79
In the 19th century, professorial salaries were viewed with distaste.22,61 Clinical teaching was supposed to be remunerated in status, through the prestige of dealing with students, which could be turned into practice income.25 When confronted with a need to protect resources, however, the 1887 medical professors opted to charge students rather than incur the risk of lower income. How often that same decision has been made in times of fiscal restraint is another intriguing question awaiting investigation.
Conclusion: What goes around, comes around
On the basis of my reading of the historical evidence, I think that tuition in Ontario may now constitute a barrier to medical (and other) education. It could also restrict the intellectual quality of our future doctors. We should endeavour to test these hypotheses by asking courageous questions about our identity and that of our students and applicants. If not, we may spend another 40 years wandering in a pedagogic wilderness before our grandchildren learn, once again, precisely what the educators of Ontario seemed to have discovered back in 1887: that a carpenter's daughter should not barred from becoming a doctor, and that publicly funded medical education is good for us all. Must history repeat itself? Perhaps not, but it seems that we will have to fight to prevent it from doing so.
Footnotes
*Presented in part as the keynote address for the Ontario Medical Students Weekend; Feb. 18, 2000; Queen's University, Kingston, Ont.
This article has been peer reviewed.
Acknowledgements: I thank Sacha Agrawal, who provided me with information on the latest U of T tuition, Professor Gert Brieger, who directed me to US surveys, Herbert Brill, who gave me information on student surveys, Irfan Dalla, who invited me to read the paper at the U of T, Drs. Dale Dotten and R.D. Wolfe, who read the paper in draft, Professor Emeritus Martin Friedland, who provided me with unpublished chapters of his forthcoming history of the U of T, Roger Healey, who helped me to find the global Queen's budgets back to 1890, Joshua Lipton-Duffin, who helped me with the illustrations, David Messenger, who invited me to give the address that became this article and gave me access to medical student literature and reports, Jeff Moon, who helped me double-check references, and the archivists and librarians at Queen's University, Kingston, Ont., the University of Western Ontario, London, Ont., and the University of Toronto, Toronto. I am also grateful to 2 professors at Queen's University, Marvin McInnis of Economics and Lisa Powell of Policy Studies, who helped me to find suitable tools for converting historical monetary amounts to current dollars.
Competing interests: None declared.
Correspondence to: Dr. Jacalyn Duffin, Hannah Professor of the History of Medicine, Queen's University, Kingston ON K7L 3N6; fax 613 533-6330; duffinj@post.queensu.ca
References
- 1.Sibbald B. Rising tuition fees a nightmare for many medical students. CMAJ 1998;159:553. Available: www.cma.ca/cmaj/vol-159/issue-5/0553.htm
- 2.Galt V. Student and teacher groups decry private universities. Globe and Mail [Toronto] 2000 Apr 3;Sect A:9 (col. 1-3).
- 3.An act to amend the laws relating to the University of Toronto, SUC 1853, 16 V, cap 89. p. 313-320 [especially section 17, p. 317-8].
- 4.Hincks F. Debates of the Legislative Assembly of United Canada (Hansard). 4th Parliament, 2nd Session. Vol 11, Pt 3 (1853 Feb 25). Montreal: Centre d'étude du Québec et Centre de recherche en histoire economique du Canada français, Concordia University; [1853] 1981. p. 1742.
- 5.Langton J. Debates of the Legislative Assembly of United Canada (Hansard). 4th Parliament, 2nd Session. Vol 11, Pt 3 (1853 Feb 25). Montreal: Centre d'étude du Québec et Centre de recherche en histoire economique du Canada français, Concordia University; [1853] 1981. p. 1756.
- 6.Gamble JW. In: Debates of the Legislative Assembly of United Canada (Hansard). Vol 11, Pt 3 (1853 Feb 25). Montreal: Centre d'étude du Québec et Centre de recherche en histoire economique du Canada français, Concordia University; [1853] 1981. p. 1758.
- 7.University bill. Globe [Toronto] 1853 Mar 3:106 (col. 7); 1853 Mar 8:113 (col. 7), 114 (cols. 1-3); 1853 Mar 24:143 (col. 3).
- 8.Richardson JH. Reminiscences of the medical profession, 1829-1905 [unpublished manuscript]. Toronto: Baldwin Room, Metropolitan Toronto Public Library. p. 8-9.
- 9.Richardson JH. Letter to U of T President Loudan, 1899. Cited in: Godfrey CM. Medicine for Ontario. Belleville (ON): Mika; 1979. p. 58.
- 10.Godfrey CM. John Rolph: rebel with causes. Madoc (ON): Codam Publishing; 1993.
- 11.Craig GM. John Rolph. In: Halpenny FG, Hamelin J, editors. Dictionary of Canadian biography. Vol 9. Toronto: University of Toronto Press; 1976. p. 683-90.
- 12.Duffin J. In view of the body of Job Broom: a glimpse of the medical knowledge and practice of John Rolph. Can Bull Med Hist 1990;7:9-30. [DOI] [PubMed]
- 13.Wallace WS. A history of the University of Toronto, 1827-1927. Toronto: University of Toronto Press; 1927. p. 208-10.
- 14.Friedland M. Ch. 4. In: The University of Toronto: a History. Toronto: University of Toronto Press. In press.
- 15.Rolph J. Debates of the Legislative Assembly of United Canada (Hansard). 4th Parliament, 2nd Session. Vol 11, Pt 3 (1853 Feb 25). Montreal: Centre d'étude du Québec et Centre de recherche en histoire economique du Canada français, Concordia University; [1853] 1981. p. 1754-5.
- 16.Dr. Rolph's marriage bill. Christian Guardian [Toronto] 1853 Mar 9:3 (col. 1).
- 17.University bill. Christian Guardian [Toronto] 1853 Mar 2:3 (col. 2).
- 18.Journals of the Legislative Assembly of Canada. 5th Provincial Parliament, 2nd Session. Vol 14, No 1, appendix 11 "University of Toronto." Toronto: Rollo Campbell printer; 1856.
- 19.Godfrey CM. Medicine for Ontario. Belleville (ON): Mika; 1979. p. 51, 62-3, 74-5.
- 20.McPhedran NT. Canadian medical schools; two centuries of medical history 1822 to 1992. Montreal: Harvest House; 1993. p. 74-5.
- 21.Friedland M. Ch. 12. In: The University of Toronto: a History. Toronto: University of Toronto Press. In press.
- 22.Gidney RD, Millar WPJ. Professional gentlemen: the professions in nineteenth-century Ontario. Toronto: University of Toronto Press; 1994. p. 38-9, 189-95.
- 23.Hamowy R. Canadian medicine. A study in restricted entry. Vancouver: Fraser Institute; 1984. p. 80-93.
- 24.Ludmerer KM. Learning to heal: the development of American medical education. New York: Basic Books; 1985. p. 54, 140, 141-3, 271.
- 25.Rothstein WG. American medical schools and the practice of medicine. New York: Oxford University Press; 1987. p. 51, 62, 92-3, 151, 153, 233-4.
- 26.Finnie R, Schwartz S. Student loans in Canada: past, present, and future. Toronto: CD Howe Institute; 1996. p. 88-94.
- 27.Naradzy JF. Into the deep well: the evolution of medical school debt. JAMA 1998;280:1881-3. [PubMed]
- 28.Medical faculty announcements (1860-1999). Kingston (ON): Archives, Queen's University.
- 29.Medical faculty announcements (1882-1999). London (ON): JJ Talman Regional Collection, University of Western Ontario.
- 30.Medical faculty announcements [bound with university calendars]. P78-0021(05) to P78-0024. Toronto: University of Toronto Archives.
- 31.Medical faculty announcements (1894, p. 106-7; 1895, p. 136-7; 1896, p. 134-5; 1897, p. 144-5; 1900, p. 144-145). Toronto: University of Toronto Archives.
- 32.Medical faculty announcement. Kingston (ON): Archives, Queen's University; 1883. p. 4.
- 33.Green AC, Urquhart MC. New estimates of output growth in Canada: measurement and interpretation. In: McCalla D, Huberman M, editors. Perspectives on Canadian economic history. Mississauga (ON): Copp Clark Longman; 1994. p. 158-75.
- 34.Annual reports of principal. Kingston (ON): Office of the Principal, Queen's University.
- 35.Pentland HC. Labour and capital in Canada, 1650-1860. Toronto: James Lorimer; 1981. p. 55.
- 36.1871 Census of Canada report. Vol 3. Ottawa: Queen's Printer; 1875. p. 310-1.
- 37.Urquhart MC, Buckley KAH. Historical statistics of Canada. Cambridge: Cambridge University Press; 1965. p. 96, 110-11. also 2nd ed. by Statistics Canada; 1980, Series E256.
- 38.Labour income per hour worked, construction industries, 1961-1998 [electronic database]. Label I606106, SDDS 1402. Toronto: Computing in the Humanities and Social Sciences, University of Toronto.
- 39.Marr WL, Paterson DG. Canada: an economic history. Toronto: Gage; 1980. p. 199-202.
- 40.Worthington WC Jr. A study in post-Flexner survival. The Medical College of the State of South Carolina. JAMA 1991;266:981-4. [DOI] [PubMed]
- 41.Fish DG, Farmer C, Nelson-Jones R. Some social characteristics of students in Canadian medical schools. 1965-66. CMAJ 1968;99:950-4. [PMC free article] [PubMed]
- 42.Donnan SPB. British medical undergraduates in 1975: a student survey in 1975 compared with 1966. Med Educ 1976;10:341-7. [DOI] [PubMed]
- 43.McManus IC. The social class of medical students. Med Educ 1982;16:72-5. [DOI] [PubMed]
- 44.Collins JP, Jones J, White GR. Demographic variables in Auckland medical students. N Z Med J 1993;106:306-8. [PubMed]
- 45.Moilanen P, Ihalainen O. Social background, choice of occupation, and occupational expectations of medical students in northern Finland. Br J Med Educ 1974;8:230-3. [DOI] [PubMed]
- 46.Haynes MA. Physician characteristics: influence of social background in medical education. J Med Educ 1973;48(12 Suppl):45-8. [PubMed]
- 47.Kleinbach G. Social structure and the education of health personnel. Int J Health Serv 1974;4:297-317. [DOI] [PubMed]
- 48.Rosinski EF. Social class of medical students. A look at an untapped pool of possible medical school applicants. JAMA 1965;193:89-92. [DOI] [PubMed]
- 49.Fredericks M, Mundy P. The relationship between social class and national board scores of students in a medical school. Soc Sci Med 1969;3:104-10. [DOI] [PubMed]
- 50.Begun MS. Legal considerations related to minority group recruitment and admissions. J Med Educ 1973;43:556-9. [DOI] [PubMed]
- 51.Blackman NS. Minority group status as an admission criteria [sic] [letter]. J Med Educ 1973;43:966. [DOI] [PubMed]
- 52.Johnson L Jr. Minorities in medical school and National Medical Fellowships, Inc.: 50 years and counting. Acad Med 1998;73:1044-51. [DOI] [PubMed]
- 53.Sandson JI. Sounding board. A crisis in medical education: the high cost of student financial assistance. N Engl J Med 1981;308:1287-9. [DOI] [PubMed]
- 54.Simon HJ, Covell JW. Performance of medical students admitted via regular and admission-variance routes. J Med Educ 1975;50:237-41. [DOI] [PubMed]
- 55.Bediako MR, McDermott BA, Bleich ME, Colliver JA. Ventures in education: a pipeline to medical education for minority and economically disadvantaged students. Acad Med 1996;71:190-2. [DOI] [PubMed]
- 56.Johnson AD. Farewell to equal access. Maclean's 1998;111(1 July):75.
- 57.Doer G. The Donald Gow Lecture [question and answer session]; School of Policy Studies, Queen's University, Kingston (ON); 28 Apr 2000.
- 58.Johnson ML. Non-academic factors in medical school selection: a report on rejected applicants. Br J Med Educ 1971;5:264-8. [DOI] [PubMed]
- 59.Debates of the Legislative Assembly of United Canada (Hansard). Vol 13, Pt 2 (28 Mar 1856). Montreal: Centre d'étude du Québec et Centre de recherche en histoire economique du Canada français, Concordia University [1856] 1981. p. 953-7.
- 60.House last night. Globe [Toronto] 1856 Mar 29:2 (col. 7).
- 61.Godfrey C. Aikins of the U of T medical faculty. Madoc (ON): Codam; 1998. p. 83, 106.
- 62.Advertisement for Trinity College Medical Department. Globe [Toronto] 1853 Mar 24.
- 63.An act to incorporate Trinity Medical School, RSO, 1877, 40 V, cap 65. p. 252-5.
- 64.Upper Can Med Surg J 1852-3;2:138-44,167-74; and 1853-4;3:229,266-72,363-71,479-82,557-61.
- 65.Medical board. Upper Can Med Surg J 1853-4;3:414-6.
- 66.Lunatic asylum. Upper Can Med Surg J 1853-4;3:123-4.
- 67.Journals of the Legislative Assembly of Canada. 5th Provincial Parliament, 2nd Session. Vol. 14. Toronto: Rollo Campbell printer; 1856 (26 Mar). p. 182.
- 68.Toronto General Hospital. Med Chron 1854;1:494-7.
- 69.Toronto General Hospital. Upper Can Med Surg J 1852-3;2:217-8,280-4; and 1853-4;3:69-77,464-9,483-7,562.
- 70.Cosbie WG. The Toronto General Hospital. A chronicle. Toronto: Macmillan; 1975. p. 51-61.
- 71.An act respecting the University of Toronto, SO 1877, c. 210, s. 61. p. 2165-6.
- 72.An act respecting the Federation of the University of Toronto, SO 1887, 50 V, c. 43. p. 188-215 [especially p. 189].
- 73.Geikie WB. Medical school amalgamation. CanLancet 1887;19:264.
- 74.Medical school amalgamation [editorial]. Can Lancet 1887;19:249-50.
- 75.Meredith WR. Debates of the Legislative Assembly of Ontario (Hansard) (1887 Apr 12). 6th Provincial Parliament, 1st Session.
- 76.Ross GW. Debates of the Legislative Assembly of Ontario (Hansard) (1887 Apr 12). 6th Provincial Parliament, 1st Session.
- 77.Gibson T. Debates of the Legislative Assembly of Ontario (Hansard) (1887 Apr 12). 6th Provincial Parliament, 1st Session.
- 78.Ontario Legislature. Globe [Toronto] 13 Apr 1887; 4-5.
- 79.Meeting of 1887 May 23, Toronto School of Medicine. In: Minute book 1877-1904. B74-0007/. Toronto: University of Toronto Archives. p. 194-7 [especially p. 196].