

Abstract
Studies indicate that the soil, water and consequently foodstuffs in Serbia are significantly poor in zinc (Zn), and thus, it is likely that there is a Zn deficiency in the Serbian population. This study examined the Zn status in multiple clinical samples, including body fluids (serum, cerebrospinal fluid), whole blood and Zn-rich solid tissues (thyroid and brain tissue). Differences between sex and age were also considered, and comparative analysis of Zn status with other world populations was performed. Serum samples from a large number of Serbian adults approximately had twofold lower Zn amounts when compared to other populations. A similar trend was obtained for whole blood. Males had significantly higher amounts of Zn in serum, whole blood and thyroid tissue samples than females. Higher amounts of Zn were observed in the group older than 50 years. Importantly, in thyroid and brain tissues, Zn was 10- and 20-fold lower, respectively, than reported in the literature. Our results indicate that the population in Serbia could be considered Zn deficient. Therefore, adequate oral Zn supplementation and/or foodstuff fortification should be considered to prevent the deleterious effects caused by Zn deficiency.
Keywords: Zinc, Body fluids, Whole blood, Thyroid tissue, Brain tissue, Serbian population
Introduction
Human biomonitoring (HBM) is an important tool used to assess human exposure to different major and trace elements in the general population (Berman et al. 2016). The data obtained from HBM are valuable for health evaluation and for measure to improve life quality (WHO 2015). HBM studies are used to ascertain potential health risks and form the basis for follow-up steps that should be taken at the individual and collective levels. These studies also tend to track and follow-up health policies that refer to the monitoring of exposure to toxic trace elements, as well as their quantification during diagnostic and detoxification treatments (Kim et al. 2014; Cui et al. 2017). Since human exposure originates from natural and anthropogenic sources, it is necessary to take into account cumulative effects that can only be assessed by solid tissue analysis, and to evaluate the potential health consequences for the examined population (Stojsavljević et al. 2019). Although whole blood and serum samples are widely used in HBM studies, more detailed information about the intrinsic conditions in the human body can be obtained by analysing solid tissue samples.
Measuring adequate zinc (Zn) intake is important for maintaining the overall health of the population, as low daily Zn intake through food is estimated to affect one-third of the world’s population (Merrington et al. 2021). Zn deficiency results in the disruption of metabolic pathways, causing numerous clinical manifestations such as depletion of immune system function, impairments to physical growth, neurobehavioral changes, sickle cell disease, chronic renal failure, adverse outcomes of pregnancies and cancer development (Nikolic et al. 2016; Barroso et al. 2018). Studies have shown that Zn deficiency is likely to be prevalent in most European countries (Moran et al. 2012). Since Zn is recognised as an essential trace element for human health and development, guidelines have been developed to protect populations from harmful health outcomes that could result from its deficiency (Poddalgoda et al. 2019). The World Health Organization (WHO) states that healthy individuals who are not professionally exposed to Zn have a higher risk of the detrimental health effects caused by Zn deficiency than by its excess (WHO 2001). Zn is widely distributed in the environment and has numerous commercial and industrial uses, but the major source that is relevant to humans comes from food (ATSDR 2005).
Previous studies have reported that there are insufficient amounts of Zn in the soil (Dragović et al. 2008; Nikolić et al. 2016), drinking water (Stojanović et al. 2015) and food (Djinovic-Stojanovic et al. 2017) in Serbia. To resolve the important question of potential Zn deficiency in the Serbian population, in this study, we investigated different clinical samples including serum, cerebrospinal fluid (CSF), whole blood and Zn-rich tissues, primarily thyroid and brain tissues. Since Zn status can vary by sex and age, this study also aimed to reveal these differences.
Materials and methods
Ethics statement
The study was approved by the Ethics Committee of Clinical Centre of Serbia, Belgrade (Ethical License Numbers: 1575/7, 623/1, and 442/3). All individuals voluntarily participated in this research (aged between 18 and 65 years), and written informed consent was obtained from every participant according to the Declaration of Helsinki. Patients with chronic medical condition such as diabetes, kidney failure, unstable coronary disease, moderate and severe hypertension, lung disease, chronic autoimmune disease and cancer, professional exposure to Zn, and smokers were excluded from the study group to avoid the effect of confounding factors on the Zn profile. Parameters such as sex and age were collected from the patient’s medical history.
Sample collection
Whole blood (n=314; female/male ratio=156/158; average age: 50±2 years) was collected by cubital venepuncture from healthy volunteers into trace metal-free evacuated tubes (BD Vacutainer) after an overnight fast. The first Vacutainer with whole blood was immediately frozen, while the second one was left to coagulate for 30 min and the serum was prepared and separated after centrifugation at 3000×g.
Healthy thyroid tissue samples were collected during thyroidectomy by excision from patients who were operated on for benign thyroid diseases (n=111, female/male ratio=88/23; average age: 50±5 years). Since one-half or the whole thyroid is surgically removed depending on the tumour size and location, healthy thyroid tissue samples were collected at the greatest possible distance from a benign tumour, which was well demarked. Histopathological analysis of healthy thyroid tissues did not reveal any pathological changes that could interfere with the results of the study.
Healthy brain tissue samples were collected from patients who were operated on for benign tumours (n=57, female/male ratio=25/32; average age: 50±3years). CSF was collected routinely from patients with hydrocephalus during a surgical shunt procedure. The clinical preoperative diagnosis of hydrocephalus was made before CSF sampling. In cases of brain tissue collection, a definitive diagnosis was confirmed by histopathological analysis. Because only healthy brain tissues were analysed, they were collected at a safe distance from the benign tumour mass, which is a regular surgical technique in terms of resection extent, and it does not introduce any additional risk to patient health. All samples were stored at −80°C until analysis.
Chemicals and instrumentation
All chemicals were supplied by Merck (Darmstadt, Germany). A single standard solution of Zn (10 mg/L) was used to prepare intermediate standard solutions. The obtained linearity of the calibration curve was above 0.999. For the correction of the matrix interferences, the internal standard solution of Ga (10 mg/L) was used after final dilution to 10 μg/L. This solution was equally distributed in the blank, standard solutions and in samples through a second channel of the peristaltic pump. To check the accuracy of the analytical method, the following standard reference materials (SRMs) were used: whole blood L-2 (SERO210205, Norway) and bovine liver (1577c, NIST, USA). All samples were decomposed by microwave digestion (ETHOS 1 Advanced System, Milestone, Italy). For the quantification of Zn, inductively coupled plasma mass spectrometry (ICP-MS, iCAP Qc, Thermo Scientific, UK) was used.
Sample preparation
All samples were weighed on an analytical balance and about 0.5 g of each sample was placed into a microwave cuvette. Nitric acid (65%) and hydrogen peroxide (30%) were added to each cuvette at a ratio of 4:1 (v/v). The following temperature program was set for digestion of whole blood, serum and CSF samples: 3 min heating to 90°C, 5 min heating to 150°C, 5 min heating to 190°C and 20 min heating at 190°C. Thyroid tissue and brain tissue samples were digested as follows: 4 min to 100°C, 5 min to 150°C, 5 min to 160°C and 20 min heating at 180°C. Decomposed samples were diluted to 10 mL with ultrapure water.
Data analysis
Descriptive statistics and the Mann Whitney U test at a significance level of p=0.05 were performed using SPSS statistical software (IBM SPSS Statistics v.20). The results were presented as the mean, standard deviation (SD), geometric mean (GM) and percentiles (Ps) from the 2.5th to the 97.5th. All figures were drawn using GraphPad Prism 5.0 (GraphPad, La Jolla, CA, USA).
Results and discussion
The amounts of Zn were found to be highest in thyroid tissue, followed by whole blood, brain tissue, serum and CSF samples (Table 1). Differences in Zn status between sex (female/male) and age (<50 years versus ≥50 years) are given in Tables 2 and 3. The amount of Zn amount in serum, whole blood and healthy thyroid tissue was significantly higher in males compared to females, and in individuals older than 50. Sex and age showed no significant differences in Zn amounts relative to CSF and healthy brain tissues. The differences between the amounts of Zn in the analysed clinical samples among different populations worldwide are given in Figs. 1, 2, 3, 4, and 5.
Table 1.
Mean, standard deviation (SD) and median Zn values for the analysed samples (ng/g)
| Serum | Whole blood | CSF | Brain tissue | Thyroid tissue | |
|---|---|---|---|---|---|
| mean | 574 | 4969 | 37.9 | 2793 | 5871 |
| SD | 139 | 1130 | 16.9 | 989 | 1201 |
| median | 526 | 4675 | 33.9 | 3003 | 5806 |
Table 2.
Percentile (P) values for Zn in all analysed samples according to sex and age (ng/g)
| P2.5 | P10 | P25 | P50 | P75 | P95 | P97.5 | ||
|---|---|---|---|---|---|---|---|---|
| Serum | Female | 371 | 431 | 467 | 509 | 619 | 748 | 771 |
| Male | 407 | 418 | 479 | 568 | 731 | 827 | 843 | |
| < 50 years | 398 | 419 | 456 | 509 | 595 | 671 | 672 | |
| ≥ 50 years | 375 | 440 | 495 | 620 | 746 | 834 | 851 | |
| Whole blood | ||||||||
| Female | 3303 | 3320 | 4083 | 4630 | 5178 | 7016 | 7685 | |
| Male | 4312 | 4390 | 5575 | 5612 | 6402 | 7084 | 7389 | |
| < 50 years | 3612 | 3798 | 4010 | 4531 | 5136 | 6483 | 6753 | |
| ≥ 50 years | 3365 | 3984 | 5032 | 5465 | 6091 | 7624 | 7712 | |
| CSF | ||||||||
| Female | 12 | 14 | 19 | 34 | 40 | 62 | 64 | |
| Male | 18 | 28 | 32 | 42 | 53 | 75 | 78 | |
| < 50 years | 10 | 12 | 17 | 31 | 38 | 60 | 62 | |
| ≥ 50 years | 19 | 25 | 29 | 39 | 50 | 71 | 74 | |
| Brain tissue | ||||||||
| Female | 1851 | 1989 | 2525 | 2611 | 2623 | 3431 | 3645 | |
| Male | 1430 | 2793 | 3023 | 3031 | 3153 | 3947 | 4010 | |
| < 50 years | 1840 | 1957 | 2516 | 2601 | 2602 | 3405 | 3631 | |
| ≥ 50 years | 1469 | 2765 | 2992 | 3002 | 3134 | 3924 | 3994 | |
| Thyroid tissue | ||||||||
| Female | 1840 | 3852 | 3031 | 5667 | 7533 | 9938 | 10341 | |
| Male | 3112 | 5381 | 3629 | 7531 | 8526 | 9924 | 10522 | |
| < 50 years | 2041 | 2963 | 3706 | 5221 | 7508 | 9621 | 9944 | |
| ≥ 50 years | 1763 | 3688 | 4831 | 4883 | 8752 | 10213 | 10432 | |
Table 3.
Geometric mean (GM) and p-values for Zn in all analysed samples according to sex and age (ng/g)
| Serum | Whole blood | CSF | Brain tissue | Thyroid tissue | ||
|---|---|---|---|---|---|---|
| Total | 552 | 5060 | 35.1 | 2616 | 5578 | |
| Sex | Female | 537 | 4710 | 30.3 | 2570 | 5329 |
| Male | 588 | 5701 | 39.0 | 2865 | 6466 | |
| p-value | 0.033 | 0.042 | 0.903 | 0.658 | 0.021 | |
| Age | < 50 years | 510 | 4649 | 37.7 | 2780 | 5178 |
| ≥ 50 years | 597 | 5373 | 42.1 | 2912 | 6036 | |
| p-value | 0.029 | 0.039 | 0.750 | 0.693 | 0.033 |
Fig. 1.

Comparison of the amounts of Zn in serum samples between population groups worldwide (ng/g)
Fig. 2.

Comparison of the amounts of Zn in whole blood samples between population groups worldwide (ng/g)
Fig. 3.
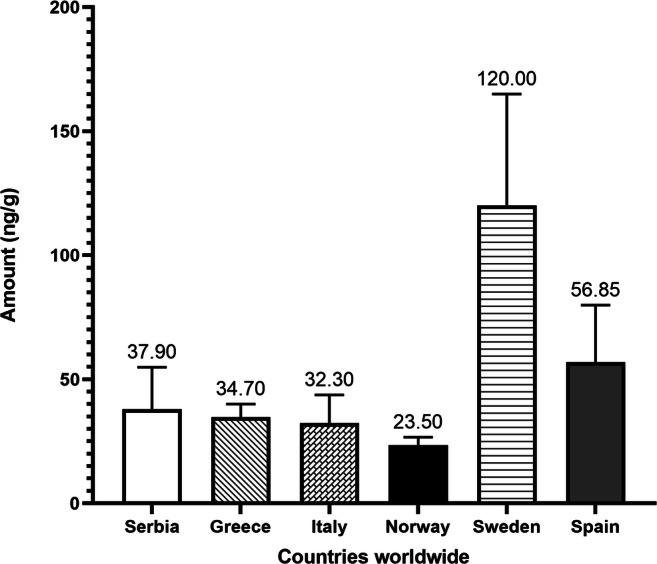
Comparison of the amounts of Zn in cerebrospinal fluid (CSF) samples between population groups worldwide (ng/g)
Fig. 4.
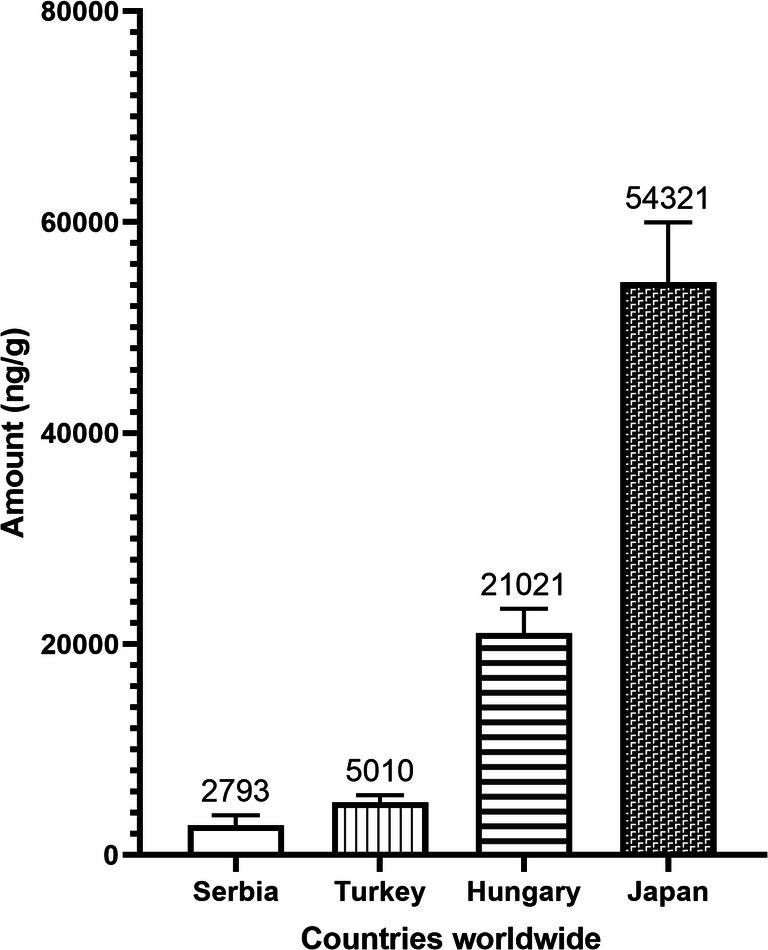
Comparison of the amounts of Zn in brain tissue samples between population groups worldwide (ng/g)
Fig. 5.

Comparison of the amounts of Zn in thyroid tissue samples between population groups worldwide (ng/g)
Since Zn intake is mainly through food ingestion, the current Zn status in the Serbian population is a cause of concern. The grain grown on all our lowland soils is poor in Zn (21 mg/kg), and even lower Zn concentrations were found in flour samples made from these grains. Since wheat bread is the basic food in the Serbian population, the low amount of Zn reported in the wheat grain is a serious concern with regard to human health (Nikolic et al. 2016). Studies have shown reduced Zn content in a wide range of foodstuffs available at local markets (Popović et al. 2017; Djinovic-Stojanovic et al. 2017). It was reported that the Zn content in canned fish was in an adequate range, as provided by National Food Databases (NFDs) (Popović et al. 2017), but it was emphasised that canned fish cannot be considered an important dietary source of Zn for the Serbian population (Popović et al. 2017). The Zn content in chicken and pork products that are part of the Serbian diet was 5- to 80-fold lower, respectively, than the amounts reported in studies conducted in other countries (Djinovic-Stojanovic et al. 2017). The United States Environmental Protection Agency (US EPA) states that the minimum amount of Zn required for normal functioning of the body is 5.5 mg/day. It was determined that the amount of Zn with potentially harmful effects on health is 60 mg/day, which is significantly more than the amount consumed daily by the Serbian population (Djinovic-Stojanovic et al. 2017); the possible toxic effects of excessive Zn intake have been mentioned by Bulat et al. (2017). They have stated that although it is beneficial for the overall health, excessive intake of Zn has toxic effects on the body (Bulat et al. 2017). The proposed reference dose (RfD) value of 0.3 mg Zn/kg/day is based on the derived minimal effect level (DMEL) on the activity of Cu2+/Zn2+-superoxide dismutase (SOD), which is an important component of the antioxidative defence system that can become insufficient as a result of Zn deficiency and subsequently lead to oxidative stress. Zn deficiency is common in countries where the diet is primarily based on vegetables. Considering that Zn tends to bind to phytates, its gastrointestinal absorption in the body can be reduced (El Missiry et al. 2014). Yedomon et al. (2016) noted that Zn deficiency is present in the rural area of Northern Benin due to its low intake via food. The mean dietary Zn intake in the adult Serbian population is below the recommended values for both genders (15 mg/day, established by the EPA 2005), with 9.1 mg/day for males and 7.3 mg/day for females (Knez et al. 2017).
Serum and/or plasma are the most commonly used clinical samples in HBM studies. These samples have been observed to reflect Zn supplementation, especially in people with a low or moderately low Zn status (Wieringa et al. 2015). Comparing the mean Zn serum values with the results for other populations, it was found that the participants in Serbia had twofold lower Zn concentrations than populations of the USA (Hennigar et al. 2018, Harrington et al. 2014), France (Arnaud et al. 2010) and New Zealand (de Jong et al. 2001). Hess et al. (2007) pointed out that the serum Zn content can vary according to sex and age, and our findings are in agreement with this study, and also with the mean values of the Spanish population (520 μg/L for males and 480 μg/L for females) (Henríquez-Hernández et al. 2020). However, the mean Zn serum value in this study was lower compared to results from Poland (824 μg/L) (Marcellini et al. 2007), Italy (732 μg/L) (Marcellini et al. 2007), Germany (830 μg/L) (Marcellini et al. 2007), Greece (741 μg/L) (Marcellini et al. 2007), France (928 μg/L) and Sweden (728 μg/L) (Schultze et al. 2014). Although a universal reference range for Zn is difficult to provide, each country needs to determine its own reference range. Compared to the reported range from 800–1200 μg/L (Burtis et al. 2012), the Serbian population had a twofold lower serum Zn concentration.
Whole blood analysis can provide an insight into the overall health of the investigated population and is widely used in HBM studies. When compared to serum/plasma samples, the content of Zn in whole blood is significantly higher and can be explained as due to the high amount of Zn in the red blood cells. Reported Zn values for whole blood samples in the US (Harrington et al. 2014), Canadian (Saravanabhavan et al. 2016) and Czech populations (Batariova et al. 2006) were about twofold higher than the result obtained herein (Fig. 2); however, values similar to ours were reported in the French population (Cesbron et al. 2013). Slightly higher blood values of Zn for the Serbian population were found when compared to Italian volunteers (4298±623 μg/L) (de Oliveira et al. 2020).
The blood-brain barrier (BBB) plays an important role in brain microenvironment homeostasis and is also included in regulating Zn balance in the brain tissue (Qi and Liu 2019). CSF is not a typical type of sample for HBM studies as it is difficult to collect. Since it could provide additional insight into Zn status, we aimed to reinforce the results of our study by including CSF samples. Our data are in agreement with results obtained for the Greek (Kapaki et al. 1989) and Italian (Alimonti et al. 2007) populations, but the Zn content in the Norwegian population (Melo et al. 2003) was about 1.2-fold lower than our value, whereas the Spanish and Swedish populations had 5- and 1.5-fold higher Zn contents, respectively (Roos et al. 2013). No significant difference in the Zn status in CSF was observed between populations.
Zn has a role in increasing the permeability of the BBB, which protects nervous tissue from harmful agents. The results for brain tissue samples presented herein are 2-, 8- and 10-fold lower when compared to the Turkish (Arslan et al. 2011), Spanish (Garcia et al. 2001) and Hungarian populations (Andrasi et al. 1993), respectively, while the Japanese population (Katoh et al. 2002) had a 20-fold higher value (52 μg/g) than the Serbian population.
A comparative analysis of the amounts of Zn in thyroid tissue in different population groups was carried out. In the Japanese (101 μg/g) (Błazewicz et al. 2010) and Polish populations (110 μg/g) (Katoh et al. 2002), the concentration of Zn was 20-fold higher, whereas in the Turkish (Baltaci et al. 2017) and Russian populations (92.5 μg/g) (Zaichick and Zaichick 2018), it was around 15-fold higher than that reported in our data. These results point to the contribution of Zn deficiency to the increased incidence of benign and malignant thyroid diseases in Serbia.
The role of Zn as a modulating factor in the clinical course of viral infections has been noted among individuals with Zn deficiency, and in light of the ongoing COVID-19 pandemic, recent studies have analysed the effect of Zn on the severity of SARS-CoV-2 infection. Thus, COVID-19 patients that were Zn deficient had more health complications caused by the primary disease (Jothimani et al. 2020; Wessels et al. 2020). Up to April 2, 2021, Serbia has 605,406 registered cases of COVID-19 and 5345 COVID-19-related deaths with a progressively increasing daily number of infected patients (IPHS 2021). Therefore, taking into consideration the possible positive effects on the patients’ health, oral Zn supplementation has been implemented into preventive and therapeutic protocols against COVID-19.
Our study was conducted on different human clinical samples that provided a comprehensive insight into the general profile of the Zn status and its distribution. This is one of the largest samples of Caucasian individuals on whom Zn profiling has been conducted, and to the best of our knowledge, it is the first of its kind as regards the type of analysed samples.
Limitations of the study include the analysis of factors that affect the amount of Zn in the body, such as the type of diet, the presence of unhealthy habits and the possible existence of other diseases, as well as random sampling without a defined region in the country.
Conclusion
By comparing our results with data for other populations around the world, we have shown for the first time that the Serbian population could be Zn deficient. Analysis of serum samples revealed about 2-fold lower amounts of Zn in the Serbian population when compared to all other populations worldwide. A similar trend was obtained for whole blood samples. Males had significantly higher amounts of Zn compared to females in the serum, whole blood and thyroid tissue samples. Also, higher Zn amounts were found in the older group of subjects (≥ 50 years). Most importantly, the amounts of Zn in thyroid and brain tissues were 10- and 20-fold lower, respectively, than reported in the literature. Therefore, adequate oral Zn supplementation and/or fortification of foodstuff should be considered in order to prevent the harmful effects caused by Zn deficiency.
Author contribution
JJ analysed the samples and wrote the first version of the manuscript. AS designed the study and contributed to the writing of the final version of the manuscript. BR and LjV collected the clinical samples. JJ, BR, SBM, VA, DM and AS participated in writing through reviewing and editing. All authors have read and approved the final version of the paper.
Funding
This research was financially supported by the Ministry of Education, Science and Technological
Development of the Republic of Serbia Contract Number: 451-03-9/2021-14/ 200288.
Data availability
The datasets used and/or analysed during the study are available from the corresponding author on reasonable request.
Declarations
Ethical approval and consent to participate
The study was approved by the Ethics Committee of the Clinical Centre of Serbia, Belgrade (Ethical License Nos.: 1575/7, 623/1 and 442/3). All individuals voluntarily participated in this research and the written informed consent was obtained from every participant according to the Declaration of Helsinki.
Consent to publish
All individuals that participated in this study have signed a written informed consent.
Conflict of interest
The authors declare no competing interests.
Footnotes
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- Alimonti A, Bocca B, Pino A, Ruggieri F, Forte G, Sancesario G. Elemental profile of cerebrospinal fluid in patients with Parkinson’s disease. J Trace Elem Med Biol. 2007;21:234–241. doi: 10.1016/j.jtemb.2007.05.001. [DOI] [PubMed] [Google Scholar]
- Andrási E, Suhajda M, Sáray I, Bezúr L, Ernyei L, Réffy A. Concentration of elements in human brain: glioblastoma multiforme. Sci Total Environ. 1993;140:399–402. doi: 10.1016/0048-9697(93)90036-6. [DOI] [PubMed] [Google Scholar]
- Arnaud J, Touvier M, Galan P, Andriollo-Sanchez M, Ruffieux D, Roussel AM, Hercberg S, Favier A. Determinants of serum zinc concentrations in a population of French middle-age subjects (SU.VI.MAX cohort) Eur J Clin Nutr. 2010;64:1057–1064. doi: 10.1038/ejcn.2010.118. [DOI] [PubMed] [Google Scholar]
- Arslan M, Demir H, Arslan H, Gokalp AS, Demir C. Trace elements, heavy metals and other biochemical parameters in malignant glioma patients. Asian Pac J Cancer Prev. 2011;12:447–451. [PubMed] [Google Scholar]
- ATSDR ( 2005) Toxicological profile for zinc. U.S. Department of health and human services public health service. Agency for toxic substances and disease registry [PubMed]
- Baltaci AK, Dundar TK, Aksoy F, Mogulkoc R. Changes in the serum levels of trace elements before and after the operation in thyroid cancer patients. Biol Trace Elem Res. 2017;175:57–64. doi: 10.1007/s12011-016-0768-2. [DOI] [PubMed] [Google Scholar]
- Barroso I, Farinha R, Guimarães JT. Proper zinc evaluation in clinical practice: effect of sample type and it’s stability. Clin Biochem. 2018;59:93–95. doi: 10.1016/j.clinbiochem.2018.07.001. [DOI] [PubMed] [Google Scholar]
- Batáriová A, Spevácková V, Benes B, Cejchanová M, Smíd J, Cerná M. Blood and urine levels of Pb, Cd and Hg in the general population of the Czech Republic and proposed reference values. Int J Hyg Environ Health. 2006;209:359–366. doi: 10.1016/j.ijheh.2006.02.005. [DOI] [PubMed] [Google Scholar]
- Berman T, Goldsmith R, Levine H, Grotto I. Human biomonitoring in Israel: Recent results and lessons learned. Int J Hyg Environ Health. 2016;220:6–12. doi: 10.1016/j.ijheh.2016.09.008. [DOI] [PubMed] [Google Scholar]
- Błazewicz A, Dolliver W, Sivsammye S, Deol A, Randhawa R, Orlicz-Szczesna G, Błazewicz R. Determination of cadmium, cobalt, copper, iron, manganese, and zinc in thyroid glands of patients with diagnosed nodular goitre using ion chromatography. J Chromatogr B Anal Technol Biomed Life Sci. 2010;878:34–38. doi: 10.1016/j.jchromb.2009.11.014. [DOI] [PubMed] [Google Scholar]
- Bulat Z, Đukić-Ćosić D, Antonijević B, Buha A, Bulat P, Pavlović Z, Matović V. Can zinc supplementation ameliorate cadmium-induced alterations in the bioelement content in rabbits? Arh Hig Rada Toksikol. 2017;68:38–45. doi: 10.1515/aiht-2017-68-2919. [DOI] [PubMed] [Google Scholar]
- Burtis CA, Ashwood ER, Bruns DE, Tietz NW (2012) Textbook of clinical chemistry and molecular diagnostics, 5th ed., Elsevier, ISBN: 978-1-4160-6164-9.
- Cesbron A, Saussereau E, Mahieu L, Couland I, Guerbet M, Goulle JP. Metallic profile of whole blood and plasma in a series of 106 healthy volunteers. J Anal Toxicol. 2013;37:401–405. doi: 10.1093/jat/bkt046. [DOI] [PubMed] [Google Scholar]
- Cui Y, Zhong Q, Hu M, Sheng J, Yang Y, Liang L, Wang X, Yang Y, Zhou M, Huang F. Human biomonitoring of eight trace elements in urine of residents living in rural areas along the Yangtze River, China. Environ Sci Pollut Res. 2017;24:27963–27973. doi: 10.1007/s11356-017-0414-3. [DOI] [PubMed] [Google Scholar]
- de Jong N, Gibson RS, Thomson CD, Ferguson EL, McKenzie JE, Green TJ, Horwath CC. Selenium and zinc status are suboptimal in a sample of older New Zealand women in a community-based study. J Nutr. 2001;131:2677–2684. doi: 10.1093/jn/131.10.2677. [DOI] [PubMed] [Google Scholar]
- de Oliveira M, Gianeti TMR, da Rocha FCG, Lisboa-Filho PN, Piacenti-Silva M. A preliminary study of the concentration of metallic elements in the blood of patients with multiple sclerosis as measured by ICP-MS. Sci Rep. 2020;10:10. doi: 10.1038/s41598-020-69979-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Djinovic-Stojanovic JM, Nikolic DM, Vranic DV, Babic JA, Milijasevic MP, Pezo LL, Jankovic SD. Zinc and magnesium in different types of meat and meat products from the Serbian market. J Food Compos Anal. 2017;59:50–54. doi: 10.1016/j.jfca.2017.02.009. [DOI] [Google Scholar]
- Dragović S, Mihailović N, Gajić B. Heavy metals in soils: distribution, relationship with soil characteristics and radionuclides and multivariate assessment of contamination sources. Chemosphere. 2008;72:491–495. doi: 10.1016/j.chemosphere.2008.02.063. [DOI] [PubMed] [Google Scholar]
- El Missiry M, Hussein MH, Khalid S, Yaqub N, Khan S, Itrat F, Uderzo C, Faulkner L (2014) Assessment of serum zinc levels of patients with thalassemia compared to their siblings. Anemia 1–6. 10.1155/2014/125452 [DOI] [PMC free article] [PubMed]
- EPA (2005) Toxicological review of zinc and compounds. EPA/635/R-05/002
- García F, Ortega A, Domingo JL, Corbella J. Accumulation of metals in autopsy tissues of subjects living in Tarragona county, Spain. J Environ Sci Heal A. 2001;36:1767–1786. doi: 10.1081/ESE-100106258. [DOI] [PubMed] [Google Scholar]
- Harrington JM, Young DJ, Essader AS, Sumner SJ, Levine KE. Analysis of human serum and whole blood for mineral content by ICP-MS and ICP-OES: development of a mineralomics method. Biol Trace Elem Res. 2014;160:132–142. doi: 10.1007/s12011-014-0033-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hennigar SR, Lieberman HR, Fulgoni VL, McClung JP. Serum zinc concentrations in the US population are related to sex, age, and time of blood draw but not dietary or supplemental zinc. J Nutr. 2018;148:1341–1351. doi: 10.1093/jn/nxy105. [DOI] [PubMed] [Google Scholar]
- Henríquez-Hernández LA, Romero D, González-Antuña A et al (2020) Biomonitoring of 45 inorganic elements measured in plasma from Spanish subjects: a cross-sectional study in Andalusian population. Sci Total Env 135750. 10.1016/j.scitotenv.2019.135750 [DOI] [PubMed]
- Hess SY, Peerson JM, King JC, Brown KH. Use of serum zinc concentration as an indicator of population zinc status. Food Nutr Bull. 2007;28:403–429. doi: 10.1177/15648265070283S303. [DOI] [PubMed] [Google Scholar]
- Institute of Public Health of Serbia (IPHS) “Dr Milan Jovanović Batut”, last seen on 02.04.2021. https://covid19.rs/
- Jothimani D, Kailasam E, Danielraj S, Nallathambi B, Ramachandran H, Sekar P, Manoharan S, Ramani V, Narasimhan G, Kaliamoorthy I, Rela M. COVID-19: poor outcomes in patients with Zinc deficiency. Int J Infect Dis. 2020;100:343–349. doi: 10.1016/j.ijid.2020.09.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kapaki E, Segditsa J, Papageorgiou C. Zinc, copper and magnesium concentration in serum and CSF of patients with neurological disorders. Acta Neurol Scand. 1989;79:373–378. doi: 10.1111/j.1600-0404.1989.tb03803.x. [DOI] [PubMed] [Google Scholar]
- Katoh Y, Sato T, Yamamoto Y. Determination of multielement concentrations in normal human organs from the Japanese. Biol Trace Elem Res. 2002;90:57–70. doi: 10.1385/BTER:90:1-3:57. [DOI] [PubMed] [Google Scholar]
- Kim K, Park H, Lee JH. Urinary concentrations of trichlorophenols in the Korean adult population: results of the National Human Biomonitoring Survey. Environ Sci Pollut Res. 2014;21:2479–2485. doi: 10.1007/s11356-013-2180-1. [DOI] [PubMed] [Google Scholar]
- Knez M, Nikolic M, Zekovic M, Stangoulis JCR, Gurinovic M, Glibetic M. The influence of food consumption and socio-economic factors on the relationship between zinc and iron intake and status in a healthy population. Public Health Nutr. 2017;20:2486–2498. doi: 10.1017/S1368980017001240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marcellini F, Giuli C, Papa R, Gagliardi C, Dedoussis G, Herbein G, Fulop T, Monti D, Rink L, Jajte J, Mocchegiani E. Zinc status, psychological and nutritional assessment in old people recruited in five European countries: zincage study. Biogerontology. 2007;7:339–345. doi: 10.1007/s10522-006-9048-4. [DOI] [PubMed] [Google Scholar]
- Melø TM, Larsen C, White LR, Aasly J, Sjøbakk TE, Flaten TP, Sonnewald U, Syversen T. Manganese, copper, and zinc in cerebrospinal fluid from patients with multiple sclerosis. Biol Trace Elem Res. 2003;93:1–8. doi: 10.1385/BTER:93:1-3:1. [DOI] [PubMed] [Google Scholar]
- Merrington G, Peters A, Wilson I, Cooper C, van Assche F, Ryan A. Deriving a bioavailability-based zinc environmental quality standard for France. Environ Sci Pollut Res. 2021;28:1789–1800. doi: 10.1007/s11356-020-10603-8. [DOI] [PubMed] [Google Scholar]
- Moran VH, Stammers AL, Warthon Medina M, Patel S, Dykes F, Souverein OW, Dullemeijer C, Pérez-Rodrigo C, Serra-Majem L, Nissensohn M, Lowe NM. The relationship between zinc intake and serum/plasma zinc concentration in children: a systematic review and dose-response meta-analysis. Nutrients. 2012;4:841–858. doi: 10.3390/nu4080841. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nikolic M, Nikolic N, Lj K, Pavlovic J, Bosnic P, Stevic N, Savic J, Hristov N. The assessment of soil availability and wheat grain status of zinc and iron in Serbia: implications for human nutrition. Sci Total Environ. 2016;553:141–148. doi: 10.1016/j.scitotenv.2016.02.102. [DOI] [PubMed] [Google Scholar]
- Poddalgoda D, Macey K, Hancock S. Derivation of biomonitoring equivalents (BE values) for zinc. Regul Toxicol Pharmacol. 2019;106:178–186. doi: 10.1016/j.yrtph.2019.04.018. [DOI] [PubMed] [Google Scholar]
- Popović AR, Relić DJ, Vranić DV, Babić-Milijašević JA, Pezo LL, Đinović-Stojanović JM. Canned sea fish marketed in Serbia: their zinc, copper, and iron levels and contribution to the dietary intake. Arh Hig Rada Toksikol. 2017;69:55–60. doi: 10.2478/aiht-2018-69-3069. [DOI] [PubMed] [Google Scholar]
- Qi Z, Liu KJ. The interaction of zinc and the blood-brain barrier under physiological and ischemic conditions. Toxicol Appl Pharmacol. 2019;364:144–119. doi: 10.1016/j.taap.2018.12.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roos PM, Vesterberg O, Syversen T, Flaten TP, Nordberg M. Metal concentrations in cerebrospinal fluid and blood plasma from patients with amyotrophic lateral sclerosis. Biol Trace Elem Res. 2013;151:159–170. doi: 10.1007/s12011-012-9547-x. [DOI] [PubMed] [Google Scholar]
- Saravanabhavan G, Werry K, Walker M, Haines D, Malowany M, Khoury C. Human biomonitoring reference values for metals and trace elements in blood and urine derived from the Canadian Health Measures Survey 2007–2013. Int J Hyg Environ Health. 2016;220:189–200. doi: 10.1016/j.ijheh.2016.10.006. [DOI] [PubMed] [Google Scholar]
- Schultze B, Lind PM, Larsson A, Lind L. Whole blood and serum concentrations of metals in a Swedish population-based sample. Scand J Clin Lab Invest. 2014;74:143–148. doi: 10.3109/00365513.2013.864785. [DOI] [PubMed] [Google Scholar]
- Stojanović ZS, Švarc-Gajić JV, Đorđević MZ, Grahovac NL, Vasin JR, Đurović AD, Kravić SZ. Study on the quality of ground, spring and river waters in South–East Serbia. Hem Ind. 2015;69:185–192. doi: 10.2298/HEMIND131115033S. [DOI] [Google Scholar]
- Stojsavljević A, Rovčanin B, Krstić Đ, Borković-Mitić S, Paunović I, Kodranov I, Gavrović-Jankulović M, Manojlović D. Evaluation of trace metals in thyroid tissues: comparative analysis with benign and malignant thyroid diseases. Ecotoxicol Environ Saf. 2019;83:109479. doi: 10.1016/j.ecoenv.2019.109479. [DOI] [PubMed] [Google Scholar]
- Wessels I, Rolles B, Rink L (2020) The potential impact of zinc supplementation on COVID-19 pathogenesis. Front Immunol 11. 10.3389/fimmu.2020.01712 [DOI] [PMC free article] [PubMed]
- WHO ( 2001) Environmental Health Criteria 221. Zinc. World Health Organization Geneva
- WHO (2015) Human biomonitoring: facts and figures. Copenhagen: WHO Regional Office for Europe
- Wieringa FT, Dijkhuizen MA, Fiorentino M, Laillou A, Berger J. Determination of zinc status in humans: which indicator should we use? Nutrients. 2015;7:3252–3263. doi: 10.3390/nu7053252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yedomon B, Menudier A, Etangs FLD, Anani L, Fayomi B, Druet-Cabanac M, Moesch C. Biomonitoring of 29 trace elements in whole blood from inhabitants of Cotonou (Benin) by ICP-MS. J Trace Elem Med Biol. 2016;43:38–45. doi: 10.1016/j.jtemb.2016.11.004. [DOI] [PubMed] [Google Scholar]
- Zaichick V, Zaichick S. Associations between age and 50 trace element contents and relationships in intact thyroid of males. Aging Clin Exp Res. 2018;30:1059–1070. doi: 10.1007/s40520-018-0906-0. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used and/or analysed during the study are available from the corresponding author on reasonable request.