

Abstract
Methods
Randomized controlled trials on manual acupuncture treatment of DPN were retrieved from the Medline, Web of Science, PubMed, Cochrane Library, EMBASE, CNKI, WanFang, and VIP databases. Extracted research data were summarized in the tables, and methodological assessment was performed using the risk-of-bias assessment tool of Cochrane. Meta-analysis was performed by Revman 5.3, Stata 14.0, and TSA 0.9.5.10 Beta software.
Results
A total of 18 randomized clinical trials (RCTs) were recruited: (1) 11 RCTs were acupuncture alone compared with vitamin B; (2) 7 RCTs were acupuncture combined with vitamin B compared with vitamin B, involving 1200 participants. Acupuncture alone improved clinical efficacy (P < 0.05) and nerve conduction velocity of the four peripheral nerves: peroneal nerve, tibial nerve, median nerve, and ulnar nerve (P < 0.05), but there was no significant difference between the group of acupuncture alone and the group of vitamin B (P = 0.36 > 0.05) in improving median nerve SCV (sensory nerve conduction velocity). Acupuncture combined with vitamin B improved clinical efficacy and nerve conduction velocity of the three peripheral nerves, peroneal nerve, tibial nerve, and median nerve (P < 0.05), and decreased the scores of the Toronto clinical scoring system (TCSS) (P < 0.05).
Conclusion
Acupuncture alone and vitamin B combined with acupuncture are more effective in treating DPN compared to vitamin B. However, more high-quality RCTs on vitamin B combined with acupuncture are required to confirm our results.
1. Introduction
Diabetic peripheral neuropathy (DPN) has been described as “signs and symptoms of peripheral nerve dysfunction in patients with diabetes mellitus (DM) after the exclusion of other causes” [1]. Physical pain, numbness, decreased sensation, or other abnormal sensations are the main symptoms. Chronic distal symmetric polyneuropathy (DSPN) is the most common diabetic neuropathy [1]. An epidemiological study found that DPN prevalence is 7% for patients with type 1 diabetes and 22% for type 2 diabetes [2]. Most patients who were diagnosed with DPN present with pain, but a considerable number of patients without pain as a symptom were misdiagnosed and therefore did not receive adequate and timely treatment [3]. Mecobalamin is recommended for the treatment of DPN in patients with type 2 DM according to the China Food and Drug Administration guideline [4]. Although duloxetine and pregabalin are still the drug of choice (DOC) for treating painful diabetic neuropathy (PDN), adverse drug reactions in the cardiovascular system and digestive system have often been reported with significant safety concerns [5].
The prevention and management of DPN currently focus primarily on glucose control [6], while the signs and symptoms of DPN are always overlooked. In China, acupuncture is regarded as a “relatively safe” therapy, which is widely accepted with a long history, good reliability, feasibility, and ease of operation [7]. It was frequently used for treating conditions in the nervous system to avoid the severe side effects of chemical drugs.
Nerve conduction velocity is the gold standard to diagnose DPN [8], and TCSS is an effective tool for screening DPN with three domains including the neurological symptom score, neurological reflex score, and sensory function score to assess the DPN patient's symptoms and/or signs. TCSS is highly consistent with the neuroelectrophysiological function where lower scores indicate greater relief [9, 10].
DPN is considered by traditional Chinese medicine as one of “Bi Zheng (arthralgia syndrome)” or “Wei zheng (flaccidity syndrome)” under a larger category of “Xiao Ke (consumptive disease).” DPN is caused by blockage of “Qi and Xue (Qi and blood)” from perfusing limbs and muscles; then, it impedes the nourishment of meridians [11]. At this point, acupuncture can be applied to adjust the “Qi and Xue (Qi and blood)” of the human body and dredge the meridians [12]. So far, the RCTs on acupuncture treatment of DPN are poorly designed, with a generally poor methodological quality. What is more, no randomized controlled clinical trial from a multicenter has been published. Only two systematic reviews have been published, one of which analyzed articles until April 2013 while the other review analyzed articles up to June 2017 [13, 14]. However, neither article has further in-depth analysis of heterogeneous indicators. Some limitations of these two studies include the following: (1) not all of the included articles were RCTs; (2) most of the participants had diabetic peripheral neuropathic pain (DPNP) and hence could not represent most DPN; and (3) Chinese databases were not searched [12]. In this review, we solely used RCT data to evaluate the efficacy of acupuncture treatment on DPN. We compared the application of combining acupuncture and vitamin B with vitamin B or compared acupuncture alone with vitamin B in treating DPN, respectively.
2. Materials and Methods
2.1. Study Registration
This protocol of systematic review and meta-analysis has been drafted under the guidance of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses protocols (PRISMA-P). Moreover, it has been registered on the open science framework (OSF) on May 14, 2020 (registration number: DOI 10.17605/OSF.IO/PZ5GC).
2.2. Search Strategy
Keywords such as “acupuncture,” “diabetic peripheral neuropathy,” and “DPN” were used to search against databases including Medline, Web of Science, PubMed, Cochrane Library, EMBASE, CNKI, WanFang, and VIP, for RCTs, systematic reviews, or meta-analyses published by April 5, 2020. There were no language restrictions. The two investigators independently reviewed all literature to determine its inclusion (Hai lun Jiang and Peng Jia). Disagreements were adjudicated by a third investigator (Yi hua Fan). The meta-analysis was conducted following the guidelines of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). The search strategy of EMBASE and CNKI is listed in Table S1, and PubMed search history is listed in Table S3
2.3. Inclusion Criteria
Patients with diabetic peripheral neuropathy.
RCT studies comparing manual acupuncture with vitamin B in the treatment of DPN; the manual acupuncture study group includes both acupuncture alone and acupuncture coupled with vitamin B; the control group was treated only with chemical drugs, and vitamin B must be included.
Primary outcome: (1) clinical efficacy. Secondary outcomes: (1) motor nerve conduction velocity (MCV) of the peroneal nerve; (2) sensory nerve conduction velocity (SCV) of the peroneal nerve; (3) motor nerve conduction velocity (MCV) of the tibial nerve; (4) sensory nerve conduction velocity (SCV) of the tibial nerve; (5) motor nerve conduction velocity (MCV) of the median nerve; (6) sensory nerve conduction velocity (SCV) of the median nerve; (7) motor nerve conduction velocity (MCV) of the ulnar nerve; and (8) Toronto clinical scoring system (TCSS). Supplementary explanation: the definition of clinical efficacy was not similar among trials. The included trials' clinical efficacy evaluation was based on the following criteria [15]:
Effectiveness. Symptoms and/or signs of peripheral nerve dysfunction improved, and MCV or SCV increased.
Ineffectiveness. Symptoms and/or signs of peripheral nerve dysfunction had not improved, or MCV or SCV did not obviously improve.
When the effect of symptoms and/or signs is inconsistent with the effect of nerve conduction velocity, the lower effective parameter is applied to show the comprehensive effect.
2.4. Exclusion Criteria
Duplicated published articles
Nonhuman limb acupoints
Incomplete data from the articles
The trials were rated as low quality by Zhao et al.'s criteria [16]
2.5. Data Extraction
Two independent investigators (Hai lun Jiang and Peng Jia) separately extract data, involving the name of authors, year of publication, sample size, age of participants, duration of DPN, intervention measures, intervention time, outcome indicators, reinforcing and reducing, acupoints, and needle retaining time. When disagreements occurred, two independent investigators (Hai lun Jiang and Peng Jia) discussed to resolve the issues. If disagreements persisted, then the third investigator (Yi hua Fan) was consulted to make the final decision. Additional information was obtained by contacting authors directly via call or email.
2.6. Risk-of-Bias Assessments
Two independent reviewers (Hai lun Jiang and Peng Jia) evaluated the quality of the included RCTs separately, based on the Cochrane risk-of-bias criteria [17]. When disagreements occurred, two independent investigators (Hai lun Jiang and Peng Jia) discussed to resolve the issues. If disagreements persisted, then the third investigator (Yi hua Fan) was consulted to make the final decision.
2.7. Data Synthesis and Statistical Analysis
In this meta-analysis, the Revman 5.3 (developed by the UK's International Cochrane Collaboration) and Stata 14.0 (developed by the USA's StataCorp LLC) software were used for analysis. Relative risks (RR) were used to express dichotomous variables, whereas the mean difference (MD) and 95% confidence interval (CI) were used to denote continuous variables. The chi-squared tests were used to assess statistical heterogeneity. When I2 < 50% or chi-squared test P ≥ 0.1, a fixed-effect model was applied. The source of heterogeneity was analyzed, when I2 > 50% or chi-squared test P < 0.1. In the absence of clinical heterogeneity or methodological heterogeneity, the random-effect model was applied. Statistical significance was set at P < 0.05. To test publication bias, Egger's test was performed. Moreover, a sensitivity analysis was conducted to test the stability of the results.
Besides, trial sequence analysis using TSA 0.9.5.10 Beta (developed by the Copenhagen Trial Unit's Centre for Clinical Intervention Research) was used to calculate the appropriate sample size for the meta-analysis and to assess the statistical boundaries for futility and efficacy. TheXaxis represents the sample size (participants),Yaxis represents the statisticZvalues, two symmetrical red curves represent the boundary value of trial sequence analysis (TSA boundary value), and symmetrical red horizontal dashed lines represent the conventional boundary values (Z = 1.96,P = 0.05(two-sided)). If the cumulativeZvalue does not cross the TSA boundary value or RIS, it indicates that the sample size is insufficient, to recommend continuing the series of experiments. If the cumulative Z value exceeds both the TSA boundary value and the RIS, then the sample size is sufficient. If the cumulative Z value exceeds the TSA boundary value and does not reach the RIS, it means that a reliable conclusion can be drawn in advance even if the sample size is insufficient. According to the TSA method, when the cumulative Z value has crossed the RIS, or the cumulative Z value intersects the TSA boundary value, the series of tests can be recommended to stop (TSA parameter setting: type I error probability 5%, type II error probability of 20%, and the relative risk reduction (RRR = −15%), to estimate the required information size (RIS)) [18].
3. Results
A total of 18 articles were selected, and the process is shown in Figure1 [19–36].
Figure 1.
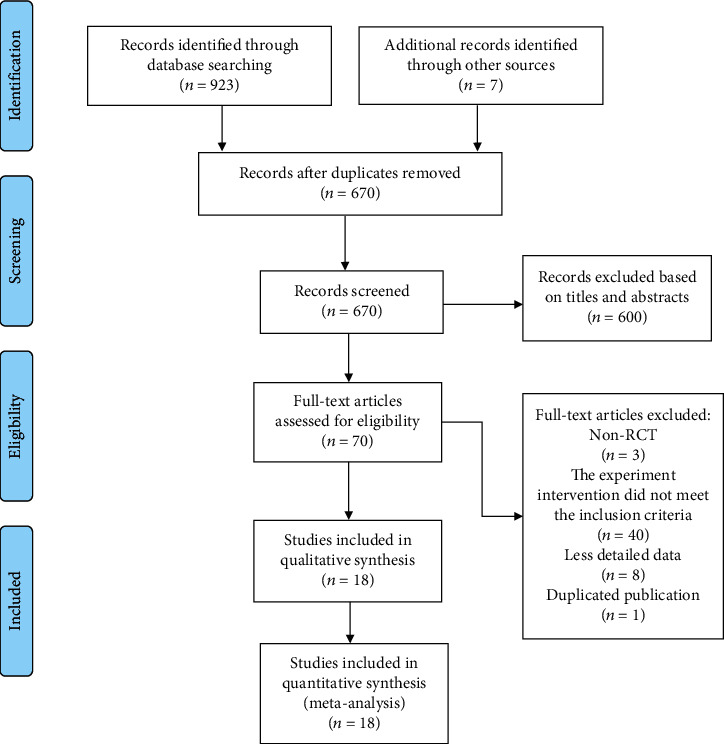
Flow chart of study identification and selection.
Only 7 of 18 randomized trials reported methods of randomization. No trial reported allocation concealment. Blinding does not affect the measure of nerve conduction velocity (NCV), and only one study reported blinding in this analysis. 15 trials showed low risk in blinding participants or outcome assessment. All studies were of low risk of incomplete outcome data, selective reporting, or other bias. Figure 2 outlines the quality and risk-of-bias evaluation of the included studies. Risk-of-bias assessments are shown in Figure 2.
Figure 2.
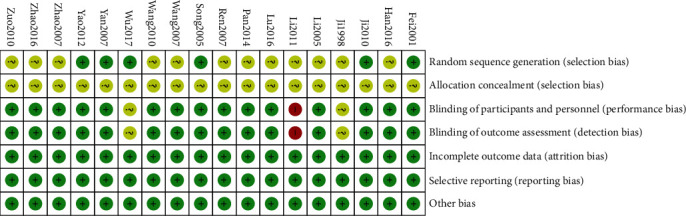
Risk-of-bias summary.
3.1. The Basic Characteristics of the Inclusion Study
Name of author, year of publication, sample size, age of participants, duration of DPN, intervention measures, intervention time, and outcome indicators are summarized in Table 1, and acupoints, reinforcing and reducing, and needle retaining time are summarized in Table 2.
Table 1.
The characteristics of the included trials.
| References | Sample size (T/C) | Age (year) | Disease duration (year) | Intervention | Intervention time (days) | Outcome | |
|---|---|---|---|---|---|---|---|
| Treatment | Control | ||||||
| Fei 2011 | 30/30 | T: 54 ± 1 C: 55 ± 1 |
T: 2.43 ± 2.23 C: 2.53 ± 0.34 |
Ac | Mec (p.o) | 30 | (4), (5) |
| Han 2016 | 42/42 | T: 56.3 C: 56.2 |
/ | Ac | Mec (p.o)+nimodipine (p.o) | 56 | (1), (2), (3) |
| Ji 2010 | 40/40 | T: 60.7 ± 4.26 C: 62.2 ± 4.13 |
T: 3.77 ± 1.16 C: 3.44 ± 1.29 |
Ac | Mec (i.m) | 28 | (1), (4), (5) |
| Li 1998 | 31/22 | / | T: 3 weeks–2 years C: 3 weeks–2 years |
Ac | VitB1, B12 (i.m) | 30 | (1) |
| Li 2005 | 30/30 | All: 56.1 ± 3.2 | / | Ac | Mec (i.v) | 120 | (1), (2), (6) |
| Li 2011 | 14/14 | / | / | Ac+Mec (p.o) | Mec (p.o) | 45 | (9) |
| Lu 2016 | 31/29 | T: 66 ± 7 C: 64 + 7 |
T: 3.6 ± 1.3 C: 3.5 ± 1.1 |
Ac | Lipoic acid (i.v.drip)+alprostadil (i.v.drip) | 30 | (1), (2), (3), (6), (7) |
| Pan 2014 | 42/42 | / | / | Ac+Mec (p.o) | Mec (p.o) | 90 | (1) |
| Ren 2007 | 30/30 | T: 63.±12.58 C: 60.±11.47 |
T: 5.64 ± 4.77 C: 5.81 ± 4.38 |
Ac | VitB1, B12 (i.m) | 30 | (2), (6) |
| Song 2005 | 22/20 | T: 58.9 ± 5.24 C: 58.9 ± 5.24 |
T: 6.91 ± 3.15 C: 6.33 ± 3.56 |
Ac | VitB12 (i.m)+VitB1, B6 (p.o) | 30 | (1), (2), (8) |
| Wang 2007 | 50/30 | T: 55.8 C: 56.1 |
T: 6.5 C: 7 |
Ac+VitB | VitB | 30 | (4), (5), (6), (7) |
| Wang 2010 | 34/32 | T: 56.1 ± 5.33 C: 58.4 ± 8.52 |
T: 2.91 ± 2.38 C: 2.86 ± 2.59 |
Ac+Mec (i.v) | Mec (i.v) | 28 | (2), (3), (6), (7) |
| Wu 2017 | 40/40 | T: 53.4 ± 8.31 C: 52.9 ± 8.45 |
T: 2.62 ± 0.56 C: 2.52 ± 0.48 |
Ac+Mec (p.o) | Mec (p.o) | 14 | (1), (2), (3), (6), (7), (9) |
| Yan 2007 | 46/42 | T: 46.7-74.98 C: 46.5-75.6 |
T: 0.8-12.4 C: 0.7-11.8 |
Ac+Mec (p.o) | Mec (p.o) | 90 | (1), (2), (3) |
| Yao 2012 | 40/40 | T: 54.5 C: 53.4 |
T: 0.67 C: 0.58 |
Ac | Mec (p.o)+nimodipine (p.o) | 28-56 | (1), (2), (3) |
| Zhao 2007 | 30/30 | T: 62.±7.33 C: 62.1 ± 7.93 |
T: 2.71 ± 2.58 C: 2.61 ± 2.22 |
Ac | Mec (p.o) | 60 | (1), (5) |
| Zhao 2016 | 30/30 | All: 53 ± 9.2 | All: 0.58 ± 0.25 | Ac | Mec (p.o)+nimodipine (p.o) | 56 | (1), (2), (3) |
| Zuo 2010 | 40/35 | T: 57.6 C: 57.1 |
T: 8.7 C: 8.5 |
Ac+Mec (i.v) | Mec (i.v) | 28 | (2), (3), (6), (7) |
Abbreviation: T: experimental group; C: control group; Ac: acupuncture; Mec: mecobalamin; p.o: per os; i.m: intramuscular vitamins; i.v: intravenous injection; i.v.drip: intravenous drip; Vit: vitamin. (1) Clinical efficacy; (2) the MCV of the peroneal nerve; (3) the SCV of the peroneal nerve; (4) the MCV of the tibial nerve; (5) the SCV of the tibial nerve; (6) the MCV of the median nerve; (7) the SCV of the median nerve; (8) the MCV of the ulnar nerve; (9) Toronto clinical scoring system (TCSS).
Table 2.
The characteristics of manual acupuncture.
| References | Acupoints | Reinforcing and reducing | Needle retaining time |
|---|---|---|---|
| Fei 2011 | Zusanli (ST36), Sanyinjiao (SP6), Pishu (BL20), Shenshu (BL23), Weiwanxiashu (EX-CA) | Mild supplementing and reducing | 30 min |
| Han 2016 | Houxi (SI13), Zhaohai (KI6), Zhaohai (KI6), Neiguan (PC6), Waiguan (TE5), Gongsun (SP4), Lieque (LU7), Lieque (LU7) | Mild supplementing and reducing | 30 min |
| Ji 2010 | Zusanli (ST36), Sanyinjiao (SP6), Quchi (LI11), Yanglingquan (GB34), Hegu (LI4), Zhongwan (RN12), Xuehai (SP10), Diji (SP8), Yinlingquan (SP9), Fenglong (ST40), Taichong (LR3) | Mild supplementing and reducing | 30 min |
| Li 1998 | Zusanli (ST36), Sanyinjiao (SP6), Quchi (LI11), Yanglingquan (GB34), Fenglong (ST40), Taibai (SP3) ⟶ Zutonggu (BL66) | Mild supplementing and reducing | 20 min |
| Li 2005 | Zusanli (ST36), Sanyinjiao (SP6), Quchi (LI11), Yanglingquan (GB34), Pishu (BL20), Hegu (LI4), Dazhui (DU14), Weiwanxiashu (EX-CA), Shenshu (BL23), Neiguan (PC6), Xuanzhong (GB39) | Mild supplementing and reducing | 20-30 min |
| Li 2011 | Quchi (LI11), Pishu (BL20), Hegu (LI4), Houxi (SI13), Shenshu (BL23), Xiawan (RN10), Zhongwan (RN12), Qihai (RN6), Guanyuan (RN4), Ganshu (BL18) | Mild supplementing and reducing | 15 min |
| Lu 2016 | Zusanli (ST36), Pishu (BL20), Shenshu (BL23), Geshu (BL17), Weiwanxiashu (EX-CA), Ganshu (BL18), Taixi (KI3), Ashi point | Mild supplementing and reducing | 30 min |
| Pan 2014 | Zusanli (ST36), Sanyinjiao (SP6), Quchi (LI11), Yanglingquan (GB34), Pishu (BL20), Hegu (LI4), Houxi (SI13), Shenshu (BL23), Ganshu (BL18), Guanyuan (RN4), Qihai (RN6), Zhongwan (RN12), Xiawan (RN10), Yinlingquan (SP9), Diji (SP8), Jiexi (ST41), Yongquan (KI1) | Mild supplementing and reducing | 20 min |
| Ren 2007 | Zusanli (ST36), Sanyinjiao (SP6), Quchi (LI11), Yanglingquan (GB34), Fengchi (G20), Waiguan (TE5), Weizhong (BL40), Fenglong (ST40), Taichong (LR3), Xuehai (SP10) | Mild supplementing and reducing | 20 min |
| Song 2005 | Zusanli (ST36), Sanyinjiao (SP6), Pishu (BL20), Feishu (BL13) | Mild supplementing and reducing | 30 min |
| Wang 2007 | Zusanli (ST36), Quchi (LI11), Yanglingquan (GB34), Hegu (LI4), Neiguan (PC6), Yangchi (TE4), Taichong (LR3), Jiexi (ST41) | / | 40 min |
| Wang 2010 | Zusanli (ST36), Sanyinjiao (SP6), Quchi (LI11), Yanglingquan (GB34), Jiexi (ST41), Neiting (ST44), Taixi (KI3), Guanyuan (RN4), Geshu (BL17), Ashi point | Mild supplementing and reducing | 30 min |
| Wu 2017 | Sanyinjiao (SP6), Taixi (KI3), Weiwanxiashu (EX-CA), Feishu (BL13), Weishu (BL21), Shenshu (BL23) | Mild supplementing and reducing | / |
| Yan 2007 | Zusanli (ST36), Sanyinjiao (SP6), Quchi (LI11), Yanglingquan (GB34), Pishu (BL20), Taichong (LR3), Neiting (ST44), Jiexi (ST41), Xingjian (LR2), Yinlingquan (SP9), Erjian (LI2), Sanjian (LI3), Yangxi (LI5), Yemen (TE2), Zhongzhu (TE3), Qiangu (SI2), Houxi (SI13), Daling (PC7), Weiwanxiashu (EX-CA) | Mild supplementing and reducing | 20 min |
| Yao 2012 | Houxi (SI13), Neiguan (PC6), Gongsun (SP4), Waiguan (TE5), Lieque (LU7), Zhaohai (KI6), Lieque (LU7), Zhaohai (KI6) | Mild supplementing and reducing | 30 min |
| Zhao 2007 | Zusanli (ST36), Sanyinjiao (SP6), Quchi (LI11), Yanglingquan (GB34), Pishu (BL20), Hegu (LI4), Weiwanxiashu (EX-CA), Shenshu (BL23), Feishu (BL13), Taixi (KI3), Ganshu (BL18) | Mild supplementing and reducing | 30 min |
| Zhao 2016 | Houxi (SI13), Zhaohai (KI6), Zhaohai (KI6), Waiguan (TE5), Neiguan (PC6), Lieque (LU7), Gongsun (SP4), Lieque (LU7) | Mild supplementing and reducing | 30 min |
| Zuo 2010 | Zusanli (ST36), Sanyinjiao (SP6), Quchi (LI11), Hegu (LI4), Taixi (KI3), Waiguan (TE5), Guanyuan (CV4), Qihai (CV6) | Mild supplementing and reducing | 60 min |
3.2. Meta-Analysis Result
In the experimental group, “acupuncture alone” means “the intervention measure contains manual acupuncture, but without neurotrophic drugs” and “acupuncture+vitamin B” means “the intervention measure contains manual acupuncture and vitamin B, but no other neurotrophic drugs.”
In the control group, “vitamin B” means “the intervention measure contains vitamin B as the only neurotrophic drug.”
3.2.1. Description of Statistical Results
Out of the 18 trials retrieved from searching published RCTs and systematic reviews, 11 trials were acupuncture alone vs. vitamin B involving 699 participants (there are 356 participants in the acupuncture alone group and 343 participants in the vitamin B group) and 7 trials were acupuncture combined with vitamin B vs. vitamin B involving 501 participants (there are 266 participants in the acupuncture+vitamin B group and 235 participants in the vitamin B group).
3.2.2. Acupuncture Alone vs. Vitamin B (Figure 3)
Figure 3.
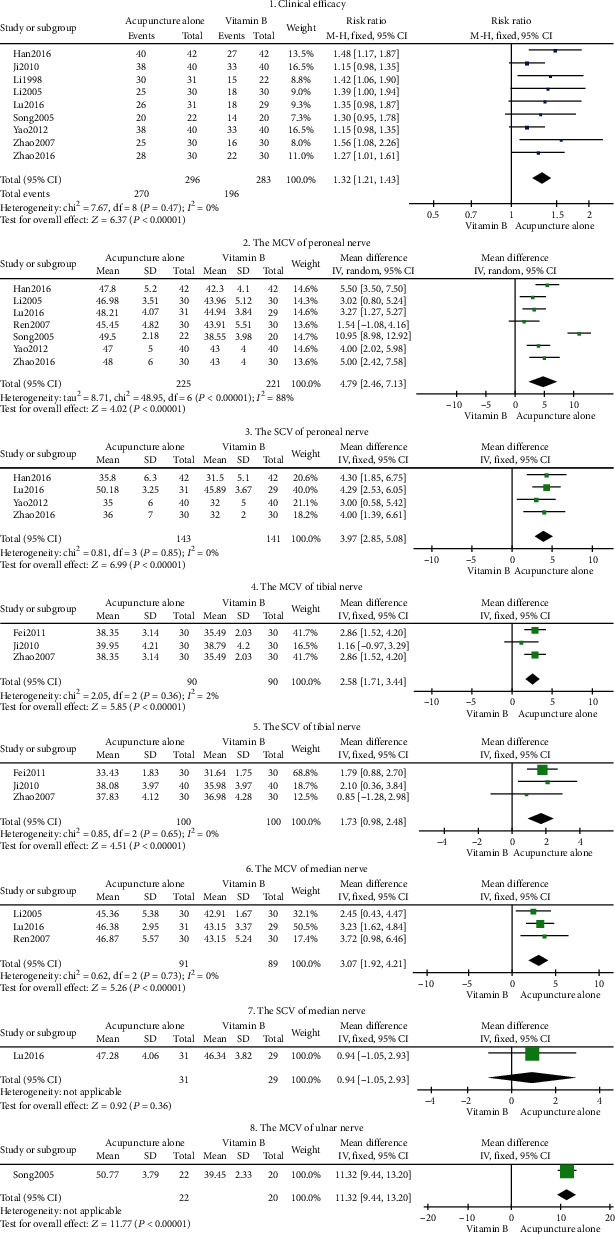
Forest plot of acupuncture alone.
Eight outcome indicators were used to compare acupuncture alone to vitamin B. The pooled results exhibited significant differences in clinical efficacy, peroneal nerve MCV, peroneal nerve SCV, tibial nerve MCV, tibial nerve SCV, median nerve MCV, and ulnar nerve MCV (P < 0.05), respectively. As shown in Figure 3, our findings suggest that acupuncture alone is more effective than using vitamin B in DPN (P < 0.05) therapy. There was no significant difference between the SCV of the median nerve of the acupuncture alone group and that of the vitamin B group (MD = 3.07, 95% CI: 1.92-4.21, P = 0.36 > 0.05; tag 7 in Figure 3). In this RCT, the efficacy of vitamin B (lipoic acid) in the treatment of DPN was compared with that of acupuncture alone. Given that only one study was included in this outcome indicator, sensitivity analysis could not be carried out for further verification.
3.2.3. Acupuncture+Vitamin B vs. Vitamin B (Figures 4 and 5)
Figure 4.
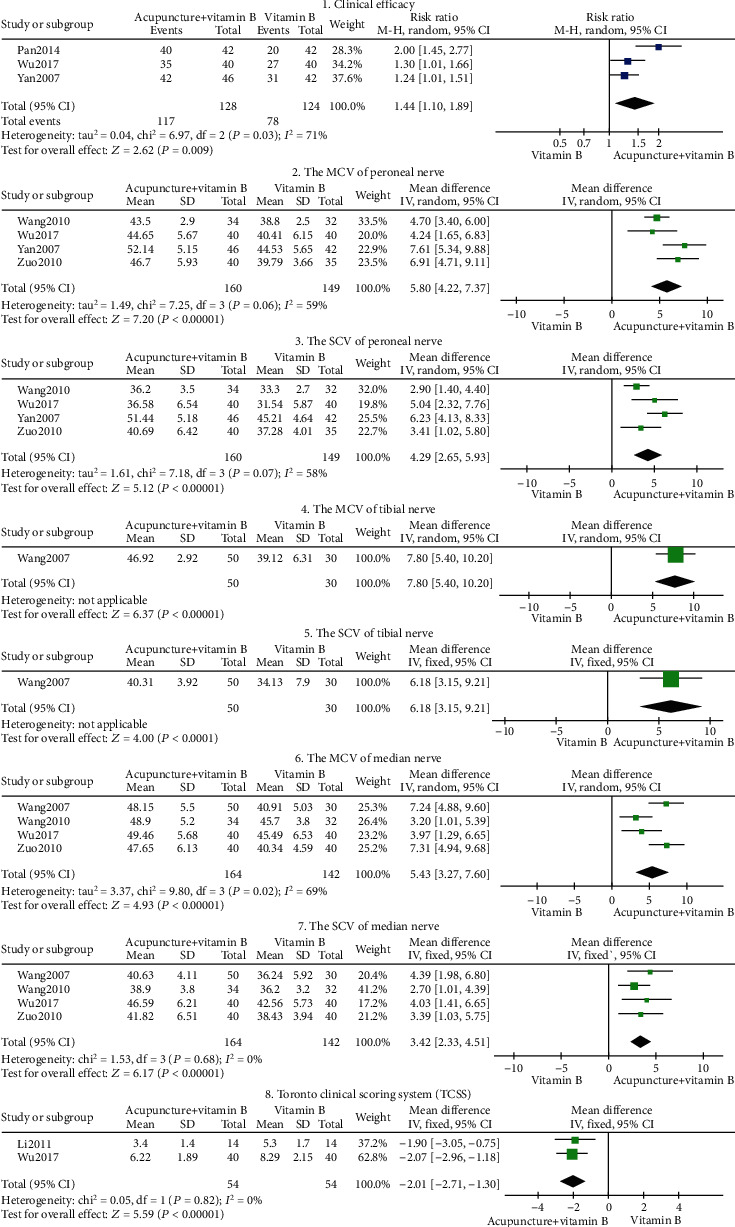
Forest plot of acupuncture+vitamin B.
Figure 5.
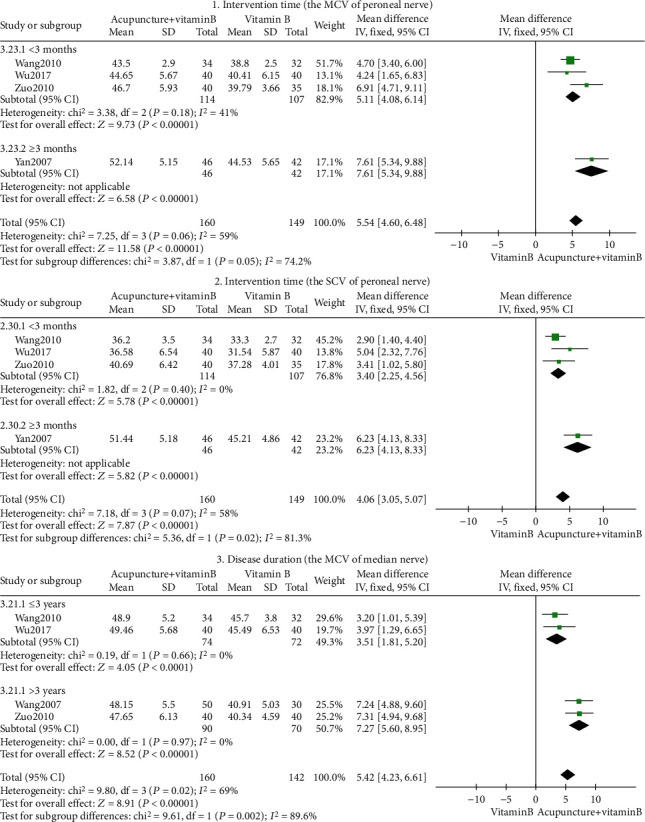
Acupuncture+vitamin B's subgroup analysis forest plot.
Eight outcome indicators were used to compare acupuncture+vitamin B with vitamin B. The pooled results displayed significant differences in clinical efficacy, peroneal nerve MCV, peroneal nerve SCV, tibial nerve MCV, tibial nerve SCV, median nerve MCV, median nerve SCV, and Toronto clinical scoring system (P < 0.05). As shown in Figure 4, our findings suggest that acupuncture combined with vitamin B is better than using vitamin B alone, in the treatment of DPN.
Peroneal nerve exposure's heterogeneity in MCV and SCV was high (I2 = 59%, I2 = 58%; Figure 4, tags 2 and 3), but all indexes were on the right of the invalid line. The MCV and SCV of the peroneal nerve had no significant clinical heterogeneity or methodological heterogeneity. We further conducted sensitivity analyses on MCV and SCV of the peroneal nerve, and the outcome was stable. Subgroup analysis was conducted based on intervention time (<3 months, ≥3months), indicating that heterogeneity was derived from intervention time (Figure 5, tags 1 and 2). Both short- and long-term acupuncture treatment therapy enhanced peroneal nerve MCV and peroneal nerve SCV (P < 0.05). While some heterogeneity was present (Figure 5, tag 1), it was still within acceptable limits. Given that treatment time is associated with restoration of nerve conduction velocity, there is still a need to determine the long-term effectiveness of acupuncture as DPN often recur after treatment [37, 38].
The heterogeneity in the MCV of the median nerve was high (I2 = 69%; tag 6 in Figure 4). Subgroup analysis conducted based on disease duration (≤3 years, >3 years) revealed heterogeneity in disease duration (Figure 5, tag 3). Acupuncture intervention can improve the MCV of the median nerve for both short-time and long-time disease duration (P < 0.05).
3.2.4. Subgroup Analysis (Figure 6)
Figure 6.
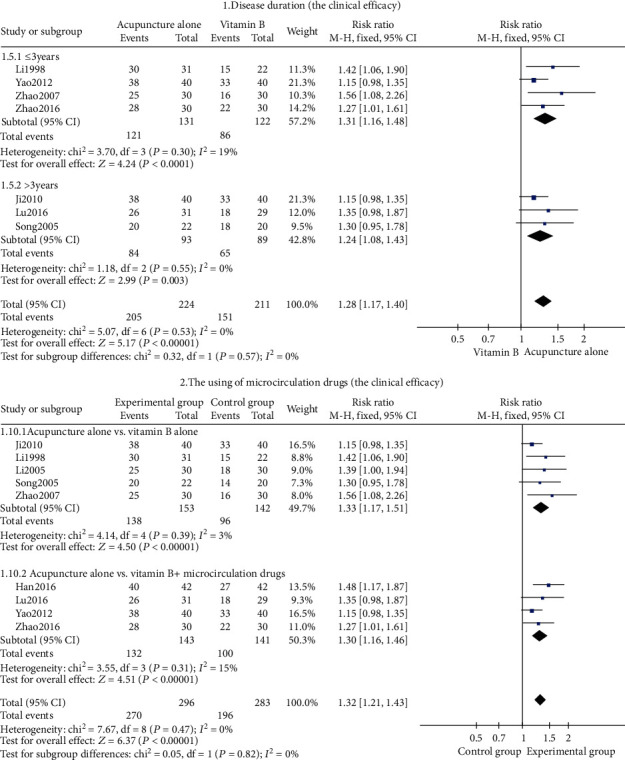
The clinical efficacy's subgroup analysis forest plot.
In the study of clinical efficacy, subgroup analysis was conducted based on the duration of the disease (≤3 years and >3 years) (Figure 6, tag 1). The result showed that acupuncture alone in the short- or long-term duration of the disease was better than using vitamin B (P < 0.05). We further conducted another subgroup analysis based on drugs used in the control group (with microcirculation drugs and no microcirculation drugs) (Figure 6, tag 2). The result showed that acupuncture alone was better than using vitamin B or vitamin B combined with microcirculation drugs (P < 0.05).
3.3. Trial Sequence Analysis (Figures 7 and 8)
Figure 7.
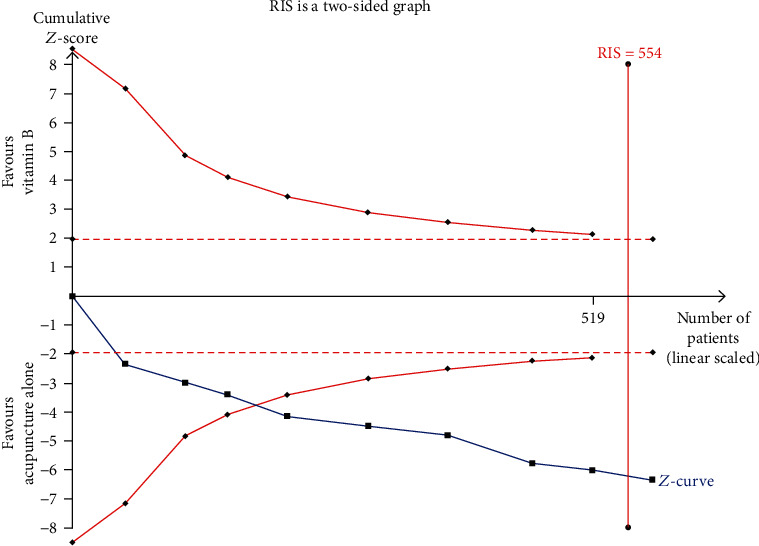
Trial sequence analysis of acupuncture alone (the clinical efficacy).
Figure 8.
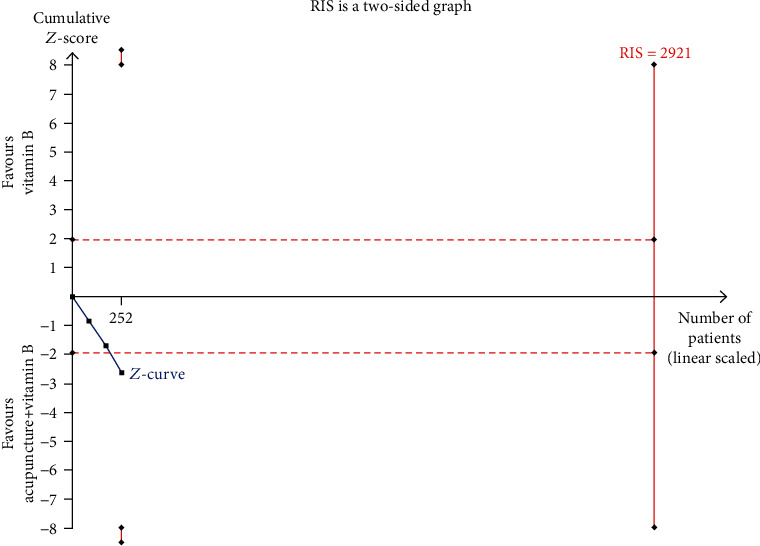
Trial sequence analysis of acupuncture+vitamin B (the clinical efficacy).
The TSA of acupuncture alone revealed that the cumulative Z-curve crossed the conventional boundary value (Z = 1.96, P = 0.05(two-sided)) and TSA boundary value and met the RIS (554 cases) (Figure 7). This result means that the cumulative sample size meets expectations; no more trials were needed.
The TSA of acupuncture combined with vitamin B revealed that the cumulative Z-curve crossed the conventional boundary value (Z = 1.96, P = 0.05 (two-sided)) but did not reach the TSA monitoring boundary and RIS (2921 cases) (Figure 8). This means that the cumulative sample size did not meet expectations; more trials were needed.
3.4. Safety Analysis
Two RCTs [27, 36] reported no adverse event, and no mention was made of the others.
3.5. Publication Bias
Egger's test was performed to evaluate the publication bias of the primary outcome. Nine studies were evaluated for the clinical efficacy of acupuncture alone (Egger's test: P = 0.005), and the results showed a statistically significant difference. Besides, the statistical significance of Egger's test indicates publication bias. Three studies were evaluated for the clinical efficacy of acupuncture combined with vitamin B (Egger's test: P = 0.207), and the results revealed no publication bias.
3.6. Sensitivity Analysis
Sensitivity analysis was performed to test the stability of the results, and the results showed that all indicators were stable.
4. Discussion
DPN pathogenesis involves interactions of multiple factors; hence, it is not yet clear. Since hyperglycemia is a well-known factor affecting many internal metabolic pathways, the key approach to DPN treatment is therefore strict control of hyperglycemia. Additionally, abnormal lipid metabolism, insulin resistance, and neurotrophasthenia may also participate in the metabolic pathway [39, 40]. Peripheral nerve edema, demyelination, and axonal degeneration are associated with the deposition of catabolic blood glucose products on peripheral nerves [41, 42].
Vitamin B restores neurotrophic factors and repairs nerves, which is used as supplementary treatment of axonal cell damage and nerve demyelination changes. Mecobalamin, a form of vitamin B12 with a high neuronal affinity, was shown to be able to repair the damaged myelin sheath and promote axon regeneration [43]. However, the efficacy of mecobalamin alone is often unsatisfactory in the treatment of DPN [44]. Combination of multiple vitamin B [27, 28] has a protective effect on micrangium of diabetic patients [45] and alleviates the symptoms. The animal experiment demonstrated that vitamin B1 can prevent abnormal lipid metabolism [46]. Lipoic acid, a form of vitamin B-like compound, was a natural antioxidant and could improve nerve conduction velocity [47]. Compared with mecobalamin, lipoic acid was more effective in treating DPN [48]. In addition, the combined use of neurotrophy medicine and drugs that improve microcirculation, such as alprostadil, has demonstrated synergistic action (Figure 6, tag 3) in the treatment of type 2 DM [49] and thus is recommended by the Chinese guideline [4]. Dilation of the vessels to enhance microcirculation is an important treatment mechanism [50].
Acupuncture exhibits a good therapeutic effect on DPN due to its direct local effect on microcirculation and its role in electrophysiological activity [51]. What is more, acupuncture can effectively reduce plasma neuropeptide Y (NPY) [52], which is one of the main risk factors for the development of type 2 diabetes via constriction of blood vessels and changes in the metabolic environment of the body [53], especially on lipid metabolism [54]. Reducing plasma neuropeptide Y (NPY) effectively delays the occurrence of diabetes and its complications [55]. Furthermore, acupuncture protects islet cells, increases insulin sensitivity, and promotes the secretion of insulin in diabetic patients to regulate the patient's blood glucose and lipid [56].
Our subgroup analysis indicates that acupuncture can achieve clinical efficacy in a short course of treatment which shows a good curative effect on patients with duration of DPN over 3 years. Of all included studies, Zusanli (ST36), Sanyinjiao (SP6), Quchi (LI11), and Yanglingquan (GB34), which are mainly distributed in the forearm and foreleg, are frequently selected for stimulation. In 18 RCTs, their acupoint frequencies were 13, 12, 11, and 9, respectively. An examination found that the distal part of extremities is the most common lesion site [57]. It is consistent with the hypothesis that an “acupoint can be used to treat unusual symptoms around this acupoint” [58].
It is related to their local anatomy structure, as these acupoints are close to the dorsal cutaneous nerve of the forearm, lateral sural cutaneous nerve, radial nerve, peroneal nerve, deep peroneal nerve, tibial nerve, etc. directly. Furthermore, an animal experiment showed that stimulating Zusanli (ST36) improves blood glucose regulation [59].
The onset and development of DPN can be explained as deficiency in the root and excess in the branch, according to the basic theory of traditional Chinese medicine (TCM), deficiency of “Qi” and “Xue” is the root, and blood stasis and phlegm are the branches [60, 61]. Sanyinjiao (SP6) is the location where the liver meridian, spleen meridian, and kidney meridian meet and can therefore nourish these three zang-fu organs (kidney, liver, and spleen). Needling Sanyinjiao (SP6) also harmonize “Qi” and “Xue” and balance Yin-Yang. Simply put, needling these acupoints can dredge the meridian and promote Qi and blood circulation. Ultimately, it relieves pain, numbness, and other symptoms, to achieve a good effect of DPN therapy. The results suggested that DPN should be treated using acupuncture. And the result of trial sequence analysis shows that the sample size of RCTs on acupuncture alone to treat DPN was enough but acupuncture combined with vitamin B to treat DPN was not.
5. Limitations
Only one of the 18 included trials was blind research, which might affect the evaluation of clinical efficacy according to the Cochrane Handbook. But it has no effect on the measurement of nerve conduction velocity
The number of the 18 included studies was small (a total of 1200 participants were involved), and 17 trials were in the Chinese language that may lead to publication bias. Based on the result of trial sequence analysis, the sample size of RCTs on acupuncture combined with vitamin B to treat DPN was not enough
Although the 18 RCTs showed that acupuncture alone and acupuncture combined with vitamin B are more effective than vitamin B in the treatment of DPN, there are some variations in acupuncture that may cause different curative effects
None of the studies reported long-term effects and safety following acupuncture treatments
There is no uniform international standard for the definition of clinical efficacy; the clinical efficacy evaluation was based on guiding principles for clinical research of new Chinese medicine [15]
6. Conclusions
The main role of acupuncture compared with vitamin B is to improve clinical efficacy. Besides, acupuncture significantly increases nerve conduction velocity and decreases the scores of the Toronto clinical scoring system (TCSS). However, further multicenter studies with large samples and high-quality RCTs on acupuncture combined with vitamin B are required, to more reliably assess the effect of acupuncture on DPN. Meanwhile, it is necessary to set standard criteria for evaluating clinical effectiveness.
Acknowledgments
The authors would like to thank freescience (http://www.home-for-researchers.com) for their help in improving the English language. This research was supported by the Apoplexy Acupuncture Inheritance Innovation Platform.
Data Availability
We searched against databases and reviewed all literature and then extracted data; additional information was obtained by contacting authors directly via call or email.
Conflicts of Interest
All authors declare that there is no conflict of interest regarding the publication of this paper.
Authors' Contributions
Hai lun Jiang and Peng Jia contributed equally to this work, and it is necessary to consider them as co-first authors.
Supplementary Materials
Table S1: search strategy. Table S2: PRISMA checklist. Table S3: PubMed search history. Figure S1: the sensitivity analysis of clinical efficacy of acupuncture alone. Figure S2: the sensitivity analysis of the MCV of the peroneal nerve of acupuncture alone. Figure S3: the sensitivity analysis of the SCV of the peroneal nerve of acupuncture alone. Figure S4: the sensitivity analysis of the MCV of the tibial nerve of acupuncture alone. Figure S5: the sensitivity analysis of the SCV of the tibial nerve of acupuncture alone. Figure S6: the sensitivity analysis of the MCV of the median nerve of acupuncture alone. Figure S7: the sensitivity analysis of clinical efficacy of acupuncture combined with vitamin B. Figure S8: the sensitivity analysis of the MCV of the peroneal nerve of acupuncture combined with vitamin B. Figure S9: the sensitivity analysis of the SCV of the peroneal nerve of acupuncture combined with vitamin B. Figure S10: the sensitivity analysis of the MCV of the median nerve of acupuncture combined with vitamin B. Figure S11: the sensitivity analysis of the SCV of the median nerve of acupuncture combined with vitamin B.
References
- 1.Pop-Busui R., Boulton A. J. M., Feldman E. L., et al. Diabetic neuropathy: a position statement by the American Diabetes Association. Diabetes Care. 40(1):136–154. doi: 10.2337/dc16-2042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Jaiswal M., Divers J., Dabelea D., et al. Prevalence of and risk factors for diabetic peripheral neuropathy in youth with type 1 and type 2 diabetes: SEARCH for Diabetes in Youth study. Diabetes Care. 40(9):1226–1232. doi: 10.2337/dc17-0179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Iqbal Z., Azmi S., Yadav R., et al. Diabetic peripheral neuropathy: epidemiology, diagnosis, and pharmacotherapy. Clinical Therapeutics. 40(6):828–849. doi: 10.1016/j.clinthera.2018.04.001. [DOI] [PubMed] [Google Scholar]
- 4.Chinese Diabetes Society. Guidelines for the prevention and treatment of type 2 diabetes in China (2017) Chinese Journal of Diabetes Mellitus. 2018;10(1):4–67. [Google Scholar]
- 5.Finnerup N. B., Attal N., Haroutounian S., et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. Lancet Neurology. 14(2):162–173. doi: 10.1016/S1474-4422(14)70251-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ismail-Beigi F., Craven T., Banerji M. A., et al. Effect of intensive treatment of hyperglycaemia on microvascular outcomes in type 2 diabetes: an analysis of the ACCORD randomised trial. Lancet. 376(9739):419–430. doi: 10.1016/S0140-6736(10)60576-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Witt C. M., Pach D., Brinkhaus B., et al. Safety of acupuncture: results of a prospective observational study with 229,230 patients and introduction of a medical information and consent form. Forsch Komplementmed. 16(2):91–97. doi: 10.1159/000209315. [DOI] [PubMed] [Google Scholar]
- 8.Zhao Y. L., Zhao G. J., Li X. G., Zhu X. X., Yang Y. X. Changes in nerve conduction velocity, F wave and sympathetic skin response in diabetic peripheral neuropathy and its clinical significance. Chinese Journal of Diabetes. 2013;21(12):1105–1107. [Google Scholar]
- 9.Liu P. Application of TCSS score in screening and treatment of peripheral neuropathy in type 2 diabetes mellitus. Hainan Medical Journal. 2012;23(17):21–23. [Google Scholar]
- 10.del Burgo Fernández J. L., Ruiz Serrano A. L., Moyano I. M., et al. Prevalence of diabetic polyneuropathy in a rural population. Application of the Toronto Clinical Scoring System (TCSS) Atencion Primaria. 2007;39(11):624–625. doi: 10.1157/13112204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Huan D., Li M. D., Lin L. Advances in the treatment of diabetic peripheral neuropathy by traditional Chinese medicine. Chinese Journal of Basic Medicine in Traditional Chinese Medicine. 2013;19(6):719–722. [Google Scholar]
- 12.Bai X., Song Z. L. Research progress in treatment of peripheral neuropathy with diabetes mellitus. Clinical Journal of Traditional Chinese Medicine. 2019;31(11):2031–2034. [Google Scholar]
- 13.Chen W., Yang G. Y., Liu B., Manheimer E., Liu J. P. Manual acupuncture for treatment of diabetic peripheral neuropathy: a systematic review of randomized controlled trials. PLoS One. 2013;8(9) doi: 10.1371/journal.pone.0073764. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Nash J., Armour M., Penkala S. Acupuncture for the treatment of lower limb diabetic peripheral neuropathy: a systematic review. Acupunct Med. 2019;37(1):3–15. doi: 10.1136/acupmed-2018-011666. [DOI] [PubMed] [Google Scholar]
- 15.Zhen X. Y. Guiding principles for clinical research of new Chinese medicine. Beijing, China: China Medical Science Press; 2002. pp. 72–73. [Google Scholar]
- 16.Zhao J. G., Zeng X. T., Wang J., Liu L. Association between calcium or vitamin D supplementation and fracture incidence in community-dwelling older adults: a systematic review and meta-analysis. Jama. 2017;318(24):2466–2482. doi: 10.1001/jama.2017.19344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Higgins J. P. T., Thomas J., Chandler J., Cumpston M., Welch V. A. Cochrane Handbook for Systematic Reviews of Interventions. Chichester, UK: John Wiley & Sons; 2019. [DOI] [Google Scholar]
- 18.Thorlund K., Engstrøm J., Wetterslev J., Brok J., Imberger G., Gluud C. User Manual for Trial Sequential Analysis (TSA) Copenhagen, Denmark: Copenhagen Trial Unit Centre for Clinical Intervention Research; 2017. [Google Scholar]
- 19.Fei A. H., Cai S. C., Chen Y., Zhu C. F., Qin X. F. Therapeutic effect of acupuncture on diabetic peripheral neuropathy and its influence on hs-CRP. Shanghai Journal of Acupuncture and Moxibustion. 2011;30(2):99–100. [Google Scholar]
- 20.Han L. Clinical observation on the treatment of 42 patients with diabetic peripheral neuropathy by acupuncture at confluent acupoints of eight extraordinary meridians. Forum on Traditional Chinese Medicine. 2016;32(1):46–48. [Google Scholar]
- 21.Ji X. Q., Wang C. M., Zhang P., Zhang X., Zhang Z. L. Effect of spleen-stomach regulation-needling on nerve conduction activity in patients with diabetic peripheral neuropathy. Acupuncture Research. 2010;35(6):443–447. [PubMed] [Google Scholar]
- 22.Li X. H., Shi H. Y., Yang X. N., Zhang Q. C., Li M., Gao W. Y. Clinical observation of acupuncture treatment of diabetic peripheral neuropathy. Journal of Clinical Acupuncture and Moxibustion. 1998;14(2):17–18. [Google Scholar]
- 23.Li J., Gao H. Clinical study on acupuncture treatment of diabetic peripheral neuropathy. Shandong Journal of Traditional Chinese Medicine. 2005;24(9):546–547. [Google Scholar]
- 24.Li W. K., Fan Z. W. Effect of acupuncture combined with mecobalamin in the treatment of 28 cases of diabetic peripheral neuropathy. The Journal of Medical Theory and Practice. 2011;24(23):2817–2818. [Google Scholar]
- 25.Lu M., Li K. S., Wang J. L. Acupuncture for distal symmetric multiple peripheral neuropathy of diabetes mellitus: a randomized controlled trial. Chinese Acupuncture & Moxibustion. 2016;36(5):481–484. [PubMed] [Google Scholar]
- 26.Pan W. T. Clinical observation of acupuncture combined with mecobalamin in the treatment of diabetic peripheral neuropathy. China Health Industry. 2014;11(2):190–192. [Google Scholar]
- 27.Ren M. Clinical observation on acupuncture treatment of diabetes with peripheral neuritis. Shenzhen Journal of Integrated Traditional Chinese and Western Medicine. 2007;17(4):239–241. [Google Scholar]
- 28.Song B. Y., Hao W. L. Acupuncture treatment of diabetic peripheral neuropathy in 22 cases. Journal of Sichuan of Traditional Chinese Medicine. 2005;23(7):104–105. [Google Scholar]
- 29.Wang J. Q., Zhou X. Y., Liang W. B., Cao Y. Z. Therapeutic effect of acupuncture on diabetic peripheral neuropathy. Journal of Emergency in Traditional Chinese Medicine. 2007;16(5):537–539. [Google Scholar]
- 30.Wang B. M., Ma J., Ma L. A clinical analysis of the curative effect of acupuncture on diabetes complicated by around neuropathological changes. Journal of Clinical Acupuncture and Moxibustion. 2010;26(8):17–18. [Google Scholar]
- 31.Wu F. H., Zhu Q. Y. Clinical research of acupuncture combined with medicine in the treatment of diabetic peripheral neuropathy. Journal of Clinical Acupuncture and Moxibustion. 2017;33(1):4–7. [Google Scholar]
- 32.Yan J. H. Treatment of 46 diabetic peripheral neuropathy with acupuncture plus methyconal. Shanghai Journal of Acupuncture and Moxibustion. 2007;26(9):14–15. [Google Scholar]
- 33.Yao X. W., Lin J. K., Li H., Wu W. J., Liu X. P. Clinical observation of eight confluent points acupuncture in the treatment of diabetic peripheral neuropathy. China Medical Herald. 2012;9(33):103–105. [Google Scholar]
- 34.Zhao J. L., Zhang S. Y. Observation of curative effect of eight confluence points acupuncture treatment in cure diabetic peripheral neuropathy. Shanxi Journal of Traditional Chinese Medicine. 2016;37(1):97–99. [Google Scholar]
- 35.Zhao H. L., Gao X., Gao Y. B., Yuan Q. Clinical observation on effect of acupuncture in treating diabetic peripheral neuropathy. Chinese Journal of Integrated Traditional and Western Medicine. 2007;27(4):312–314. [PubMed] [Google Scholar]
- 36.Zuo L., Zhang L. Study on the effect of acupuncture plus methylcobalamin in treating diabetic peripheral neuropathy. JOURNAL OF ACUPUNCTURE AND TUINA SCIENCE. 2010;8(4):249–252. doi: 10.1007/s11726-010-0420-1. [DOI] [Google Scholar]
- 37.Ye D. Z. Study on the influence of acupuncture and moxibustion on the nerve conduction function of patients with diabetic peripheral neuropathy. Chinese Journal of practical Neruous Diseases. 2013;16(24):41–42. [Google Scholar]
- 38.Guo Y. H., Guo Y. Advances in the research on acupuncture treatment of diabetic peripheral neuropathy. Acupuncture Research. 2003;28(2):157–161. [Google Scholar]
- 39.Mohapatra D., Damodar K. S. Glycaemia status, lipid profile and renal parameters in progressive diabetic neuropathy. Journal of Clinical and Diagnostic Research. 2016;10(9):cc14–cc17. doi: 10.7860/JCDR/2016/20004.8515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Mielke J. G., Wang Y. T. Insulin, synaptic function, and opportunities for neuroprotection. Progress in Molecular Biology and Translational Science. 2011;98:133–186. doi: 10.1016/B978-0-12-385506-0.00004-1. [DOI] [PubMed] [Google Scholar]
- 41.Lutty G. A. Effects of diabetes on the eye. Investigative Opthalmology & Visual Science. 2013;54(14):ORSF81–ORSF87. doi: 10.1167/iovs.13-12979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Costa P. Z., Soares R. Neovascularization in diabetes and its complications. Unraveling the angiogenic paradox. Life Sciences. 2013;92(22):1037–1045. doi: 10.1016/j.lfs.2013.04.001. [DOI] [PubMed] [Google Scholar]
- 43.Chen X. Q., Jin Y. Y., Tang G. New Edition of Pharmacology. Beijing, China: People’s Medical Publishing House(PMPH); 2011. p. p. 552. [Google Scholar]
- 44.Zhang Y. J., Ding J. Q., Li J. H. Application of mecobalamin in nervous system diseases. China Medicine and Pharmacy. 2012;2(14):19–21. [Google Scholar]
- 45.Wong C. Y., Qiuwaxi J., Chen H., et al. Daily intake of thiamine correlates with the circulating level of endothelial progenitor cells and the endothelial function in patients with type II diabetes. Molecular Nutrition & Food Research. 2008;52(12):1421–1427. doi: 10.1002/mnfr.200800056. [DOI] [PubMed] [Google Scholar]
- 46.Naveed A. K., Qamar T., Ahmad I., Raheem A., Malik M. M. Effect of thiamine on lipid profile in diabetic rats. Journal of theCollege of Physicians and Surgeons Pakistan. 2009;19(3):165–168. [PubMed] [Google Scholar]
- 47.Zhang X. L., Guo H. Alpha-lipoic acid for diabetic peripheral neuropathy. Medical Recapitulate. 2011;17(2):281–283. [Google Scholar]
- 48.Fen Y. Clinical observation of α-lipoic acid and mecobalamin in the treatment of type 2 diabetic peripheral neuropathy. Guide of China Medicine. 2020;18(7):38–39+41. [Google Scholar]
- 49.Sun X. J. Effect of alpha-lipoic acid, mecobalamin and alprostadil on diabetic peripheral neuropathy. Chinese and Foreign Medical Research. 2019;17(11):25–27. [Google Scholar]
- 50.Yang X. H. Integrated Chinese and western medicine diagnosis and treatment of DPN. in The 12th national academic conference on endocrine and metabolic diseases of integrated traditional Chinese and western medicine and summit forum on diabetes and thyroid diseases; 2019; Shenyang, Liaoning, China. p. p. 7. [Google Scholar]
- 51.Liu G. Z., Guo H. H., Wang R., Chen M. H., Wang Z. M. Clinical and mechanism research on acupuncture treatment of diabetic peripheral neuropathy. Chinese Acupuncture & Moxibustion. 1999;(5):261–264. [Google Scholar]
- 52.Sun N., Liu H. J., Ma S. X., Gao X. J. Effects of acupuncture prevention and treatment on plasma neuropeptide y in rats with diabetes. Acta Chinese Medicine. 2014;29(12):1731–1732. [Google Scholar]
- 53.Wang M. Y., Wang J. B., Tang Z. H., Liu J. R., Liu N. O., Zhen R. M. Metabolic regulatory function of Ag RP/NPY neurons. Progress in Physiological Sciences. 2019;50(1):67–75. [Google Scholar]
- 54.Balasubramaniam A., Joshi R., Su C., Friend L. A., James J. H. Neuropeptide Y (NPY) Y2 receptor-selective agonist inhibits food intake and promotes fat metabolism in mice: combined anorectic effects of Y2 and Y4 receptor-selective agonists. Peptides. 2007;28(2):235–240. doi: 10.1016/j.peptides.2006.08.041. [DOI] [PubMed] [Google Scholar]
- 55.Jaakkola U., Kallio J., Heine R. J., et al. Neuropeptide Y polymorphism significantly magnifies diabetes and cardiovascular disease risk in obesity: the Hoorn Study. European Journal of Clinical Nutrition. 2009;63(1):150–152. doi: 10.1038/sj.ejcn.1602964. [DOI] [PubMed] [Google Scholar]
- 56.Liu M. J., Liu Z. C., Xu B. Effect of acupuncture on fatty-insulin endocrine axis in 2 type diabetes mellitus with Qi and Yin deficiency pattern. Lishizhen Medicine and Materia Medica Research. 2014;25(7):1783–1785. [Google Scholar]
- 57.Dyck P. J., Kratz K. M., Karnes J. L., et al. The prevalence by staged severity of various types of diabetic neuropathy, retinopathy, and nephropathy in a population-based cohort: the Rochester Diabetic Neuropathy Study. Neurology. 1993;43(4):817–824. doi: 10.1212/WNL.43.4.817. [DOI] [PubMed] [Google Scholar]
- 58.Li Z. D. The rule of far treatment of acupoints is where is meridian across, where could correspond with indicate. Journal of Clinical Acupuncture and Moxibustion. 1995;11(9):1–3. [Google Scholar]
- 59.Lin Y. P., Wang Q. Q., Peng Y., He F. E., Shen J. Effect of electroacupuncture at Zusanli (ST 36),etc. on gastrointestinal motility and expression of ghrelin mRNA and growth hormone secretagogue receptor mRNA in diabetic gastroparesis rats. Acupuncture Research. 2015;40(4):290–295. [PubMed] [Google Scholar]
- 60.Sha W. J., Lei T. The distribution of TCM syndromes in peripheral neuropathy of type 2 diabetes mellitus. World's latest medical information digest. 2019;19(88):228–229. [Google Scholar]
- 61.Shi R., Wang G. Q. A study on TCM syndromes in DPN patients. Clinical Journal of Chinese Medicine. 2019;11(32):13–16. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1: search strategy. Table S2: PRISMA checklist. Table S3: PubMed search history. Figure S1: the sensitivity analysis of clinical efficacy of acupuncture alone. Figure S2: the sensitivity analysis of the MCV of the peroneal nerve of acupuncture alone. Figure S3: the sensitivity analysis of the SCV of the peroneal nerve of acupuncture alone. Figure S4: the sensitivity analysis of the MCV of the tibial nerve of acupuncture alone. Figure S5: the sensitivity analysis of the SCV of the tibial nerve of acupuncture alone. Figure S6: the sensitivity analysis of the MCV of the median nerve of acupuncture alone. Figure S7: the sensitivity analysis of clinical efficacy of acupuncture combined with vitamin B. Figure S8: the sensitivity analysis of the MCV of the peroneal nerve of acupuncture combined with vitamin B. Figure S9: the sensitivity analysis of the SCV of the peroneal nerve of acupuncture combined with vitamin B. Figure S10: the sensitivity analysis of the MCV of the median nerve of acupuncture combined with vitamin B. Figure S11: the sensitivity analysis of the SCV of the median nerve of acupuncture combined with vitamin B.
Data Availability Statement
We searched against databases and reviewed all literature and then extracted data; additional information was obtained by contacting authors directly via call or email.