

Abstract
目的
阐明乙型肝炎肝硬化(CHB-Cir)合并2型糖尿病(T2DM)时发生肝细胞癌(HCC)的风险及其协同因素。
方法
以2010年6月~2019年6月在南方医院肝病中心随访的CHB-Cir患者为研究对象,依性别、年龄、HBeAg状态、HBV DNA水平基本匹配后,构成CHB-Cir合并T2DM队列(观察组)和CHB-Cir无T2DM队列(对照组),半年随访1次。取已完成2年或以上随访且数据完整的病例纳入统计分析。采用Kaplan-Meier法比较两组HCC累积发生率;以Cox比例风险回归模型分析CHB-Cir合并T2DM时发生HCC的风险及其协同因素。
结果
纳入分析的467例研究对象平均随访时间为4.4±1.62年。观察组(n=203)和对照组(n=264)新发HCC病例分别为69例和48例,观察组HCC发病密度明显高于对照组(P < 0.001)。观察组HCC累积发生率明显高于对照组(P < 0.001),相对危险度为2.096(P < 0.01)。调整年龄(≥40岁)、肝癌家族史、既往抗病毒治疗、胆固醇升高、低密度脂蛋白胆固醇升高等因素后,T2DM仍是CHB-Cir患者发生HCC的独立危险因素(P=0.000)。
结论
T2DM是HCC的独立危险因素;CHB-Cir患者合并T2DM时HCC的发生风险增加2倍左右,提示及早控制糖尿病对降低CHB-Cir患者发生HCC的风险具有重要临床意义。
Keywords: 慢性乙型肝炎, 肝硬化, 肝细胞癌, 2型糖尿病, 队列研究
Abstract
Objective
To elucidate the risk and synergistic factors of hepatocellular carcinoma (HCC) in patients with chronic hepatitis B-associated cirrhosis (CHB-Cir) complicated by type 2 diabetes (T2DM).
Methods
The patients with CHB-Cir who were followed up in Hepatology Center of Nanfang Hospital from June 2010 to June 2019 were divided based on their T2DM status into two cohorts matched for gender, age, HBeAg status and HBV DNA load: CHB-Cir with T2DM group (observation group) and CHB-Cir without T2DM group (control group). All the patients were followed up at a 6-month interval, and the cases with complete clinical data and follow-up data for more than 2 years were included in the analysis. Kaplan- Meier method was used to compare the cumulative incidence of HCC between the two groups. A Cox proportional hazard regression model was used to analyze the relationship between T2DM and the risk of HCC in these patients.
Results
A total of 467 patients with a mean follow-up time of 4.4±1.62 years were included in the analysis, including 203 in the observation group and 264 in the control group. Sixty-nine and forty-eight new HCC cases occurred in the observation group and control group, respectively, showing a significantly higher incidence rate of HCC in the observation group (P < 0.001). The cumulative incidence of HCC in the observation group was significantly higher than that in the control group (P < 0.001), with a relative risk of 2.096 (P < 0.01). After adjustment for age (≥40 years), family history of liver cancer, previous antiviral therapy, elevated cholesterol and elevated LDL cholesterol, T2DM remained an independent risk factor for HCC in CHB-Cir patients (P=0.000).
Conclusion
T2DM is an independent risk factor for HCC, and the risk of HCC increases by more than two folds in CHB-Cir patients complicated by T2DM, suggesting the clinical significance of early interventions of diabetes to reduce the risk of HCC in CHB-Cir patients.
Keywords: chronic hepatitis B, cirrhosis, hepatocellular carcinoma, type 2 diabetes mellitus, cohort study
一直以来,HBV感染被公认为我国肝细胞癌(HCC)发生最重要的病因,肝硬化是HCC发生主要的病理背景[1-2]。然而近20年来,在我国HBV现症感染率从9.09%持续下降到6.0%以下的背景下[3],HCC的发病率和病死率却持续增加,发病率和病死率占全球50%以上,持续威胁着我国人民的健康和生命安全[4-5]。HBV现症感染率下降和HCC发病率升高形成了剪刀差。文献报道,HCC主要发生在40岁以上的人群,HBV现症感染率降低主要见于20岁以下,特别是10岁以下人群,归因于近20年来乙肝疫苗的普遍接种[1]。30岁以上HBV感染人群HCC发病率升高的推动因素是什么?近20年来,具有促进肿瘤发生的2型糖尿病(T2DM)发病率持续大幅升高[6-7]引起了我们的重视。T2DM是否HCC发病率升高的重要病因?针对这些临床亟待解答的科学问题,我们采用最可能阐明病因联系的队列研究方法,以HCC发病率较高的慢性乙型肝炎肝硬化(CHB-Cir)人群为研究对象,构成伴有T2DM的CHBCir观察组,按配对对照原则组成不伴有T2DM的CHBCir对照组,进行了平均5年的大样本队列随访研究。试图阐明T2DM是我国CHB-Cir患者HCC高发的重要危险因素,取得了较好的研究结果和客观的临床调查数据。
1. 资料和方法
1.1. 研究对象及分组
以2010年6月~2019年6月在南方医科大学南方医院肝病中心接受抗病毒治疗随访的CHB患者为基础对象,确诊为CHB-Cir的患者为队列筛选对象。纳入标准:年龄≥30岁;符合下述肝硬化诊断标准的CHB-Cir患者;同意基线调查并接受规律的复查和随访。排除标准:合并丙型肝炎病毒和艾滋病病毒感染者;其他原因引起的肝纤维化、肝硬化患者;合并酒精性肝病、自身免疫性肝病者;已有证据提示或证实为肝脏恶性肿瘤者;明确诊断1型糖尿病者。根据CHB-Cir患者是否合并T2DM,分为观察组筛选群和对照组筛选群;再按照病例对照研究的设计,从2个群中依性别、年龄(相差≤5岁)、HBeAg状态、HBV DNA定量基本匹配后,按1∶1的比例入组,构成队列研究的CHB-Cir合并糖尿病组(简称观察组,下同)和无糖尿病的CHB-Cir组(对照组)。并进行每半年一次的复查和随访。2020年12月底止,已经完成2年或以上随访且数据完整的病例纳入统计分析。
本研究为前瞻性、对照、开放的队列研究,已通过南方医科大学南方医院伦理委员会批准,所有纳入研究对象均为自愿参与并签署书面知情同意书。研究队列入组流程见图 1。
1.
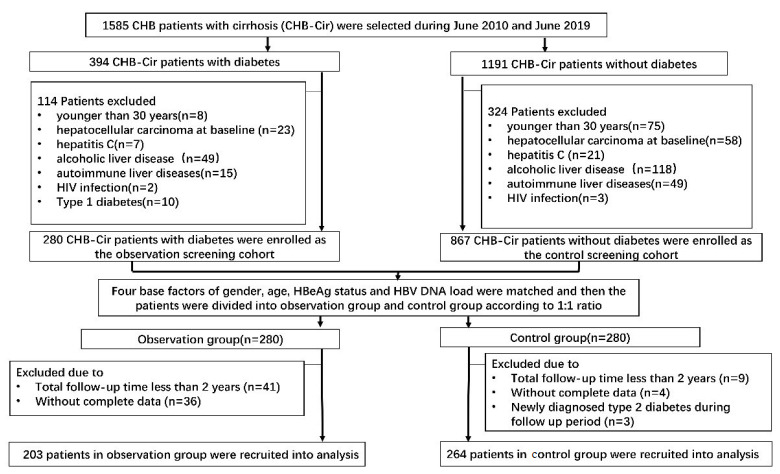
队列研究观察组和对照组入组流程图
Flowchart of patient enrollment. CHB: Chronic hepatitis B; CHB-Cir: Chronic hepatitis B with cirrhosis.
1.2. 诊断标准
慢性乙型肝炎的诊断符合2010年中华医学会肝病学分会与感染病学分会联合制订的《慢性乙型肝炎防治指南》[8]诊断标准;肝硬化的诊断符合2014年版《乙型肝炎病毒相关肝硬化的临床诊断、评估和抗病毒治疗的综合管理》[9]诊断标准;HCC的诊断符合《原发性肝癌诊疗规范(2011年版)》[10]诊断标准;2型糖尿病的诊断符合《中国2型糖尿病防治指南(2010年版)》[11]诊断标准。
1.3. 基线调查与随访
基线调查以检查结果和病历记录为依据,内容包括人口统计学数据、生活方式、既往史、肿瘤家族史等信息以及相关实验室检查结果。研究中所有对象均接受口服一线抗病毒药物—核苷类似物(NAs)治疗,每半年定期复查1次。有可疑HCC发生情况(例如AFP升高、B超发现肝内结节增大,可见低回声结节)的病例,改为每2个月随访1次,以及时确诊HCC发病。对于随访过程中的新发HCC病例,收集、核实其诊断依据,包括B超、增强CT、普美显Ⓡ增强磁共振等影像学检查结果,AFP以及病理诊断等,以确认HCC的诊断。
1.4. 统计学分析方法
应用SPSS25.0进行数据分析。以KolmogorovSmirnov法检验数据正态分布与否,根据是否服从正态分布,分别采用均数±标准差或中位值(IQR)描述变量;对于正态分布计量资料,两组间比较采用两独立样本t检验;非正态分布计量资料两组间比较采用Wilcoxon秩和检验;计数资料以例数和百分数表示,组间比较采用χ2检验。采用Kaplan-Meier法计算HCC累积发生率;以Cox比例风险回归模型分析T2DM与CHB-Cir相关HCC发生风险的关系。所有统计分析基于双侧假设检验,以α=0.05为检验水准,P < 0.05为差异具有统计学意义。
2. 结果
2.1. 患者基线特征
CHB-Cir队列共随访560例患者,剔除其中缺乏重要随访节点数据的病例、脱落病例以及随访时间不到2年的病例,最终进入统计分析的病例共467例,其中男403例,女64例,CHB-Cir合并糖尿病203例(观察组),无糖尿病的CHB-Cir264例(对照组)。467例研究对象共随访2262.42人年,随访时间4.4±1.62年。观察组和对照组在性别、年龄、随访时间、肝癌家族史、抗病毒治疗、肝硬化代偿情况、HBeAg(+)、HBV DNA定量方面具有良好的可比性(P>0.05,差异均无统计学意义,表 1)。
1.
观察组和对照组的基线指标比较分析
Comparison of baseline clinical characteristics between CHB-Cir patients with and without diabetes
| Characteristics | Observation group (n=203) | Control group (n=264) | χ2/F | P |
| *Antiviral treatment: NAs antiviral therapy for more than one year prior to admission. #Diabetes treatment: Drugs for the treatment of diabetes determined by specialists in the Department of Endocrinology. HBeAg + : Positive for HBeAg. For descriptive purposes, quantitative variables are presented as Mean ± SD. Categorical variables are presented as number and percentages. Comparisons across two groups were performed using chi-square test or Fisher's exact test for categorical variables. | ||||
| Age (years) | 48.49±9.692 | 47.81±9.137 | -1.272 | 0.203 |
| Follow-up time (years) | 4.70±1.55 | 4.96±1.67 | -1.390 | 0.164 |
| Male (%) | 171(84.2) | 232(87.9) | 1.287 | 0.257 |
| Family history of liver cancer (%) | 29(14.3) | 25(9.5) | 2.603 | 0.107 |
| Antiviral treatment* (%) | 183(90.1) | 246(93.2) | 1.413 | 0.235 |
| Diabetes treatment# (%) | 159(78.3) | 0(0) | 313.524* | 0.000 |
| Decompensated cirrhosis (%) | 97(47.8) | 110(41.7) | 1.74 | 0.187 |
| hyperlipidaemia | 71(34.9) | 83(31.4) | 0.159 | 0.69 |
| HBeAg+ (%) | 68(33.5) | 98(37.1) | 0.658 | 0.417 |
| HBV DNA(lg IU/mL) | 3.95±2.01 | 3.92±2.24 | 0.178 | 0.859 |
2.2. 两组HCC发病密度、HCC累积发生率的比较
观察组203例研究对象共随访962.42人年,人均随访时间4.70±1.55年,随访期间新发HCC 69例,HCC发病率34.0%,发病密度71.69/千人年。对照组264例研究对象共随访1300人年,人均随访时间4.96±1.67年,新发HCC48例,HCC发病率18.2%,发病密度36.92/千人年。观察组HCC发病率明显高于对照组,差异有统计学显著性意义(χ2=15.273,P < 0.001)。用KaplanMeier法比较两组HCC累积发生率的相对危险度,观察组HCC累计发生率高于对照组(Log-rank检验,P < 0.001),相对危险度(RR)为2.096[95%置信区间(CI):1.450~3.032,P < 0.01,图 2]。本研究揭示:乙型肝炎肝硬化合并糖尿病时发生HCC的风险是无糖尿病时的2.096倍,差异具有统计学意义(P < 0.001)。
2.
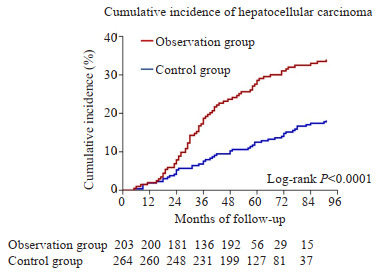
观察组和对照组HCC累积发生率的比较
Comparison of rates of cumulative incidence of HCC in the two groups.
2.3. 糖尿病与CHB-Cir患者HCC发生风险的关系
2.3.1. HCC相关因素的单因素Cox比例风险分析
选取既往文献报道可影响HCC发生的因素,如性别、年龄≥40岁、合并糖尿病、肝癌家族史、抗病毒治疗、肝硬化失代偿、HBeAg状态、病毒载量、血脂,进行单因素Cox比例风险分析,结果显示:糖尿病、年龄≥40岁、肝癌家族史、低密度脂蛋白(LDL)升高、胆固醇升高(CHOL)是HCC的相关危险因素;其风险率(HR)分别为2.656(95% CI: 1.831~3.853)、2.334(95% CI: 1.831~3.853)、2.438(95% CI: 1.831~3.853)、1.944(95% CI: 1.831~ 3.853)、1.980(95% CI: 1.831~3.853),差异均具有统计学意义(P均 < 0.05)。抗病毒治疗是HCC发生的保护因素,HR为0.087(95% CI: 1.831~3.853,P=0.0000,表 2)。
2.
HCC相关因素的单因素Cox比例风险分析
Univariate Cox proportional hazards analysis of risk factors of HCC
| Variable | Hazard ratios (HR) | 95% confidence interval (95%CI) | P |
| *NAs antiviral therapy for more than one year prior to admission. #TG↑: TG>1.70 mmol/L; LDL-C↑: LDL-C>3.36 mmol/L; CHOL↑: CHOL>5.17 mmom/L. | |||
| With diabetes | 2.656 | 1.831-3.853 | 0.000 |
| Male | 1.047 | 0.598-1.832 | 0.873 |
| Older than 40 years | 2.334 | 1.439-3.785 | 0.001 |
| Family history of liver cancer | 2.438 | 1.539-3.860 | 0.000 |
| Antivirial treatment* | 0.087 | 0.056-0.134 | 0.000 |
| Decompensated cirrhosis | 1.375 | 0.956-1.976 | 0.086 |
| HBeAg(+) | 0.873 | 0.587-1.299 | 0.505 |
| HBV DNA≥3lgIU/mL | 1.075 | 0.740-1.562 | 0.704 |
| TG↑# | 1.373 | 0.809-2.328 | 0.240 |
| LDL-C↑ | 1.944 | 1.277-2.960 | 0.002 |
| CHOL↑ | 1.98 | 1.340-2.924 | 0.001 |
2.3.2. HCC相关因素的多因素Cox比例风险分析
根据单因素Cox比例风险分析结果,对有统计学意义的HCC相关因素进一步行多因素Cox比例风险分析,发现:合并糖尿病、年龄≥40岁、有肝癌家族史是HCC发生的独立危险因素,调整风险率(aHR)分别为2.092(95% CI: 1.420~3.096)、2.095(95% CI: 1.268~3.463)、1.892(95%CI: 1.192~3.001)。调整年龄(≥40岁)、肝癌家族史、抗病毒治疗、胆固醇升高、低密度脂蛋白胆固醇升高后,CHB-Cir合并糖尿病时发生HCC的风险是单纯CHB-Cir患者的2.092倍(95% CI:1.420-3.096,P= 0.000,表 3)。
3.
HCC相关因素的多因素Cox比例风险分析
Multivariate Cox proportional hazards analysis of risk factor for HCC
| Variable | Ajusted hazard ratios (aHR) | 95% CI | P |
| *NAs antiviral therapy for more than one year prior to admission. #LDL-C↑: >3.36 mmol/L; CHOL↑: CHOL>5.17 mmom/L. | |||
| With diabetes | 2.092 | 1.420-3.096 | 0.000 |
| Older than 40 years | 2.095 | 1.268-3.463 | 0.004 |
| Family history of liver cancer | 1.892 | 1.192-3.001 | 0.007 |
| Antivirial treatment* | 0.093 | 0.060-0.145 | 0.000 |
| LDL-C↑# | 1.650 | 0.969-2.810 | 0.065 |
| CHOL↑# | 1.442 | 0.875-2.375 | 0.151 |
3. 讨论
慢性乙型肝炎(CHB)肝硬化(Cir)是我国HCC发生发展的主要病因和重要病理背景。近20年来,我国CHB防治取得了举世瞩目的成就:HBV现症感染率由9.09%下降到6%以下,但HCC的发病率和病死率却持续升高,形成了剪刀差。这个剪刀差的驱动因素是什么?广泛调研后,具有促进肿瘤发生、呈逐年快速上升趋势的T2DM引起了我们的深切关注。为揭示T2DM在CHB-Cir相关HCC高发中的驱动作用,我们采用前瞻性队列研究设计,聚焦于CHB-Cir人群,按1∶1的病例对照比例构成观察组(CHB-Cir合并T2DM组)和对照组(单纯CHB-Cir组)。对纳入的467例患者共随访2262.42人年,人均随访时间4.4±1.62年,新发HCC共117例,HCC发病率为25.1%,HCC发病密度为51.71/千人年。其中,CHB-Cir合并糖尿病(观察组203例)时HCC发病率34.0%,发病密度71.69/千人年,风险比RR是对照组的2.096倍。提示CHB-Cir合并T2DM时HCC发病密度明显增高。在调整了年龄、肝癌家族史、病毒水平、血脂等混杂因素后,调整风险值未明显改变。揭示T2DM是CHB-Cir相关HCC发生的重要危险因素。
近年来,CHB相关HCC与T2DM之间的联系引起了研究者的较多重视。一项来自中国台湾的病例对照研究[12]纳入了4179例伴或不伴糖尿病的CHB患者,结果发现并发糖尿病的CHB患者的HCC累积发生率显着高于无糖尿病的CHB患者(RR=1.628,P=0.012)。在调整了年龄、性别、高脂血症、抗病毒治疗、他汀类药物治疗和肝硬化之后,糖尿病仍然是HCC的独立预测因素(HR=1.798,P=0.005)。Kim[13]、Li[14]和Shyu等[15]也报道了类似的结果。一项来自新西兰的回顾性研究则纳入了223例CHB-Cir患者,结果表明合并T2DM的CHB-Cir患者的HCC发病密度为60.5/千人年,而非T2DM的CHB-Cir患者仅为25.4/千人年(P=0.006)[16]。以上研究均提示T2DM是HCC发生的危险因素。但这些研究多为回顾性研究,纳入的分析对象多为CHB患者,而关注CHB-Cir人群的研究则存在病例数较少、随访时间较短等情况。尚未见到来自中国大陆CHB-Cir合并糖尿病时发生HCC风险分析的3年以上队列研究报道。由于HCC的发生是多因素、多步骤、多基因参与的复杂的致癌过程,我们在队列研究设计时综合考虑既往文献报道的风险因素,采用倾向得分匹配法(PSM)按比例配对,以平衡已经报道的混杂因素,如性别、年龄、HBeAg状态和HBV DNA载量水平,突出血糖升高对HCC发生的影响,取得了良好的结果:队列研究中,HCC相关因素的单因素Cox比例风险分析和多因素Cox比例风险分析糖尿病均为HCC发生的独立危险因素;与对照组相比较,观察组中,糖尿病的调整风险率(aHR)为2.092(95% CI: 1.420~3.096),得出了明确的T2DM是CHB-Cir相关HCC高发的重要危险因素的结论。
CHB-Cir合并T2DM时HCC发生风险显著升高的机制是什么?在“乙肝-肝硬化-肝癌”三步曲的进展模式中,由于肝脏持续受到CHB炎症活动的影响,肝内T细胞表型和功能逐渐缺失,导致功能上的不足和细胞活性的降低,即T细胞耗竭,进而造成肝脏局部“免疫抑制微环境”[17-20]。近来研究认为,糖尿病所致的高血糖、胰岛素抵抗和慢性炎症等均会增加恶性肿瘤的发病风险[21-22]。糖尿病患者由于血糖、血脂代谢紊乱产生过量自由基、TNF-α、IL-6、C-反应蛋白和其他炎性因子,从而促进炎症反应的发生,也使肝内局部“炎症微环境”恶化[23-24];此外,糖尿病时微血管病变、组织微循环障碍、能量供应缺乏,易引发机体局部或全身性感染[25-27],使糖尿病患者呈现慢性炎症状态。越来越多的证据表明,持续性的慢性炎症增加基因的不稳定性和肿瘤的发病风险[28-29]。CHB-Cir患者合并糖尿病时叠加了肝内的炎症,促进了假小叶内肝细胞的异型性变,同时T细胞功能耗竭加快,进一步降低了机体的免疫监视功能和调节功能,进而增加了HCC的发生风险。
既往研究提示,肝硬化、年龄大于50岁、高脂血症、糖尿病是HBV相关HCC的风险因素,各因素与HCC发生的关系因研究差异而呈现不同特点[30-32]。本研究Cox比例风险分析提示T2DM、年龄≥40岁、肝癌家族史、LDL-C≥3.36 mmol/L、CHOL≥5.17 mmol/L是HCC的相关危险因素,HR分别为2.656、2.334、2.438、1.944和1.980,差异均具有统计学意义;早期(入组前1年以上)抗病毒治疗是HCC发生的保护因素,HR为0.087(P=0.000)。因此,在CHB防治过程中,阻止或延缓CHB朝肝硬化进展,以及T2DM的早发现、早诊断、早治疗,对改善CHB患者远期预后至关重要。
本研究有以下亮点:立足于我国慢性HBV感染者病程长、已进展为CHB-Cir患者较多的现状,把研究对象聚焦于HCC高发的CHB-Cir高危人群;研究样本量足够大,并对CHB-Cir患者进行了5年的队列随访,调整混杂因素之后重点分析T2DM是否协同CHB-Cir促进HCC的发生,为HCC的早期干预研究提供了重要的循证医学依据和深入研究的线索。本研究的不足之处:包括未评估超重与肥胖、T2DM病程、不同的降糖药物治疗(既往由内分泌科专家制定)对HCC发生的影响。尚需纳入相关因素深入开展多中心、大样本量的队列研究,以阐明体质量、T2DM病程、不同降糖治疗药物对CHB-Cir人群HCC发生风险的影响。
综上所述,本研究通过建立前瞻性、配对对照的研究队列,聚焦于CHB-Cir人群,经过长达5年的队列随访的结果揭示:CHB-Cir合并糖尿病时HCC发生风险明显增加;糖尿病是CHB-Cir相关HCC的独立危险因素;年龄大于40岁、有肝癌家族史、LDL升高、CHOL升高也是HCC的相关风险因素。在临床实践中对于年龄大于40岁的CHB-Cir患者,需要高度重视血糖、血脂等早期HCC风险因素的检测。下一步对这些风险因素深入开展多中心的干预和控制研究,可望为明显降低CHB-Cir相关HCC的发生率提供循证医学依据和临床数据支持。
Biographies
唐淬蓉,硕士研究生,E-mail: 18802084147@163.com
胡承光,博士研究生,E-mail: chegguanghu@163.com
周宇辰,主治医师,E-mail: yuchenzhou@163.com
Funding Statement
国家自然科学基金(81772923,81774212)
Supported by National Natural Science Foundaton of China (81772923,81774212).
Contributor Information
唐 淬蓉 (Cuirong TANG), Email: 18802084147@163.com.
胡 承光 (Chengguang HU), Email: chegguanghu@163.com.
周 宇辰 (Yuchen ZHOU), Email: yuchenzhou@163.com.
林 志昭 (Zhizhao LIN), Email: 13662419976@163.com.
周 元平 (Yuanping ZHOU), Email: yuanpingzhou@163.com.
References
- 1.Wang MJ, Wang YT, Feng XS, et al. Contribution of hepatitis B virus and hepatitis C virus to liver cancer in China north areas: Experience of the Chinese national cancer center. Int J Infect Dis. 2017;65:15–21. doi: 10.1016/j.ijid.2017.09.003. [Wang MJ, Wang YT, Feng XS, et al. Contribution of hepatitis B virus and hepatitis C virus to liver cancer in China north areas: Experience of the Chinese national cancer center[J]. Int J Infect Dis, 2017, 65: 15-21.] [DOI] [PubMed] [Google Scholar]
- 2.Tang A, Hallouch O, Chernyak V, et al. Epidemiology of hepatocellular carcinoma: target population for surveillance and diagnosis. Abdom Radiol (NY) 2018;43(1):13–25. doi: 10.1007/s00261-017-1209-1. [Tang A, Hallouch O, Chernyak V, et al. Epidemiology of hepatocellular carcinoma: target population for surveillance and diagnosis[J]. Abdom Radiol (NY), 2018, 43(1): 13-25.] [DOI] [PubMed] [Google Scholar]
- 3.Zhou M, Wang H, Zeng X, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2019;394(10204):1145–58. doi: 10.1016/S0140-6736(19)30427-1. [Zhou M, Wang H, Zeng X, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017[J]. Lancet, 2019, 394(10204): 1145-58.] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.de Martel C, Georges D, Bray F, et al. Global burden of cancer attributable to infections in 2018: a worldwide incidence analysis. Lancet Glob Health. 2020;8(2):e180–90. doi: 10.1016/S2214-109X(19)30488-7. [de Martel C, Georges D, Bray F, et al. Global burden of cancer attributable to infections in 2018: a worldwide incidence analysis[J]. Lancet Glob Health, 2020, 8(2): e180-90.] [DOI] [PubMed] [Google Scholar]
- 5.Sagnelli E, Macera M, Russo A, et al. Epidemiological and etiological variations in hepatocellular carcinoma. Infection. 2020;48(1):7–17. doi: 10.1007/s15010-019-01345-y. [Sagnelli E, Macera M, Russo A, et al. Epidemiological and etiological variations in hepatocellular carcinoma[J]. Infection, 2020, 48(1): 7-17.] [DOI] [PubMed] [Google Scholar]
- 6.Qi JY, He P, Yao HY, et al. Cancer risk among patients with type 2 diabetes: a real-world study in Shanghai, China. J Diabetes. 2019;11(11):878–83. doi: 10.1111/1753-0407.12926. [Qi JY, He P, Yao HY, et al. Cancer risk among patients with type 2 diabetes: a real-world study in Shanghai, China[J]. J Diabetes, 2019, 11(11): 878-83.] [DOI] [PubMed] [Google Scholar]
- 7.Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract. 2019;157:107843. doi: 10.1016/j.diabres.2019.107843. [Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition[J]. Diabetes Res Clin Pract, 2019, 157: 107843.] [DOI] [PubMed] [Google Scholar]
- 8.中华医学会肝病学分会, 中华医学会感染病学分会 慢性乙型肝炎防治指南(2015年更新版) https://www.cnki.com.cn/Article/CJFDTOTAL-LCGD201512003.htm. 中国病毒病杂志. 2015;5(6):401–24. [中华医学会肝病学分会, 中华医学会感染病学分会. 慢性乙型肝炎防治指南(2015年更新版) [J]. 中国病毒病杂志, 2015, 5(6): 401-24.] [Google Scholar]
- 9.科技部十二五重大专项联合课题组专家 乙型肝炎病毒相关肝硬化的临床诊断、评估和抗病毒治疗的综合管理. 临床肝胆病杂志. 2014;30(2) doi: 10.3969/j.issn.1001-5256.2014.02.002. [科技部十二五重大专项联合课题组专家. 乙型肝炎病毒相关肝硬化的临床诊断、评估和抗病毒治疗的综合管理[J]. 临床肝胆病杂志, 2014, 30(2). DOI:10.3969/j.issn.1001-5256.2014.02.002.] [DOI] [Google Scholar]
- 10.中华人民共和国卫生部 原发性肝癌诊疗规范(2011年版) 临床肝胆病杂志. 2011;27(11):1141–59. doi: 10.3969/j.issn.1001-5256.2011.11.004. [中华人民共和国卫生部. 原发性肝癌诊疗规范(2011年版)[J]. 临床肝胆病杂志, 2011, 27(11): 1141-59.] [DOI] [Google Scholar]
- 11.中华医学会糖尿病学分会 中国2型糖尿病防治指南(2010年版) https://www.cnki.com.cn/Article/CJFDTOTAL-ZGTL201201036.htm. 中国医学前沿杂志: 电子版. 2011;3(6) [中华医学会糖尿病学分会. 中国2型糖尿病防治指南(2010年版)[J]. 中国医学前沿杂志: 电子版, 2011, 3(6).] [Google Scholar]
- 12.Fu SC, Huang YW, Wang TC, et al. Increased risk of hepatocellular carcinoma in chronic hepatitis B patients with new onset diabetes: a nationwide cohort study. Aliment Pharmacol Ther. 2015;41(11):1200–9. doi: 10.1111/apt.13191. [Fu SC, Huang YW, Wang TC, et al. Increased risk of hepatocellular carcinoma in chronic hepatitis B patients with new onset diabetes: a nationwide cohort study[J]. Aliment Pharmacol Ther, 2015, 41(11): 1200-9.] [DOI] [PubMed] [Google Scholar]
- 13.Kim K, Choi S, Park SM. Association of fasting serum glucose level and type 2 diabetes with hepatocellular carcinoma in men with chronic hepatitis B infection: a large cohort study. Eur J Cancer. 2018;102:103–13. doi: 10.1016/j.ejca.2018.07.008. [Kim K, Choi S, Park SM. Association of fasting serum glucose level and type 2 diabetes with hepatocellular carcinoma in men with chronic hepatitis B infection: a large cohort study[J]. Eur J Cancer, 2018, 102: 103-13.] [DOI] [PubMed] [Google Scholar]
- 14.Li Q, Li WW, Yang X, et al. Type 2 diabetes and hepatocellular carcinoma: a case-control study in patients with chronic hepatitis B. Int J Cancer. 2012;131(5):1197–202. doi: 10.1002/ijc.27337. [Li Q, Li WW, Yang X, et al. Type 2 diabetes and hepatocellular carcinoma: a case-control study in patients with chronic hepatitis B [J]. Int J Cancer, 2012, 131(5): 1197-202.] [DOI] [PubMed] [Google Scholar]
- 15.Shyu YC, Huang TS, Chien CH, et al. Diabetes poses a higher risk of hepatocellular carcinoma and mortality in patients with chronic hepatitis B: a population-based cohort study. J Viral Hepat. 2019;26(6):718–26. doi: 10.1111/jvh.13077. [Shyu YC, Huang TS, Chien CH, et al. Diabetes poses a higher risk of hepatocellular carcinoma and mortality in patients with chronic hepatitis B: a population-based cohort study[J]. J Viral Hepat, 2019, 26(6): 718-26.] [DOI] [PubMed] [Google Scholar]
- 16.Hsiang JC, Gane EJ, Bai WW, et al. Type 2 diabetes: a risk factor for liver mortality and complications in hepatitis B cirrhosis patients. J Gastroenterol Hepatol. 2015;30(3):591–9. doi: 10.1111/jgh.12790. [Hsiang JC, Gane EJ, Bai WW, et al. Type 2 diabetes: a risk factor for liver mortality and complications in hepatitis B cirrhosis patients[J]. J Gastroenterol Hepatol, 2015, 30(3): 591-9.] [DOI] [PubMed] [Google Scholar]
- 17.张 锋. 肝癌免疫耐受机制研究进展. 复旦学报: 医学版. 2020;47(2):280–7. doi: 10.3969/j.issn.1672-8467.2020.02.023. [张锋. 肝癌免疫耐受机制研究进展[J]. 复旦学报: 医学版, 2020, 47 (2): 280-7.] [DOI] [Google Scholar]
- 18.李 杰, 闫 堃, 杨 屹, et al. 白介素-17通过拮抗γ-干扰素的作用促进小鼠肝癌细胞的生长与增殖. http://www.j-smu.com/oa/darticle.aspx?type=view&id=2019011. 南方医科大学学报. 2019;39(1):1–5. [李杰, 闫堃, 杨屹, 等. 白介素-17通过拮抗γ-干扰素的作用促进小鼠肝癌细胞的生长与增殖[J]. 南方医科大学学报, 2019, 39(1): 1-5.] [Google Scholar]
- 19.Levrero M, Zucman-Rossi J. Mechanisms of HBV-induced hepatocellular carcinoma. http://www.sciencedirect.com/science/article/pii/S0168827816001525. J Hepatol. 2016;64(1 Suppl):S84–101. doi: 10.1016/j.jhep.2016.02.021. [Levrero M, Zucman-Rossi J. Mechanisms of HBV-induced hepatocellular carcinoma[J]. J Hepatol, 2016, 64(1 Suppl): S84-101.] [DOI] [PubMed] [Google Scholar]
- 20.任 彦瑜, 袁 国盛, 周 宇辰, et al. 慢性乙型肝炎患者肝脏良性占位的发病率及其特点: 基于39450例彩色多普勒超声的病例对照研究. http://www.j-smu.com/oa/darticle.aspx?type=view&id=2019101149. 南方医科大学学报. 2019;39(10):1149–54. doi: 10.12122/j.issn.1673-4254.2019.10.03. [任彦瑜, 袁国盛, 周宇辰, 等. 慢性乙型肝炎患者肝脏良性占位的发病率及其特点: 基于39450例彩色多普勒超声的病例对照研究[J]. 南方医科大学学报, 2019, 39(10): 1149-54.] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Ward PS, Thompson CB. Metabolic reprogramming: a cancer hallmark even Warburg did not anticipate. Cancer Cell. 2012;21(3):297–308. doi: 10.1016/j.ccr.2012.02.014. [Ward PS, Thompson CB. Metabolic reprogramming: a cancer hallmark even Warburg did not anticipate[J]. Cancer Cell, 2012, 21 (3): 297-308.] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Roberts DL, Dive C, Renehan AG. Biological mechanisms linking obesity and cancer risk: new perspectives. Annu Rev Med. 2010;61:301–16. doi: 10.1146/annurev.med.080708.082713. [Roberts DL, Dive C, Renehan AG. Biological mechanisms linking obesity and cancer risk: new perspectives[J]. Annu Rev Med, 2010, 61: 301-16.] [DOI] [PubMed] [Google Scholar]
- 23.Tilg H, Moschen AR, Roden M. NAFLD and diabetes mellitus. Nat Rev Gastroenterol Hepatol. 2017;14(1):32–42. doi: 10.1038/nrgastro.2016.147. [Tilg H, Moschen AR, Roden M. NAFLD and diabetes mellitus[J]. Nat Rev Gastroenterol Hepatol, 2017, 14(1): 32-42.] [DOI] [PubMed] [Google Scholar]
- 24.Li XF, Chen C, Xiang DM, et al. Chronic inflammation-elicited liver progenitor cell conversion to liver cancer stem cell with clinical significance. Hepatology. 2017;66(6):1934–51. doi: 10.1002/hep.29372. [Li XF, Chen C, Xiang DM, et al. Chronic inflammation-elicited liver progenitor cell conversion to liver cancer stem cell with clinical significance[J]. Hepatology, 2017, 66(6): 1934-51.] [DOI] [PubMed] [Google Scholar]
- 25.Altalhi W, Sun X, Sivak JM, et al. Diabetes impairs arterio-venous specification in engineered vascular tissues in a perivascular cell recruitment-dependent manner. Biomaterials. 2017;119:23–32. doi: 10.1016/j.biomaterials.2016.12.003. [Altalhi W, Sun X, Sivak JM, et al. Diabetes impairs arterio-venous specification in engineered vascular tissues in a perivascular cell recruitment-dependent manner[J]. Biomaterials, 2017, 119: 23-32.] [DOI] [PubMed] [Google Scholar]
- 26.Okonkwo U, DiPietro L. Diabetes and wound angiogenesis. Int J Mol Sci. 2017;18(7):1419. doi: 10.3390/ijms18071419. [Okonkwo U, DiPietro L. Diabetes and wound angiogenesis[J]. Int J Mol Sci, 2017, 18(7): 1419.] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.陈 镜妃, 罗 启慧, 黄 超, et al. 血管内皮生长因子与色素上皮衍生因子在糖尿病猕猴视网膜病变早变早期的表达. http://www.j-smu.com/oa/darticle.aspx?type=view&id=2017091217. 南方医科大学学报. 2017;37(9):1217–21. doi: 10.3969/j.issn.1673-4254.2017.09.13. [陈镜妃, 罗启慧, 黄超, 等. 血管内皮生长因子与色素上皮衍生因子在糖尿病猕猴视网膜病变早变早期的表达[J]. 南方医科大学学报, 2017, 37(9): 1217-21.] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Moore MM, Chua W, Charles KA, et al. Inflammation and cancer: causes and consequences. Clin Pharmacol Ther. 2010;87(4):504–8. doi: 10.1038/clpt.2009.254. doi: 10.1038/clpt.2009.254. [Moore MM, Chua W, Charles KA, et al. Inflammation and cancer: causes and consequences[J]. Clin Pharmacol Ther, 2010, 87(4): 504-8.] [DOI] [PubMed] [Google Scholar]
- 29.Mitra A, Yan J, Xia X, et al. IL6-mediated inflammatory loop reprograms normal to epithelial-mesenchymal transition + metastatic cancer stem cells in preneoplastic liver of transforming growth factor beta-deficient β2-spectrin +/- mice. Hepatology. 2017;65(4):1222–36. doi: 10.1002/hep.28951. [Mitra A, Yan J, Xia X, et al. IL6-mediated inflammatory loop reprograms normal to epithelial-mesenchymal transition + metastatic cancer stem cells in preneoplastic liver of transforming growth factor beta-deficient β2-spectrin +/- mice[J]. Hepatology, 2017, 65(4): 1222-36.] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Hsu YC, Yip TC, Ho HJ, et al. Development of a scoring system to predict hepatocellular carcinoma in Asians on antivirals for chronic hepatitis B. J Hepatol. 2018;69(2):278–85. doi: 10.1016/j.jhep.2018.02.032. [Hsu YC, Yip TC, Ho HJ, et al. Development of a scoring system to predict hepatocellular carcinoma in Asians on antivirals for chronic hepatitis B[J]. J Hepatol, 2018, 69(2): 278-85.] [DOI] [PubMed] [Google Scholar]
- 31.Chen CL, Yang HI, Yang WS, et al. Metabolic factors and risk of hepatocellular carcinoma by chronic hepatitis B/C infection: a follow-up study in Taiwan. Gastroenterology. 2008;135(1):111–21. doi: 10.1053/j.gastro.2008.03.073. [Chen CL, Yang HI, Yang WS, et al. Metabolic factors and risk of hepatocellular carcinoma by chronic hepatitis B/C infection: a follow-up study in Taiwan[J]. Gastroenterology, 2008, 135(1): 111-21.] [DOI] [PubMed] [Google Scholar]
- 32.Tan YF, Wei SY, Zhang W, et al. Type 2 diabetes mellitus increases the risk of hepatocellular carcinoma in subjects with chronic hepatitis B virus infection: a meta-analysis and systematic review. Cancer Manag Res. 2019;11:705–13. doi: 10.2147/CMAR.S188238. [Tan YF, Wei SY, Zhang W, et al. Type 2 diabetes mellitus increases the risk of hepatocellular carcinoma in subjects with chronic hepatitis B virus infection: a meta-analysis and systematic review [J]. Cancer Manag Res, 2019, 11: 705-13.] [DOI] [PMC free article] [PubMed] [Google Scholar]