

Abstract
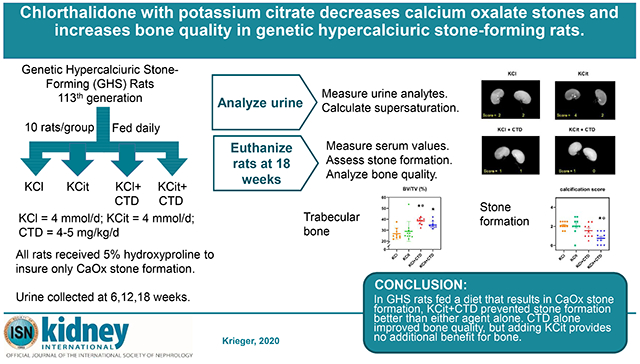
To study human idiopathic hypercalciuria we developed an animal model, genetic hypercalciuric stone-forming rats, whose pathophysiology parallels that of human idiopathic hypercalciuria. Fed the oxalate precursor, hydroxyproline, every rat in this model develops calcium oxalate stones. Using this rat model, we tested whether chlorthalidone and potassium citrate combined would reduce calcium oxalate stone formation and improve bone quality more than either agent alone. These rats (113 generation) were fed a normal calcium and phosphorus diet with hydroxyproline and divided into four groups: diets plus potassium chloride as control, potassium citrate, chlorthalidone plus potassium chloride, or potassium citrate plus chlorthalidone. Urine was collected at six, 12, and 18 weeks and kidney stone formation and bone parameters were determined. Compared to potassium chloride, potassium citrate reduced urinary calcium, chlorthalidone reduced it further and potassium citrate plus chlorthalidone even further. Potassium citrate plus chlorthalidone decreased urine oxalate compared to all other groups. There were no significant differences in calcium oxalate supersaturation in any group. Neither potassium citrate nor chlorthalidone altered stone formation. However, potassium citrate plus chlorthalidone significantly reduced stone formation. Vertebral trabecular bone increased with chlorthalidone and potassium citrate plus chlorthalidone. Cortical bone area increased with chlorthalidone but not potassium citrate or potassium citrate plus chlorthalidone. Mechanical properties of trabecular bone improved with chlorthalidone, but not with potassium citrate plus chlorthalidone. Thus in genetic hypercalciuric stone-forming rats fed a diet resulting in calcium oxalate stone formation, potassium citrate plus chlorthalidone prevented stone formation better than either agent alone. Chlorthalidone alone improved bone quality, but adding potassium citrate provided no additional benefit.
Keywords: nephrolithiasis, hypercalciuria, chlorthalidone, potassium citrate, calcium oxalate
Graphical Abstract
INTRODUCTION
Calcium (Ca) oxalate (Ox) stones are most common in human stone formers1, the majority of whom have idiopathic hypercalciuria (IH)2. The increase in urine Ca leads to increased supersaturation with respect to Ca-containing solid phases, principally CaOx and Ca hydrogen phosphate (CaP), which increases the probability for nucleation and growth of crystals into clinically significant stones.
To model human IH we generated a strain of rats, the genetic hypercalciuric stone-forming (GHS) rats. Selectively inbred for over 113 generations, GHS rats are hypercalciuric compared to their parent Sprague-Dawley rats3. When fed a normal Ca diet, all GHS rats form CaP kidney stones4. Like patients with IH, these rats have increased intestinal Ca absorption4, 5, decreased renal Ca reabsorption6, and increased bone resorption7, leading to increased urine Ca excretion and CaP stone formation4 as well as a decrease in BMD8, 9 The addition of the oxalate precursor, hydroxyproline, to the diet of GHS rats results in universal formation of CaOx stones10. Serum 1,25-dihydroxyvitamin D3 levels are normal11. We have shown that hypercalciuria in the GHS rats is polygenic12 as it is in humans13. Thus the pathophysiology of the hypercalciuria in the GHS rats closely mirrors that of humans with IH.
Two pharmacologic therapies used to decrease recurrent stone formation in humans are potassium citrate (KCit) or thiazide diuretics, alone or in combination2, 14 In humans both KCit and thiazides individually have been shown to decrease stone formation15 and improve bone quality; however, there is little data directly comparing the efficacy of these two medications in combination. We have previously shown that giving GHS rats thiazides (specifically chlorthalidone, CTD) decreases urine Ca, reduces urine CaP supersaturation and decreases CaP stone formation16. We also found that CTD improves BMD and bone quality in GHS rats17. In another study we observed that giving GHS rats KCit also decreases urine Ca, but increases CaP supersaturation and does not decrease stone formation18. Most recently we found that CTD alone was superior to the combination of CTD plus KCit for reducing CaP stone formation and improving BMD and bone quality in the GHS rats19. As CaOx stones are the type most commonly found in humans, in the current study we tested the hypothesis that the combination of CTD and KCit would reduce CaOx stone formation and improve bone quality in GHS rats better than either agent alone.
METHODS (full Methods in supplement)
Study Protocol
Three month old male 113th generation GHS rats were randomly divided into 4 groups (each n=10) and housed individually in metabolic cages. All rats were fed a fixed amount of a normal Ca (1.2% Ca) and phosphorus (0.65%) diet containing 5% hydroxyproline, supplemented with either KCl (4 mmol/d) as control, KCit (4 mmol/d), CTD (4-5mg/kg/d)+KCl or KCit+CTD. At weeks 6, 12 and 18, 24h urine was collected for analyses as described previously19. Each rat received an intraperitoneal injection of 1% calcein green at 10 and 2 days prior to sacrifice for dynamic histomorphometry. At 18 weeks, rats were euthanized, blood collected and organs removed. Univ. of Rochester Committee for Animal Resources approved all procedures.
Urine and Serum Chemistries
Urine Ca, P, ammonium, potassium, and sodium were measured on a Beckman AU autoanalyzer and urine pH using a glass electrode. Urine citrate and sulfate were measured by ion chromatography and oxalate was measured enzymatically. All urine solutes were measured at 6, 12 and 18 weeks and a mean value for each time period as well as an overall mean was calculated. Serum Ca, P, Na, K, Cl, bicarbonate and creatinine were measured with a Roche 501 clinical chemistry analyzer which utilizes ion selective electrodes for determinations of Na, K and Cl and chemical assays for Ca, P, bicarbonate and creatinine. All methods have been used previously17–23.
Urine Supersaturation
Urine supersaturation with respect to CaOx and CaP solid phases were calculated using the computer program EQUIL224 as done previously4, 10, 18, 19, 23.
Kidney Stone Formation
Kidneys, ureters and bladders were imaged to determine extent of kidney stone formation. Three observers blinded to treatment scored all radiographs on a scale ranging from 0 (no stones) to 4 (extensive stones) and the mean score reported for each rat.
Bone Measurements
Dual Energy X-ray Absorptiometry
Dual energy X-ray absorptiometry was used to determine tissue density and mineral content. The areal bone mineral density (aBMD), bone mineral content (BMC) and bone area (BArea) were measured.
Micro-Computed Tomography
Micro-computed tomography (microCT) was used to measure volumetric bone mineral density (vBMD) and microarchitecture of the mid-diaphysis of right femurs and L6 vertebrae.
Tissue-Level Remodeling
Tissue-level remodeling was assessed via histomorphometry on both mineralized (undecalcified) bone and unmineralized (decalcified) bone. Stained sections were viewed microscopically and results quantified.
Histomorphometry
Undecalcified histomorphometry differentiates between mineralized and demineralized tissue. Sections were used for static and dynamic histomorphometric analysis. Cross-sections of the left distal tibiae were used for back-scattered electron microscopy. Sections of undecalcified right tibiae were stained and quantified. Trabecular bone was analyzed in the proximal tibia metaphysis. Sections of calcein labeled undecalcified right tibiae were used for dynamic histomorphometry and quantified. Sections of decalcified left tibiae were stained for tartrate-resistant acid phosphatase for assessment of osteoclasts and bone resorption.
Biomechanical Properties
Biomechanics of femurs were assessed to define a load-displacement curve and ultimate load, stiffness, ultimate displacement, and energy to break. Data were normalized for specimen geometry. Three-point bending was performed on the right femurs. Vertebral compression was measured on L6 vertebrae. Vertebral compression does not result in complete fracture; the failure point was determined by an 8-10% reduction in load. The proximal end of the femurs was subjected to femoral neck fracture.
Degree of Mineralization
Back-scattered electron microscopy (BSE) on both right tibiae and left distal tibiae cross-section samples was done with a scanning electron microscope and images were taken using a solid state BSE detector.
Statistical Analysis
Urine analytes, serum values and stone formation, expressed as mean±SE, were compared among the four treatment groups by a one-way ANOVA with subsequent Bonferroni correction for pairwise comparison among the treatment groups (Statistica, StatSoft, Tulsa, OK). The interaction effects of KCit and CTD at 18 weeks were tested by comparing to KCI using linear regression models on urine analytes, serum values and stone formation (SAS 9.4, Cary, NC), assuming normally distributed. Bone parameters were compared by t-test using the SPSS Statistics 20 program (SPSS, Chicago, IL) and expressed as mean±SD. p<0.05 was considered significant.
RESULTS
Urine and Serum
Mean overall urine Ca for the entire 18 week study was decreased in rats fed KCit and in those fed CTD while the combination of KCit+CTD decreased it further (Figure 1, Supplemental Figure 1 for each collection period). Mean overall urine citrate and urine P were both increased by KCit but not CTD. KCit+CTD increased both urine citrate and urine P compared to KCl and to CTD; however, the increases were less than that observed with KCit alone. There were no drug interactions between KCit and CTD for any of these parameters.
Figure 1. Urine calcium, citrate and phosphate.
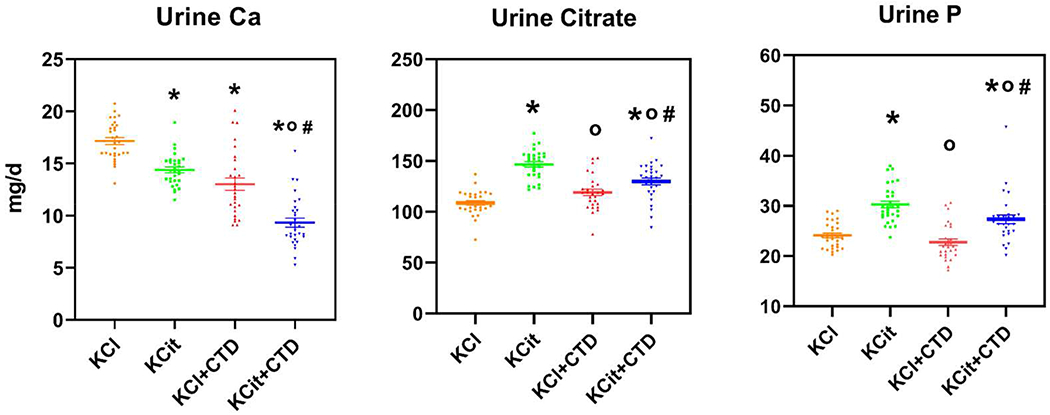
Rat diets were all supplemented hydroxyproline and with either KCl (4 mmol/d) as a control, potassium citrate (KCit, 4 mmol/d), chlorthalidone (CTD, 4-5mg/kg/d)+KCl or KCit+CTD. Twenty-four-hour urine collections were done at 6, 12 and 18 wks for analysis of solute levels as described in Methods and an overall mean of all three collections was calculated. Results are mean±SE for 10 rats/group. *p<0.05 vs KCl, op<0.05 vs KCit alone, #p<0.05 vs CTD alone.
Mean overall urine oxalate was not altered by KCit alone or CTD alone compared to KCl while KCit+CTD decreased urine oxalate compared to each of the other groups (Figure 2, Supplemental Figure 2 for each collection period). Mean urine ammonium (NH4) was decreased by KCit, but increased by CTD. KCit+CTD decreased urine NH4 comparably to KCit alone. There was a negative drug interaction for the effects of KCit and CTD on urine NH4 (p<0.0001). Urine pH was increased by KCit and decreased by CTD. KCit+CTD increased urine pH comparably to KCit alone. There was a positive drug interaction for the effects of KCit and CTD on urine pH (p<0.0001).
Figure 2. Urine oxalate, NH4 and pH.
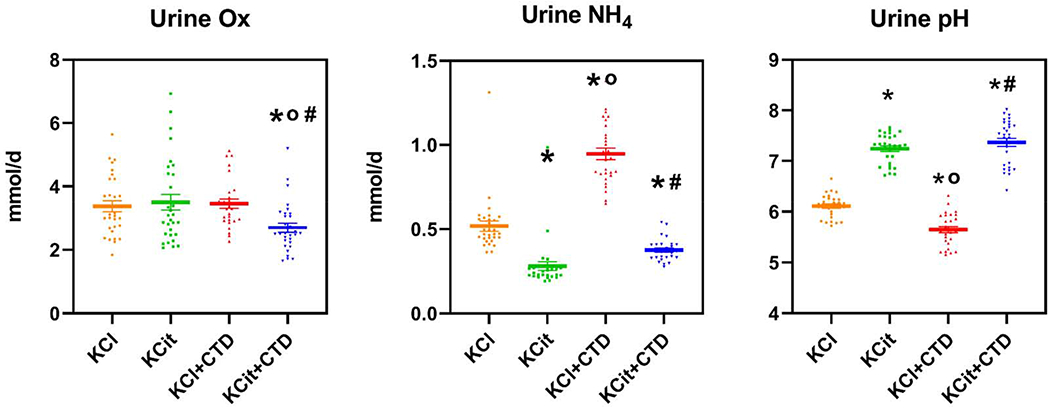
Rat diets were all supplemented hydroxyproline and with either KCl (4 mmol/d) as a control, potassium citrate (KCit, 4 mmol/d), chlorthalidone (CTD, 4-5mg/kg/d)+KCl or KCit+CTD. Twenty-four hour-urine collections were done at 6, 12 and 18 wks for analysis of solute levels as described in Methods and an overall mean of all three collections was calculated. Results are mean±SE for 10 rats/group. *p<0.05 vs KCl, op<0.05 vs KCit alone, #p<0.05 vs CTD alone.
Mean overall urine volume for the entire 18 week study was decreased in rats fed CTD while the combination of KCit+CTD decreased it further (Figure 3, Supplemental Figure 3 for each collection period). There were no drug interactions between KCit and CTD on urine volume. Mean overall urine Na was not altered by KCit and KCl+CTD but fell with KCit+CTD. There were no drug interactions between KCit and CTD on urine Na. Mean urine K was not altered by KCit but increased with CTD and fell with KCit+CTD compared to CTD alone. There was a positive drug interaction between KCit and CTD for urine K (p=.012).
Figure 3. Urine volume, Na, K.
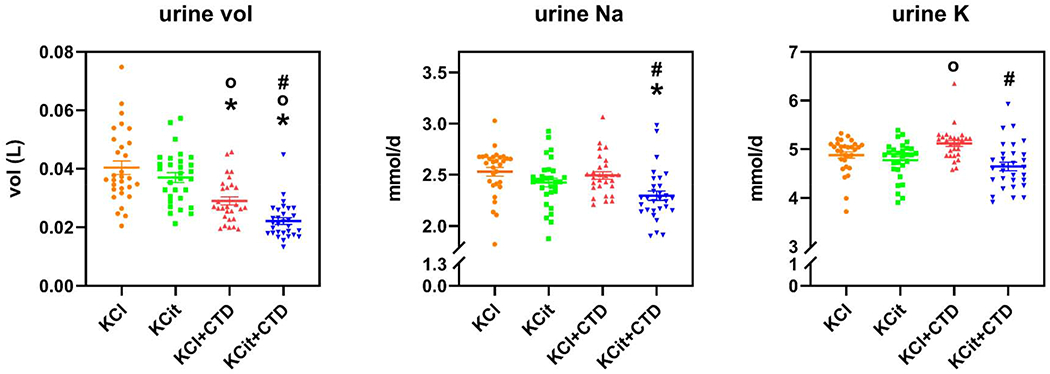
Rat diets were all supplemented hydroxyproline and with either KCl (4 mmol/d) as a control, potassium citrate (KCit, 4 mmol/d), chlorthalidone (CTD, 4-5mg/kg/d)+KCl or KCit+CTD. Twenty-four hour-urine collections were done at 6, 12 and 18 wks for analysis of solute levels as described in Methods and an overall mean of all three collections was calculated. Results are mean±SE for 10 rats/group. *p<0.05 vs KCl, op<0.05 vs KCit alone, #p<0.05 vs CTD alone.
Mean overall urine supersaturation with respect to CaP was increased by KCit, while CTD had no effect on supersaturation compared to KCl (Figure 4, Supplemental Figure 4 for each collection period). KCit+CTD increased CaP supersaturation compared to KCl and to CTD. There was a positive drug interaction for the effects of KCit and CTD on CaP supersaturation (p=0.0003). There was no effect of KCit, CTD or the combination of KCit+CTD on overall CaOx supersaturation and no drug interaction for the effects of KCit and CTD on CaOx supersaturation.
Figure 4. Urine supersaturation of CaP and CaOx.
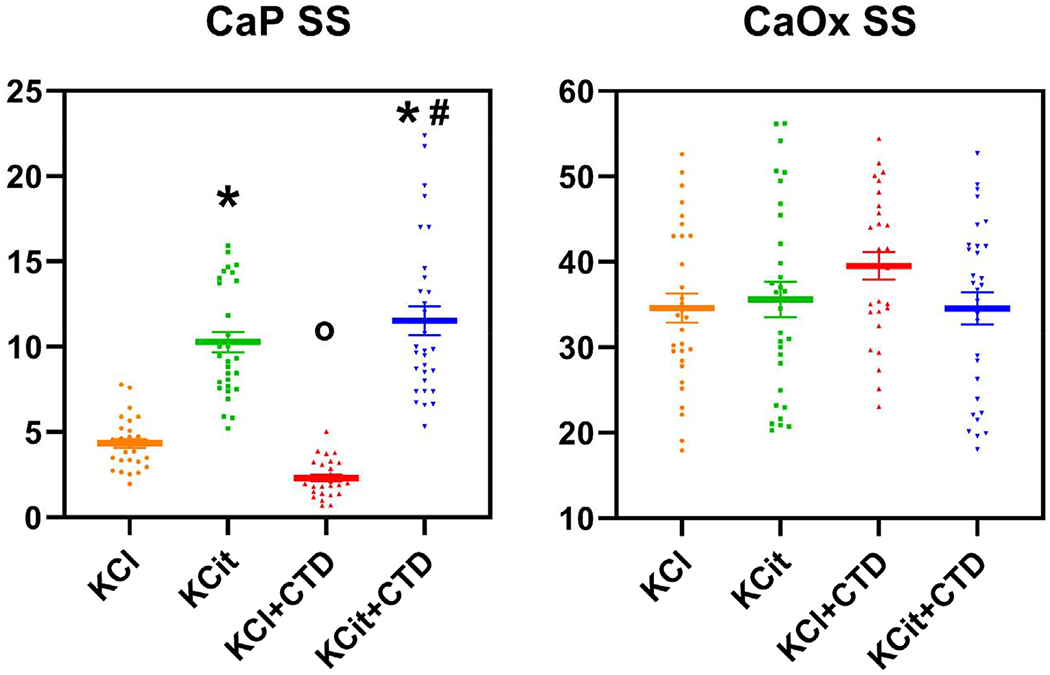
Rat diets were all supplemented with hydroxyproline and with either KCl (4 mmol/d) as a control, potassium citrate (KCit, 4 mmol/d), chlorthalidone (CTD, 4-5mg/kg/d) + KCl or KCit+CTD. Twenty-four-hour urine collections were done at 6, 12 and 18 wks for analysis of solute levels as described in Methods. These values were used to calculate relative supersaturation and an overall mean of all three collections was calculated. Values for relative supersaturation are unitless. Results are mean±SE for 10 rats/group. *p<0.05 vs KCl, op<0.05 vs KCit alone, #p<0.05 vs CTD alone.
At 18 weeks on each diet, serum values for chloride, bicarbonate, P and creatinine were not different between groups (Table 1). Serum Na was decreased by KCit+CTD compared to KCl. Serum potassium was decreased by CTD and by KCit+CTD compared to KCl. Serum Ca was increased by CTD and by KCit+CTD compared to both KCl and KCit alone.
Table 1.
Serum measurements after 18 weeks in GHS rats fed KCl, KCit, KCl+CTD or KCit+CTD with OH-proline.
| solute | KCl | KCit | KCl+CTD | KCit+CTD |
|---|---|---|---|---|
| Sodium (mmol/L) | 144.8 ± 0.7 | 142.7 ± 0.7 | 142.7 ± 0.5 | 141.5 ± 0.9a |
| Potassium (mmol/L) | 4.67 ± 0.13 | 4.44 ± 0.18 | 3.88 ± 0.17a | 3.73 ± 0.14a,b |
| Chloride ( mmol/L) | 100.4 ± 0.5 | 89.4 ± 8.9 | 95.3 ± 0.6 | 93.9 ± 0.6 |
| Bicarbonate (mmol/L) | 24.6 ± 0.5 | 24.8 ± 0.7 | 25.0 ± 0.4 | 26.4 ± 0.2 |
| Calcium (mg/dL) | 10.2 ± 0.08 | 10.2 ± 0.07 | 10.7 ± .06a,b | 10.6 ± 0.3a,b |
| Phosphate (mg/dL) | 5.56 ± 0.20 | 6.08 ± 0.40 | 5.97 ± 0.21 | 5.74 ± 0.22 |
| Creatinine (mg/dL) | 0.30 ± 0.01 | 0.30 ± 0.01 | 0.32 ± 0.01 | 0.32 ± 0.02 |
Results are mean ± SE for 9-10 rats/group.
p <0.05 vs KCl alone;
p<0.05 vs KCit alone.
There were no significant differences comparing KCl+CTD to KCit+CTD.
Stone Formation
Representative radiographs of kidneys at 18 weeks on the indicated diets are shown in Figure 5a and quantitation of the radiographs from all the rats in Figure 5b. Significant CaOx calcification was found in all rats fed the KCl control diet. KCit alone and CTD alone had no effect on CaOx stone formation. The combination of KCit+CTD led to less stone formation than those given KCl or KCit. There was no drug interaction for the effects of KCit and CTD.
Figure 5. Kidney stones and calcification.
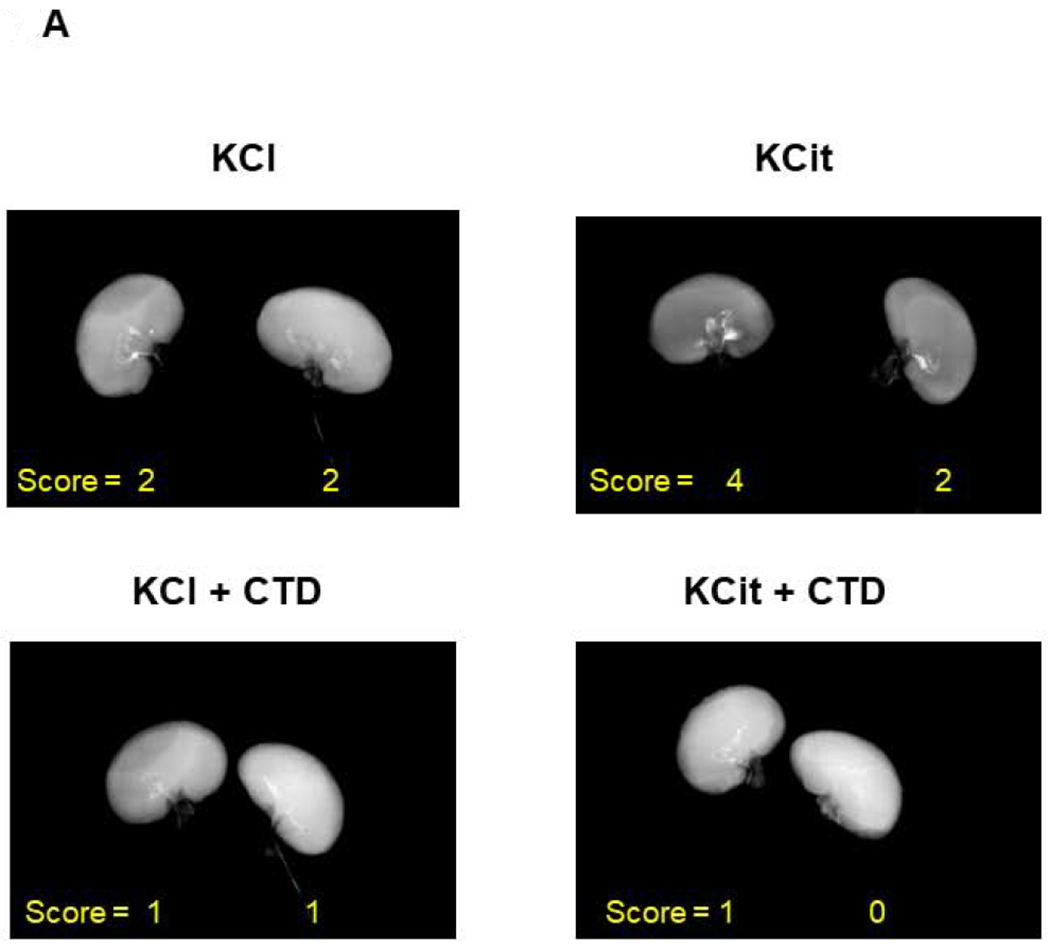
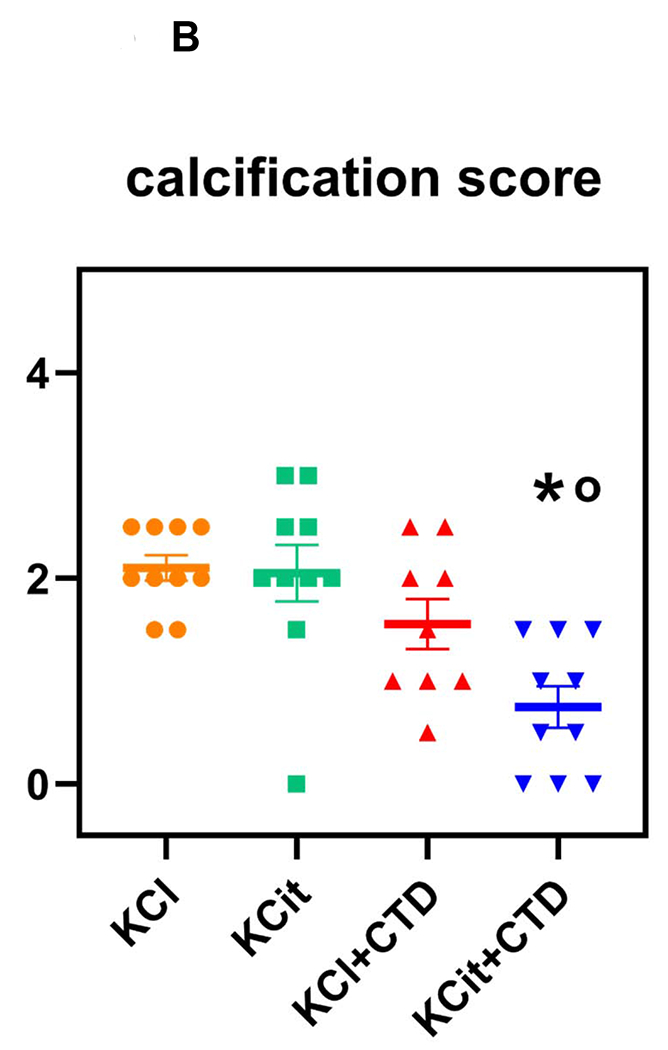
At the conclusion of the 18 wk study the extent of kidney stones and calcification were determined by three observers as described in Methods. A) Representative x-rays of kidneys from rats receiving KCl, KCit, CTD or KCit+CTD. B) Quantitation of stone formation and calcification in all rats (Mean±SE, n=10/group). *p<0.05 vs KCl, op<0.05 vs KCit alone, #p<0.05 vs CTD alone.
Bone
MicroCT analysis demonstrated that trabecular bone volume (BV/TV) in the L6 vertebrae was increased with both CTD and KCit+CTD compared to KCl and with CTD compared to KCit (Figure 6A). There was no difference in trabecular thickness (Tb. Th.) in L6 in response to any of the treatments. Trabecular number (Tb.N.) in L6 was increased by CTD compared to KCl and to KCit and KCit+CTD increased Tb.N compared to KCl. Trabecular spacing (Tb.Sp.) in L6 was decreased by CTD compared to KCl and to KCit while KCit+CTD decreased Tb.Sp. compared to KCl.
Figure 6. Changes in bone parameters after 18 weeks.
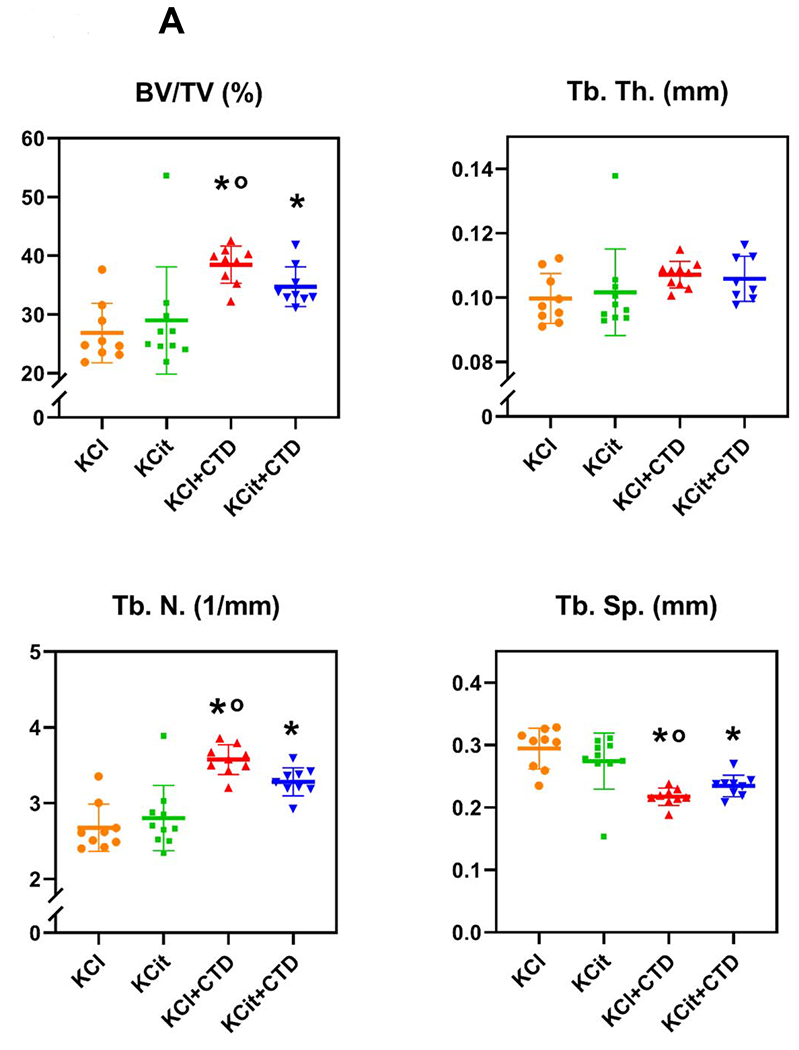
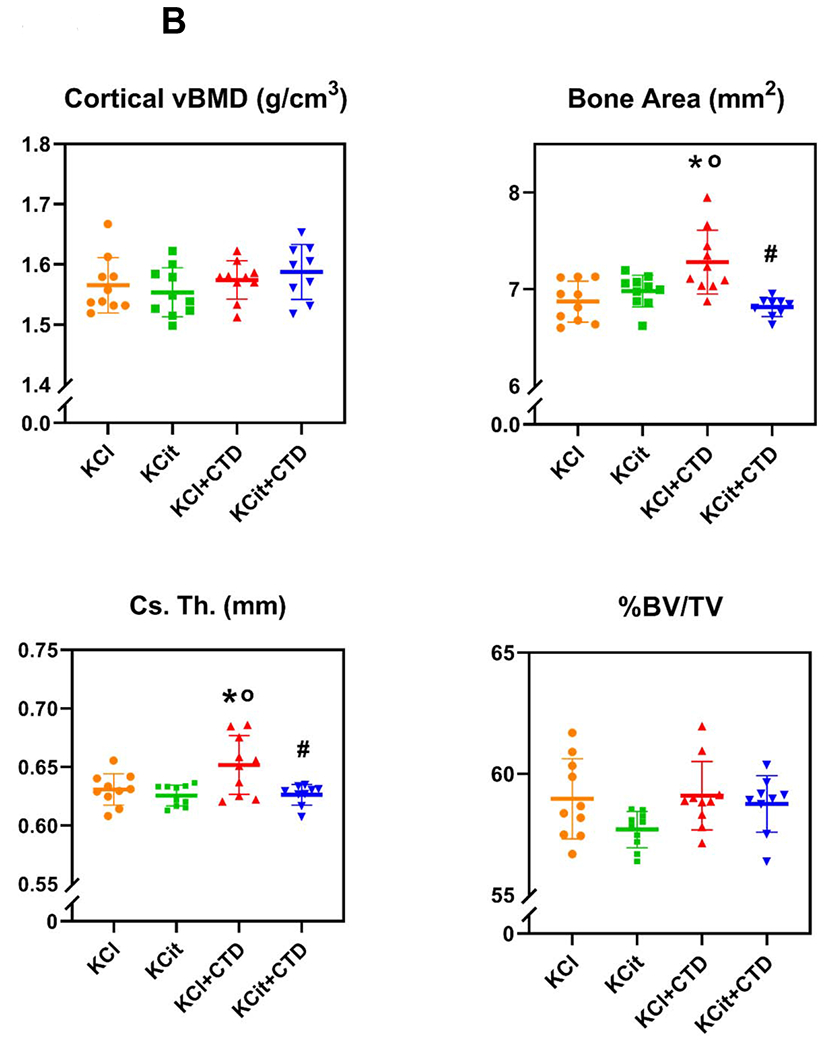
Rat diets were all supplemented with hydroxyproline and with either KCl (4 mmol/d) as a control, potassium citrate (KCit, 4 mmol/d), chlorthalidone (CTD, 4-5mg/kg/d) + KCl or KCit+CTD. At the conclusion of the 18 wk study, bones were collected from all rats and analyzed as described in Methods. A) Percent bone volume (BV/TV), trabecular thickness (Tb.Th.), trabecular number (Tb.N.) and trabecular separation (Tr. Sp.) of L6 vertebrae are presented. B) Cortical volumetric bone mineral density (vBMD), bone area (B.Ar.), cortical thickness (Cs.Th), and % bone volume/total volume (%BV/TV) of femoral cortical bone are presented. Results are mean±SD for n=10 bones/group. p<0.05 vs KCl, op<0.05 vs KCit alone. There were no significant differences comparing KCl+CTD to KCit+CTD.
There was no change in volumetric BMD in cortical bone from the femur of rats on any of the treatments (Figure 6B). Bone area and cross sectional thickness in femurs from rats fed KCit were not different from KCl and were increased with CTD alone compared to both KCl and KCit. KCit+CTD did not alter bone area or cross sectional thickness compared to KCl and to KCit; however, both were decreased compared to CTD alone. There was no change in percent bone volume to total volume on any of the treatments.
Vertebral compression tests indicate that CTD supported a greater ultimate load, a greater failure load and a greater energy to fail compared to the KCl control, while KCit and KCit+CTD had no effect on any of these parameters (Table 2). For material properties, there was increased ultimate stress, failure stress and toughness with CTD compared to KCl and to KCit+CTD. When rats received KCit+CTD there was no difference compared to KCl. The results from three-point bending tests indicate that cortical bone from KCit fed rats supported a larger failure displacement and larger failure strain compared to KCl (Table 2), while stiffness and failure strain were increased by CTD. KCit+CTD did not alter any cortical mechanical properties compared to KCl.
Table 2.
Mechanical properties of trabecular (vertebral compression) and cortical (three-point bending) bone from GHS rats fed KCl, KCit, KCl+CTD or KCit+CTD.
| KCl | KCit | KCl+CTD | KCit+CTD | |
|---|---|---|---|---|
| Vertebral compression | ||||
| Structural Properties | ||||
| Ultimate load (N) | 185.9±34.1 | 225.6±34.4 | 269.5±40.6a | 227.5±43.8 |
| Failure load (N) | 169.1±44.2 | 216.2±43.2 | 262.9±38.2a | 219.6±52.3 |
| Energy to fail (mJ) | 28.5±16.8 | 44.5±17.1 | 62.8±17.7a | 46.9±18.0 |
| Failure displacement (mm) | 0.45±0.21 | 0.49±0.22 | 0.57±0.20 | 0.58±0.26 |
| Stiffness (N/mm) | 744.0±417.4 | 685.6±219.1 | 686.6±123.3 | 634.9±129.7 |
| Material Properties | ||||
| Ultimate stress (MPa) | 33.6±6.8 | 41.9±6.5 | 51.9±11.9a | 38.7±8.5b |
| Failure stress (MPa) | 30.5±8.4 | 40.1±7.9 | 50.7±11.6a | 37.2±9.6b |
| Failure strain (%) | 9.8±4.1 | 10.0±4.5 | 11.9±4.2 | 12.0±4.8 |
| Toughness (mJ/mm3) | 0.7±0.4 | 1.4±0.6 | 2.1±0.8a | 1.2±0.6b |
| Young’s Modulus (MPa) | 614.6±364.6 | 598.4±140.5 | 626.0±145.3 | 512.6±112.4 |
| Three-point bending | ||||
| Structural Properties | ||||
| Failure Displacement (mm) | 0.44±0.07 | 0.57±0.10a | 0.57±0.12 | 0.57±0.14 |
| Failure Load (N) | 152.1±5.0 | 144.8±15.2 | 155.0±14.9 | 144.5±11.7 |
| Energy to fail (N) | 49.2±10.3 | 45.7±15.2 | 47.1±14.5 | 43.4±15.4 |
| Stiffness (N/mm) | 450.8±47.3 | 496.0±49.2 | 513.9±46.4a | 480.5±40.8 |
| Material Properties | ||||
| Failure Stress (MPa) | 89.1±6.0 | 85.5±9.6 | 88.1±16.8 | 85.4±7.8 |
| Failure Strain (%) | 4.9±0.7 | 6.3±1.1a | 6.4±1.4a | 6.2±1.5 |
| Toughness (mJ/mm3) | 317.1±67.7 | 300.0±106.0 | 303.7±123.7 | 280.3±101.2 |
| Young’s Modulus (MPa) | 2395.5±244.2 | 2660.5±216.6 | 2602.5±430.1 | 2606.1±291.5 |
Results are mean ± SD for 9-10 rats/group.
p <0.05 vs KCl alone
p<0.05 vs KCl+CTD.
For dynamic undecalcified histomorphometry, the percent bone volume to total volume was increased by KCit, CTD and KCit+CTD compared to KCl control (Table 3). Percent osteoid volume and percent osteoid surface were decreased by KCit, CTD and KCit+CTD compared to KCl. There were no changes in dynamic histomorphometry with any of the diets. The number of osteoclasts/total volume was significantly increased by KCit+CTD.
Table 3.
Histomorphometry analyses of tibiae from GHS rats fed KCl, KCit, KCl+CTD or KCit + CTD.
| KCl | KCit | KCl+CTD | KCit+CTD | |
|---|---|---|---|---|
| Histomorphometry | ||||
| Undecalcified Static | ||||
| BV/TV (%) | 0.18±0.05 | 0.25±0.03a | 0.31±0.04a,b | 0.29±0.04a |
| OV/BV (%) | 0.002±0.002 | 0.0005±0.0005a | 0.0003±0.0003a | 0.0002±0.0002a |
| OS/BS (%) | 0.10±0.18 | 0.01±0.01a | 0.006±0.007a | 0.008±0.008a |
| Osteoid width (μm) | 4.4±2.1 | 2.7±2.0 | 3.6±5.9 | 1.4±1.68 |
| Dynamic | ||||
| MS/BS (%) | 0.27±0.26 | 0.26±0.08 | 0.20±0.08 | 0.18±0.06 |
| MAR (μm/day) | 1.51±0.21 | 1.43±0.24 | 1.38±0.16 | 1.38±0.14 |
| BFR/BS (μm3/μm2/day) | 0.42±0.28 | 0.38±0.15 | 0.28±0.11 | 0.25±0.09 |
| Decalcified | ||||
| Oc.S/BS (%) | 0.47±0.29 | 0.32±0.19 | 0.41±0.17 | 0.42±0.12 |
| N.Oc/BS (1/mm) | 6.7±2.9 | 7.4±1.4 | 5.6±2.0 | 6.8±1.7 |
| N.Oc/TV (1/mm2) | 15.4±11.6 | 23.8±5.8 | 25.1±10.0 | 32.6±12.0a |
Results are mean ± SD for 8-10 rats/group. OV = osteoid volume; BV = bone volume; OS= osteoid surface; BS = bone surface; MS = mineralized surface; MAR = mineral apposition rate; BFR = bone formation rate; Oc.S = osteoclast surface; N.Oc. = number of osteoclasts; TV = total volume.
p <0.05 vs KCl alone;
p<0.05 vs KCit alone.
There were no significant differences comparing KCl+CTD to KCit+CTD.
DISCUSSION
Calcium oxalate stones are most prevalent in human stone formers1, the majority of whom have IH1, 2 . The increased urinary Ca excretion leads to an increase in supersaturation with respect to the Ca containing solid phases which increases the probability for nucleation and growth of crystals into clinically significant kidney stones. In addition to non-pharmacologic therapy, CaOx stones are generally treated with KCit and/or thiazide diuretics such as CTD2, 14 Each of these pharmacologic therapies has been shown to be effective in reducing stone recurrence; however, there is little data with respect to efficacy of combining them to further reduce stone formation15. Patients with IH often have reduced bone density and increased rate of fractures25. KCit and thiazide diuretics have also been shown individually to increase bone density26; and one study of 18 men and 10 women found that the combination of thiazides and potassium citrate reduced stone formation and increased bone density when combined with a low calcium diet27. The study presented here found that in GHS rats fed a diet that results solely in CaOx stone formation, the combination of KCit+CTD prevented stone formation better than either agent alone and that CTD alone improves bone quality, but the addition of KCit provides no additional benefit for bone.
The administration of KCit led to an increase in urinary citrate, a reduction in urinary Ca and an increase in urinary phosphate, all similar to what we have reported previously18, 19 After intestinal absorption, citrate leads to systemic alkalization leading to less tubular reabsorption of citrate and an increase in its excretion28. Increasing dietary citrate leads to a decrease in urine Ca through several known mechanisms. The systemic alkalization induced by dietary citrate leads to an increase in tubular fluid pH and an increase in renal tubular Ca reabsorption. It also leads to increased bone formation and decreased bone resorption29. The increased urinary P with KCit appears secondary to intestinal citrate binding Ca which decreases intestinal CaP complexation allowing more P to be absorbed and excreted. The administration of CTD also decreased urinary Ca. Thiazide diuretics increase tubular Ca reabsorption in animals and in man. We have shown in rats16 and in humans30 that the decrease in urinary Ca persists due to a concomitant reduction in intestinal Ca absorption. It is unclear why urine Ox was not altered by either KCit or KCl+CTD but fell significantly with KCit+CTD. This reduction of urine Ox with the combination therapy, but not with either therapy alone, was observed in each of the 3 individual urine collection periods. In our previous publication urinary oxalate also fell with KCit+CTD19 providing further validity to the observation. While we do not have a clear explanation as to why oxalate excretion fell with the combined therapy, it is possible that thiazides reduce Ca absorption and therefore leave more Ca in the intestine to bind oxalate and lower net absorption31. Citrate has been shown to reduce intestinal Ca absorption in a rat model32 so CTD and citrate together may be additive, or even synergistic, in lowering Ca absorption, providing greater Ca to bind intestinal oxalate and therefore reducing renal oxalate excretion. Further studies will be required to understand this interesting observation.
Neither KCit nor CTD alone or in combination led to an alteration in CaOx supersaturation yet the combination significantly reduced CaOx kidney stone formation. The reasons that stone formation fell, yet supersaturation was not altered, are not clear from this study. Urine CaOx supersaturation was almost twice as high in each of the four groups compared to GHS rats fed a diet without added hydroxyproline19; perhaps any changes induced by these medications were not sufficient to alter these high levels of supersaturation. While CaOx supersaturation was numerically lower with KCit+CTD than in any of the other groups, this reduction was not significant. While we present supersaturation data, as it appears to be an important parameter in regulating stone formation33, 34, we recognize that it is not the sole determinant of stone formation. For example calculated supersaturation dues not account for inhibitors or promoters of stone formation24. In addition, no calculated measure of supersaturation has been formally validated for use in rodents.
The increase in urine oxalate caused by the addition of the oxalate precursor hydroxyproline to the diet of GHS rats results in the formation of only CaOx stones10. Indeed in this study with hydroxyproline added to the diet, urine oxalate was approximately twice that of a similar study in which hydroxproline was not added to diet19. Previously we have shown that in GHS rats not given hydroxyproline, which form only CaP stones, CTD alone is superior to KCit or to KCit+CTD in reducing CaP stone formation and improving bone quality19. In both studies KCit and CTD, alone and in combination had remarkably similar effects on urine Ca, citrate, P, NH4 and pH. However, CaP crystal formation is sensitive to pH, the higher the pH the greater the supersaturation with respect to CaP, while CaOx crystal formation and supersaturation is relatively pH insensitive35. Similar to this prior study CTD, but not KCit, led to an improvement in bone density and quality, the addition of KCit to CTD did not improve density or quality further.
Thus based on the results of this study and that of our previous study19, the approach to preventing stones in hypercalciuric stone formers differs with stone type. With CaOx stones, KCit+CTD is most beneficial in preventing stones while with CaP stones CTD alone appears to be the optimal treatment.
In considering a direct interaction between the effects of KCit and the effects of CTD, there were differences in some, but not all, urine parameters that demonstrated a significant interaction effect when rats received both KCit+CTD. There was a lesser effect on urine NH4 and uric acid SS when both drugs were given than the sum of either alone. There was a greater effect on urine pH and CaP SS when both drugs were given than the sum of either alone. There was no significant interaction on urine Ca, citrate, oxalate, CaOx SS or stone formation when both drugs were given. Since there is no drug interaction with respect to CaOx SS or stone formation, the importance of these drug interactions is not clear.
Hypercalciuric stone formers generally have decreased bone density and increased propensity to fracture25. As we found previously, GHS rats given CTD with or without KCit had increased trabecular bone volume, though there was no increase in cortical bone mineral density. Most rat models are more sensitive to changes in trabecular bone than cortical bone because trabecular bone has many more cells than cortical bone and remodels eight times faster36. Rats given CTD alone demonstrated increased vertebral bone strength and material properties which was not observed when KCit was also given. KCit and CTD increased different structural properties of the bone, though the combination had no effect compared to control rats fed KCl. An increase in percent bone volume and a decrease in unmineralized osteoid was found in rats fed KCit alone, CTD alone or the combination when compared to control rats. The greater improvements in bone quality in response to CTD compared to KCit are similar to what we have found previously17, 19
In human studies both thiazide diuretics and KCit have been shown to improve bone mineral density26, 35 In three small studies of hypercalciuric stone formers, improvements in bone density and/or quality were found25, 37, 38 Many patients receive thiazide diuretics for hypertension. A meta-analysis of twenty-one observational studies including almost four hundred thousand patients concluded that there was a significant 24% reduction in the risk of hip fracture in those receiving thiazide diuretics39. Potassium citrate therapy for 11 months improved vertebral bone mineral density in patients with Ca nephrolithiasis40. Potassium citrate also improved distal radius BMD in hypercalciuric patients41. Bone mineral density as measured by CT scan was also improved by both thiazides and KCit42. In this study we again demonstrate that a thiazide diuretic improves bone density and the mechanical properties of bone which is consistent with observations in humans37,38. Why we did not find that KCit improved bone in GHS rats is unclear. Humans tend to eat an acid producing diet and KCit has been shown, in at least one study, to improve bone density in osteoporotic humans43. Perhaps if our GHS rats were fed a diet that results in more endogenous acid production KCit would lead to an improvement in bone density and quality.
In conclusion, we found that in GHS rats who universally form CaOx stones when fed hydroxyproline, the combination of KCit+CTD led to a greater reduction in stone formation than either agent alone. CTD alone improved bone density and quality while the addition of KCit had no additional benefit. Previously we have shown that for CaP stones, CTD alone is superior to KCit alone or KCit+CTD in preventing stone formation and, similar to the current study, to improve bone density and quality19. Thus, in this hypercalciuric model of kidney stones, optimal treatment appears to differ for the two most common types of kidney stones found in humans; KCit+CTD for CaOx stones and CTD alone for CaP stones. If these results are confirmed in human hypercalciuric CaOx stone formers, then the combination of these two agents, which are often used alone, would be beneficial in prevention of stone formation and at least the thiazide would help improve bone density and quality.
Supplementary Material
Figure 1 – Urine calcium, citrate and phosphate at 6, 12 and 18 weeks.
Figure 2 – Urine oxalate, NH4 and pH at 6, 12 and 18 weeks.
Figure 3 – Urine volume, sodium and potassium at 6, 12 and 18 weeks.
Figure 4 – Urine supersaturation of calcium phosphate and calcium oxalate at 6, 12 and 18 weeks.
Translational Statement.
Calcium oxalate (CaOx) stones are the most common kidney stone formed by humans, most of whom have idiopathic hypercalciuria (IH) and reduced bone density. To model human IH we generated the genetic hypercalciuric stone-forming (GHS) rats, which form solely CaOx stones when fed hydroxyproline. In humans, both potassium citrate and thiazide diuretics individually decrease stone formation; however, there is little data comparing these medications in combination. In GHS rats, the combination of potassium citrate and a thiazide prevented CaOx stone formation better than either agent alone. CTD alone improved bone quality, adding KCit provides no additional benefit for bone.
ACKNOWLEDGMENTS
This work was supported by Grant RO1 DK075462 from the National Institutes of Health to D.A.B.
DISCLOSURE
The authors have no competing financial interests. Dr. Krieger reports grants from National Institutes of Health, during the conduct of the study; and stock, stock options, spouse is a consultant for Tricida; stock from Amgen; spouse consults and receives speaking fees from Sanofi/Genzyme; spouse is a consultant for Relypsa/Vifor/Fresenius; spouse is an adjudicator for adverse events from Novo Nordisk/Covance. Dr. Bushinsky reports personal fees and other from Tricida, personal fees and other from Amgen, personal fees from Relypsa,Vifor/Fresenius, personal fees and other from Sanofi/Genzyme, outside the submitted work. All other authors have nothing to disclose.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Supplementary information is available on Kidney International’s website.
REFERENCES
- 1.Bose A, Monk RD, Bushinsky DA. Kidney stones. In: Melmed S, Polonsky KS, Larsen PR, Kronenberg HM (eds). Williams Textbook of Endocrinology, 13 edn. Elsevier: Philadelphia, 2016, pp 1365–1384. [Google Scholar]
- 2.Coe FL, Worcester EM, Evan AP. Idiopathic hypercalciuria and formation of calcium renal stones. Nat Rev Nephrol 2016; 12: 519–533. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bushinsky DA, Frick KK, Nehrke K. Genetic hypercalciuric stone-forming rats. Curr Opinion Nephrol Hyperten 2006; 15: 403–418. [DOI] [PubMed] [Google Scholar]
- 4.Bushinsky DA, Parker WR, Asplin JR. Calcium phosphate supersaturation regulates stone formation in genetic hypercalciuric stone-forming rats. Kidney international 2000; 57: 550–560. [DOI] [PubMed] [Google Scholar]
- 5.Li XQ, Tembe V, Horwitz GM, et al. Increased intestinal vitamin D receptor in genetic hypercalciuric rats. A cause of intestinal calcium hyperabsorption. The Journal of clinical investigation 1993; 91: 661–667. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Tsuruoka S, Bushinsky DA, Schwartz GJ. Defective renal calcium reabsorption in genetic hypercalciuric rats. Kidney international 1997; 51: 1540–1547. [DOI] [PubMed] [Google Scholar]
- 7.Krieger NS, Stathopoulos VM, Bushinsky DA. Increased sensitivity to 1,25(OH)2D3 in bone from genetic hypercalciuric rats. Am J Physiol (Cell Physiol) 1996; 271: C130–C135. [DOI] [PubMed] [Google Scholar]
- 8.Grynpas M, Waldman S, Holmyard D, et al. Genetic hypercalciuric stone-forming rats have a primary decrease in BMD and strength. Journal of bone and mineral research 2009; 24: 1420–1426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ng AH, Frick KK. Krieger NS, Asplin JR, Cohen-McFarlane M. Culbertson CD, Kyker-Snowman K, Grynpas MD, Bushinsky DA. 1,25(OH)2D3-enhanced hypercalciuria in genetic hypercalciuric stone-forming rats. Calc Tiss Int 2014; 94: 531–543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bushinsky DA, Asplin JR, Grynpas MD, et al. Calcium oxalate stone formation in genetic hypercalciuric stone-forming rats. Kidney international 2002; 61: 975–987. [DOI] [PubMed] [Google Scholar]
- 11.Karnauskas AJ, van Leeuwen JP, van den Bemd GJ, et al. Mechanism and function of high vitamin D receptor levels in genetic hypercalciuric stone-forming rats. Journal of Bone and Mineral Research 2005; 20: 447–454. [DOI] [PubMed] [Google Scholar]
- 12.Hoopes RR Jr., Middleton FA, Sen S, et al. Isolation and confirmation of a calcium excretion quantitative trait locus on chromosome 1 in genetic hypercalciuric stone-forming congenic rats. Journal of the American Society of Nephrology 2006; 17: 1292–1304. [DOI] [PubMed] [Google Scholar]
- 13.Moe OW, Bushinsky DA. Genetic Hypercalciuria: A Major Risk Factor in Kidney Stones. In: Thakker RV, Whyte MP, Eisman JA, Igarashi T (eds). Genetics of Bone Biology and Skeletal Disease. Elsevier: London, UK, 2013, pp 585–604. [Google Scholar]
- 14.Zisman AL. Effectiveness of treatment modalities on kidney stone recurrence. Clin J Am Soc Nephrol 2017; 12: 1699–1708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Fink HA, Wilt TJ, Eidman KE, et al. Medical management to prevent recurrent nephrolithiasis in adults: A systematic review for an american college of physicians clinical guideline. Annals of Internal Medicine 2013; 158: 535–543. [DOI] [PubMed] [Google Scholar]
- 16.Bushinsky DA, Asplin JR. Thiazides reduce brushite, but not calcium oxalate, supersaturation and stone formation in genetic hypercalciuric stone-forming rats. Journal of the American Society of Nephrology 2005; 16: 417–424. [DOI] [PubMed] [Google Scholar]
- 17.Bushinsky DA, Willett T, Asplin JR, et al. Chlorthalidone improves vertebral bone quality in genetic hypercalciuric stone-forming rats. Journal of Bone and Mineral Research 2011; 26: 1904–1912. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Krieger NS, Asplin JR, Frick KK, et al. Effect of potassium citrate on calcium phosphate stones in a model of hypercalciuria. Journal of the American Society of Nephrology 2015; 26: 3001–3008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Krieger NS, Asplin JR, Granja I, et al. Chlorthalidone Is superior to potassium citrate in reducing calcium phosphate stones and increasing bone quality in hypercalciuric stone-forming rats. Journal of the American Society of Nephrology 2019; 30: 1163–1173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Asplin JR, Bushinsky DA, Singharetnam W, et al. Relationship between supersaturation and crystal inhibition in hypercalciuric rats. Kidney international 1997; 51: 640–645. [DOI] [PubMed] [Google Scholar]
- 21.Asplin JR, Donahue SE, Lindeman C, et al. Thiosulfate reduces calcium phosphate nephrolithiasis. Journal of the American Society of Nephrology : JASN 2009; 20: 1246–1253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Frick KK, Asplin JR, Favus MJ, et al. Increased biological response to 1,25(OH)2D3 in genetic hypercalciuric stone-forming rats. Am J Physiol Renal Physiol 2013; 304: F718–726. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Frick KK, Asplin JR, Krieger NS, Culbertson CD, Asplin DM, Bushinsky DA. 1,25(OH)2D3-enhanced hypercalciuria in genetic hypercalciuric stone-forming rats fed a low calcium diet. Am J Physiol Renal Physiol 2013; 305: F1132–F1138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Werness PG, Brown CM, Smith LH, et al. Equil2: A BASIC computer program for the calculation of urinary saturation. The Journal of Urology 1985; 134: 1242–1244. [DOI] [PubMed] [Google Scholar]
- 25.Sakhaee K, Maalouf NM, Kumar R, et al. Nephrolithiasis-associated bone disease: pathogenesis and treatment options. Kidney international 2011; 79: 393–403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Moe OW, Pearle MS, Sakhaee K. Pharmacotherapy of urolithiasis: evidence from clinical trials. Kidney international 2011; 79: 385–392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Pak CY, Heller HJ, Pearle MS, et al. Prevention of stone formation and bone loss in absorptive hypercalciuria by combined dietary and pharmacological interventions. J Urol 2003; 169: 465–469. [DOI] [PubMed] [Google Scholar]
- 28.Sakhaee K, Williams RH, Oh MS, et al. Alkali absorption and citrate excretion in calcium nephrolithiasis. Journal of Bone and Mineral Research 1993; 8: 789–794. [DOI] [PubMed] [Google Scholar]
- 29.Bushinsky DA. Metabolic alkalosis decreases bone calcium efflux by suppressing osteoclasts and stimulating osteoblasts. AmJPhysiol(Renal Fluid Electrolyte Physiol40) 1996; 271: F216–F222. [DOI] [PubMed] [Google Scholar]
- 30.Coe FL, Parks JH, Bushinsky DA, et al. Chlorthalidone promotes mineral retention in patients with idiopathic hypercalciuria. Kidney international 1988; 33: 1140–1146. [DOI] [PubMed] [Google Scholar]
- 31.Bushinsky DA, Favus MJ, Coe FL. Mechanism of chronic hypocalciuria with chlorthalidone: reduced calcium absorption. AmJPhysiol(Renal Fluid Electrolyte Physioll6) 1984; 247: F746–F752. [DOI] [PubMed] [Google Scholar]
- 32.Rümenapf G, Schwille P. The influence of citrate on the duodenal absorption of calcium in the rat. Calc Tiss Int 1988; 42: 326–330. [DOI] [PubMed] [Google Scholar]
- 33.Ferraro PM, Ticinesi A, Meschi T, et al. Short-term changes in urinary relative supersaturation predict recurrence of kidney stones: A tool to guide preventive measures in urolithiasis. The Journal of Urology 2018; 200: 1082–1087. [DOI] [PubMed] [Google Scholar]
- 34.Prochaska M, Taylor E, Ferraro PM, et al. Relative Supersaturation of 24-Hour Urine and Likelihood of Kidney Stones. J Urol 2018; 199: 1262–1266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Bushinsky DA, Coe FL, Moe OW. Nephrolithiasis. In: Brenner BM (ed). The Kidney, 9 edn, vol. 2. W.B. Saunders: Philadelphia, 2012, pp 1455–1507. [Google Scholar]
- 36.Parfitt AM. The physiological and clinical significance of bone histomorphometric data. In: Recker R (ed). Bone Histomorphometry. Techniques and Interpretations. CRC Press: Boca Raton, 1983, pp 143–223. [Google Scholar]
- 37.Adams JS, Song CF, Kantorovich V. Rapid recovery of bone mass in hypercalciuric, osteoporotic men treated with hydrochlorothiazide. Ann Intern Med 1999; 130: 658–660. [DOI] [PubMed] [Google Scholar]
- 38.Steiniche T, Mosekilde L, Christensen MS, et al. Histomorphometric analysis of bone in idiopathic hypercalciuria before and after treatment with thiazide. APMIS 1989; 97: 302–308. [DOI] [PubMed] [Google Scholar]
- 39.Aung K, Htay T. Thiazide diuretics and the risk of hip fracture. Cochrane Database of Systematic Reviews 2011: CD005185. [DOI] [PubMed] [Google Scholar]
- 40.Pak CYC, Peterson RD, Poindexter J. Prevention of spinal bone loss by potassium citrate in cases of calcium urolithiasis. The Journal of Urology 2002; 168: 31–34. [PubMed] [Google Scholar]
- 41.Vescini F, Buffa A, LaManna G, et al. Long-term potassium citrate therapy and bone mineral density in idopathic calcium stone formers. J Endocrinol Invest 2005; 28: 218–222. [DOI] [PubMed] [Google Scholar]
- 42.Alshara L, Batagello CA, Armanyous S, et al. The impact of thiazides and potassium citrate on bone mineral density evaluated by CT scan in stone formers. Journal of Endourology 2018; 32: 559–564. [DOI] [PubMed] [Google Scholar]
- 43.Jehle S, Hulter HN, Krapf R. Effect of potassium citrate on bone Density, microarchitecture, and fracture risk in healthy older adults without osteoporosis: A randomized controlled trial. The Journal of Clinical Endocrinology & Metabolism 2013; 98: 207–217. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure 1 – Urine calcium, citrate and phosphate at 6, 12 and 18 weeks.
Figure 2 – Urine oxalate, NH4 and pH at 6, 12 and 18 weeks.
Figure 3 – Urine volume, sodium and potassium at 6, 12 and 18 weeks.
Figure 4 – Urine supersaturation of calcium phosphate and calcium oxalate at 6, 12 and 18 weeks.