

Abstract
Objective.
Sobriety checkpoints have strong empirical and theoretical support as an intervention to reduce alcohol-involved motor vehicle crashes. The purpose of this study was to examine whether checkpoint size (the number of police officers) and checkpoint duration (the amount of time in operation) affect associations between individual checkpoints and subsequent alcohol-related crash incidence.
Method.
Queensland Police Service provided latitude-longitude coordinates and date and time data for all breath tests that occurred in Brisbane, Australia, from January 2012 to June 2018. We applied hierarchical cluster analysis to the latitude-longitude coordinates for breath tests, identifying checkpoints as clusters of ≥ 25 breath tests conducted by ≥ 3 breath testing devices over a duration of 3 to 8 hours. Generalized linear autoregressive moving average (GLARMA) models related counts of alcohol-involved motor vehicle crashes to the number of checkpoints conducted per week, as well as 1 week prior and 2 weeks prior.
Results.
A total of 3,420 alcohol-related crashes occurred and 2,069 checkpoints were conducted in Brisbane over the 6.5-year (339-week) study period. On average, checkpoints included a mean of 266.0 breath tests (SD=216.3), 16.4 devices (SD=13.7), and were 286.3 minutes duration (SD=104.2). Each 10 additional checkpoints were associated with a 12% decrease in crash incidence at a lag of 1 week (IRR=0.88; 95%CI: 0.80,0.97). We detected no differential associations according to checkpoint size or duration.
Conclusions.
Sobriety checkpoints are associated with fewer alcohol-related motor vehicle crashes for around 1 week. Checkpoint size and duration do not appear to affect this relationship.
Keywords: alcohol, motor vehicle, crash, sobriety, checkpoint, police
Introduction
Road traffic crashes are a major contributor to the global burden of disease and injury. Approximately 1.35 million people die and a further 50 million are injured in crashes around the world each year. Road traffic crashes are the leading cause of death for young people aged 5 to 29 years (World Health Organization, 2018). Alcohol consumption is a leading contributor to crash incidence. Around 21.8% of fatal crashes globally are alcohol-involved, producing over 270,000 deaths each year (Vissers, Houwing, & Wegman, 2017). Preventive interventions to reduce the incidence of alcohol-involved crashes could therefore save many lives and avert millions of injuries each year around the world.
One universal prevention strategy to reduce alcohol-involved crashes that has a compelling theoretical foundation is sobriety checkpoints. In this intervention, a team of law enforcement officers establishes a roadside checkpoint at which passing drivers are stopped for a possible sobriety test. According to general deterrence theory, the approach affects crash incidence by raising the perceived risk of detection and arrest among all drivers within a population, which, in turn, increases the perceived individual costs of drunk-driving, leading to fewer people choosing to drive after drinking (Homel, 1993). Additional specific deterrent effects against drunk driving apply to the people who pass through the checkpoint; however, the proportion of all drivers who are tested at sobriety checkpoints and the arrest rates among those who are tested are very low (Voas, 2008), so specific deterrent effects are likely to be minimal (Watson & Freeman, 2007).
Sobriety checkpoints have very strong empirical support from studies around the world as a cost-effective and high-impact intervention to reduce alcohol-involved motor vehicle crashes (Community Preventive Services Task, 2014; Miller, Galbraith, & Lawrence, 1998). Multiple published reviews (Bergen et al., 2014; Elder et al., 2002; Erke, Goldenbeld, & Vaa, 2009; Shults et al., 2001) have concluded that crash rates are at least 8% lower in jurisdictions that use sobriety checkpoints compared to those that do not. These associations have been observed at a wide range of spatial scales—including within 2-mile buffers of checkpoint locations (Nunn & Newby, 2011), within cities (Voas, 2008), within counties (Lacey, Ferguson, Kelley-Baker, & Rider, 2006), and within states (Lacey & Jones, 2000)—and have been shown to be dose-responsive, in that programs that conduct more frequent checkpoints have greater reductions in crashes (Bergen et al., 2014). In addition to these studies that assess global associations for overall checkpoint programs, our previous analysis identified that individual checkpoint sites (couched within an overall program) are associated with reductions in alcohol-involved motor vehicle crashes for around one week (Morrison, Ferris, Wiebe, Peek-Asa, & Branas, 2019). In the absence of experimental research, observational studies provide convincing evidence that sobriety checkpoints are likely to be causally related to fewer subsequent crashes (National Academies of Sciences & Medicine, 2018). Rather than reproducing these many prior analyses, the imperative for research is now to identify optimal checkpoint configurations that maximize public health benefits while minimizing costs (Bergen et al., 2014). Such evidence will encourage and enable more law enforcement agencies around the world to use the intervention, thereby preventing more alcohol-involved crashes and reducing the global health burden.
The aim of this study is to assess the impact of sobriety checkpoint site configuration on alcohol-involved motor vehicle crash incidence. We selected the Australian state of Queensland as a study location because the Queensland Police Service has one of the most comprehensive sobriety checkpoint programs in the world, which included a process goal of achieving a ratio of one breath test per licensed driver in the state each year (Ferris et al., 2013). Queensland Police Service operates a program of random breath testing, which is a variant of sobriety checkpoints in which drivers can be stopped and subjected to a breath test without suspicion that they have been drinking. Full and highly resolved space-time data were available for all breath tests and all alcohol-involved motor vehicle crashes in the state, enabling assessment of the associations of interest at fine geographic and temporal scale. We focused on two elements of checkpoint configurations that are modifiable and important contributors to the total economic costs of checkpoint implementation: the duration that checkpoint sites are in operation, and the number of police officers involved.
Method
Study Design
The study setting was the greater metropolitan area around Brisbane, which is the capital city of the state of Queensland in Australia’s north east. We defined the geographic extent for the study based on population density because sobriety checkpoints are likely to affect alcohol-impaired driving and crashing across a full metropolitan region. Using administrative bounds, such as the Brisbane city limits, could introduce boundary effects (and resultant attenuation of parameter estimates) due to checkpoints and crashes occurring within the functional metropolitan area but outside these administrative borders. Therefore, consistent with our previous analyses (Morrison, 2015), we included Statistical Area level 1 (SA1) units from the 2016 Australian census units with population density of 50 people/km2 or that had a total land area smaller than 5 km2. We also included any SA1 units that were not selected using these criteria but were wholly surrounded by selected SA1 units. The internal SA1 boundaries were then dissolved, yielding a single polygon that had a population at the 2016 census of 2,138,033 and a total land area of 3,046.6 km2. For this time series analysis, all data for Brisbane were aggregated as weeks from 5:00am Tuesday to 4:59am on the following Tuesday, because this time typically has very low activity for sobriety checkpoints and alcohol-involved motor vehicle crashes (NHTSA, 2011). The full time series was 339 weeks beginning at 5:00am Tuesday January 3, 2012 and ending at 4:59am Tuesday June 26, 2018.
Dependent Measure
The dependent measure was a count of alcohol-involved motor vehicle crashes per week, calculated using a publicly available registry of motor vehicle crashes from the Queensland Department of Transport and Main Roads. Available crash-level data include the latitude, longitude, date, time, and an indicator of alcohol involvement, recorded when a driver, pedestrian, or cyclists involved in a crash is positive for any alcohol according to a roadside breath test, fixed site breath test, or a laboratory blood or saliva test. We aggregated alcohol-involved motor vehicle crashes as counts per week of all motor vehicle crashes that (i) occurred on a public road in Brisbane, (ii) caused a fatality or injury that required medical treatment or caused ≥ $A2,500 property damage, and (iii) included alcohol as a contributing factor.
The denominator was the size of the residential population of Brisbane per week. The Australian Census Bureau provides annual estimates of the total population per SA1 for June 30 each year. The sum of these values across all SA1s provided the annual population for Brisbane, and we linearly interpolated these values to estimate the total population per week.
Checkpoints
Queensland Police Service operates a comprehensive program of random roadside breath testing, including checkpoints in which police stationed at temporary sites systematically stop drivers to conduct sobriety checks. Breath testing devices automatically record a date and time stamp for each test. An embedded Global Positioning System (GPS) records a single pair of latitude and longitude coordinates each time the device is activated and the officer specifies that the testing is part of a stationary checkpoint, otherwise a new pair of coordinates is generated for every test. We accessed data for individual breath tests conducted between January 3, 2012, and June 26, 2018.
Hierarchical cluster analyses identified checkpoints within the breath test data. First, the latitude and longitude coordinates for each breath test were converted into X and Y values for a projected coordinate system (GDA_1994_BCSG02; WKID: 3113; Units: Meters). We then conducted complete linkage cluster analyses using data for each 24-hour period (5:00am to 4:59am) and grouped breath tests that were within 100 meters. To exclude breath tests that occurred at the same coordinates as a checkpoint but outside the hours that checkpoints were in operation (e.g., during regular traffic stops), we defined checkpoints as groups of breath tests that were within 3 standard deviations of the mean time for tests conducted within a cluster. Based on consultations with operations personnel from the Queensland Police Service, we defined checkpoints as groups of breath tests that were between 180- and 640-minutes duration, used ≥ 3 breath testing devices, and included ≥ 25 tests. This procedure thus identified clusters of breath tests in space and time. Figure 1 shows an example of the five checkpoints that were identified in a single 24-hour period, from 5:00am December 21, 2017, to 4:59am December 22, 2017. Manual checks against police operations logs confirmed that a random sample of 10 space-time clusters of breath tests corresponded with checkpoint activity at the identified dates and times.
Figure 1.
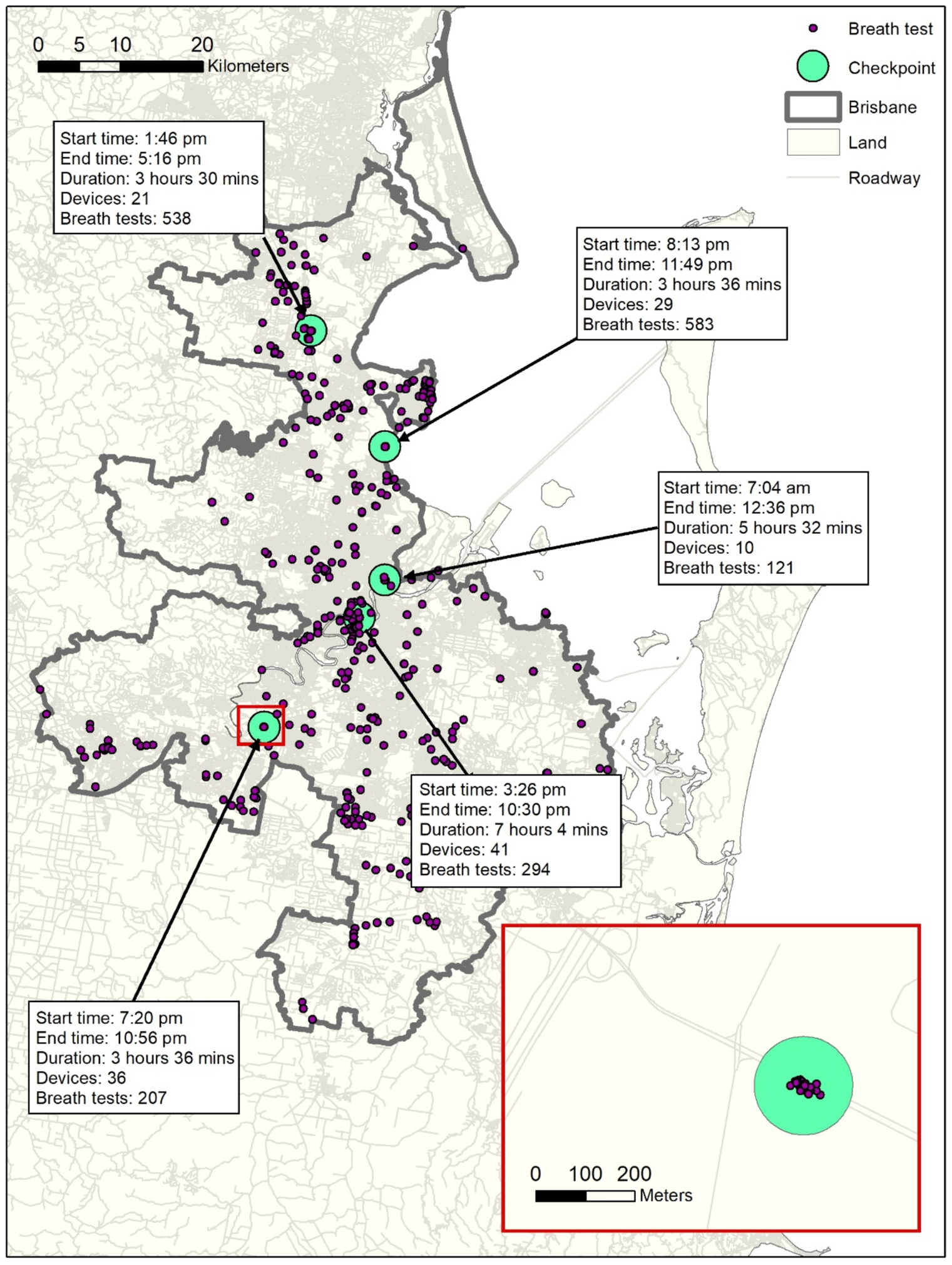
Breath tests (n = 3,673) conducted between 5:00am on Thursday December 21, 2017 and 4:59am on Friday December 22, 2017. Checkpoints (n = 5) identified among breath tests based on complete linkage hierarchical cluster analysis with cut points at 100 meters.
Each checkpoint site was characterized according to the two theoretically relevant elements that affect law enforcement resources. Duration was calculated as the time elapsed between the first breath test and the last breath test in the checkpoint. The number of devices (a proxy for the number of officers present) was calculated as a count of the number of unique latitude and longitude coordinate pairs. We further categorized checkpoints based on the duration and size. Checkpoints that took 180–300 minutes were defined as “short” checkpoints, while those taking 300–640 minutes were defined as “long” checkpoints. Small checkpoints had 3–10 devices, and large checkpoints had more than 10 devices. We also calculated the number of tests conducted within each checkpoint as a count of the total number of breath test readings.
Covariates
Time-varying characteristics that are causally related to alcohol-involved crash incidence and are associated with checkpoint implementation may confound associations between checkpoints and alcohol-involved crashes. We measured the total rainfall, the number of days with rain, and the average maximum temperature per week using data from the Australian Government Bureau of Meteorology. The Queensland government provided counts of the number of holidays per week. We also coded dummy variables for Australian seasons (Spring, Summer, Autumn, and Winter).
Statistical Analysis
Generalized Linear Autoregressive Moving Average (GLARMA) models assessed associations between checkpoints and the alcohol-involved crash rate defined as the number of alcohol-involved crashes per 1 million population per week. The GLARMA models here accommodate time series of alcohol-involved crash counts that are assumed to follow a Poisson distribution:
Where Ct is a count of crashes at time t and Pt is the time varying population size for Brisbane. The term ut is the log of the crash incidence rate, which we modelled linearly:
α0 is a constant term. Parameters γb measure associations between counts of checkpoints (CP) at temporal lags of b = 0, b = 1, and b = 2 weeks. Parameters β measure associations for time varying covariates X*, which were the average rainfall, the number of days with rain in a week, the average maximal temperature, the number of holidays, and the Australian season (Spring, Summer, Autumn, and Winter). Covariates were not temporally lagged.
Temporal trends were captured in terms T, T2, and the trigonometric function:
The error term Zt accounted for temporal autocorrelation with an AR(4) correlation structure (et is a scaled residual):
We fitted six variants of this model. Model 1 considered the total number of all checkpoints at lag 0, lag 1 and lag 2. Model 2 added the average duration per checkpoint, the total number of devices per checkpoint, and the total number of breath tests per checkpoint at these temporal lags. The main independent measures in Models 3–6 were counts of short, long, small, and large checkpoints, respectively. We reported adjusted incidence rate ratios (RRs) and their 95% confidence intervals (CIs). The analysis was conducted using the “glarma” package in R (Dunsmuir & Scott, 2015).
Note that Queensland Police Service targets operations to peak alcohol drinking times, such as the holiday season (Lloyd, Matthews, Livingston, Jayasekara, & Smith, 2013). Increased activity may correspond with increased temporary populations and may vary by location. Therefore, we expected relationships between checkpoints and alcohol-involved crashes to be positive at lag 0. After controlling for this confounder, the deterrent effect of checkpoints on alcohol-impaired driving during subsequent weeks will be captured in the associations at lag 1 and lag 2.
Results
In the 339 weeks between January 2012 and June 2018, there were 3,420 alcohol-involved motor vehicle crashes in Brisbane and Queensland Police Service conducted 5,654,715 breath tests. The hierarchical cluster analysis identified 2,069 checkpoints in which 550,415 (9.7%) of the breath tests were conducted. On average, there were 266.0 tests conducted per checkpoint (SD = 216.3). Checkpoints were an average of 286.3 minutes duration (SD = 261.3) and included 16.4 devices (SD = 13.7). Table 1 is a two-by-two table showing the checkpoint distribution according to dichotomized duration and size.
Table 1.
Number of checkpoints according to duration and size in Brisbane, January 3, 2012 to June 26, 2018; n = 2,069. Short checkpoints were 180 mins to 300 mins duration; large checkpoints were 300 mins to 640 mins duration. Small checkpoints had 3 to 10 devices; large checkpoints had > 10 devices.
| Short | Long | Total | |
|---|---|---|---|
| Small | 552 | 366 | 918 |
| Large | 893 | 258 | 1,151 |
| Total | 1,445 | 624 | 2,069 |
The weekly number of crashes followed an increasing trend which tapered around 2015. The weekly number of checkpoints followed a decreasing trend over time which also tapered around 2015 (Figure 2). Table 2 shows the descriptive statistics of all variables of interest in this analysis. On average, there were 10 crashes (SD = 3.5) and 6.3 checkpoints (SD = 3.9) per week, including 4.4 short checkpoints (SD = 3.3) and 1.9 long checkpoints (SD = 1.6); and 2.8 small checkpoints (SD = 1.9), and 3.5 large checkpoints (SD = 3.0). After aggregating within weeks, there was an average of 15.0 devices per checkpoint (SD = 6.9) and 241.8 tests per checkpoint (SD = 130.1), and checkpoints lasted an average of 292.9 minutes (SD = 65.5).
Figure 2.
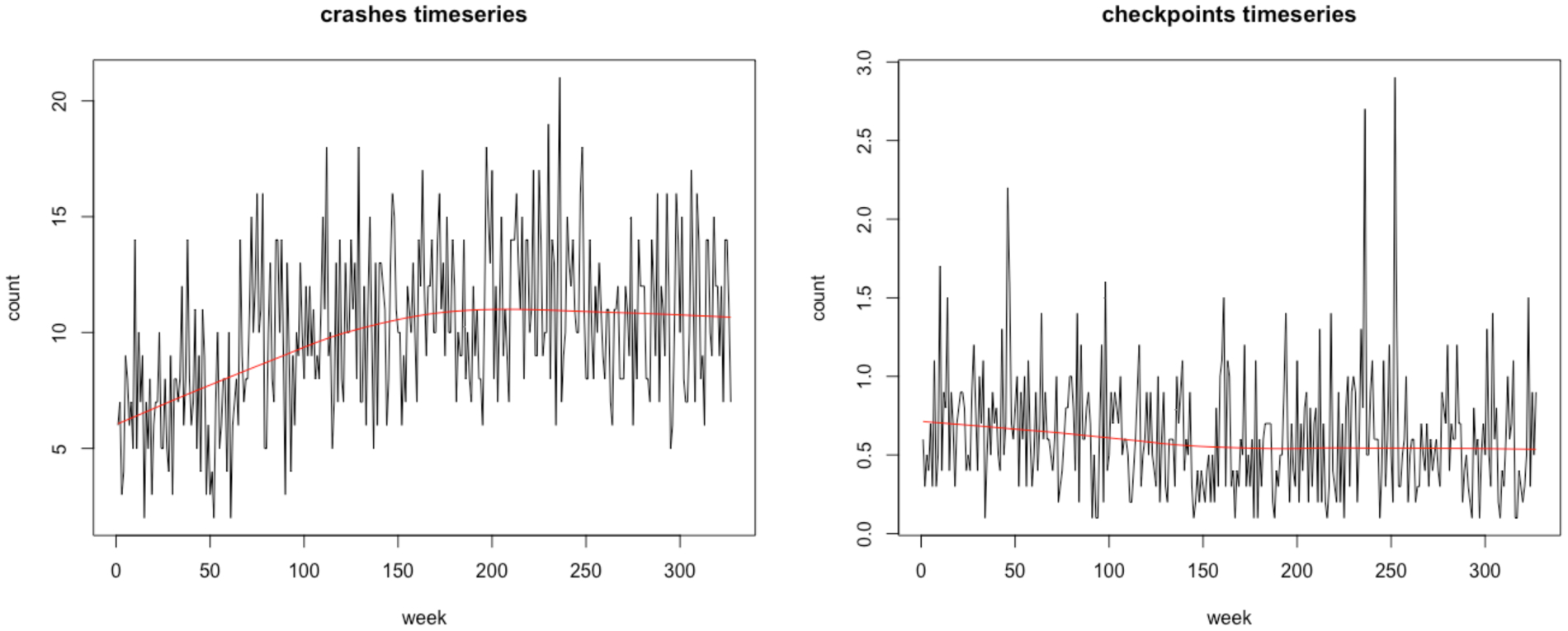
Trend in the number of crashes (left) and in the number of all checkpoints (right) for Brisbane (n = 339). Week 0 corresponds to the first week of 2012
Table 2.
Descriptive statistics for alcohol-involved motor vehicle crashes per week, checkpoints per week, and time varying covariates per week; Brisbane, Australia (n = 339 weeks)
| Variable | Mean | SD | Min | Median | Max |
|---|---|---|---|---|---|
| Dependent Variable | |||||
| Alcohol-Involved Crashes | 10.04 | 3.49 | 2.00 | 10.00 | 21.00 |
| Checkpoints | |||||
| Checkpoints (count) | 6.27 | 3.88 | 1.00 | 6.00 | 29.00 |
| Short checkpoints (180–300 minutes) | 4.39 | 3.29 | 0.00 | 4.00 | 24.00 |
| Long checkpoints (300–640 minutes) | 1.87 | 1.57 | 0.00 | 2.00 | 9.00 |
| Small checkpoints (3–10 devices) | 2.77 | 1.93 | 0.00 | 3.00 | 13.00 |
| Large checkpoints (≥10 devices) | 3.49 | 3.03 | 0.00 | 3.00 | 21.00 |
| Weekday checkpoints (Monday, Tuesday, Wednesday, Thursday) | 3.07 | 2.03 | 0.00 | 3.00 | 9.00 |
| Weekend checkpoints (Friday, Saturday, Sunday) | 3.20 | 3.02 | 0.00 | 3.00 | 24.00 |
| Devices per checkpoint (count) | 15.00 | 6.92 | 3.00 | 13.86 | 38.00 |
| Tests per checkpoint (count) | 241.77 | 130.12 | 27.00 | 229.38 | 715.00 |
| Tests not in checkpoints (count) | 11,763.70 | 4,973.60 | 1,120.00 | 11,427.00 | 28,507.00 |
| Checkpoint duration | 292.88 | 65.49 | 187.00 | 280.00 | 592.00 |
| Covariates | |||||
| Number of holidays (count) | 0.24 | 0.65 | 0.00 | 0.00 | 4.00 |
| Precipitation (millimeters) | 2.76 | 5.46 | 0.00 | 0.77 | 36.29 |
| Days with precipitation | 2.45 | 1.89 | 0.00 | 2.00 | 7.00 |
| Mean temperature (degrees Celsius) | 26.82 | 3.40 | 18.64 | 27.26 | 34.43 |
| Mean interpolated population (million) | 2.18 | 0.07 | 2.05 | 2.18 | 2.32 |
Table 3 shows the results of the GLARMA models. In Model 1, a 10-unit increase in the number of checkpoints per week had a weak association with the alcohol-involved crash rate for the one week later (RRlag1 = 0.92; 95% CI: 0.84, 1.01) and the association was slightly attenuated two weeks later, though the 95% confidence intervals overlapped substantially (RRlag2 = 0.96; 95% CI: 0.87, 1.05). In Model 2, after adjusting for the total number of devices per checkpoints, the total number of tests per checkpoints, and the average duration per checkpoint, a 10-unit increase in the number of all checkpoints per week was associated with a 12% decrease in the alcohol-involved crash rate for the following week (RRlag1 = 0.88; 95% CI:0.80, 0.97). In Models 3 to 6, associations remained comparably weak but in the expected direction for short, long, small, and large checkpoints. In all models except Model 6 (large checkpoints only), associations were attenuated at a lag of 2 weeks compared to a lag of 1 week.
Table 3.
Results (Rate Ratios and 95% CIs) of Generalized Linear Autoregressive Moving Average (GLARMA) models for counts of alcohol-involved motor vehicle crashes per 1 million population; Brisbane, Australia (n = 339 weeks).
| Model 1: All |
Model 2: All |
Model 3: Short only |
Model 4: Long only |
Model 5: Small only |
Model 6: Large only |
|
|---|---|---|---|---|---|---|
| Lag 0 | ||||||
| Checkpoints* | 1.15 (1.05,1.25) | 1.23 (1.12,1.36) | 1.12 (1.01,1.24) | 1.41 (1.12,1.77) | 1.48 (1.23,1.79) | 1.09 (0.97,1.22) |
| Duration per checkpoint** | 1.02 (0.99,1.06) | |||||
| Devices per checkpoint | 0.99 (0.98,1.00) | |||||
| Tests per checkpoint*** | 1.00 (0.96,1.03) | |||||
| Lag 1 | ||||||
| Checkpoints* | 0.92 (0.84,1.01) | 0.88 (0.80,0.97) | 0.92 (0.83,1.03) | 0.85 (0.67,1.07) | 0.84 (0.69,1.01) | 0.94 (0.83,1.06) |
| Duration per checkpoint** | 1.01 (0.97,1.05) | |||||
| Devices per checkpoint | 1.00 (1.00,1.01) | |||||
| Tests per checkpoint*** | 1.02 (0.99,1.06) | |||||
| Lag 2 | ||||||
| Checkpoints* | 0.96 (0.87,1.05) | 0.95 (0.86,1.05) | 0.93 (0.84,1.04) | 1.05 (0.84,1.31) | 1.00 (0.83,1.21) | 0.93 (0.83,1.05) |
| Duration per checkpoint** | 1.01 (0.98,1.05) | |||||
| Devices per checkpoint | 1.00 (0.99,1.00) | |||||
| Tests per checkpoint*** | 1.02 (0.98,1.05) | |||||
| Covariates (Lag 0) | ||||||
| Number of Holidays | 1.00 (0.95,1.06) | 0.99 (0.94,1.05) | 1.01 (0.96,1.07) | 0.99 (0.93,1.04) | 0.98 (0.92,1.03) | 1.01 (0.96,1.07) |
| Precipitation | 1.06 (0.98,1.14) | 1.04 (0.97,1.13) | 1.06 (0.98,1.14) | 1.05 (0.97,1.13) | 1.06 (0.99,1.15) | 1.05 (0.98,1.14) |
| Days with Precipitation | 1.01 (0.99,1.03) | 1.01 (0.99,1.04) | 1.01 (0.98,1.03) | 1.01 (0.99,1.03) | 1.01 (0.98,1.03) | 1.01 (0.99,1.03) |
| Mean Temperature | 1.00 (0.98,1.02) | 1.00 (0.98,1.02) | 1.00 (0.98,1.02) | 1.00 (0.98,1.02) | 1.00 (0.98,1.02) | 1.00 (0.98,1.02) |
| Season+ | ||||||
| Spring | 1.01 (0.91,1.12) | 1.01 (0.92,1.12) | 1.01 (0.91,1.11) | 1.01 (0.91,1.12) | 1.00 (0.90,1.11) | 1.01 (0.92,1.12) |
| Summer | 0.93 (0.82,1.05) | 0.93 (0.82,1.05) | 0.93 (0.83,1.05) | 0.93 (0.82,1.05) | 0.93 (0.82,1.05) | 0.94 (0.83,1.06) |
| Winter | 1.06 (0.93,1.20) | 1.06 (0.93,1.21) | 1.06 (0.93,1.20) | 1.05 (0.93,1.20) | 1.06 (0.93,1.21) | 1.06 (0.93,1.2) |
| Week | 1.69 (1.45,1.97) | 1.61 (1.37,1.88) | 1.68 (1.45,1.95) | 1.70 (1.46,1.99) | 1.69 (1.45,1.97) | 1.67 (1.44,1.94) |
| Week Squared | 0.65 (0.56,0.76) | 0.69 (0.59,0.81) | 0.66 (0.57,0.76) | 0.65 (0.56,0.75) | 0.66 (0.57,0.76) | 0.66 (0.57,0.76) |
| Annual Cosine | 0.98 (0.93,1.04) | 0.99 (0.93,1.04) | 0.98 (0.94,1.04) | 0.99 (0.94,1.04) | 0.99 (0.94,1.04) | 0.98 (0.94,1.04) |
| Annual Sine | 1.01 (0.95,1.06) | 1.00 (0.95,1.06) | 1.01 (0.96,1.06) | 1.00 (0.95,1.05) | 1.00 (0.95,1.06) | 1.01 (0.96,1.06) |
checkpoints were scaled by 10.
duration was scaled by 10 minutes.
tests were scaled by 100.
Autumn is the reference season
Checkpoints in the current week (lag 0) were associated with additional alcohol-involved crashes. For example, all checkpoints were associated with a 15% increase in the alcohol-involved crash rate for the current week (RRlag0 = 1.15; 95% CI: 1.05, 1.25). In Model 2, an additional 10 devices per checkpoint per week was also associated with a 1% decrease in the alcohol-involved crash rate for the same week (RRlag0 = 0.99; 95% CI: 0.99, 1.00). All covariates were not associated with the alcohol-involved crash rate, except for a quadratic association for time (i.e., for week and week-squared).
Discussion
Theory and empirical studies provide strong evidence that sobriety checkpoints are causally related to fewer alcohol-involved motor vehicle crashes (Bergen et al., 2014; Elder et al., 2002; Erke et al., 2009; Shults et al., 2001). Research efforts are now required to identify the optimal configuration of individual checkpoints within an overall program to balance public health benefits while minimizing costs to law enforcement (Bergen et al., 2014). This analysis of sobriety checkpoints conducted by the Queensland Police Service identified that checkpoints are associated with fewer alcohol-involved crashes for approximately one week, and that there was no detectable difference in associations based on two key modifiable features of checkpoint sites—their duration and size. This research accords with previous studies of sobriety checkpoints and alcohol involved crashes. In addition to confirming the abundant published analyses demonstrating that checkpoints are generally associated with fewer alcohol-involved crashes (National Academies of Sciences & Medicine, 2018), this work also corroborates Stuster and Blower’s finding in six California communities that smaller checkpoints staffed by 3 to 5 officers had similar effect sizes compared to larger checkpoints staffed by 8 to 12 officers (Stuster & Blowers, 1995). Further, the temporal extent over which we observed associations in Brisbane is also consistent with our previous work in Los Angeles, California, where we identified individual sobriety checkpoints were associated with fewer subsequent alcohol-involved crashed over periods of approximately one week (Morrison et al., 2019). Prior studies (Morrison et al., 2019; Stuster & Blowers, 1995) detected no such relationships for saturation patrols (i.e. heightened police activity in a specified area without a dedicated checkpoint site; Fell, Lacey, & Voas, 2004). This collective evidence suggests that individual sobriety checkpoints are associated with fewer alcohol-involved crashes for approximately one week and that checkpoint duration and size do not affect these associations, but that having physical and observable checkpoint sites is an important element of the intervention design.
The findings of the current study are mostly consistent with general deterrence theory. According to this theory, the causal mechanism through which sobriety checkpoints affect drunk driving and alcohol-involved crashing is through increased perceived risks of detection and punishment for all drivers within a population at subsequent times, not just those who are caught offending while the checkpoint is in operation (Homel, 1993). Thus, the most important feature of a checkpoint is the number of people who are aware of its presence. Larger checkpoints with more officers testing more drivers will theoretically have the same impact as smaller checkpoints with fewer officers testing fewer drivers, provided the same number of motorists drive past or otherwise become aware of its presence. For that reason, longer checkpoints will theoretically have stronger effects than shorter checkpoints, although we did not detect such an association. It is possible that other checkpoint features not assessed here, such as accompanying advertising (e.g. marketing blitzes), are more important contributors to checkpoint effectiveness than the precise size and duration of each site (Saltz, Paschall, & O’Hara, 2021).
This work has important implications for law enforcement resources and public health. Police officers identify several important impediments to implementing sobriety checkpoint programs, including boredom, perceived risks for officers, perceived ineffectiveness, and economic constraints (Ross, 1993). Our results suggest it may be possible to reduce the human and financial costs associated with checkpoints by reducing checkpoint duration and size. Smaller, shorter checkpoints with fewer officers involved will reduce operational costs because they require fewer officer-hours.
As expected, we detected strong positive associations between counts of checkpoints and the incidence of alcohol-involved crashes during the same week (lag 0). This association underscores a key limitation of using an observational study design to relate checkpoints to crashes. Queensland Police Service has intimate local knowledge, decades of experience, and large volumes of driver impairment data to guide operational decisions about where and when to locate sobriety checkpoints. Systematically conducting checkpoints during weeks when drivers are more likely to be impaired is an important component of this preventive intervention (Community Preventive Services Task, 2014), but, from a research perspective, it also introduces endogeneity that manifests as a positive statistical association. Identifying the immediate deterrent effect of checkpoints on crashes during the same week requires an experimental design in which checkpoints are randomly distributed across time.
Other limitations may have affected these results. First, we did not have access to direct measures of checkpoint sites (day, time, duration, size, tests); rather we reverse engineered these measures using a hierarchical cluster analysis based on space-time data for individual breath tests. The identification of checkpoint sites appears to have criterion validity when compared to Queensland Police Service’s qualitative operations logs, but we were not able to assess validity quantitatively. Further, the number of unique latitude-longitude coordinates as a proxy measure for the number of officers present may be non-differentially misclassified and could inflate standard errors. Other misclassification could bias results in either direction. Additionally, the observational design critically limits our ability to assert that weeks are exchangeable units. We controlled statistically for Queensland Police Service differentially choosing to hold checkpoints during weeks when drunk driving and alcohol-involved crash incidence is greater, which will also account for systematic negative autocorrelation when high risk weeks are followed by low risk weeks. However, there may be other unmeasured confounders that affect these analyses and impede causal inference.
Conclusion
Comprehensive approaches to reducing alcohol-involved harms use a broad range of evidence-based strategies (Babor et al., 2010). Sobriety checkpoints are universal prevention strategy with a clear theoretical basis and strong empirical support as an intervention to reduce alcohol-involved crashes (Bergen et al., 2014; Elder et al., 2002; Erke et al., 2009; Shults et al., 2001). The intervention complements other evidence-based strategies, and should be part of a comprehensive approach to reduce the burden due to alcohol-involved crashes (National Academies of Sciences & Medicine, 2018). This analysis adds that individual checkpoints are associated with fewer alcohol-involved motor vehicle crashes for approximately one week, and that less resource intensive checkpoints of shorter duration and with fewer officers may achieve comparable public health benefits while reducing costs to law enforcement.
Funding:
Research reported in this publication was supported by the National Institute on Alcohol Abuse and Alcoholism of the National Institutes of Health under Award Number R21AA025749. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The authors wish to acknowledge the support and assistance from the Queensland Police Service in undertaking this research. The views expressed in this publication are not necessarily those of the Queensland Police Service and any errors of omission or commission are the responsibility of the authors.
Financial Disclosures: None.
References
- Babor T, Caetano R, Casswell S, Edwards G, Giesbrecht N, Graham K, Grube JW, Hill L, Holder H, Homel R, Livingston M, Österberg E, Rehm J, Room R, Rossow I. (2010). Alcohol: No Ordinary Commodity: Research and Public Policy: Oxford University Press. [Google Scholar]
- Bergen G, Pitan A, Qu S, Shults RA, Chattopadhyay SK, Elder RW, Sleet DA, Coleman HL, Compton RP, Nichols JL, Clymer JM, Calvert WB, Community Preventive Services Task Force (2014). Publicized sobriety checkpoint programs: a community guide systematic review. Am J Prev Med, 46(5), 529–539. doi: 10.1016/j.amepre.2014.01.018 [DOI] [PubMed] [Google Scholar]
- Community Preventive Services Task Forve. (2014). Publicized sobriety checkpoint programs to reduce alcohol-impaired driving: recommendation of the Community Preventive Services Task Force. Am J Prev Med, 46(5), 540–541. [DOI] [PubMed] [Google Scholar]
- Dunsmuir WTM, & Scott DJ (2015). The glarma package for observation-driven time series regression of counts. J Stat Softw, 67(7), 1–36. doi: 10.18637/jss.v067.i07 [DOI] [Google Scholar]
- Elder RW, Shults RA, Sleet DA, Nichols JL, Zaza S, & Thompson RS (2002). Effectiveness of sobriety checkpoints for reducing alcohol-involved crashes. Traffic Inj Prev, 3(4), 266–274. [Google Scholar]
- Erke A, Goldenbeld C, & Vaa T (2009). The effects of drink-driving checkpoints on crashes—A meta-analysis. Accident Anal Prev, 41(5), 914–923. [DOI] [PubMed] [Google Scholar]
- Fell JC, Lacey JH, & Voas RB (2004). Sobriety checkpoints: evidence of effectiveness is strong, but use is limited. Traffic Inj Prev, 5(3), 220–227. [DOI] [PubMed] [Google Scholar]
- Ferris J, Mazerolle L, King M, Bates L, Bennett S, & Devaney M (2013). Random breath testing in Queensland and Western Australia: Examination of how the random breath testing rate influences alcohol related traffic crash rates. Accident Anal Prev, 60, 181–188. [DOI] [PubMed] [Google Scholar]
- Homel R (1993). Drivers who drink and rational choice: Random breath testing and the process of deterrence. In: Routine Activity and Rational Choice: Advances in Criminological Theory, Clarke RV & Felson M (Eds.), 5, 59–84. [Google Scholar]
- Lacey JH, Ferguson SA, Kelley-Baker T, & Rider RP (2006). Low-manpower checkpoints: can they provide effective DUI enforcement in small communities? Traffic Inj Prev, 7(3), 213–218. [DOI] [PubMed] [Google Scholar]
- Lacey JH, & Jones RK (2000). Evaluation of New Mexico’s anti-DWI efforts. Washington, D.C.: US Department of Transportation. [Google Scholar]
- Lloyd B, Matthews S, Livingston M, Jayasekara H, & Smith K (2013). Alcohol intoxication in the context of major public holidays, sporting and social events: a time–series analysis in Melbourne, Australia, 2000–2009. Addiction, 108(4), 701–709. [DOI] [PubMed] [Google Scholar]
- Miller TR, Galbraith MS, & Lawrence BA (1998). Costs and benefits of a community sobriety checkpoint program. J Stud Alcohol Drugs, 59(4), 462–468. [DOI] [PubMed] [Google Scholar]
- Morrison C (2015). Exposure to alcohol outlets in rural towns. Alcohol Clin Exp Res, 39(1), 73–78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morrison CN, Ferris J, Wiebe DJ, Peek-Asa C, & Branas CC (2019). Sobriety checkpoints and alcohol-involved motor vehicle crashes at different temporal scales. Am J Prev Med, 56(6), 795–802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Academies of Sciences, Engineering & Medicine. (2018). Getting to Zero Alcohol-Impaired Driving Fatalities: A Comprehensive Approach to a Persistent Problem. Washington, DC: The National Academies Press. [PubMed] [Google Scholar]
- National Highway Traffic Safety Administration. (2011). Time of Day and Demographic Perspective of Fatal Alcohol-Impaired-Driving Crashes. DOT HS 811 523. Washington, DC: US Department of Transportation. [Google Scholar]
- Nunn S, & Newby W (2011). The geography of deterrence: exploring the small area effects of sobriety checkpoints on alcohol-impaired collision rates within a city. Eval Rev, 35(4), 354–378. [DOI] [PubMed] [Google Scholar]
- Ross HL (1993). Reasons for non-use of sobriety checkpoints. Police Chief, 59, 58–63. [Google Scholar]
- Saltz RF, Paschall MJ, & O’Hara SE (2021). Effects of a community-level intervention on alcohol-related motor vehicle crashes in California cities: A randomized trial. Am J Prev Med, 60(1):38–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shults RA, Elder RW, Sleet DA, Nichols JL, Alao MO, Carande-Kulis VG, Zaza S, Sosin DM, Thompson RS, Task Force on Community Preventive Services (2001). Reviews of evidence regarding interventions to reduce alcohol-impaired driving. Am J Prev Med, 21(4 Suppl), 66–88. [DOI] [PubMed] [Google Scholar]
- Stuster J, & Blowers P (1995). Experimental evaluation of sobriety checkpoint programs. HS 808 287. Washington, DC: US Department of Transportation. [Google Scholar]
- Vissers L, Houwing S, & Wegman F (2017). Alcohol-Related Road Casualties in Official Crash Statistics. Paris, France: International Transport Forum. [Google Scholar]
- Voas RB (2008). A new look at NHTSA’s evaluation of the 1984 charlottesville sobriety checkpoint program: implications for current checkpoint issues. Traffic Inj Prev, 9(1), 22–30. [DOI] [PubMed] [Google Scholar]
- Watson B, & Freeman J (2007). Perceptions and experiences of random breath testing in Queensland and the self-reported deterrent impact on drunk driving. Traffic Inj Prev, 8(1), 11–19. [DOI] [PubMed] [Google Scholar]
- World Health Organization. (2018). Global status report on road safety 2018. Geneva, Switzerland: WHO. [Google Scholar]