

Supplemental Digital Content is Available in the Text.
BACKGROUND
HARK is an FDA-approved flexible filler designed for lips.
OBJECTIVE
To quantitatively evaluate subject outcomes by measuring the change in lip texture, color (redness), lip fullness, and lip and perioral surface stretch (dynamic strain) after treatment.
METHODS AND MATERIALS
In this 8-week open-label, Phase IV multicenter study, subjects were treated with HARK in the lips and HARR and/or HARD in perioral wrinkles and folds as add-on treatment. Assessments included 2D photographic analyses of lip texture and color, and 3D photographic assessments of lip enhancement and dynamic strain.
RESULTS
HARK significantly improved lip texture (p ≤ .002), lip redness (p < .001), and added fullness to the lips (lip enhancement measurements; p < .001), at Week 8 after treatment. In addition, lower lip wrinkles were significantly reduced (p = .007) and there was a reduction in upper lip wrinkles (not statistically significant). Surface stretch (dynamic strain) in the lip and perioral region was significantly increased after treatment (p < .001).
CONCLUSION
This analysis provides an objective measure of the beneficial effects of flexible hyaluronic acid fillers in lip augmentation and perioral enhancement and demonstrates a significantly improved lip texture, red color, and fullness. A significant increase in surface stretch (dynamic strain) is indicative of tissue expansion and improvement in lip smoothness.
Lip proportions are believed to influence an aesthetically youthful appearance and lip augmentation is one of the most commonly requested aesthetic procedures.1,2 Three categories of patients seeking lip improvement have been described: those with pleasing lip shape who want more fullness, those with genetically thin lips and/or poor definition of the vermilion border, and those with atrophic lips and poor definition of the vermilion border because of advancing age.3 Aging can result in upper lip atrophy because of loss of fat tissue, which can be associated with a widening of the Cupid's bow, and loss of the natural lip “pout.”4,5
The overall objective of lip and perioral augmentation and aesthetic treatment should be a natural 3D improvement of lip volume with a well-defined vermilion border and improved texture, without compromising naturalness of lower facial expressions.5–9
Restylane Kysse (HARK), Restylane Refyne (HARR), and Restylane Defyne (HARD) are hyaluronic acid (HA) dermal fillers formulated with XpresHAn Technology (known as Optimal Balance Technology outside the US). These fillers achieve distributed tissue integration, and provide flexibility and support to maintain natural movement and dynamic expression.6,10–13 HARK, a filler specifically designed for lip augmentation, has been approved in various countries outside the US since 2010 and was recently FDA-approved.10,14 HARR and HARD are used as add-on treatments for subjects who also require nasolabial fold (NLF) or marionette line (ML) correction to optimize aesthetic results. The softer gel structure of HARR is best used for moderate wrinkles and folds, whereas the firmer texture of HARD is more suitable for correction of severe wrinkles and folds.11,15,16
Analog rating scales provide important feedback on the success of lip augmentation procedures but can be limited by their subjective nature. In this open-label Phase IV postmarketing study, objective photographic measures were used to evaluate HARK compared with baseline, with and without treatment for perioral wrinkles and folds with HARR or HARD. This article reports the objective assessment outcomes used to assess lip texture and redness, lip enhancement, and facial dynamics.
Materials and Methods
An open-label Phase IV postmarketing study (NCT03967444) was conducted between 29 May and 18 September 2019 at 3 investigational sites in Canada.
Subjects
The criteria for inclusion in the study were adult men and nonpregnant women who were healthy and seeking lip augmentation. Subjects had to agree to abstain from prohibited facial cosmetic treatments for the duration of the study. Exclusion criteria were: subjects with a previous implant other than HA in or near the intended treatment site; history of other facial treatment/procedure in the previous 6 months below the level of the lower orbital rim that, in the treating investigator's opinion, would interfere with the study injections and/or study assessments or exposes the subject to undue risk by study participation, for example Botulinum toxin injections or another HA filler; a known allergy to HA; and active disease in or near the intended treatment site.
The study was performed in compliance with the ethical principles of the Declaration of Helsinki, Good Clinical Practice (GCP), International Conference on Harmonization guideline for GCP (E6), and the International Organization for Standardization guidelines for clinical studies of medical devices in humans (ISO 14155:2011), including the archiving of essential documents.
Treatment
Treating investigators determined the subjects' treatment group based on their optimal correction required. HARK was injected into the submucosal layer of the lips (up to 2.5 mL in total). Injection techniques included serial puncture, linear threading, and/or cross-hatching. HARR or HARD were injected into moderate or severe NLFs and MLs, respectively (up to 4 mL or 6 mL in total, respectively). These were to be injected into the mid-to-deep dermis using similar injection techniques to HARK.
Eligible subjects were injected by the investigator at baseline. If optimal correction of the lips or surrounding facial wrinkles and folds (if treated) was not achieved at baseline or if the aesthetic appearance could be further improved, a touch-up was offered after 4 weeks; this decision was agreed upon by the investigator and the subject.
Assessments
Subject photographs were captured by personnel from Canfield Scientific Inc. using the VECTRA M3 LIP 3D and VISIA CR 2D imaging systems. Photographs of “at rest” facial expressions were taken before the first injection at baseline and Week 8.
Lip texture and color measurements were evaluated using 2D image analysis with 3 different lens filters. For lip roughness and wrinkles, a fixed automated algorithm analyzed the topographic lip roughness or number of lip lines for both lips from the fusion of standardized, parallel, and cross polarized images. A value was assigned on a scale from 0 to 1, with a higher value indicating greater surface roughness or fractional area of lines detected across the lips. Lip red color was measured via image analysis software that applied an automated RBX-Red algorithm to determined average redness (0–225).
Lip enhancement was evaluated using 3D image analysis similar to previous methodology.17 Lip projection was assessed by measuring the distance (mm) from a reference plane to the most protruding point of the upper and lower lip vermillion border. The reference plane was Burstone's line (B-line).18,19 An ad hoc analysis was conducted using Ricketts' line (E-line)19 as a reference point to assess upper lip projection.
Lip surface area (mm2) was calculated for both lips using the vermillion borders as boundaries. Net lip volume change from baseline (cubic centimeters [cc]) was calculated for both lips for Week 8 after treatment.
Lip distance (height) was assessed by measuring the mean change in distance (mm) from the stomion to the upper and lower lips, or the Cupid's bow. An ad hoc assessment for mouth width was measured as the x-axis distance (mm) between the left oral commissure and the right oral commissure. Philtrum height was considered the y-axis distance (mm) between the philtral crest and the subnasal.
Dynamic strain for the subjects' “blow a kiss” expression was also measured using 3D image analysis.20,21 Positive strain was an indication of surface stretch (i.e., major strain). The areas of interest measured were the upper and lower lips, and the upper and lower perioral area.
Statistical Analysis
Lip photography assessments at baseline and Week 8 were analyzed using descriptive statistics in the full analysis set population. Change from baseline was calculated and the statistical significance of the change from baseline was measured using the one-sample Student t-test if the data were normally distributed or the one-sample Wilcoxon signed rank test if the data required a nonparametric approach. For lip texture and color measurements, data is displayed as percent change from baseline.
Results
Subject Population
A total of 59 subjects were enrolled in the study (HARK group, n = 19; HARK + HARR/HARD group, n = 40). Overall, the mean age of study subjects was 46.2 years. The mean age in the HARK only group was 36.1 years and in the HARK + HARR/HARD group, it was 50.9 years.
For the HARK only group, the total mean volume (initial and touch-up) injected into both lips combined was 1.80 mL (±0.391). For the HARK + HARR/HARD group, the total mean volume (initial and touch-up) injected into both lips combined was 1.6 mL (±0.496). The total mean volume (initial and touch-up) of HARR and/or HARD injected into the facial wrinkles and folds was 2.65 mL (±0.910).
Lip Texture
Lip Roughness
Lip roughness assessments demonstrated that the mean values for upper and lower lip roughness significantly decreased at Week 8 compared with baseline (p ≤ .002), indicating that lip texture was improved following treatment (Figure 1). An example of the lip roughness image analysis is shown in Figure 2A, which shows a 52% and 49% reduction in lip roughness in the upper and lower lips, respectively.
Figure 1:
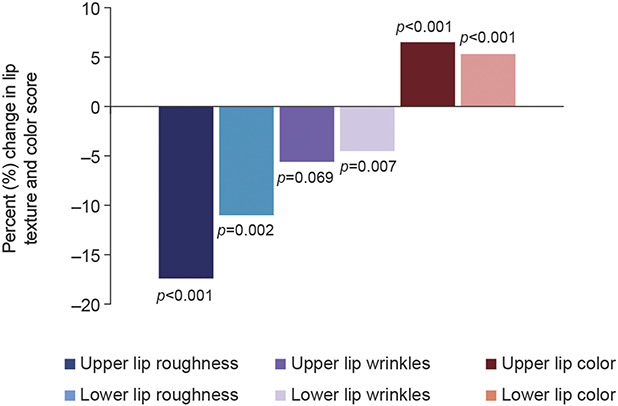
Mean percent change from baseline to Week 8 for lip texture and color measurements.
Figure 2:
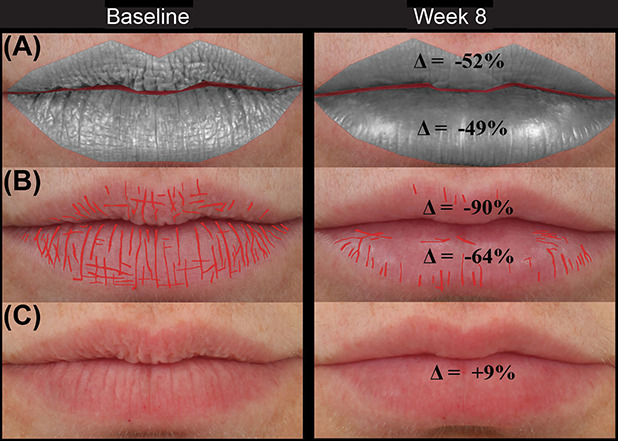
Lip texture of a 51-year-old subject treated with 0.9 mL and 0.55 mL HARK in the upper and lower lip with a (A) reduction in lip roughness (texture) (B) reduction in lip lines and (C) improvement in lip redness at Week 8 compared with baseline.
Lip Wrinkles
At Week 8 compared with baseline, there was a significant reduction in lower lip (p = .007) and reduction in upper lip (p = .069) wrinkles that was not significant (Figure 1). An example of the lip wrinkle image analysis is shown in Figure 2B, which shows a 90% and 64% reduction in lip lines in the upper and lower lips, respectively.
Lip Color
The mean values for upper and lower lip color (redness) significantly increased at Week 8 compared with baseline (Figure 1, p < .001). An example of the lip color image analysis is shown in Figure 2C, which shows a 9% improvement in lip redness at Week 8 compared with baseline.
Lip Enhancement
Lip Projection
Using the B-line as a reference point, lip projection significantly increased at Week 8 compared with baseline (p < .001, Figure 3A). The average distance of projection from the reference B-line for the upper lip increased from 3.09 mm at baseline to 4.23 mm at Week 8. For the lower lip, the average projection increased from 1.82 mm at baseline to 2.74 mm at Week 8.
Figure 3:
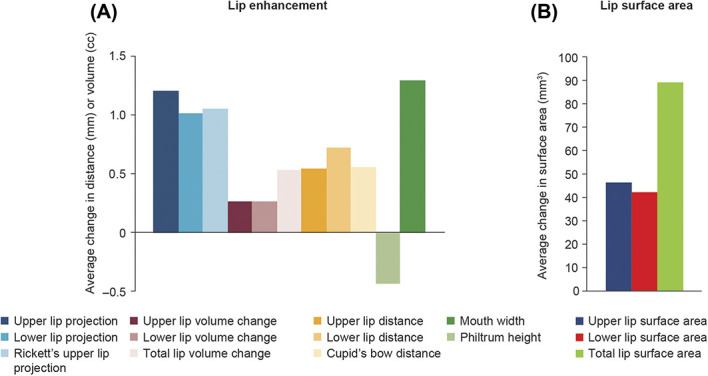
Mean change from baseline to Week 8 for lip enhancement and surface area measurements were all significantly different from baseline (p < .001).
In an ad hoc analysis using the E-line as a reference point, the distance between the furthest projected Cupid's bow landmark and the reference line decreased from 5.97 mm at baseline to 4.96 mm at Week 8, thus indicating increased projection of the upper lip (Figure 3A).
Examples of lip projection image analysis at baseline and Week 8, with both reference lines, is shown in Figure 4, which shows an increase in B-line upper and lower lip projection of 1.16 and 0.78 mm respectively and an increase of 1.47 mm in upper lip distance to the E-line.
Figure 4:
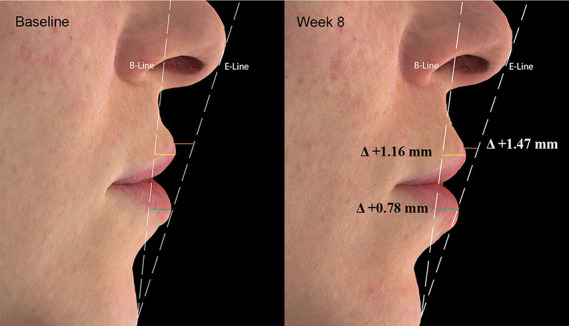
Lip projection of a 33-year-old subject treated with 1.2 mL and 1.1 mL HARK in the upper and lower lips with an increase in B-line and E-line lip projection at Week 8 compared with baseline.
Lip Volume and Surface Area
Overall, the mean changes from baseline in total lip volume and surface area, both lips separately and combined, increased significantly following treatment at Week 8 (Figure 3A and B, p < .001). An example of the lip surface area and total volume change image analysis is shown in Figure 5, which shows an increase of 90 mm3 in total lip surface area and 0.38 cc's in total lip volume using photographic analysis.
Figure 5:
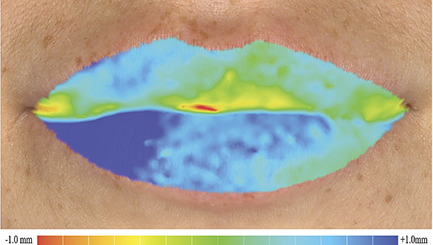
Lip surface area and total volume change of a 26-year-old subject treated with 1.1 mL and 0.4 mL HARK in the upper and lower lips, respectively, with an increase in total lip surface area and in total lip volume.
Lip Height and Width
Overall, there was a significant increase in the mean upper and lower lip height, and Cupid's bow distance at 8 weeks compared with baseline (Figure 3A, p < .001). An ad hoc assessment of philtrum height indicated that the mean distance between the philtral crest and the subnasal significantly decreased (p < .001) at Week 8. In addition, another ad hoc analysis showed that the mean mouth width significantly increased post-treatment (p < .001).
An example of these lip height and width image analyses at baseline and Week 8 is shown in Figure 6, which shows an increase of 0.72, 1.06, 0.41, and 0.78 mm in the upper lip, lower lip, Cupid's bow height, and mouth width measurements at Week 8 compared with baseline. Philtral height decreased by 1.20 mm at Week 8 compared with baseline.
Figure 6:
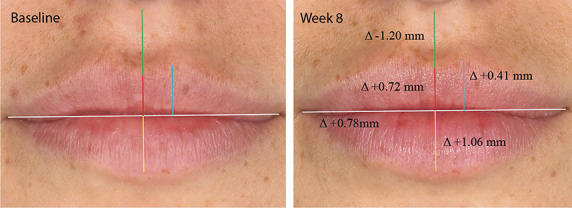
Lip distance of a 26-year-old subject treated with 1.1 mL and 0.4 mL HARK in the upper and lower lips with an increase of lip height, Cupid's bow height, mouth width, and decrease in Philtral height at Week 8 compared with baseline.
Lip Dynamics
Major (stretching) dynamic strain was assessed for the “blow a kiss” facial expression in this study.
Overall, mean changes in major strain (stretch) increased post-treatment compared with baseline (p < .001; Table 1), which shows that the “Blow a Kiss” dynamic strain results from baseline to Week 8; all dynamic strain percentages were significantly different from baseline to Week 8 [p < .001]). An example of the dynamic strain image analysis at Week 8 compared with baseline is shown in Figure 7, which shows a major strain increase of 7%, 6%, 18%, and 8% in the upper perioral, lower perioral, upper lip, and lower lip regions, respectively.
TABLE 1.“.
Blow a Kiss” Dynamic Strain Results
| Area of Interest (AOI) | ||||
| Upper Lip | Lower Lip | Upper Perioral | Lower Perioral | |
| Strain (stretch) (%) | ||||
| Baseline → Week 8 | +9.81 | +9.29 | +5.92 | +6.27 |
All strain (stretch) percentages were significantly different from baseline to Week 8 (p < .001).
Figure 7.
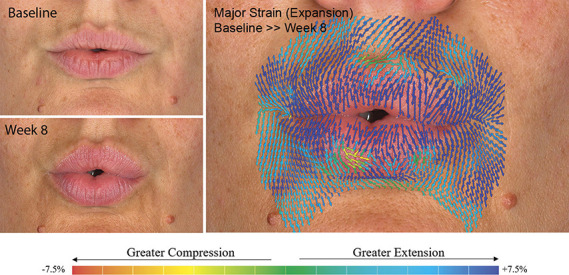
Dynamic strain of a 36-year-old subject treated with 0.5 mL and 0.4 mL HARK in the upper and lower lips with an increase of major strain at Week 8 compared with baseline.
Discussion
The ideal lip is difficult to define but is believed to include good definition of the vermillion border and a balance of lower and upper lip fullness and projection.22 After lip enhancement, it is also important to maintain naturalness of facial expressions.5,6,9
In this study, the goal for lip augmentation was to use flexible XpresHAn technology dermal fillers (HARK, HARR, and HARD) to achieve natural-looking fullness to the lips with appropriate projection of the vermilion and balanced proportions of both the lower and upper lip.
In the current study, a reduction in lip wrinkles and significant improvement in lip texture (lip roughness), and lip color (redness) was observed. Interestingly, enhanced lip redness was a secondary effect of HARK volumization in this study, and has previously been associated with attractiveness in female faces.23 In addition, a significant increase in lip fullness for both upper and lower lips was observed, which included significant enhancement of lip projection, lip surface area and volume, lip and Cupid's bow height, and mouth width, as evidenced by 3D image analysis. Two examples of aesthetic improvement of the lip and perioral region are shown in Supplemental Digital Contents 1 and 2 (see Videos 1 and 2, http://links.lww.com/DSS/A647 and http://links.lww.com/DSS/A648), which are videos of subject results from baseline to Week 8.
Interestingly, lip projection assessments showed that treatment with HARK resulted in increased lip projection closer to ideal lip profiles (B-line: projection of upper lip at 3–4 mm and lower lip at 2–3 mm; E-line: projection of upper lip around 3–4 mm behind the line).19 In addition to increased forward projection of the lips, the ad hoc analysis of philtrum height indicated significant vertical lip projection was achieved. This could be explained by the structural properties of HARK and placement of the product.
Facial expressions are a key aspect of nonverbal communication, and the perioral area, which is especially mobile and prone to significant rhytide formation and volume loss, requires more attention to dynamic evaluation.21,24–26 Assessment of dynamic strain (surface stretch) can provide a quantitative measure of facial aging and is becoming an important aspect of evaluation for rejuvenation treatments designed to produce natural-appearing results.20,21
Previously, it was found that older subjects exhibited significantly greater stretch in the perioral region (NLFs and MLs) compared with younger subjects for a “pursed lip” expression; treatment with HARR and/or HARD significantly reduced the amount of stretch in older subjects at Day 42 compared with baseline.20,21 These results support a dermal tightening effect, likely secondary to volumization of the wrinkles and/or folds.
In the current study, 3D imaging quantified strain (stretch) during the “blow a kiss” facial expression (which also activates the orbicularis oris muscle) both before and after treatment. In contrast to previous studies, the areas of interest analyzed were the lips and upper and lower perioral regions. Treatment with HARK and/or HARR/HARD significantly increased strain (stretch) at Week 8 compared with baseline. The changes observed are indicative of tissue expansion, structural support, and smoothing of lip texture. The tissue expansion in the lips after treatment with HARK increases support for the local muscle activity (orbicularis oris), thus increasing strain (stretch) after treatment. This contrasts to changes previously reported for the NLFs and MLs, which is indicative of volumization of deeper folds and wrinkles (dermal tightening) in areas where less muscle activity is seen.20
Conclusion
This analysis provides an objective measure of the beneficial effects of HARK for lip augmentation with or without HARR/HARD for perioral enhancement, and demonstrates significant improvements in lip texture, color (redness), and enhancement, and an increase in surface stretch (dynamic strain) in the lips and perioral region.
Acknowledgments
The authors would like to thank MedSense Ltd for their assistance in the preparation of this manuscript. The authors would also like to thank Anthony Melione, Nicole Matisak, Anthony Whittaker, and Canfield Scientific for interpretation of quantitative data and figure preparation.
Footnotes
Supplemental digital content is available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal's Web site (www.dermatologicsurgery.org).
A. Nikolis, V. Bertucci and N. Solish are consultants to Galderma.
Contributor Information
Vince Bertucci, Email: vince.bertucci@utoronto.ca.
Nowell Solish, Email: n.solish@utoronto.ca.
Vanessa Lane, Email: vanessa@medicalwritingltd.co.uk.
Alessandra Nogueira, Email: alessandra.nogueira@galderma.com.
References
- 1.Smith S, Lin X, Shamban A. Small gel particle hyaluronic acid injection technique for lip augmentation. J Drugs Dermatol 2013;12:764–9. [PubMed] [Google Scholar]
- 2.Alam M, Gladstone H, Kramer E, Murphy JP, et al. ASDS guidelines of care: injectable fillers. Dermatol Surg 2008;34(Suppl 1):S115–48. [DOI] [PubMed] [Google Scholar]
- 3.Beer KR. Rejuvenation of the lip with injectables. Skin Ther Lett 2007;12:5–7. [PubMed] [Google Scholar]
- 4.Rohrich RJ, Pessa JE. The anatomy and clinical implications of perioral submuscular fat. Plast Reconstr Surg 2009;124:266–71. [DOI] [PubMed] [Google Scholar]
- 5.Lemperle G, Anderson R, Knapp TR. An index for quantitative assessment of lip augmentation. Aesthet Surg J 2010;30:301–10. [DOI] [PubMed] [Google Scholar]
- 6.Solish N, Bertucci V, Percec I, Wagner T, et al. Dynamics of hyaluronic acid fillers formulated to maintain natural facial expression. J Cosmet Dermatol 2019;18:738–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Trookman NS, Rizer RL, Ford R, Mehta R, et al. Clinical assessment of a combination lip treatment to restore moisturization and fullness. J Clin Aesthet Dermatol 2009;2:44–8. [PMC free article] [PubMed] [Google Scholar]
- 8.Penna V, Stark GB, Voigt M, Mehlhorn A, et al. Classification of the aging lips: a foundation for an integrated approach to perioral rejuvenation. Aesthet Plast Surg 2015;39:1–7. [DOI] [PubMed] [Google Scholar]
- 9.Philipp-Dormston WG, Wong C, Schuster B, Larsson MK, et al. Evaluating perceived naturalness of facial expression after fillers to the nasolabial folds and lower face with standardized video and photography. Dermatol Surg 2018;44:826–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hilton S, Sattler G, Berg AK, Samuelson U, et al. Randomized, evaluator-blinded study comparing safety and effect of two hyaluronic acid gels for lips enhancement. Dermatol Surg 2018;44:261–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Segura S, Anthonioz L, Fuchez F, Herbage B. A complete range of hyaluronic acid filler with distinctive physical properties specifically designed for optimal tissue adaptations. J Drugs Dermatol 2012;11(1 Suppl):S5–8. [PubMed] [Google Scholar]
- 12.Lundgren B, Sandkvist U, Bordier N, Gauthier B. Using a new photo scale to compare product integration of different hyaluronan-based fillers after injection in human ex vivo skin. J Drugs Dermatol 2018;17:982–6. [PubMed] [Google Scholar]
- 13.Öhrlund Å. Evaluation of rheometry amplitude sweep cross-over point as an index of flexibility for HA fillers. JCDSA 2018;8:47–54. [Google Scholar]
- 14.Restylane K. Instructions for Use. Fort Worth, TX: Galderma Laboratories, L.P.; 2020. [Google Scholar]
- 15.Baumann L, Weiss RA, Grekin S, Narins R, et al. Comparison of Hyaluronic Acid Gel with (HARDL) and without Lidocaine (HAJUP) in the treatment of moderate-to-severe nasolabial folds: a randomized, evaluator-blinded study. Dermatol Surg 2018;44:833–40. [DOI] [PubMed] [Google Scholar]
- 16.Fagien S, Monheit G, Jones D, Bank D, et al. Hyaluronic Acid Gel with (HARRL) and without Lidocaine (HAJU) for the treatment of moderate-to-severe nasolabial folds: a randomized, evaluator-blinded, phase III study. Dermatol Surg 2018;44:549–56. [DOI] [PubMed] [Google Scholar]
- 17.Sawyer AR, See M, Nduka C. 3D stereophotogrammetry quantitative lip analysis. Aesthetic Plast Surg 2009;33:497–504. [DOI] [PubMed] [Google Scholar]
- 18.Karunakara RV, Sahoo N, Singaraju GS. Which line to kiss? A review of reference lines for lip profile. Ann Essen Dentistry 2013;4:35–9. [Google Scholar]
- 19.Legan HL, Burstone CJ. Soft tissue cephalometric analysis for orthognathic surgery. J Oral Surg 1980;38:741–51. [PubMed] [Google Scholar]
- 20.Percec I, Bertucci V, Solish N, Wagner T, et al. An objective, quantitative, dynamic assessment of hyaluronic acid fillers that adapt to facial movement. Plast Reconstr Surg 2020;145:295e–305e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Hsu VM, Wes AM, Tahiri Y, Cornman-Homonoff J, et al. Quantified facial soft-tissue strain in animation measured by real-time dynamic 3-dimensional imaging. Plast Reconstr Surg Glob Open 2014;2:e211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Garcia de Mitchell C, Pessa J, Schaverien M, Rohrich R. The Philtrum: anatomical observations from a new perspective. Plast Reconstr Surg 2008;122:1756–60. [DOI] [PubMed] [Google Scholar]
- 23.Stephen ID, McKeegan AM. Lip colour affects perceived sex typicality and attractiveness of human faces. Perception 2010;39:1104–10. [DOI] [PubMed] [Google Scholar]
- 24.Lin Y, Lin H, Lin Q, Zhang J, et al. A novel three-dimensional smile analysis based on dynamic evaluation of facial curve contour. Sci Rep 2016;6:22103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Jack RE, Schyns PG. The human face as a dynamic tool for social communication. Curr Biol 2015;25:R621–34. [DOI] [PubMed] [Google Scholar]
- 26.Michaud T, Gassia V, Belhaouari L. Facial dynamics and emotional expressions in facial aging treatments. J Cosmet Dermatol 2015;14:9–21. [DOI] [PubMed] [Google Scholar]